quand associer anticoagulants et anti- aggrégants ... · engl. j. med. 19 juill 2007;357(3):217‑...
TRANSCRIPT
Quand associer anticoagulants et anti-aggrégants plaquettaires
Gabriel O'CONNELL, Interne en médecine générale, UJF Médecine Grenoble
Introduction
• Large prescrip+on des AAP et AVK
• Bénéfices démontrés en monothérapie
• Par+cularité de certaines situa+ons amenant à une bithérapie voir trithérapie an+-‐thrombo+que
– Risque hémorragique mineur et majeur accru.

PLAN
l INTRODUCTION l I. Méthode l II. Résultats
l A. Après un infarctus du myocarde l B. Fibrillation auriculaire l C. Artériopathie oblitérante des membres inférieurs l D. Prothèses valvulaires cardiaques mécaniques l E. Cas particulier des stents l F. Les nouveaux anticoagulants
l II. Synthèse l CONCLUSION
I. Méthode
l Renouvellement d'une prescription en cabinet de médecine générale l → état actuel des connaissances ? l Institutions :
l HAS l Société Française de Cardiologie l Société Européenne de Cardiologie l Health InternetWork Acces to Research Initiative
(HINARI) l Recherche par mots clés sur PubMed
l Association antiagrégant plaquettaire anticoagulant - anticoagulants oraux - traitement antithrombotique - risque hémorragique - risque thrombo-embolique.
l Revue narrative de la littérature 1987-2012 l 28 références sélectionnées.
II. RESULTATS
A. Après un infarctus du myocarde • Pas de bénéfice à l'association (1)(2)
– Diminution non significative du risque de thrombo-embolie artérielle (AVK+AAP vs AVK)
• OR 0,69 ; IC 95% 0,35-1,36 (1) – Ou d'une récidive d'infarctus (AVK+AAP vs AAP)
• RR 0,77 ; IC 95 % 0,58-1,03 (2) • AVK>AAP pour traiter la coronaropathie chronique (3)
– Warfarine vs aspirine : risque (mort, IDM, AVC) diminué de 19% • RR 0,81 ; IC 95% 0,69-0,95 ; p=0,03
– Au prix d'un risque hémorragique majeur accru. • RR 0,25 ; IC 95% 0,10-0,60 (AAP vs AVK)
• Idem si AVK INR<2 + aspirine faible dose (4)(5)

B. Fibrillation auriculaire (CHADSVASC≥2)
• Pas de bénéfice à l'association (1)(2)(4)(6) que ce soit pour un INR>2 (1)(2)(4), ou <2 (6)
– Risque thrombo-embolique artériel inchangé • OR 0,99 ; IC 95% 0,47-2,07 (1) • RR 2,13 ; IC 95%0,20-23,03 (2)
– Risque hémorragique majeur augmenté • OR 1,43 ; IC 95% 1-2,02 (1)
• Or,
– AVK>AAP pour traiter les coronaropathes chroniques (3) – AVK>Aspirine + clopidogrel (7)
• Donc pour un patient en FA CHADS>2 AVK seul même si coronaropathie associée
...Cependant
→ 20 % des patients sous anticoagulants reçoivent également une antiagrégation (8), généralement pour une coronoropathie
associée.

C. Artériopathie oblitérante des membres inférieurs
• Pas de bénéfice à l'association (9)(10) – AVK+AAP n'est pas > AAP seul
• RR 0,92, IC 95% 0,73-1,16, p = 0,48 – plus d'hémorragies mortelles
• RR 3,41, IC 95% 1,84-6,35, p<0,001. • Idem pour les pontages artériels périphériques (11) • Pas de bénéfice des anticoagulants versus placebo (12)(13)
– augmentation de la mortalité : • RR 2,19 IC 95% 0,84-5,73
– augmentation du risque hémorragique • RR 24,84 IC95% 1,48-416,93.
• Donc AAP obligatoire si AOMI.
D. les prothèses valvulaires cardiaques
• Bénéfice à l'association pour les prothèses mécaniques (1)(2)
– Risque thrombo-embolique diminué • OR 0,27 ; IC 95% 0,15-0,49 (1) • RR 0,3 ; IC 95% 0,19-0,58 (2)
– Risque d'hémorragies majeures augmenté • OR 1,49 ; IC 95% 1-2,23 (1) • RR 1,58% ; IC 95% 1,02-2,44 (2)
– mortalité diminuée • RR 0,43 ; IC 95% 0,23-0,81 (2)
E. Cas particulier des stents
• Réduction du risque de mort de cause cardio-vasculaire ou de récidive d'IDM de 31% (p=0,002) avec bithérapie AAP après pose de stent (vs monothérapie) (14) → Mais que faire avec les patients déjà sous AVK avant la pose de stent??
→ efficacité/sûreté de la triple association (AVK+2AAP)? (4)
• Étude WOEST (15) – AVK+clopidogrel vs AVK+aspirine+clopidogrel
• Réduction de 64% des saignements • Mortalité diminuée RR 0,39 ; p=0,027
→ Donc après IDM+stent, AVK+clopidogrel 1 an
F. Les nouveaux anticoagulants oraux (NAO)
l En post-IDM l Pas de bénéfices pour Dabigatran (16) et
Apixaban (17) l Bénéfice montré dans l'étude ATLAS ACS2-
TIMI (18) pour le rivaroxaban, à très faible dose.
l Pas d'AMM l Et les autres indications ?

III. Synthèse
Bénéfices reconnus de l'association AAP-AVK • Prothèses valvulaires mécaniques cardiaques • Dans l'année de pose d'un stent cardiaque + indication préalable d'AVK • AOMI + indication d'AVK → Une question ressort de cette recherche : supériorité des AVK sur les AAP en post-IDM ? Hémorragies...
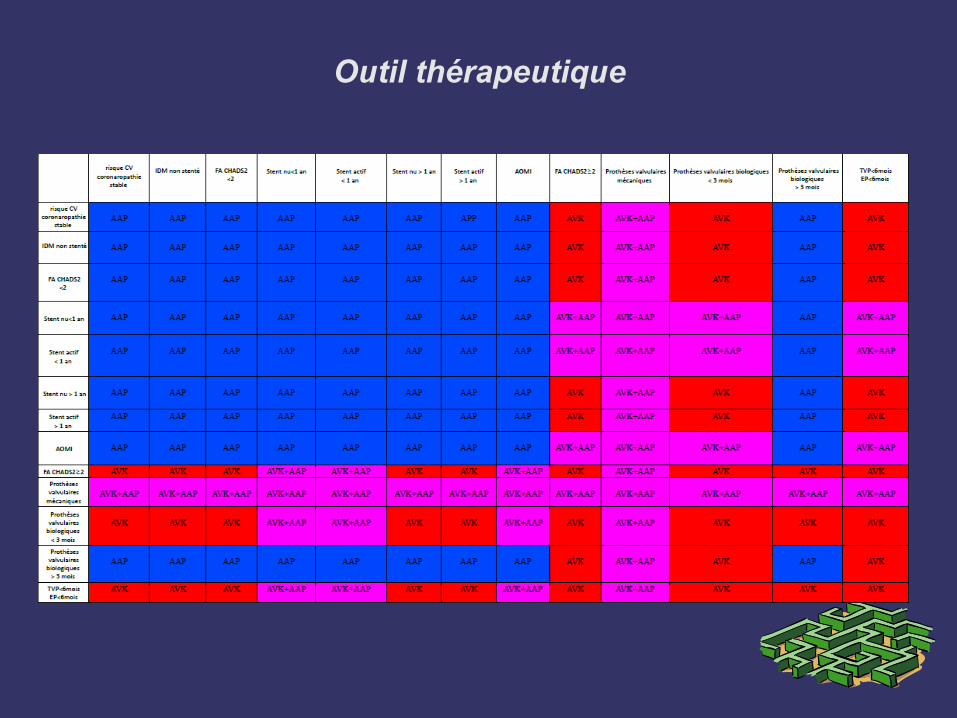
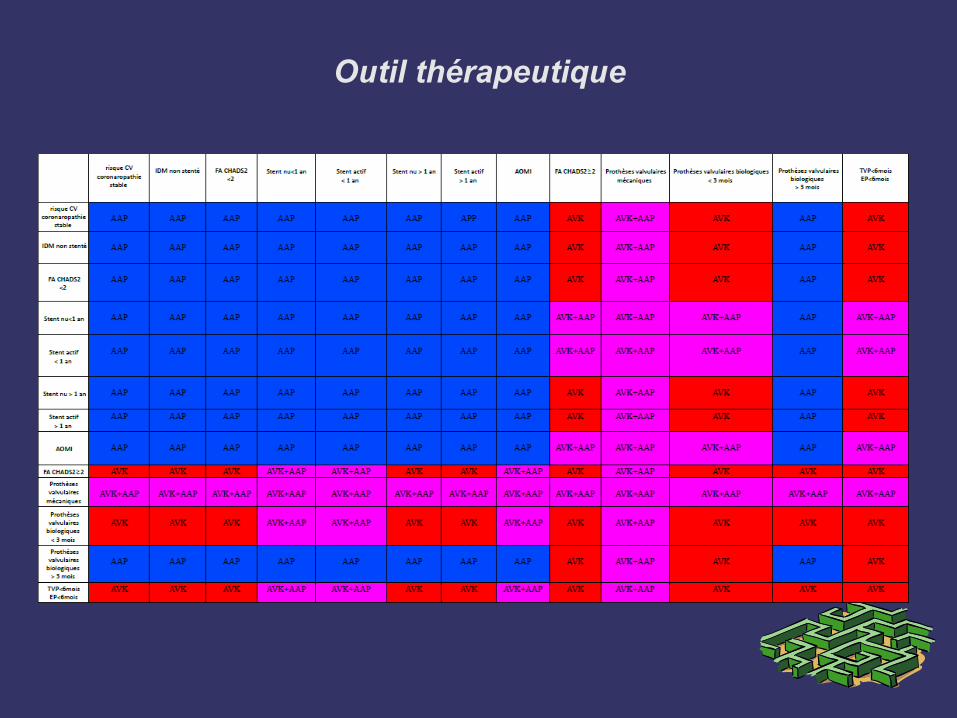
Outil thérapeutique

Conclusion : dans les zones floues, optimiser le traitement

Conclusion : suite
• Score HAS-BLED (2010) (24) • Score CHADS-VASC
Outil thérapeutique
Merci pour votre écoute
Gabriel O'CONNELL, Interne en médecine générale, UJF Médecine Grenoble
Références
1. Randomised double-blind trial of fixed low-dose warfarin with aspirin after myocardial infarction. The Lancet. août 1997;350(9075):389‑ 396.
2. Adjusted-dose warfarin versus low-intensity, fixed-dose warfarin plus aspirin for high-risk patients with atrial fibrillation: Stroke Prevention in Atrial Fibrillation III randomised clinical trial. Lancet. 7 sept 1996;348(9028):633‑ 638.
3. Shireman TI, Howard PA, Kresowik TF, Ellerbeck EF. Combined anticoagulant-antiplatelet use and major bleeding events in elderly atrial fibrillation patients. Stroke. oct 2004;35(10):2362‑ 2367.
4. Mehta SR, Yusuf S, Peters RJ, Bertrand ME, Lewis BS, Natarajan MK, et al. Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE study. Lancet. 18 août 2001;358(9281):527‑ 533.
5. Larson RJ, Fisher ES. Should aspirin be continued in patients started on warfarin? J Gen Intern Med. août 2004;19(8):879‑ 886.

Références : suite
6. Johnson WC, Williford WO. Benefits, morbidity, and mortality associated with long-term administration of oral anticoagulant therapy to patients with peripheral arterial bypass procedures: a prospective randomized study. J. Vasc. Surg. mars 2002;35(3):413‑ 421.
7. Hurlen M, Abdelnoor M, Smith P, Erikssen J, Arnesen H. Warfarin, aspirin, or both after myocardial infarction. N. Engl. J. Med. 26 sept 2002;347(13):969‑ 974.
8. Dewilde W, Berg JT. Design and rationale of the WOEST trial: What is the Optimal antiplatElet and anticoagulant therapy in patients with oral anticoagulation and coronary StenTing (WOEST). Am. Heart J. nov 2009;158(5):713‑ 718.
9. Dettori AG, Pini M, Moratti A, Paolicelli M, Basevi P, Quintavalla R, et al. Acenocoumarol and pentoxifylline in intermittent claudication. A controlled clinical study. The APIC Study Group. Angiology. avr 1989;40(4 Pt 1):237‑ 248.
Références : suite
10. Dentali F, Douketis JD, Lim W, Crowther M. Combined aspirin-oral anticoagulant therapy compared with oral anticoagulant therapy alone among patients at risk for cardiovascular disease: a meta-analysis of randomized trials. Arch. Intern. Med. 22 janv 2007;167(2):117‑ 124.
11. Connolly S, Pogue J, Hart R, Pfeffer M, Hohnloser S, Chrolavicius S, et al. Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): a randomised controlled trial. Lancet. 10 juin 2006;367(9526):1903‑ 1912.
12. Anand S, Yusuf S, Xie C, Pogue J, Eikelboom J, Budaj A, et al. Oral anticoagulant and antiplatelet therapy and peripheral arterial disease. N. Engl. J. Med. 19 juill 2007;357(3):217‑ 227.

Références : suite
13. Alonso-Coello P, Bellmunt S, McGorrian C, Anand SS, Guzman R, Criqui MH, et al. Antithrombotic therapy in peripheral artery disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. févr 2012;141(2 Suppl):e669S‑ 90S.
14. You JJ, Singer DE, Howard PA, Lane DA, Eckman MH, Fang MC, et al. Antithrombotic Therapy for Atrial FibrillationAntithrombotic Therapy for Atrial FibrillationAntithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. CHEST Journal. 1 févr 2012;141(2_suppl):e531S‑ e575S.
15. De Smit P, Van Urk H. Dutch oral anticoagulant trial. Acta Chir Austriaca. 1992;5‑ 7.

Références : suite
16. Oldgren J, Budaj A, Granger CB, Khder Y, Roberts J, Siegbahn A, et
al. Dabigatran vs. placebo in patients with acute coronary syndromes on dual antiplatelet therapy: a randomized, double-blind, phase II trial. Eur. Heart J. nov 2011;32(22):2781‑2789.
17. Alexander JH, Lopes RD, James S, Kilaru R, He Y, Mohan P, et al.
Apixaban with antiplatelet therapy after acute coronary syndrome. N. Engl. J. Med. 25 août 2011;365(8):699‑708
18. Mega JL, Braunwald E, Wiviott SD, Bassand J-P, Bhatt DL, Bode C,
et al. Rivaroxaban in patients with a recent acute coronary syndrome. N. Engl. J. Med. 5 janv 2012;366(1):9‑19.