prise en charge initiale des avc ischémiques · pdf fileprise en charge initiale des...
TRANSCRIPT
Prise en charge initiale des AVC ischémiques
Vincent Larrue
Service de Neurologie Vasculaire
INSERM U1048
Hôpital Rangueil CHU de Toulouse
Prise en charge initiale des AVC ischémiquesLes interventions d’efficacité prouvée
• Unité médicale spécialisée en neurologie vasculaire
• Fibrinolyse intraveineuse < 4,5 h
• Aspirine
Efficacité des stroke units
• Diminution de mortalité : 15%
• Diminution de dépendance : 22%
• Diminution d’institutionnalisation : 20%
Cochrane Database Syst Rev 2007
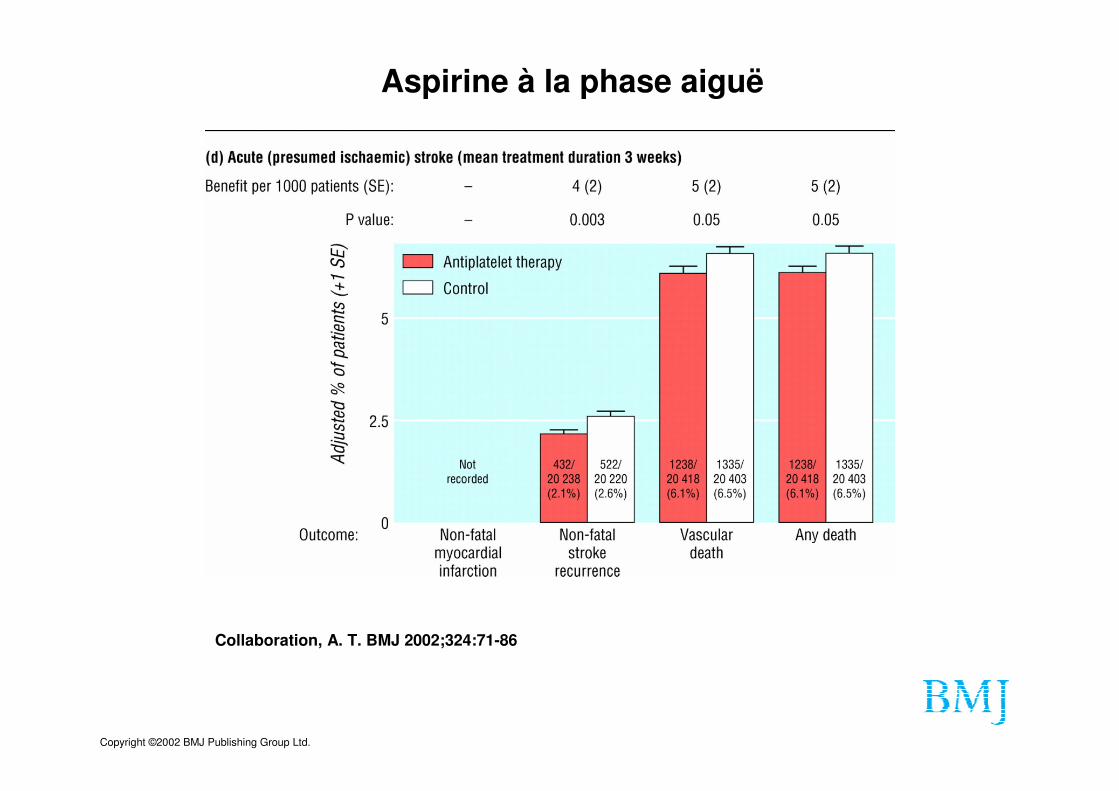
Copyright ©2002 BMJ Publishing Group Ltd.
Collaboration, A. T. BMJ 2002;324:71-86
Aspirine à la phase aiguë
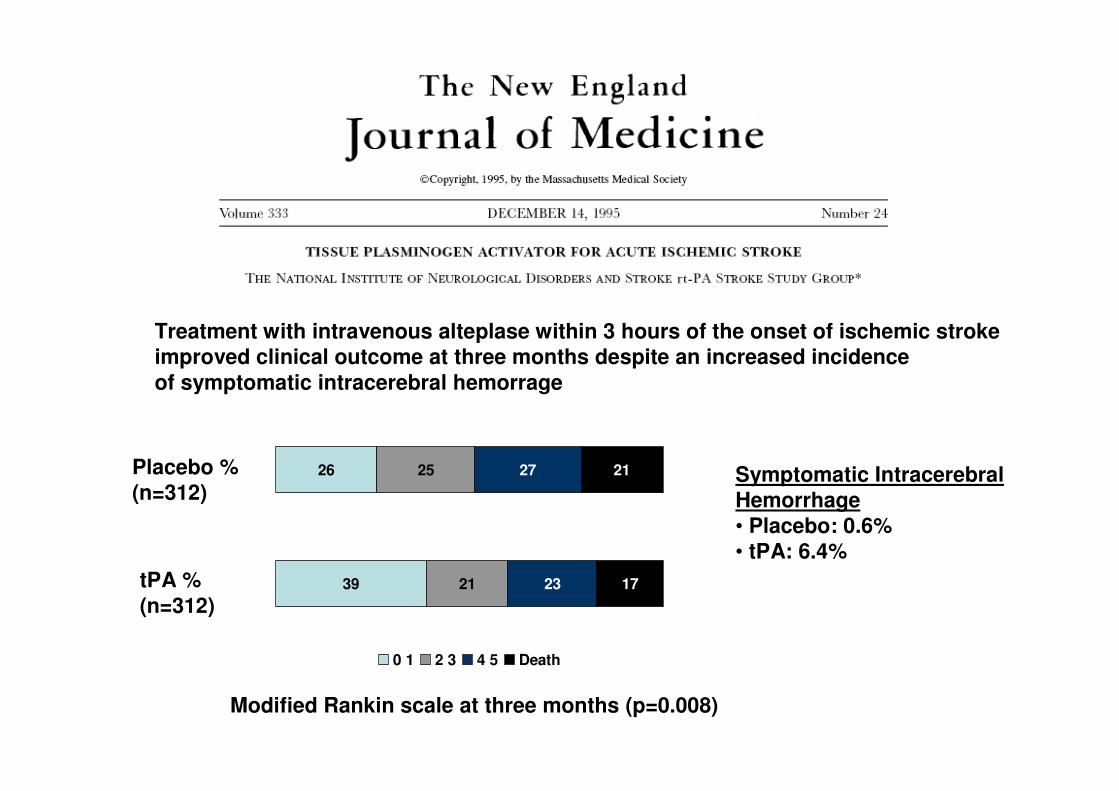
39
26
21
25
23 17
2127
0 1 2 3 4 5 Death
Symptomatic IntracerebralHemorrhage• Placebo: 0.6%• tPA: 6.4%
Treatment with intravenous alteplase within 3 hours of the onset of ischemic strokeimproved clinical outcome at three months despite an increased incidenceof symptomatic intracerebral hemorrage
Placebo %(n=312)
tPA %(n=312)
Modified Rankin scale at three months (p=0.008)
Clinal trials of intravenous alteplase with a longer delay in treatment initiation (up to six hours) are negative
• ECASS 1: 0-6 h (620 patients)
• ECASS 2 : 0-6 h (800 patients)
• ATLANTIS A : 0-6 h (142 patients)
• ATLANTIS B : 3-5 h (547 patients)
• IST 3 : 0-6h (3035 patients)
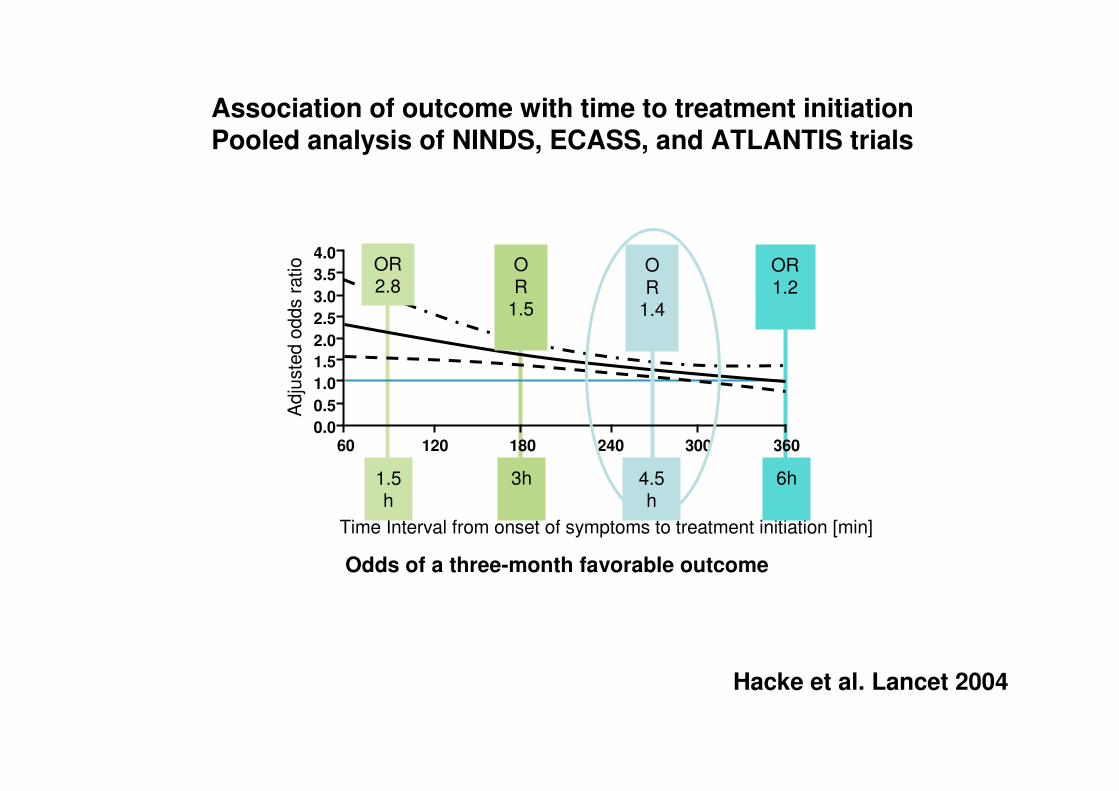
Time Interval from onset of symptoms to treatment initiation [min]
Adju
ste
d o
dds r
atio
1.5h
OR 2.8
3h
OR
1.5
4.5h
OR
1.4
6h
OR 1.2
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
60 120 180 240 300 360
Hacke et al. Lancet 2004
Association of outcome with time to treatment initiationPooled analysis of NINDS, ECASS, and ATLANTIS trials
Odds of a three-month favorable outcome

53
45
24
28
16 7
819
0 1 2 3 4 5 Death
Modified Rankin scale at three months (p=0.02)
Placebo %(n=403)
tPA %(n=418)
Symptomatic IntracerebralHemorrhage• tPA: 7.9%• Placebo: 3.5%
Alteplase was associated with a modest but significant improvement in clinical outcome
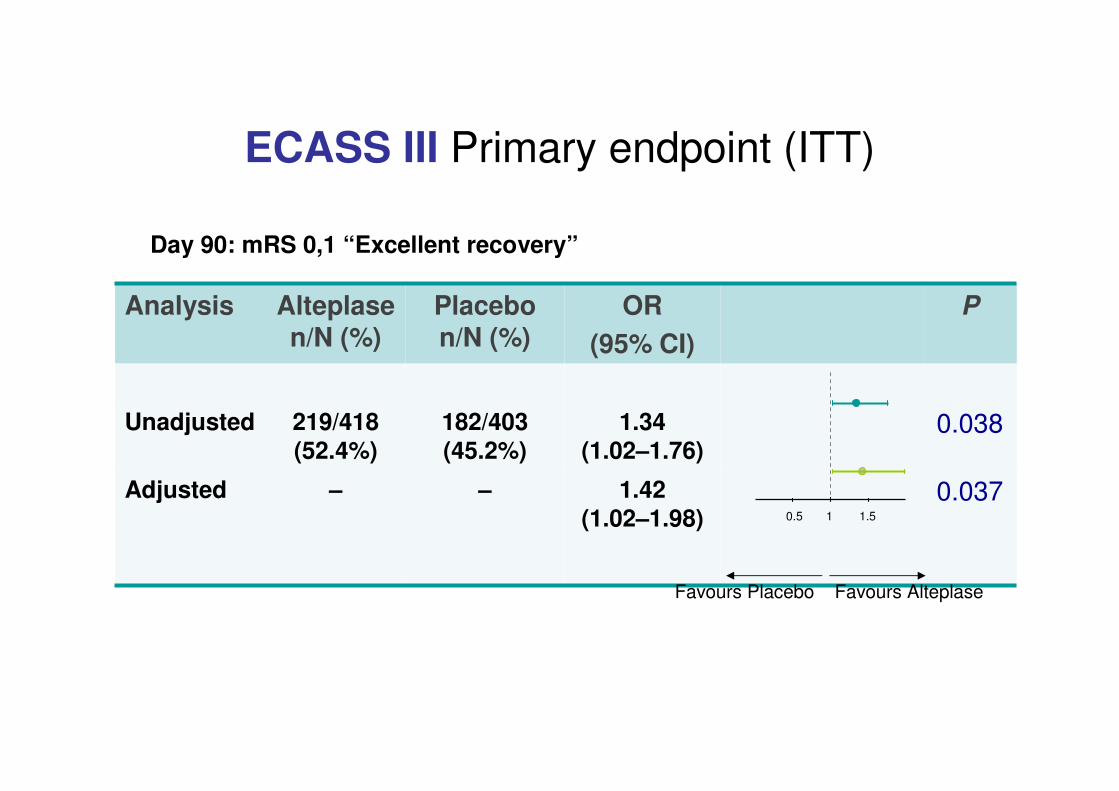
ECASS III Primary endpoint (ITT)
Analysis Alteplasen/N (%)
Placebon/N (%)
OR
(95% CI)
P
Unadjusted 219/418 (52.4%)
182/403 (45.2%)
1.34 (1.02–1.76)
0.038
Adjusted – – 1.42 (1.02–1.98)
0.037
Day 90: mRS 0,1 “Excellent recovery”
0.5 1 1.5
Favours Placebo Favours Alteplase
Time Interval from onset of symptoms to treatment initiation [min]
Adju
ste
d o
dds r
atio
1.5h
OR 2.8
3h
OR 1.5
4.5h
OR 1.4
6h
OR 1.2
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
60 120 180 240 300 360
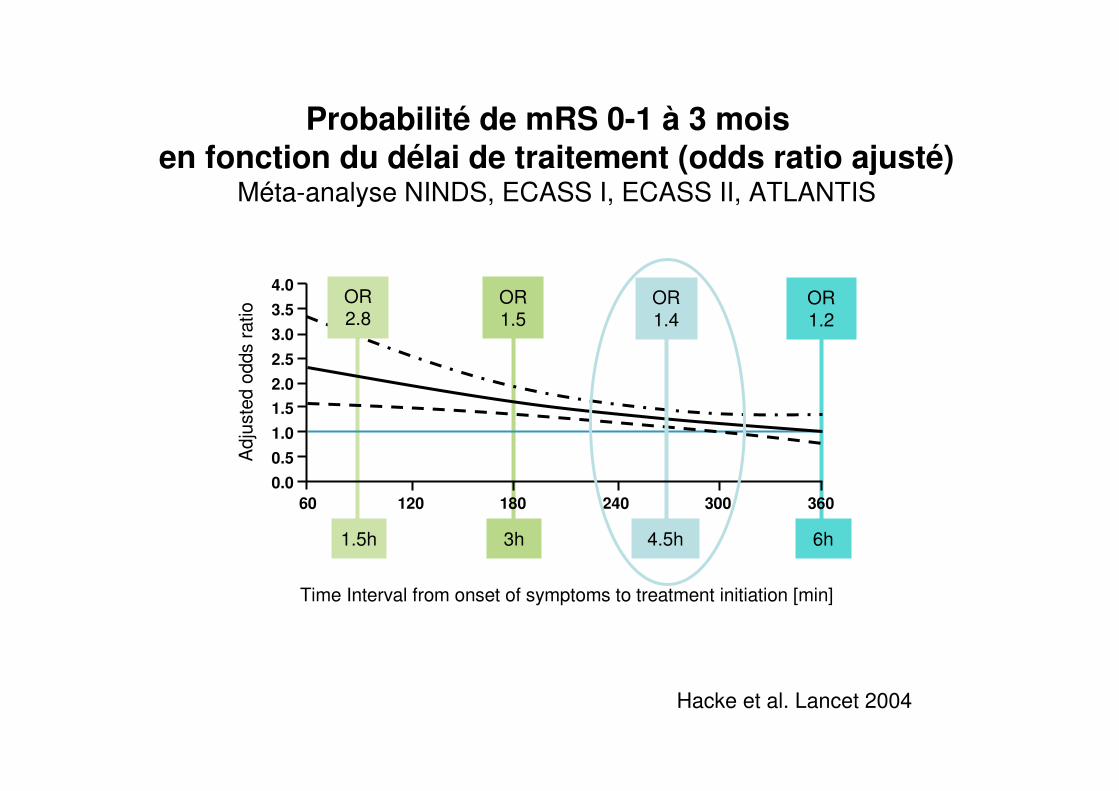
Probabilité de mRS 0-1 à 3 mois en fonction du délai de traitement (odds ratio ajusté)
Méta-analyse NINDS, ECASS I, ECASS II, ATLANTIS
Hacke et al. Lancet 2004

Updated pooled analysis of ECASS, NINDS, ATLANTIS, and EPITHET trials
• Approximately 5 patients need to be treated 0-90 min, 9 patients 91-180 min, and 15 patients 181-270 min after symptom onset for one of them to have an excellent outcome (mRS 0-1) attributable to treatment
Lees et al. Lancet 2010
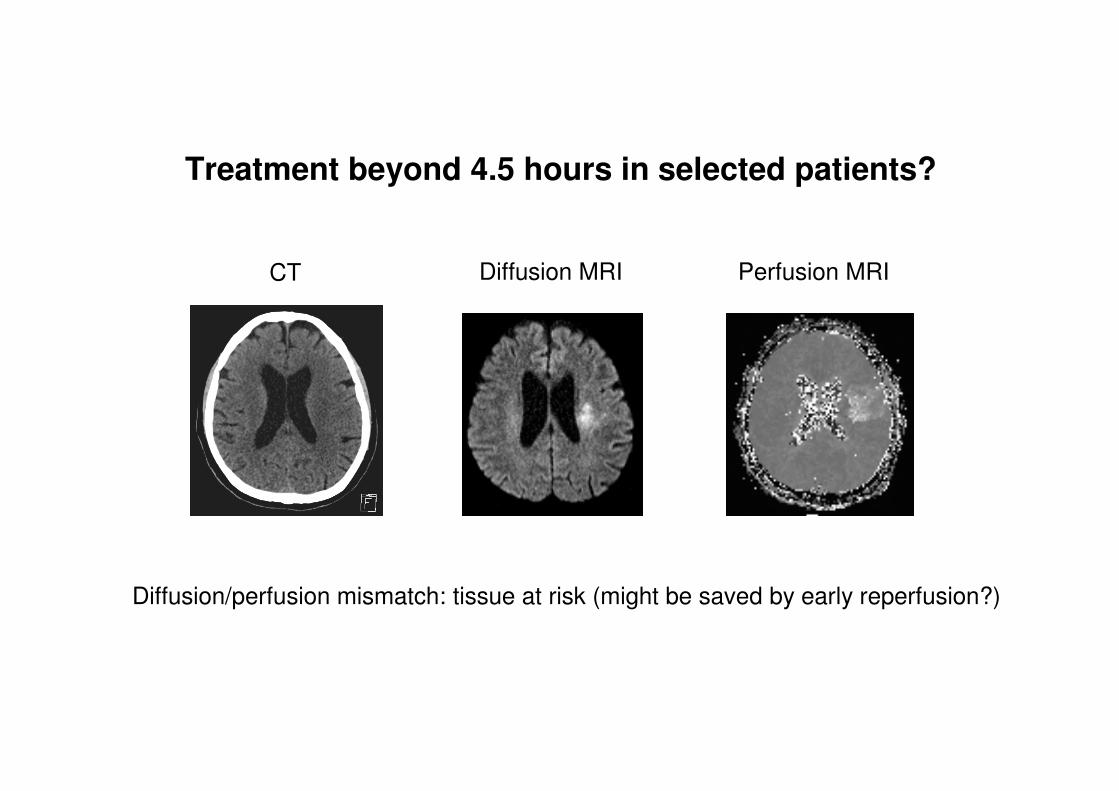
Diffusion MRI Perfusion MRI
Diffusion/perfusion mismatch: tissue at risk (might be saved by early reperfusion?)
Treatment beyond 4.5 hours in selected patients?
CT
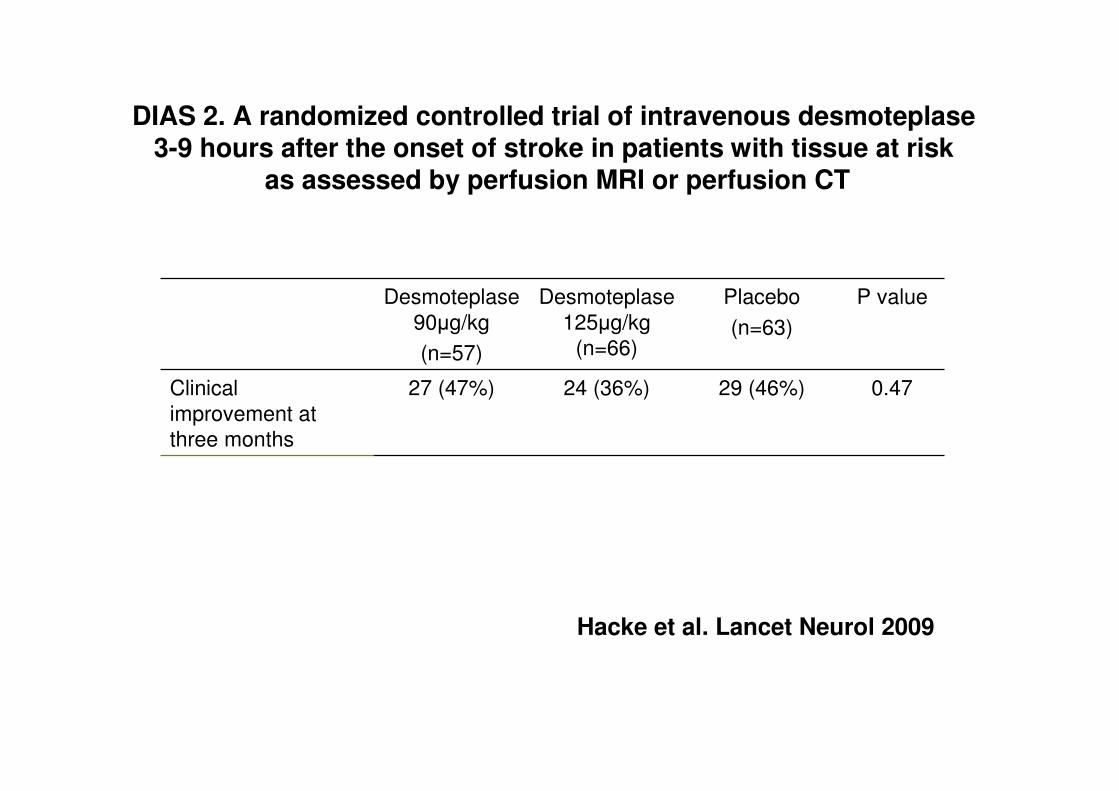
DIAS 2. A randomized controlled trial of intravenous desmoteplase3-9 hours after the onset of stroke in patients with tissue at risk
as assessed by perfusion MRI or perfusion CT
Desmoteplase
90µg/kg
(n=57)
Desmoteplase
125µg/kg
(n=66)
Placebo
(n=63)
P value
Clinical
improvement at
three months
27 (47%) 24 (36%) 29 (46%) 0.47
Hacke et al. Lancet Neurol 2009

Prise en charge initiale des AVC ischémiquesCe qui se fait mais n’a pas encore d’efficacité certaine
• Fibrinolyse intraveineuse hors AMM
• Thrombectomie
• Traitement anticoagulant
• Traitements antiagrégants plaquettaires combinés
• Craniectomie
Fibrinolyse intraveineuse hors AMM
• Patients >80 ans
• AVC du réveil
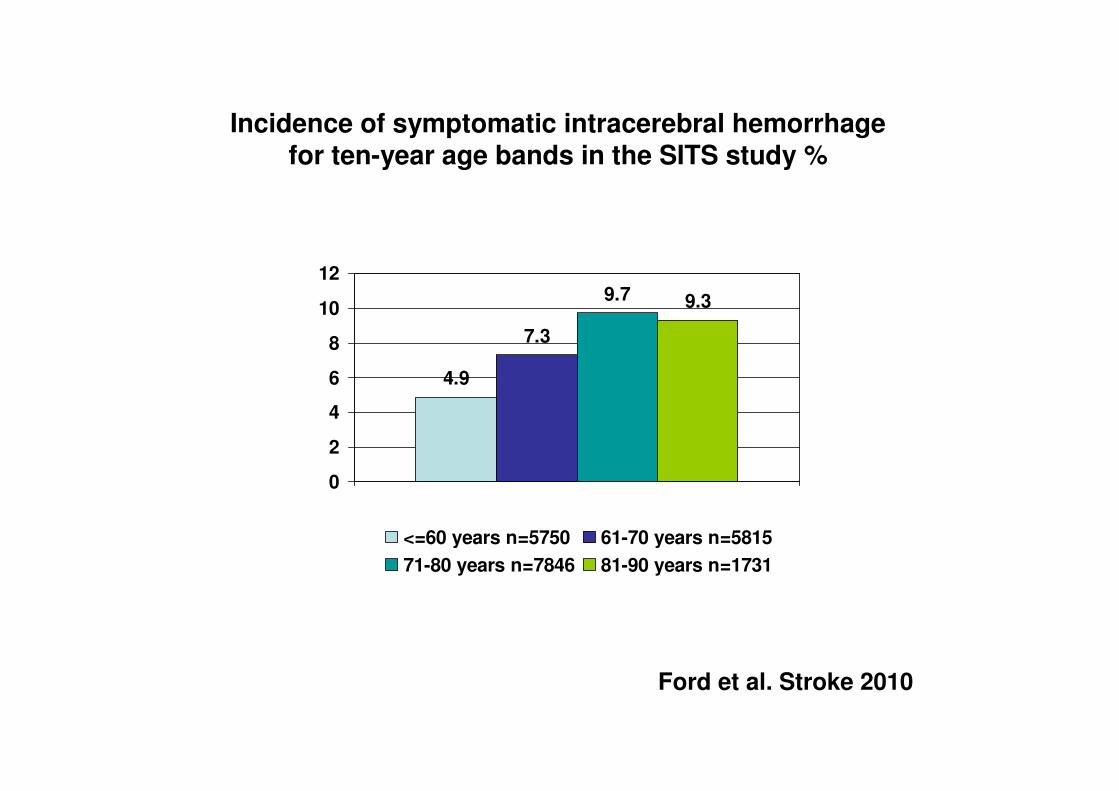
4.9
7.3
9.7 9.3
0
2
4
6
8
10
12
<=60 years n=5750 61-70 years n=5815
71-80 years n=7846 81-90 years n=1731
Ford et al. Stroke 2010
Incidence of symptomatic intracerebral hemorrhagefor ten-year age bands in the SITS study %
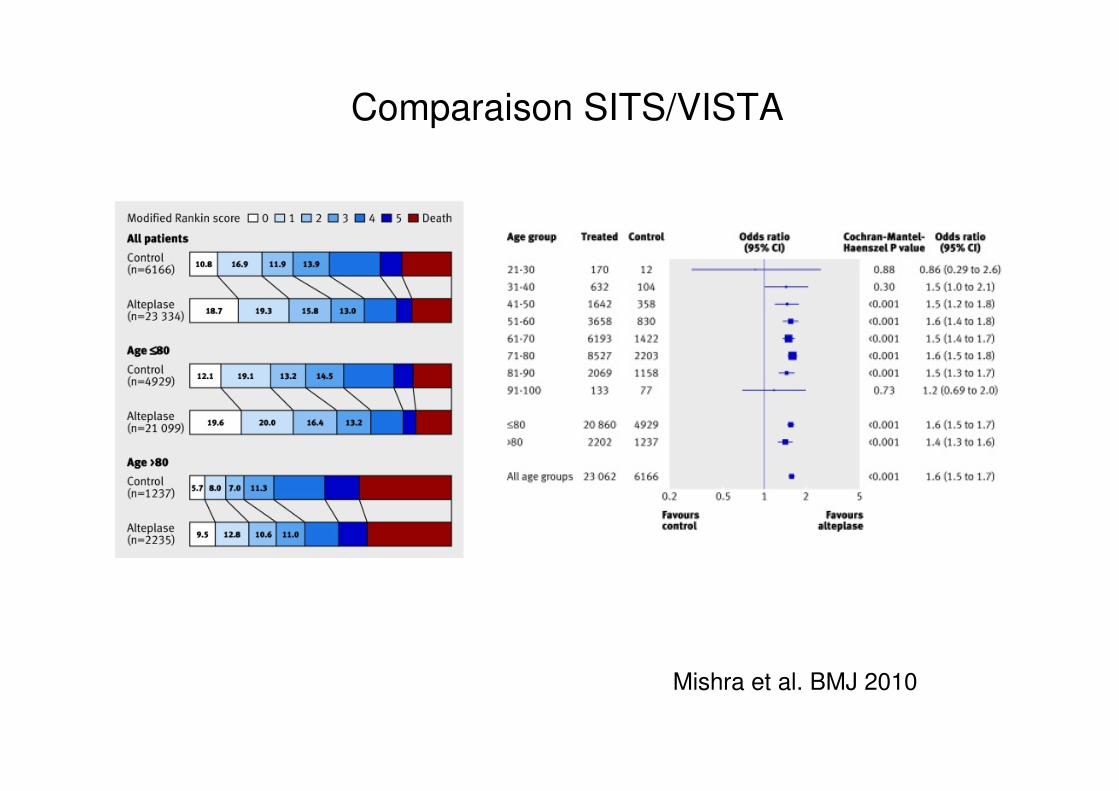
Mishra et al. BMJ 2010
Comparaison SITS/VISTA
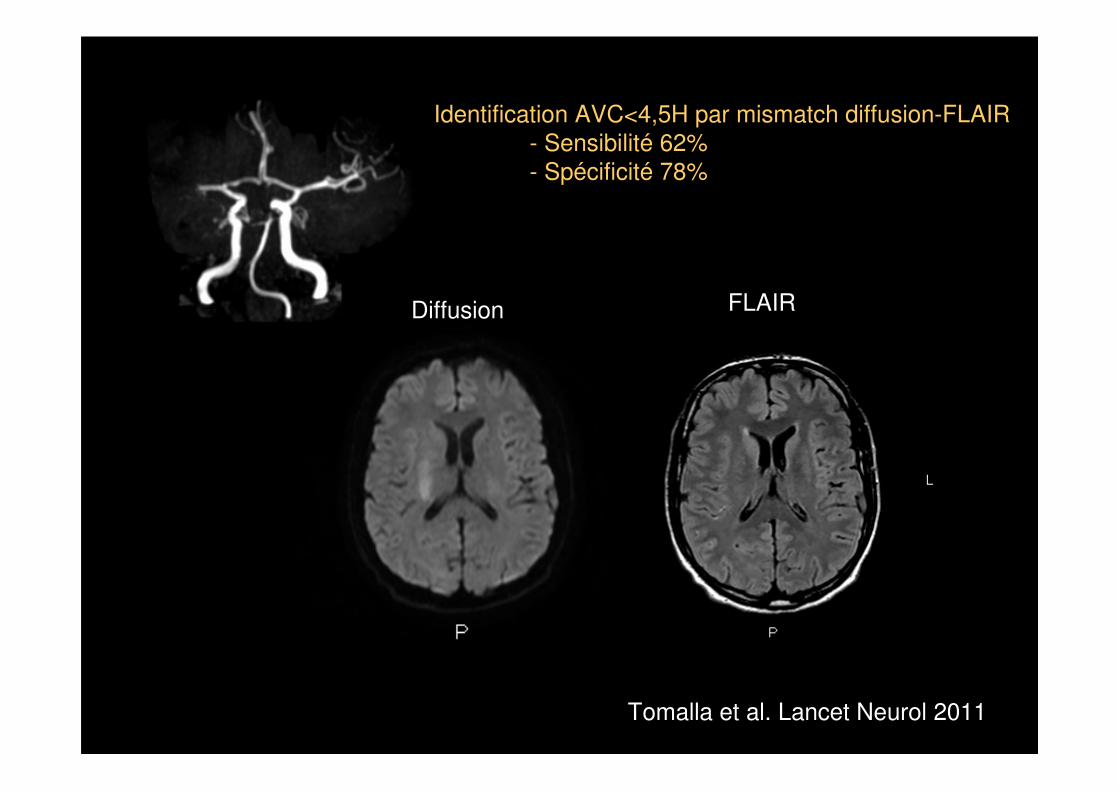
Diffusion FLAIR
Identification AVC<4,5H par mismatch diffusion-FLAIR
- Sensibilité 62%- Spécificité 78%
Tomalla et al. Lancet Neurol 2011
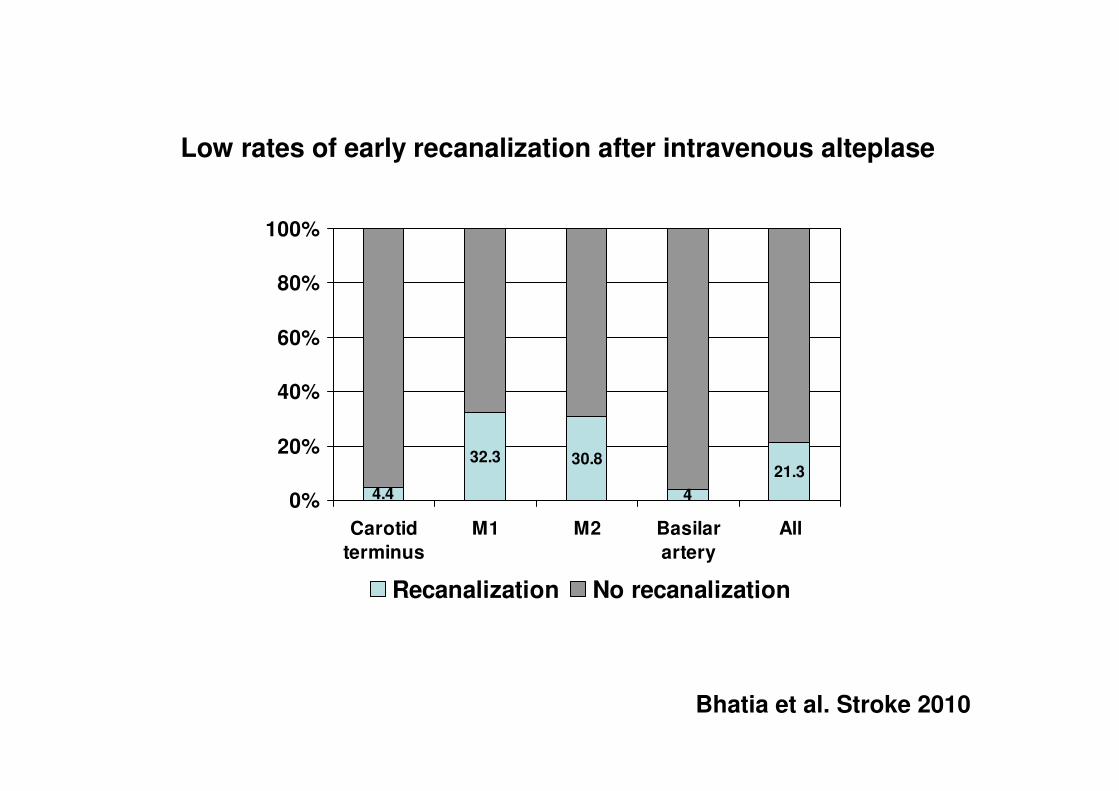
Low rates of early recanalization after intravenous alteplase
4.4
32.3 30.8
4
21.3
0%
20%
40%
60%
80%
100%
Carotid
terminus
M1 M2 Basilar
artery
All
Recanalization No recanalization
Bhatia et al. Stroke 2010
Thrombectomie
• Dans les occlusions emboliques(=la plupart des AVC en dehors deslacunes)
• Maturité de la technique, excellents résultats en termes de désobstruction avec les stents récupérables
• Seule ou après fibrinolyse intraveineuse
• A évaluer contre fibrinolyse intraveineuse dans phase 3
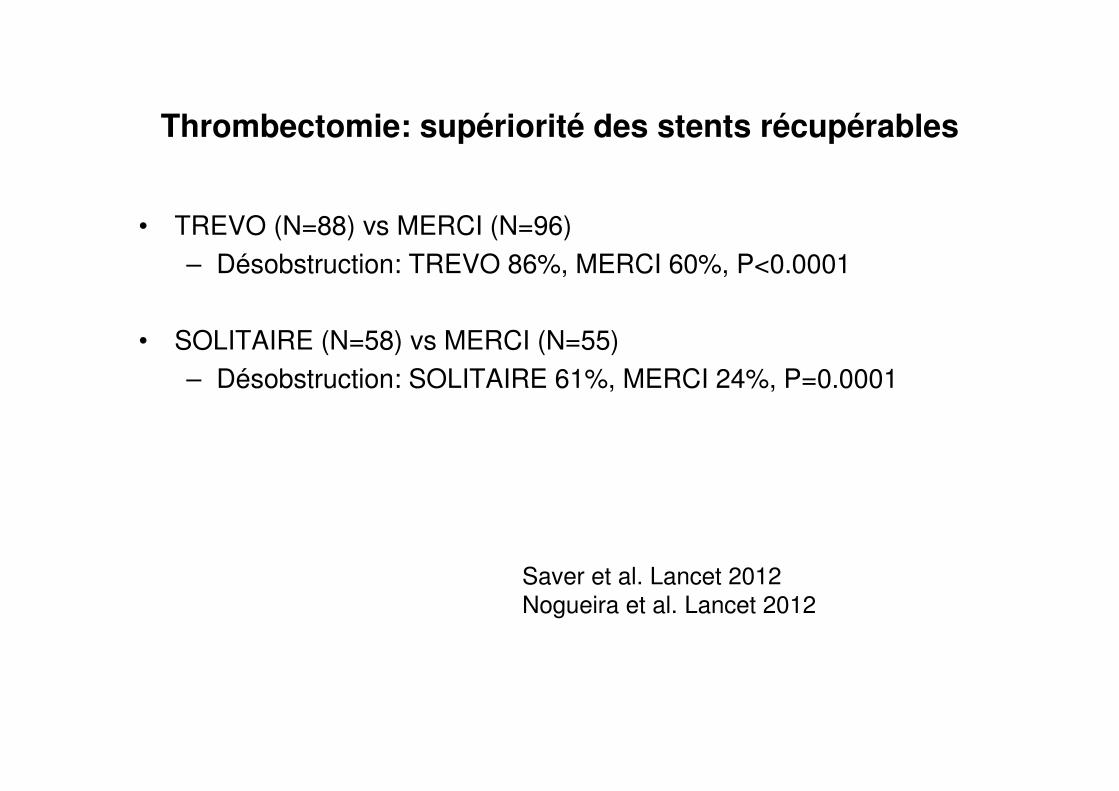
Thrombectomie: supériorité des stents récupérables
• TREVO (N=88) vs MERCI (N=96)
– Désobstruction: TREVO 86%, MERCI 60%, P<0.0001
• SOLITAIRE (N=58) vs MERCI (N=55)
– Désobstruction: SOLITAIRE 61%, MERCI 24%, P=0.0001
Saver et al. Lancet 2012
Nogueira et al. Lancet 2012

Ongoing trials of combined i.v/i.a approach to recanalization
• IMS 3
– 900 patients
– Intravenous thrombolysis with full dose alteplase vs low dose completed with intra-arterial alteplase, mechanicalthrombectomy (MERCI device), or intra-arterial ultrasound(EKOS device)
• THRACE
– 480 patients
– Intravenous thrombolysis with full dose alteplase vs intravenousfull dose completed with mechanical thrombectomy (MERCI, PENUMBRA, SOLITAIRE, or CATCH) and intra-arterialalteplase
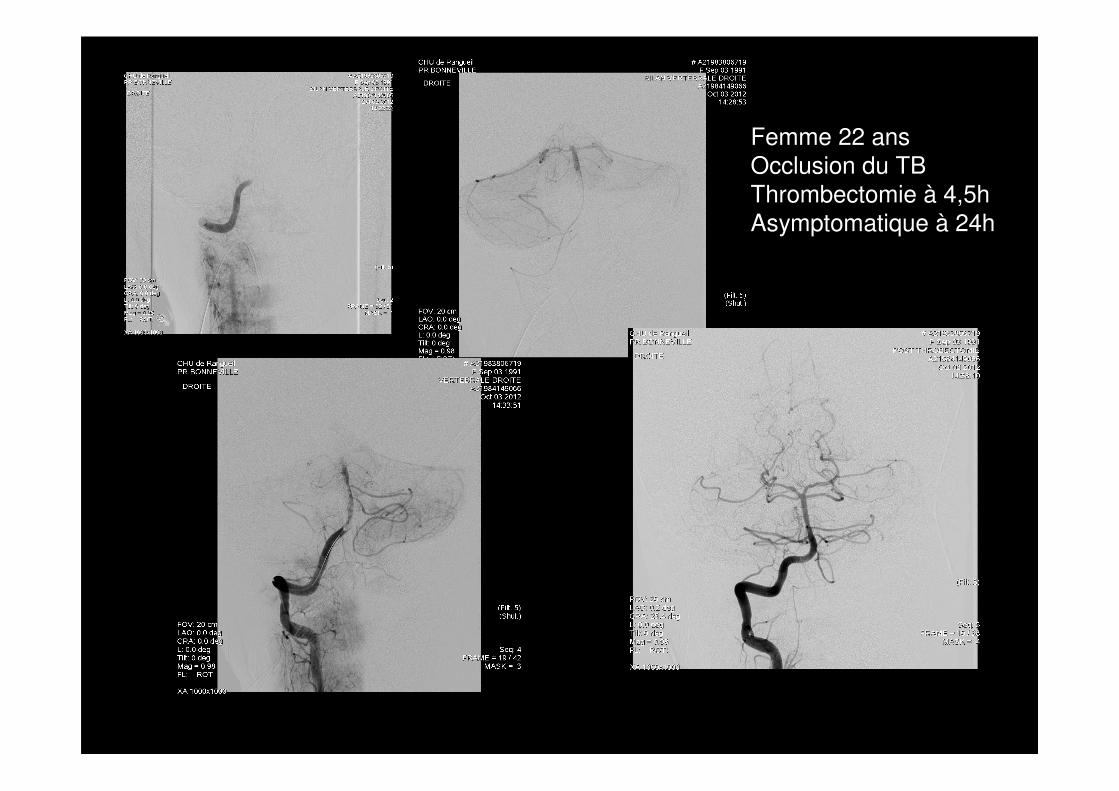
Femme 22 ansOcclusion du TB
Thrombectomie à 4,5h
Asymptomatique à 24h

Angioplastie à la phase aiguë
• Dans les occlusions thrombotiques
• Mauvais résultats dans les troncs basilaires
• A envisager dans les occlusions cervicales avec suppléances insuffisantes et aggravation clinique

Femme, 47 ans, hypertendue, tabagique, NIHSS=14
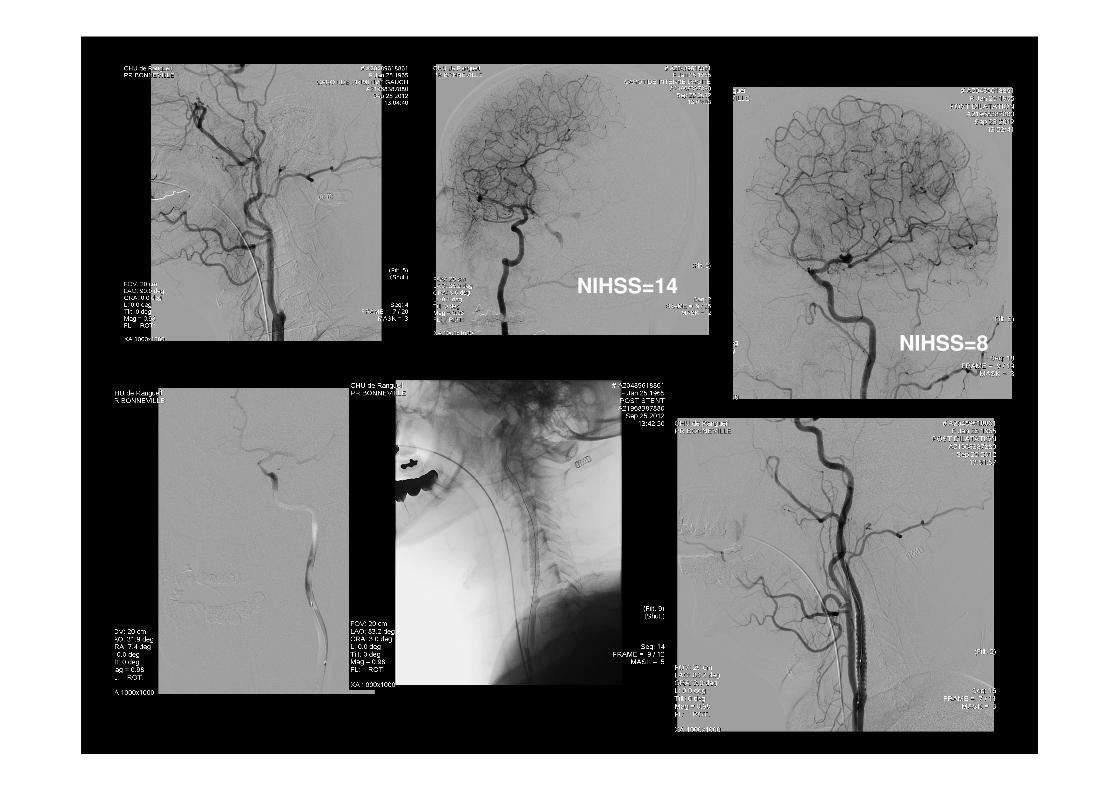
NIHSS=14
NIHSS=8
Traitement anticoagulant par héparine àdose curative
• Essais de phase 3 (AVC ischémiques non triés; patients en FA; AVC liés à athérome de grosse artère) tous négatifs: le bénéfice du traitement est annulé par les complications hémorragiques intra et extra-crâniennes
• Indications dans certains sous-groupes?
– Thrombus sur plaque
– Thrombus intracardiaque
– Dissection cervicale
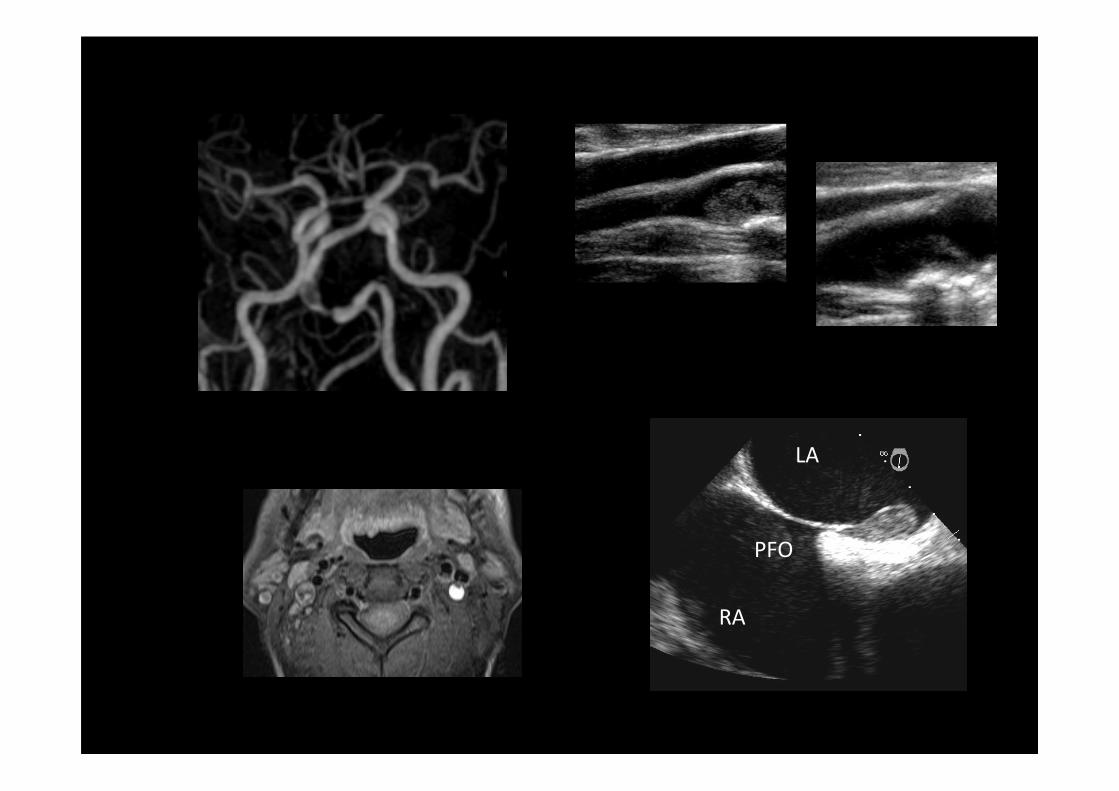
RA
PFO
LA

Traitements antiagrégants plaquettaires combinés
• Aspirine + clopidogrel
• Dans les AVC par athérome des gros troncs
• Rationnel (inhibition de l’activation plaquettaire par différentes voies de signalisation; faible efficacité de l’aspirine seule)
• Traitement de courte durée. L’association n’a pas d’efficacité au long cours par rapport à l’aspirine ou au clopidogrel en monothérapie
• Niveau de preuve intermédiaire
– Microembolisation en aval plaque carotide ou sylvienne est davantage inhibée par clopidogrel+aspirine que par l’aspirine seule (RCT: CARESS, CLAIR)
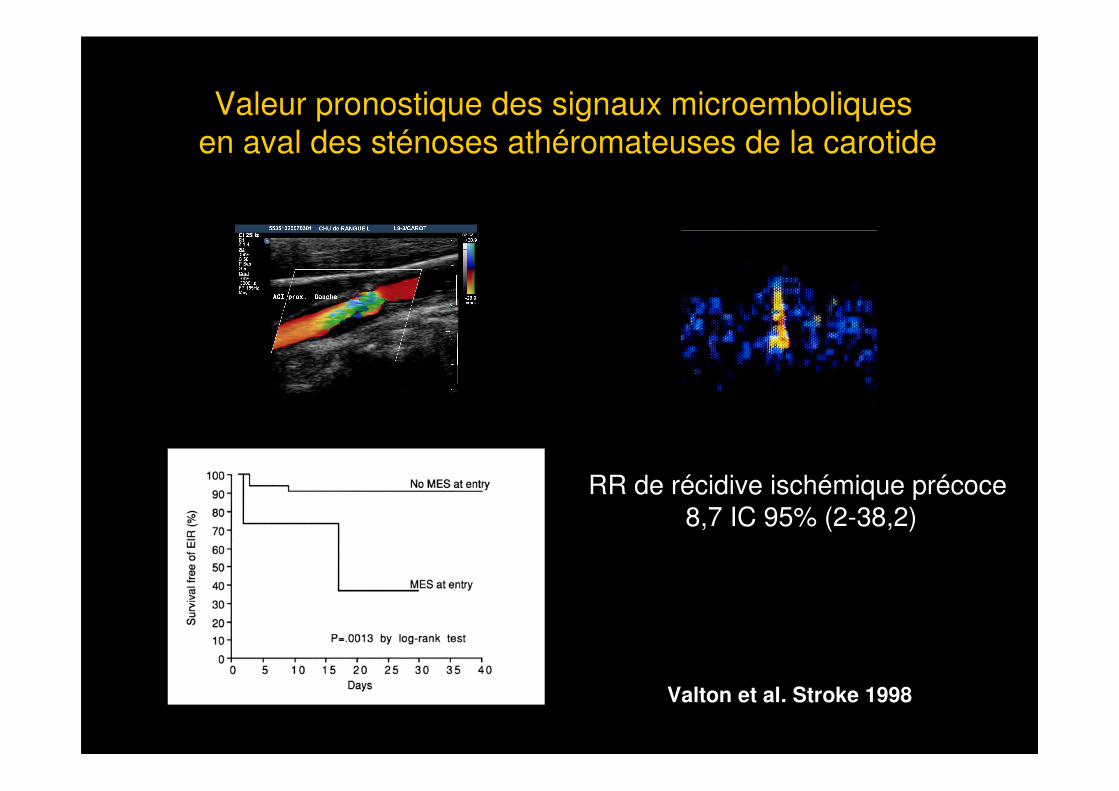
RR de récidive ischémique précoce8,7 IC 95% (2-38,2)
Valton et al. Stroke 1998
Valeur pronostique des signaux microemboliques
en aval des sténoses athéromateuses de la carotide
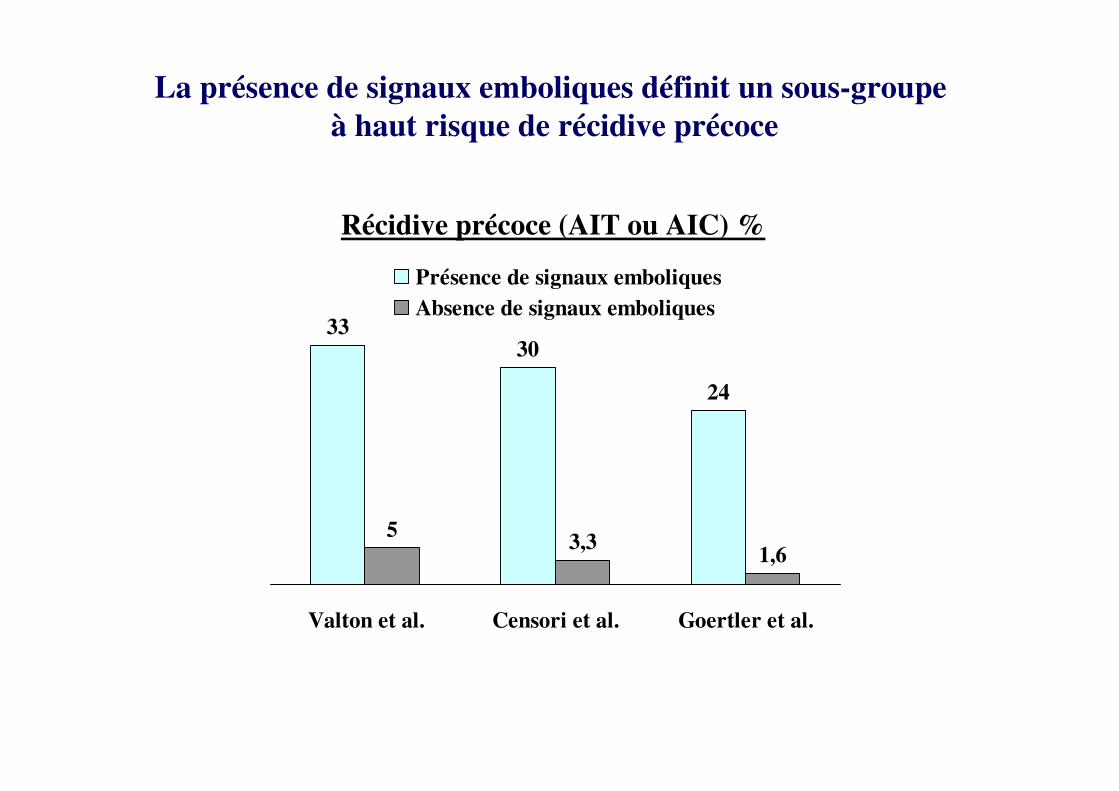
3330
24
53,3
1,6
Valton et al. Censori et al. Goertler et al.
Présence de signaux emboliques
Absence de signaux emboliques
Récidive précoce (AIT ou AIC) %
La présence de signaux emboliques définit un sous-groupe
à haut risque de récidive précoce
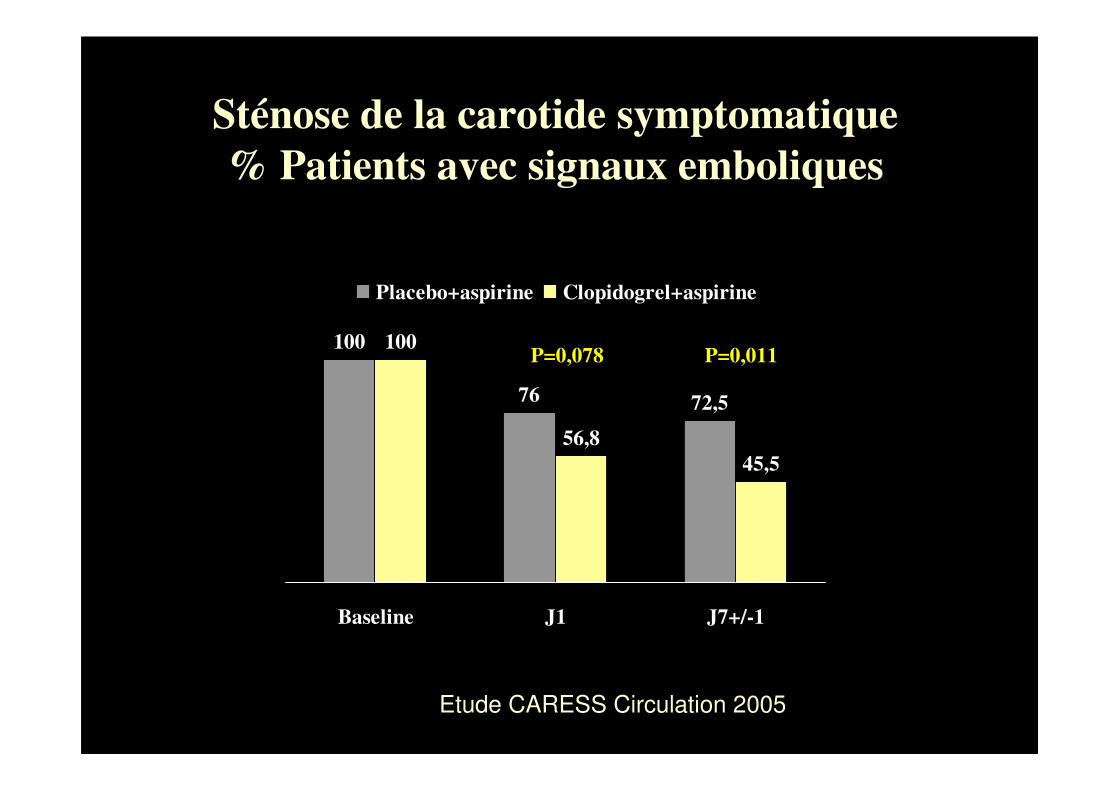
100
76 72,5
100
56,8
45,5
Baseline J1 J7+/-1
Placebo+aspirine Clopidogrel+aspirine
Sténose de la carotide symptomatique
% Patients avec signaux emboliques
P=0,078 P=0,011
Etude CARESS Circulation 2005
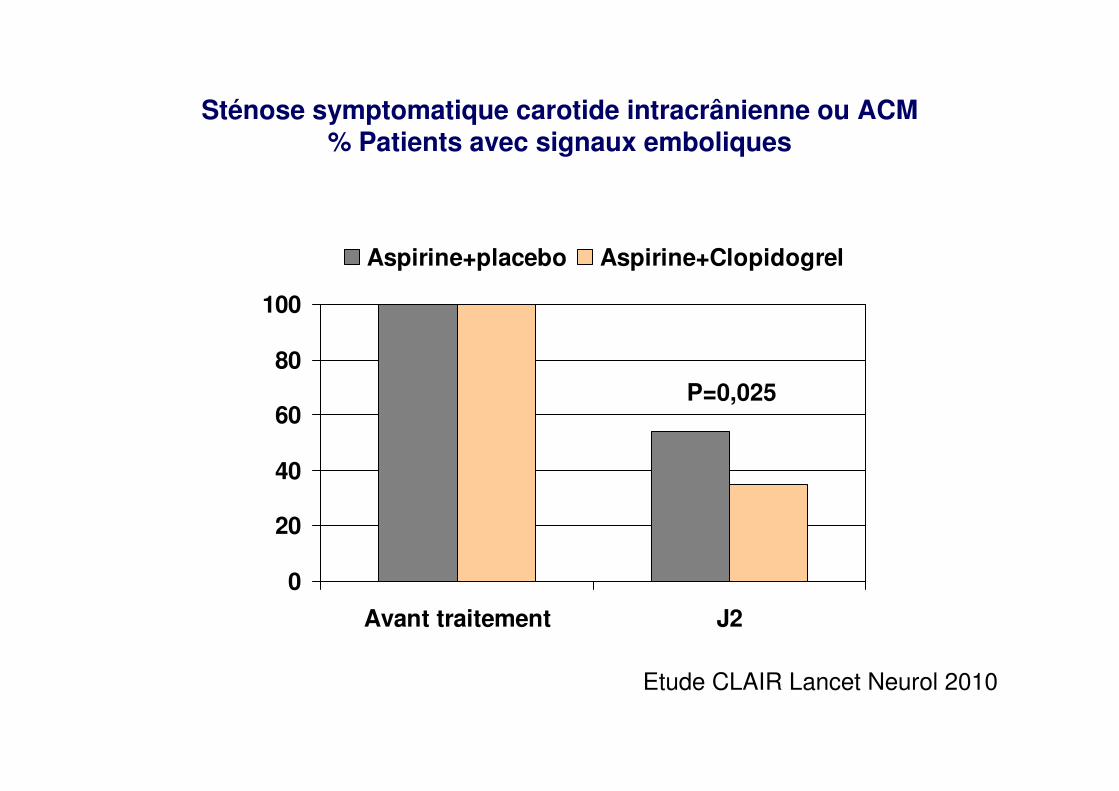
Sténose symptomatique carotide intracrânienne ou ACM% Patients avec signaux emboliques
0
20
40
60
80
100
Avant traitement J2
Aspirine+placebo Aspirine+Clopidogrel
Etude CLAIR Lancet Neurol 2010
P=0,025
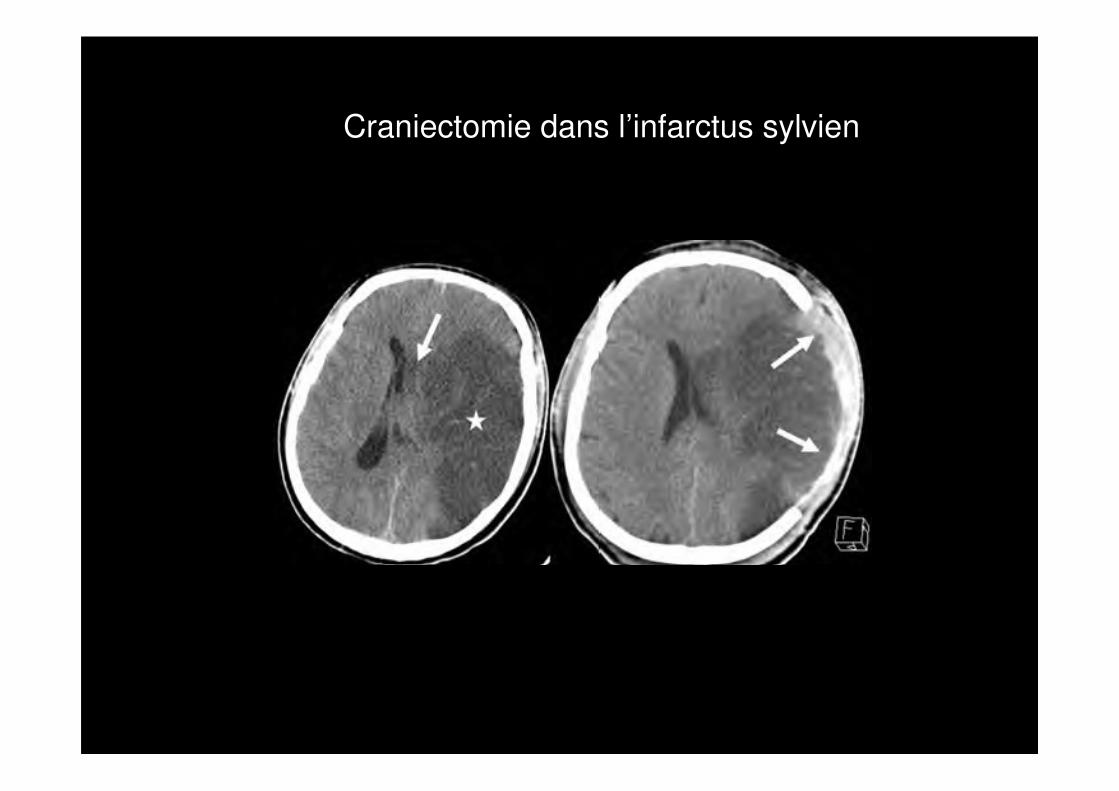
Craniectomie dans l’infarctus sylvien
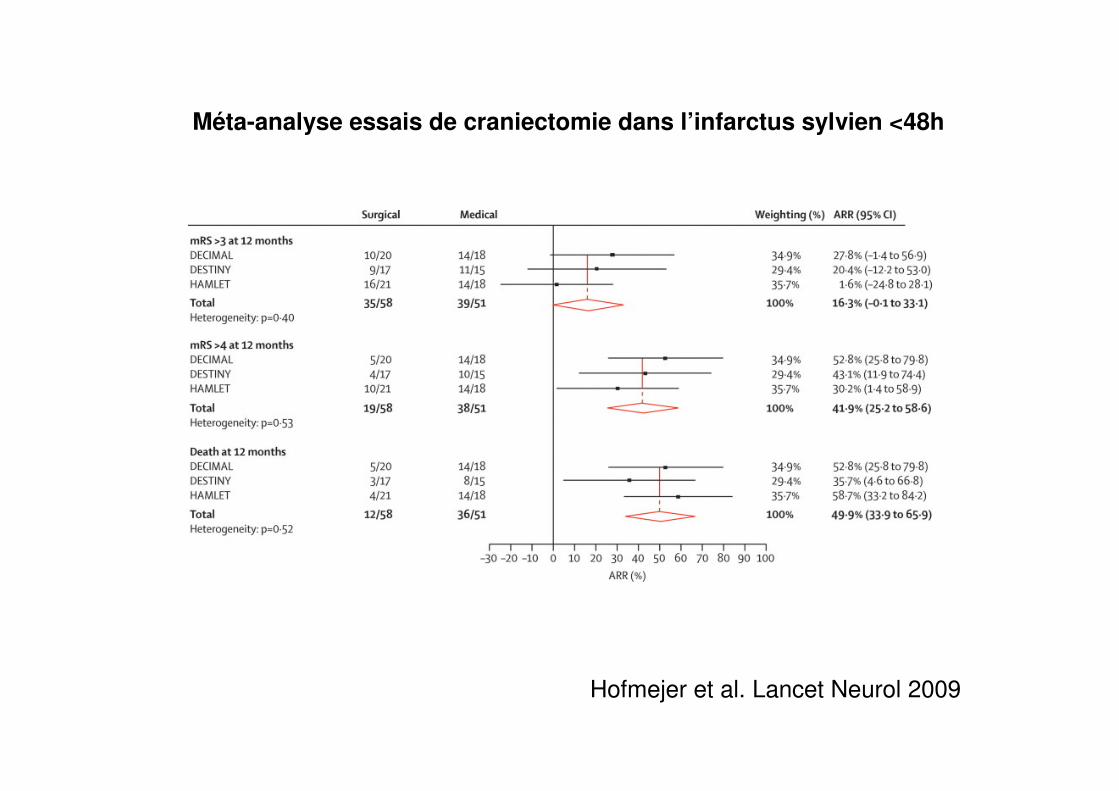
Méta-analyse essais de craniectomie dans l’infarctus sylvien <48h
Hofmejer et al. Lancet Neurol 2009
Craniectomie
• L’échelle de Rankin n’évalue pas les déficits cognitifs
• Qualité de vie?
• Discussion cas par cas avec entourage
• Délai d’intervention: asap (avant aggravation)
• Volume lésion (>145 cc en diffusion <14h, sensibilité 100%, spécificité 94% pour infarctus malin)
• Les RCT ont exclu les patients>60 ans

Sonothrombolyse
• Accélération de la thrombolyse enzymatique par application d’ultrasons (effets mécaniques des US sur le thrombus et àl’interface sang circulant/thrombus)
• Les ultrasons de basse fréquence sont beaucoup plus thrombolytiques que les ultrasons de haute fréquence mais ils entraînent des hémorragies intracrâniennes massives (TRUMBI)
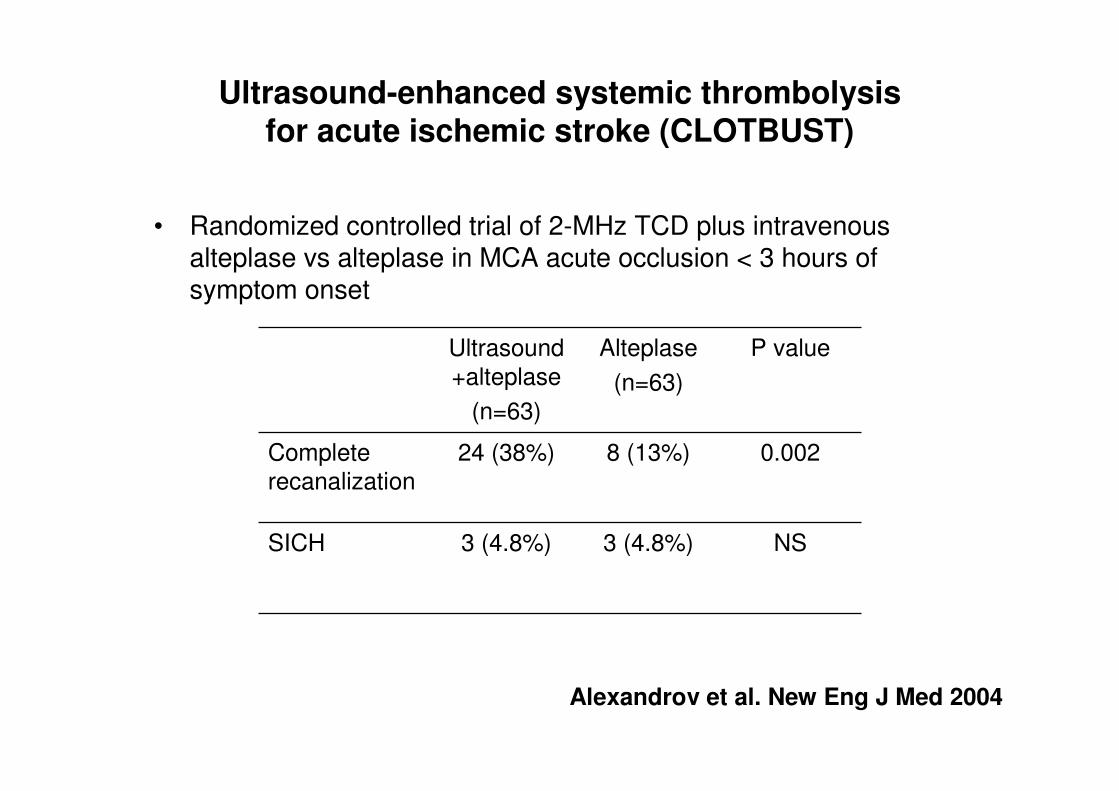
Ultrasound-enhanced systemic thrombolysisfor acute ischemic stroke (CLOTBUST)
• Randomized controlled trial of 2-MHz TCD plus intravenousalteplase vs alteplase in MCA acute occlusion < 3 hours of symptom onset
Ultrasound
+alteplase
(n=63)
Alteplase
(n=63)
P value
Complete
recanalization
24 (38%) 8 (13%) 0.002
SICH 3 (4.8%) 3 (4.8%) NS
Alexandrov et al. New Eng J Med 2004
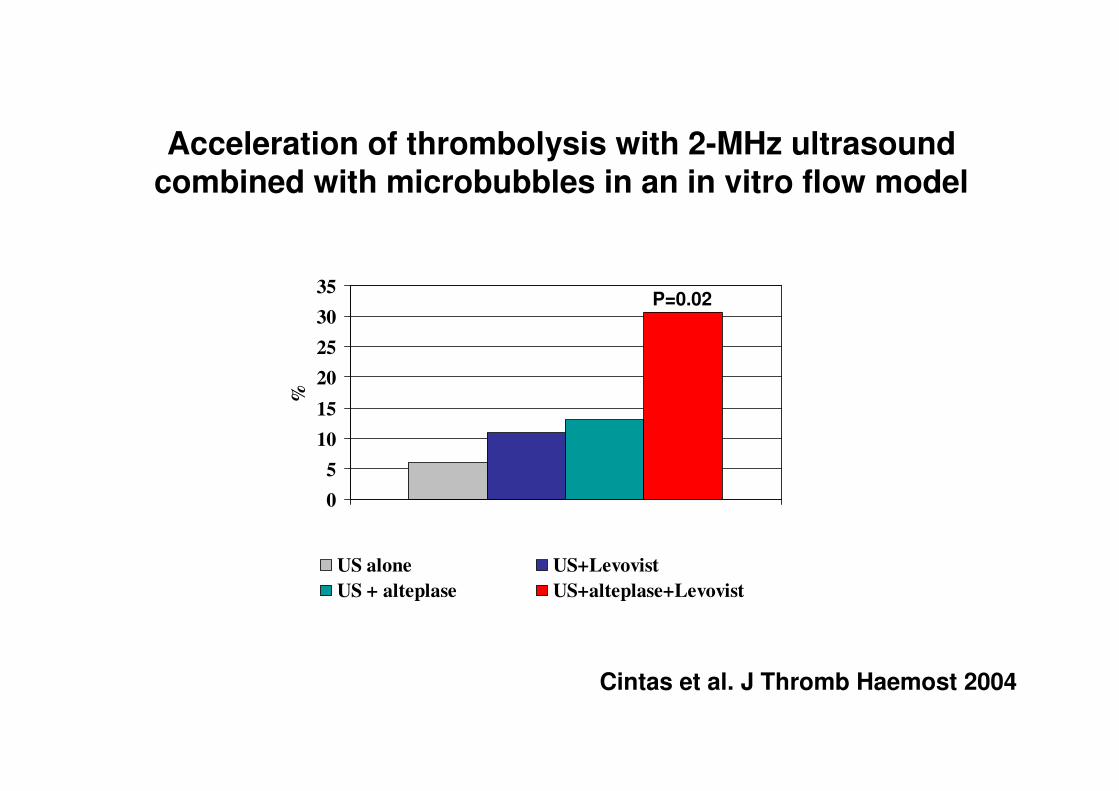
0
5
10
15
20
25
30
35%
US alone US+Levovist
US + alteplase US+alteplase+Levovist
Acceleration of thrombolysis with 2-MHz ultrasoundcombined with microbubbles in an in vitro flow model
Cintas et al. J Thromb Haemost 2004
P=0.02
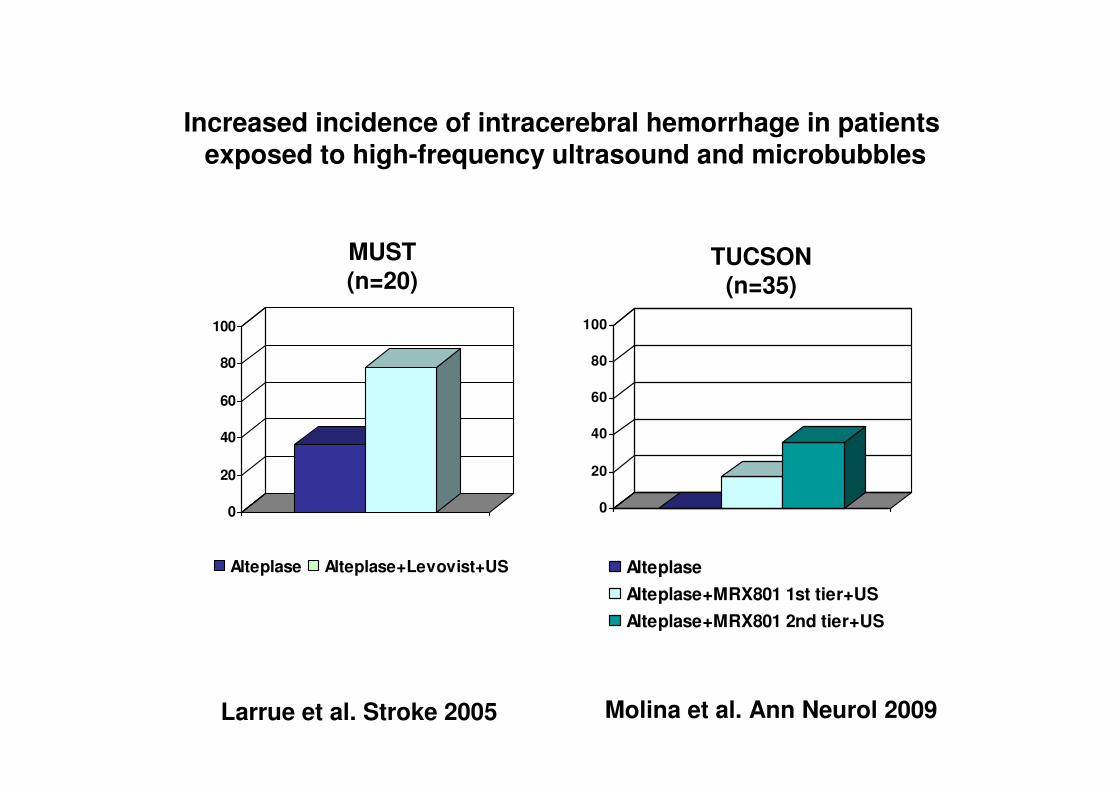
0
20
40
60
80
100
Alteplase Alteplase+Levovist+US
0
20
40
60
80
100
Alteplase
Alteplase+MRX801 1st tier+US
Alteplase+MRX801 2nd tier+US
Larrue et al. Stroke 2005 Molina et al. Ann Neurol 2009
MUST(n=20)
TUCSON(n=35)
Increased incidence of intracerebral hemorrhage in patients exposed to high-frequency ultrasound and microbubbles
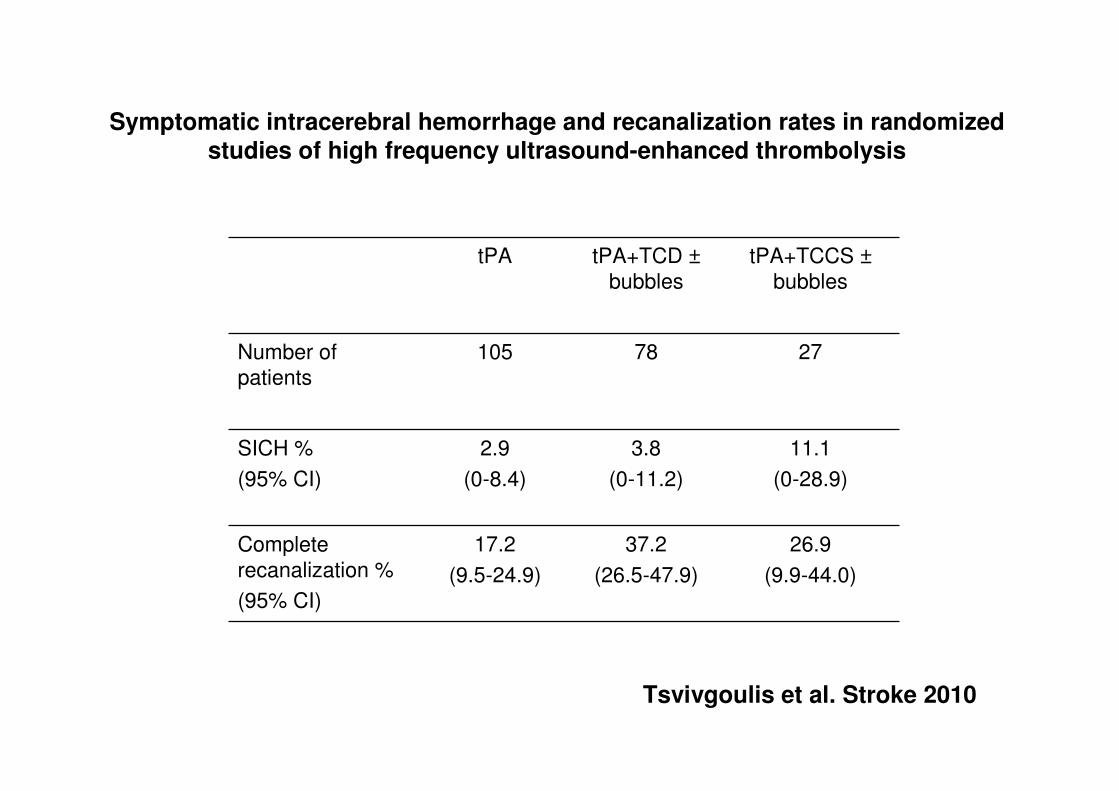
Symptomatic intracerebral hemorrhage and recanalization rates in randomizedstudies of high frequency ultrasound-enhanced thrombolysis
tPA tPA+TCD ±
bubbles
tPA+TCCS ±
bubbles
Number of
patients
105 78 27
SICH %
(95% CI)
2.9
(0-8.4)
3.8
(0-11.2)
11.1
(0-28.9)
Complete
recanalization %
(95% CI)
17.2
(9.5-24.9)
37.2
(26.5-47.9)
26.9
(9.9-44.0)
Tsvivgoulis et al. Stroke 2010

Conclusion
• Transformation en cours de la prise en charge des AVC ischémiques à la phase aiguë
• Les UNV sont en place, la fibrinolyse intraveineuse est utilisée en routine
• La thrombectomie est, de toute évidence, très efficace chez certains malades. Ses indications sont à préciser par des études de phase 3 bien conçues
• L’utilisation généralisée de la thrombectomie en pratique quotidienne supposerait une réorganisation profonde de l’offre de soins.