inotropes & inodilatateurs - cemir · inotropes & inodilatateurs ... epi/ne/dopa pirracchio...
TRANSCRIPT
Inotropes & Inodilatateurs
Alexandre Mebazaa Département d’Anesthésie-Réanimation
Hôpitaux Universitaires Saint Louis – Lariboisière
Université Paris 7; INSERM – UMR 942
Inotropes and inodilatateurs
• Ils sont encore TROP utilisés en France et
dans le monde
• Ils ne doivent être utilisés que quand il y a
des signes patents de baisse de la
perfusion
• Leur durée d’utilisation doit être courte
Cecconi et al Intensive Care Medicine, 2014
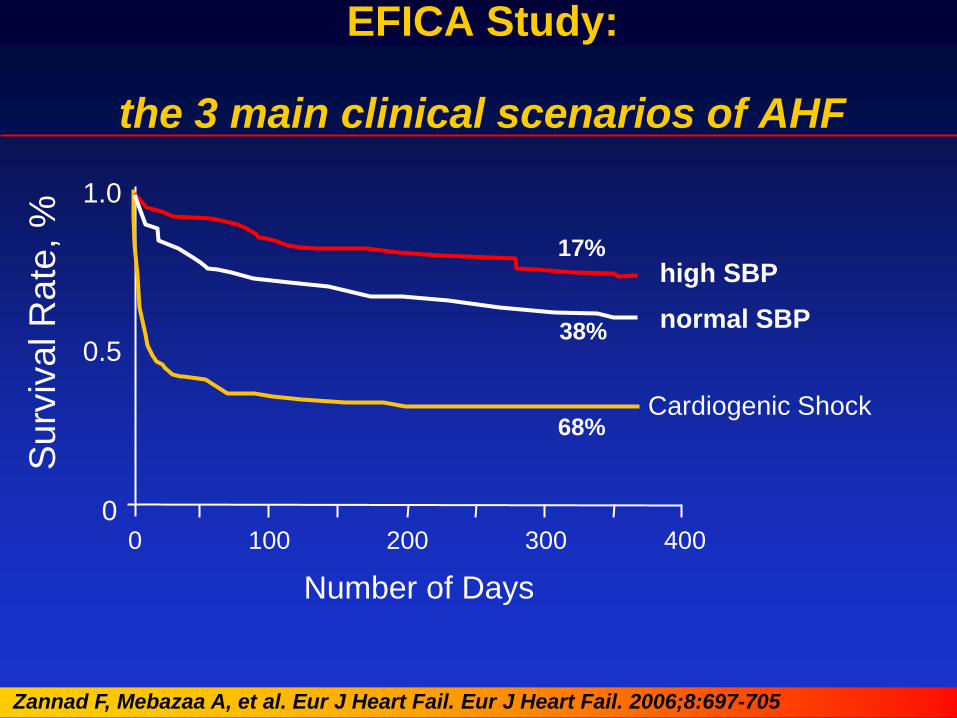
0
0.5
1.0
0 100 200 300 400
normal SBP
high SBP
Cardiogenic Shock
Number of Days
Surv
ival R
ate
, %
68%
38%
17%
EFICA Study:
the 3 main clinical scenarios of AHF
Zannad F, Mebazaa A, et al. Eur J Heart Fail. Eur J Heart Fail. 2006;8:697-705
Mistakes we did for years concerning the use of catecholamines
Acute heart failure: we did not explain well enough that AHF is about CONGESTION and rarely low cardiac output (CO)
Catecholamines: we did not insist on « low CO » beeing the only indication of catecholamines
Cardiogenic shock: we only looked at short-term effect of catecholamines and missed long-term effects
What we should learn today
« Tailored » therapy: restrict the use of catecholamines to patients with low CO
New inotropic agents:
– Need of short & long term beneficial effect
– Myocardial protection
VP Harjola et al, Eur J Heart Failure 2015
CardShock Study (clinicaltrials.gov NCT01374867)
Principal investigator
Veli-Pekka Harjola
Harjiola VP et al, EJHF in press 2015
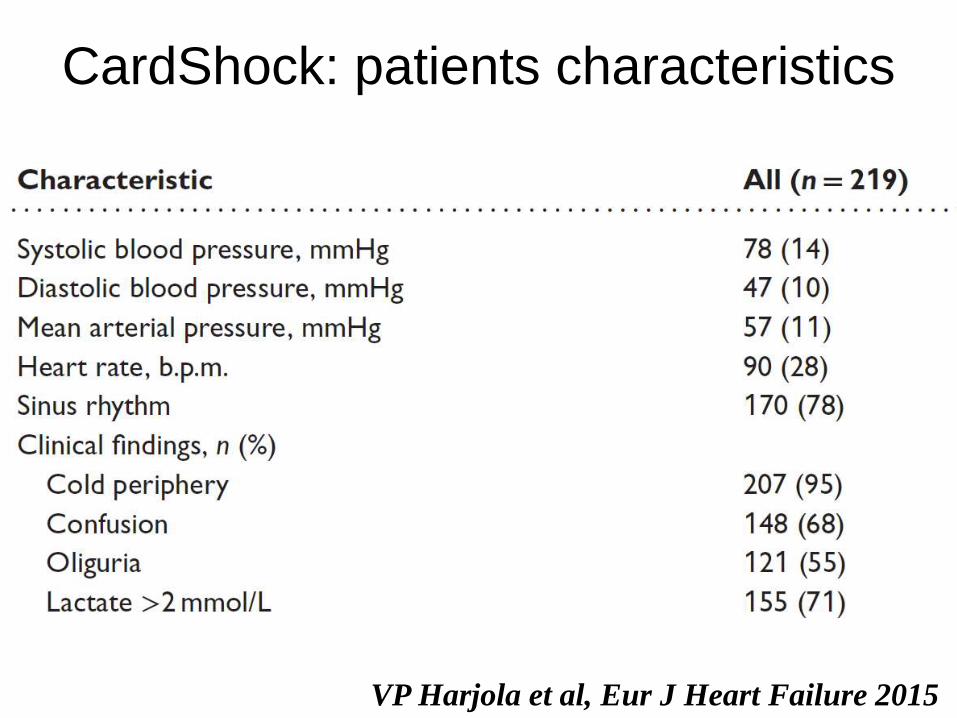
CardShock: patients characteristics
VP Harjola et al, Eur J Heart Failure 2015
Crit Care Medicine 2013
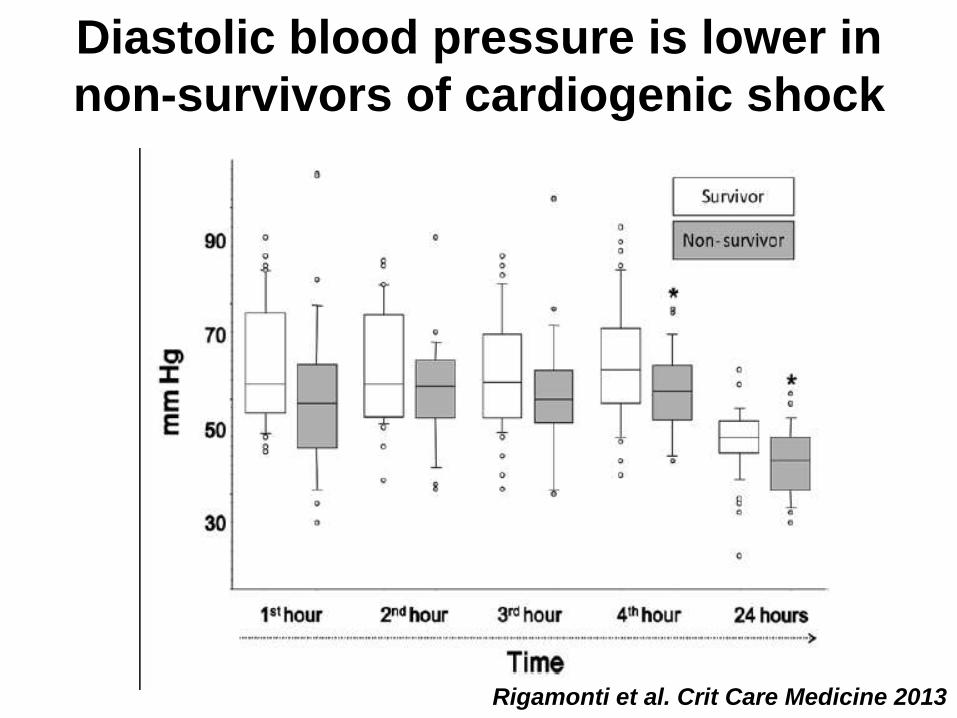
Diastolic blood pressure is lower in
non-survivors of cardiogenic shock
Rigamonti et al. Crit Care Medicine 2013
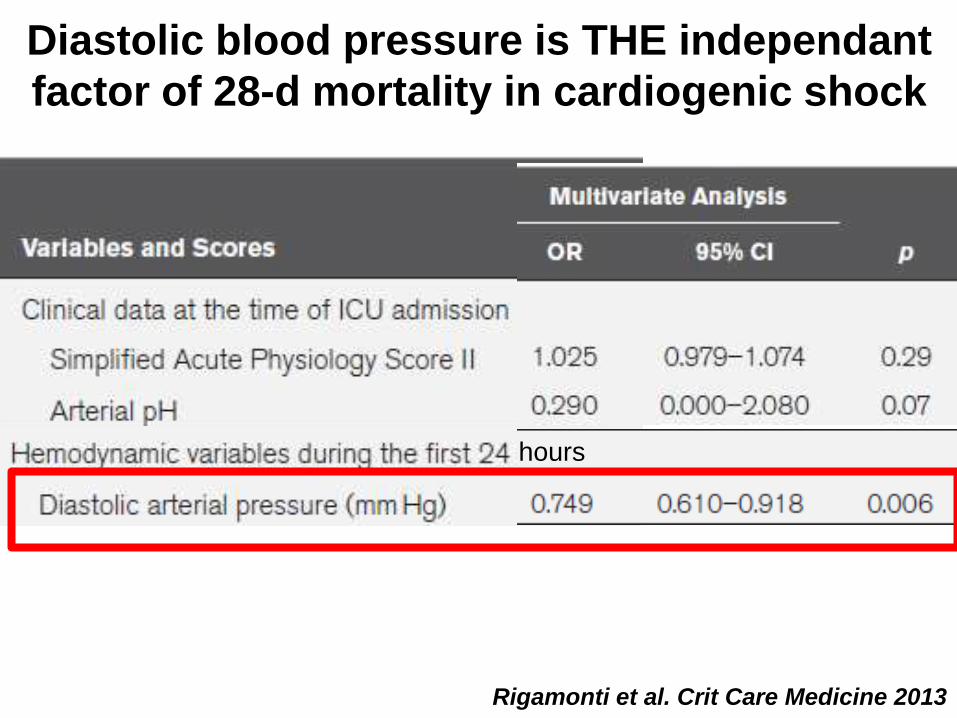
hours
Diastolic blood pressure is THE independant
factor of 28-d mortality in cardiogenic shock
Rigamonti et al. Crit Care Medicine 2013
Arrigo M & Mebazaa A, Intensive Care Medicine, in press 2015
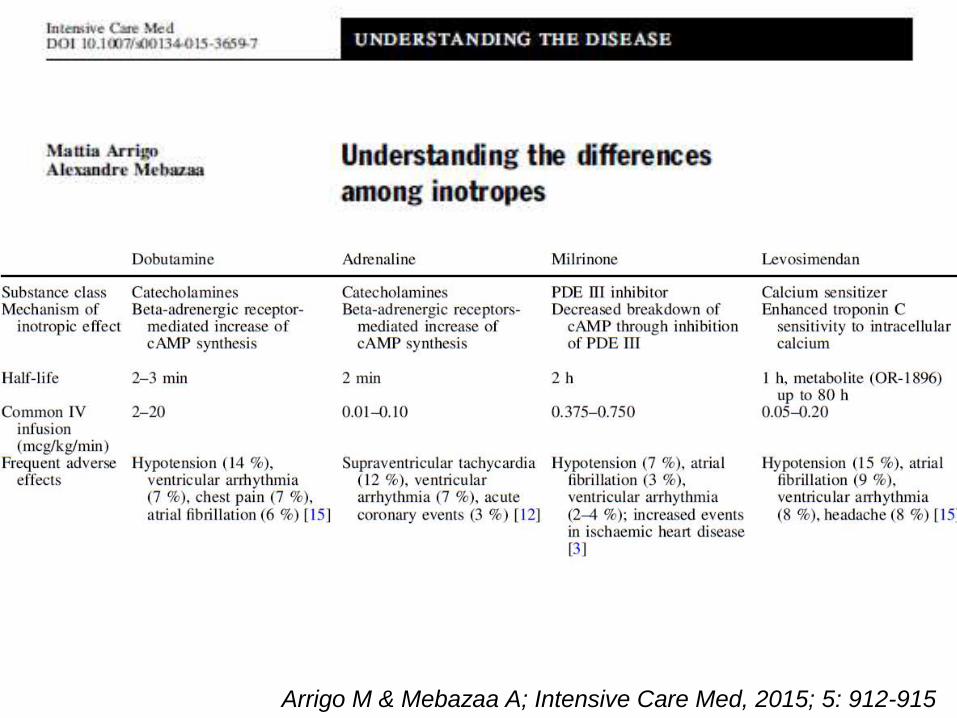
Arrigo M & Mebazaa A; Intensive Care Med, 2015; 5: 912-915
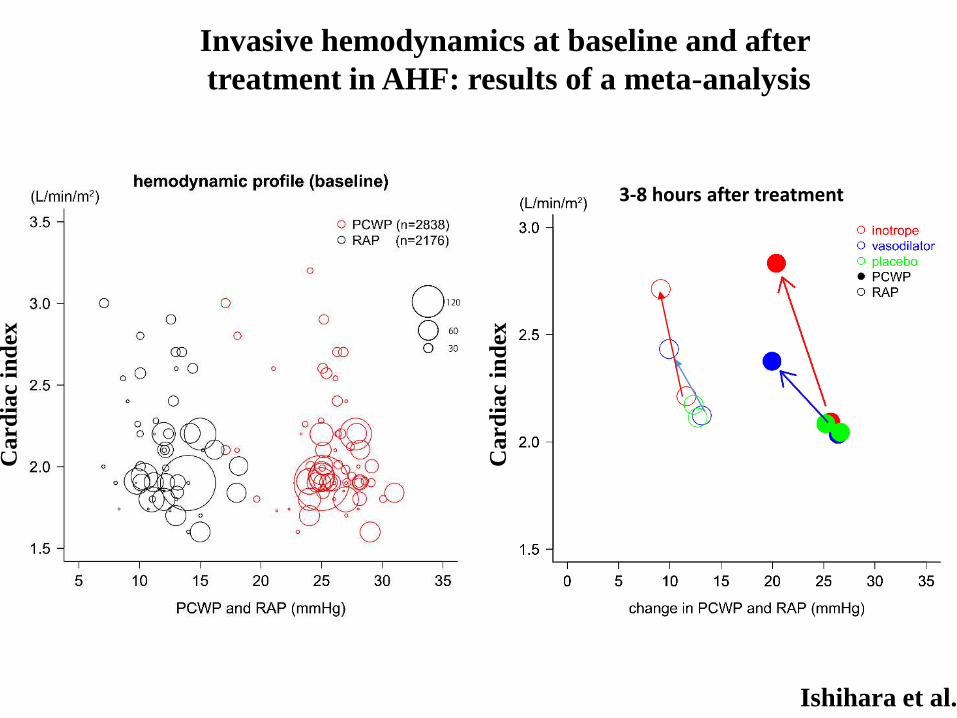
Ishihara et al.
Invasive hemodynamics at baseline and after
treatment in AHF: results of a meta-analysis
Card
iac i
nd
ex
3-8 hours after treatment
Card
iac i
nd
ex
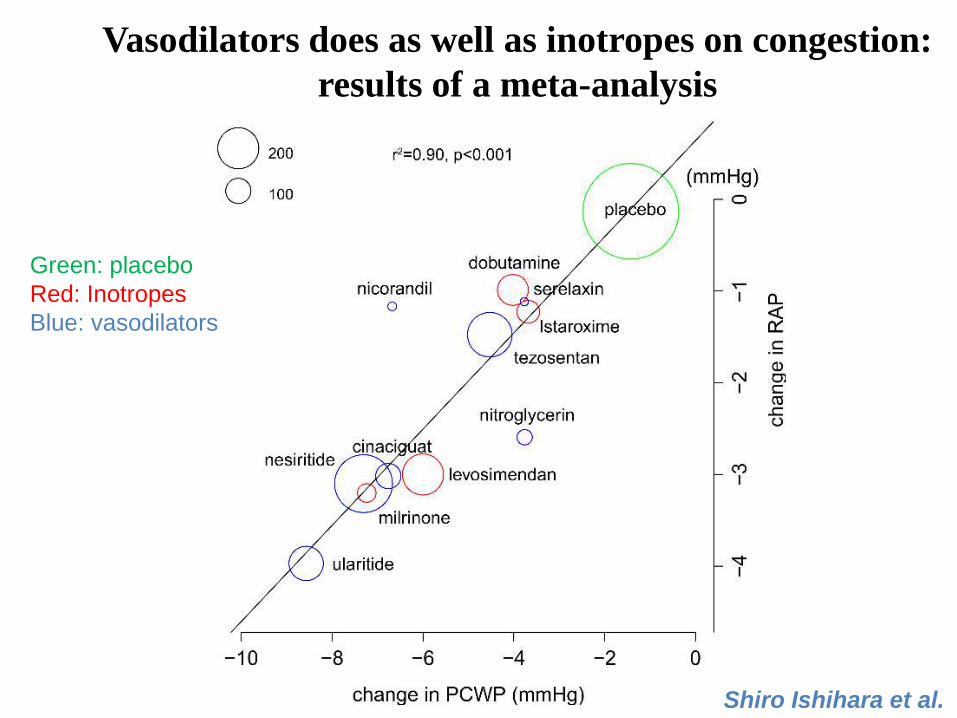
Shiro Ishihara et al.
Vasodilators does as well as inotropes on congestion:
results of a meta-analysis
Green: placebo
Red: Inotropes
Blue: vasodilators
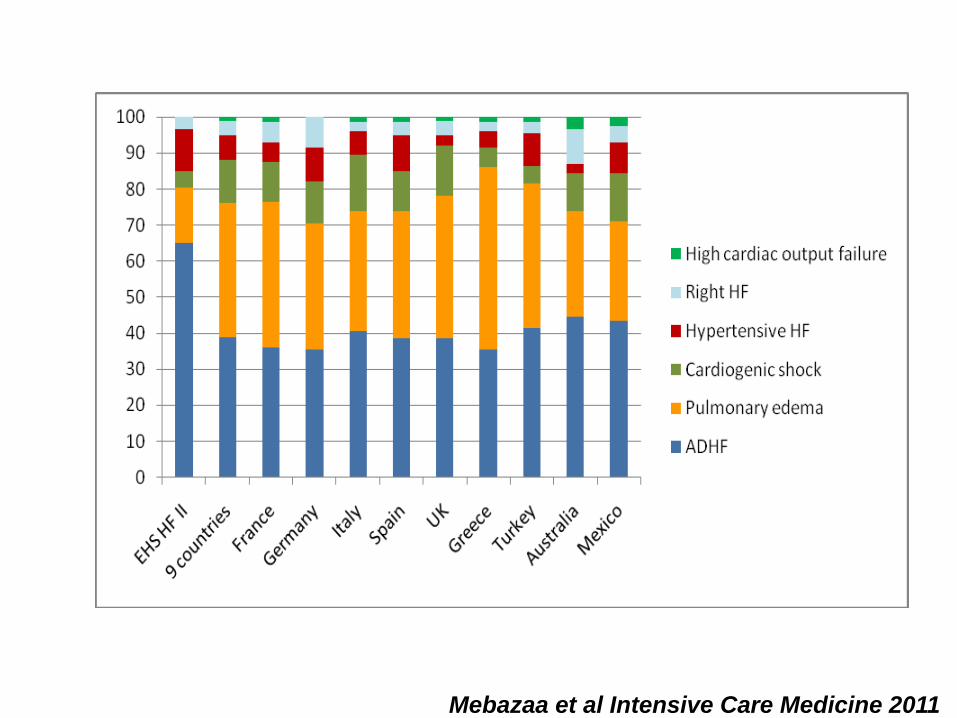
Mebazaa et al Intensive Care Medicine 2011
Mebazaa et al Intensive Care Medicine 2011
inotropes
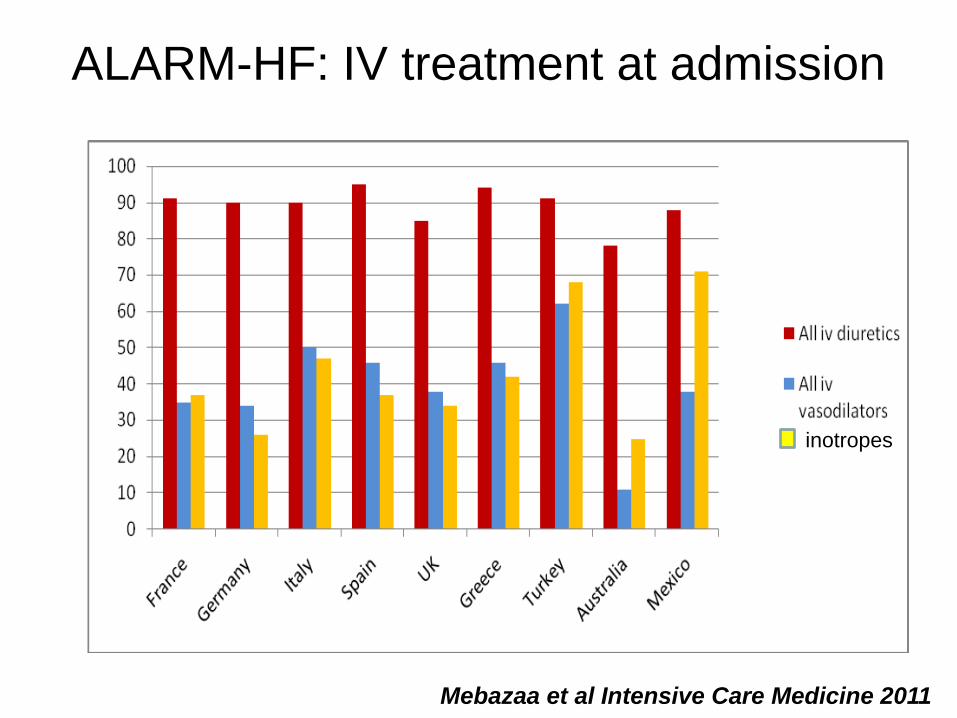
ALARM-HF: IV treatment at admission
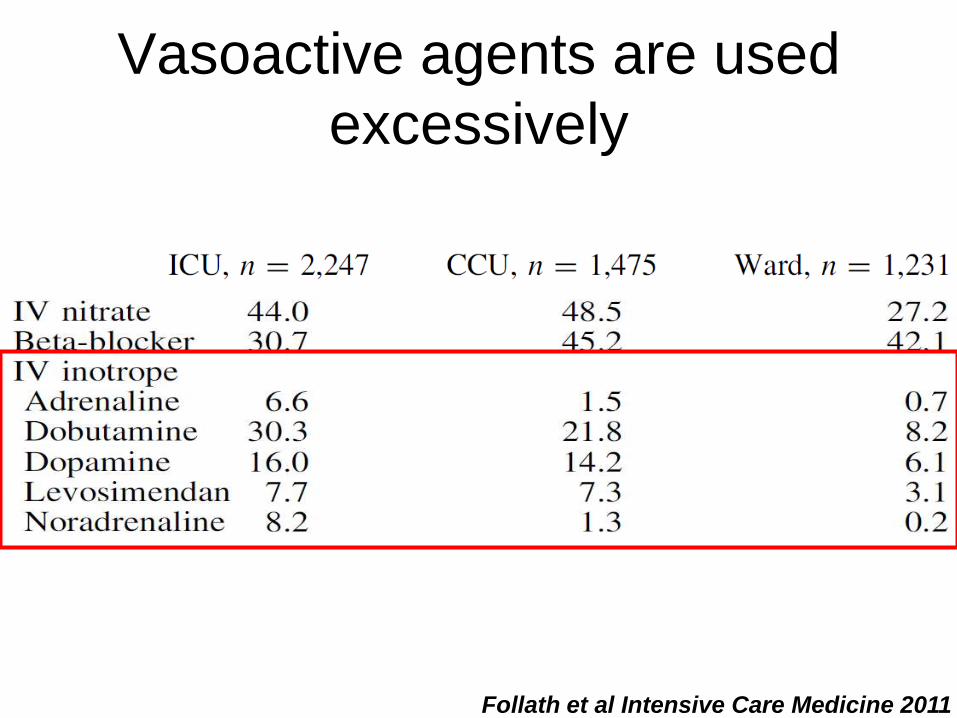
Vasoactive agents are used
excessively
Follath et al Intensive Care Medicine 2011
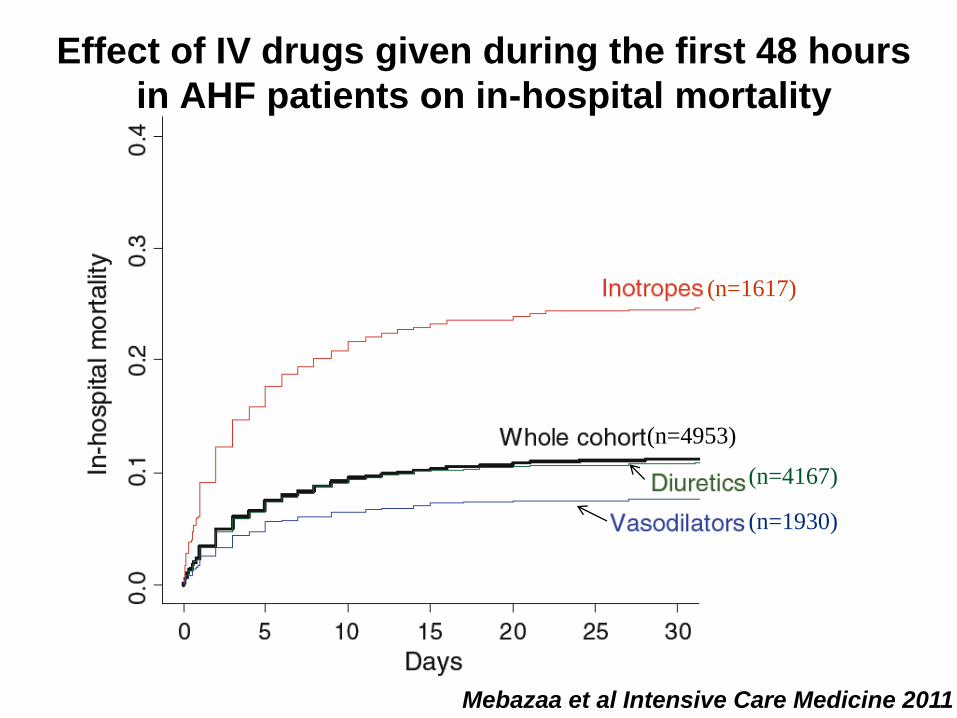
(n=4953)
(n=4167)
(n=1930)
(n=1617)
Effect of IV drugs given during the first 48 hours
in AHF patients on in-hospital mortality
Mebazaa et al Intensive Care Medicine 2011
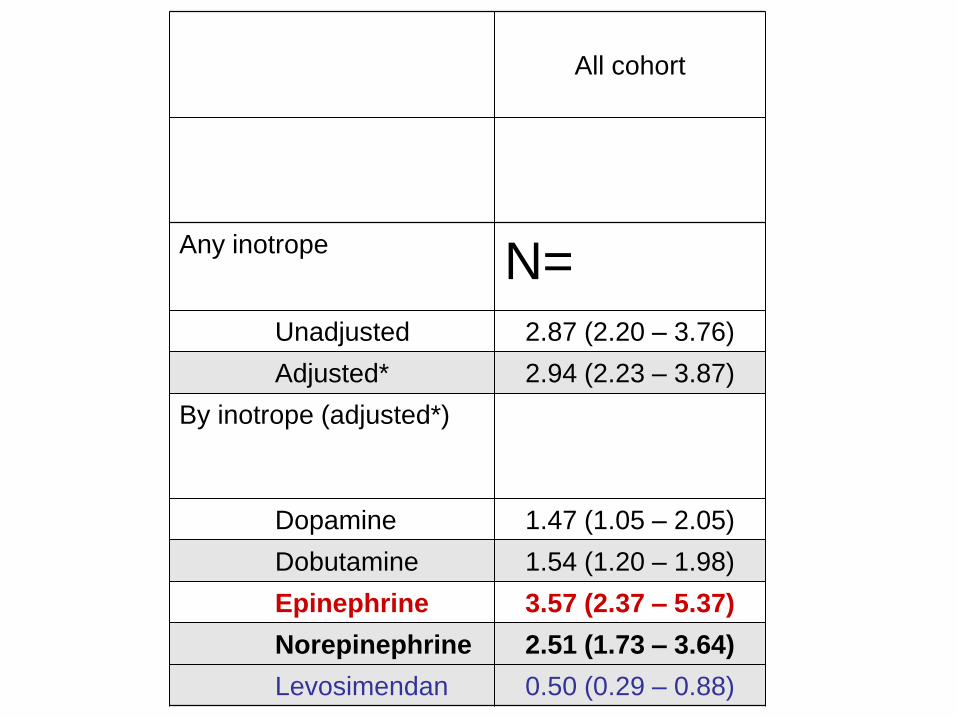
All cohort
Any inotrope N=
Unadjusted 2.87 (2.20 – 3.76)
Adjusted* 2.94 (2.23 – 3.87)
By inotrope (adjusted*)
Dopamine 1.47 (1.05 – 2.05)
Dobutamine 1.54 (1.20 – 1.98)
Epinephrine 3.57 (2.37 – 5.37)
Norepinephrine 2.51 (1.73 – 3.64)
Levosimendan 0.50 (0.29 – 0.88)
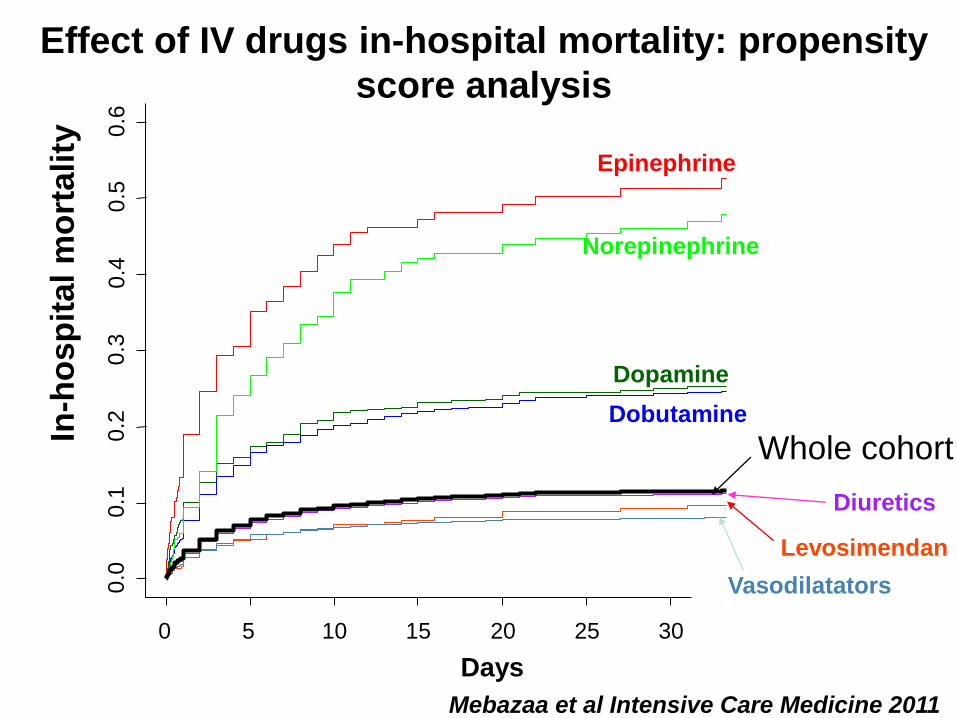
0 5 10 15 20 25 30
0.0
0
.1
0.2
0
.3
0.4
0
.5
0.6
Days
In-h
osp
ital
mo
rtality
Whole cohort
Dopamine
Dobutamine
Epinephrine
Norepinephrine
Levosimendan
Diuretics
Vasodilatators
Mebazaa et al Intensive Care Medicine 2011
Effect of IV drugs in-hospital mortality: propensity
score analysis
An Investigator-initiated European
Multicenter Study on Cardiogenic Shock
CardShock Study
clinicaltrials.gov NCT01374867
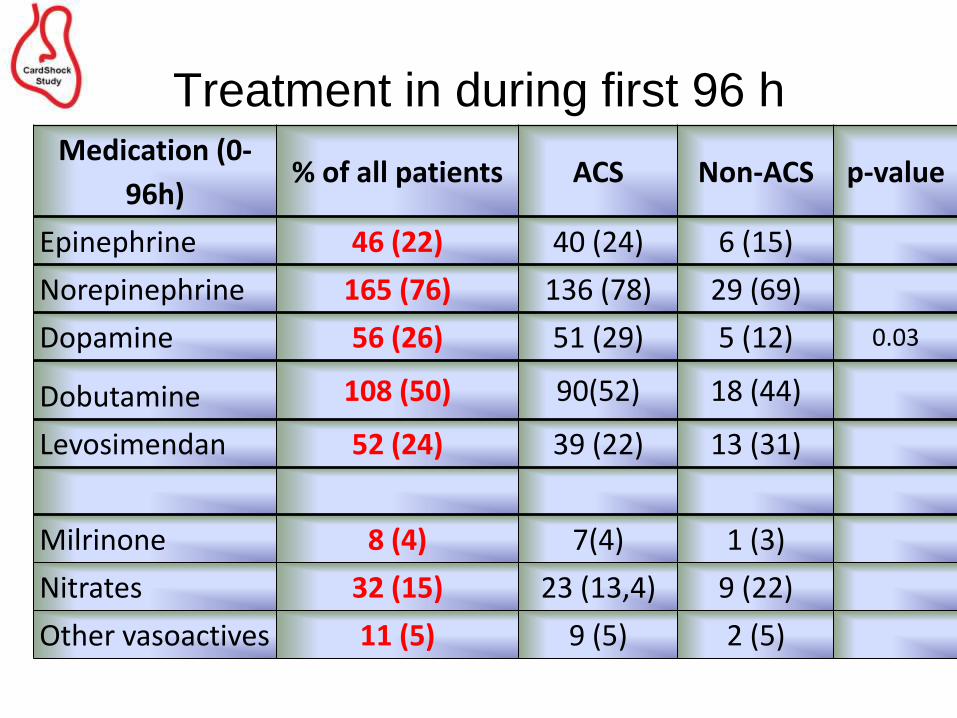
Treatment in during first 96 h Medication (0-
96h) % of all patients ACS Non-ACS p-value
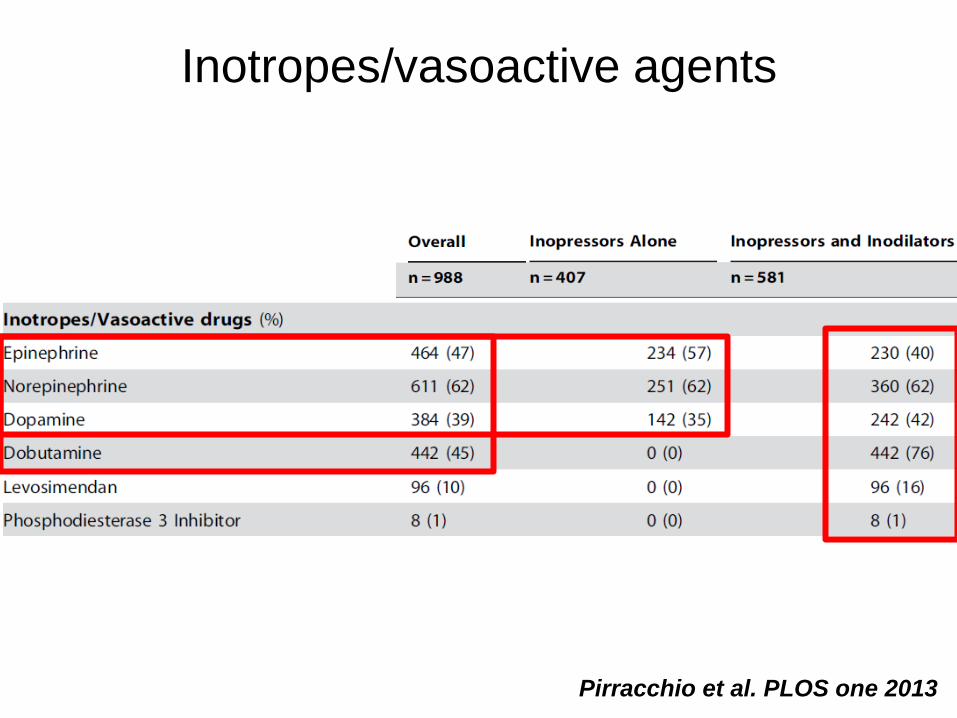
Epinephrine 46 (22) 40 (24) 6 (15)
Norepinephrine 165 (76) 136 (78) 29 (69)
Dopamine 56 (26) 51 (29) 5 (12) 0.03
Dobutamine 108 (50) 90(52) 18 (44)
Levosimendan 52 (24) 39 (22) 13 (31)
Milrinone 8 (4) 7(4) 1 (3)
Nitrates 32 (15) 23 (13,4) 9 (22)
Other vasoactives 11 (5) 9 (5) 2 (5)
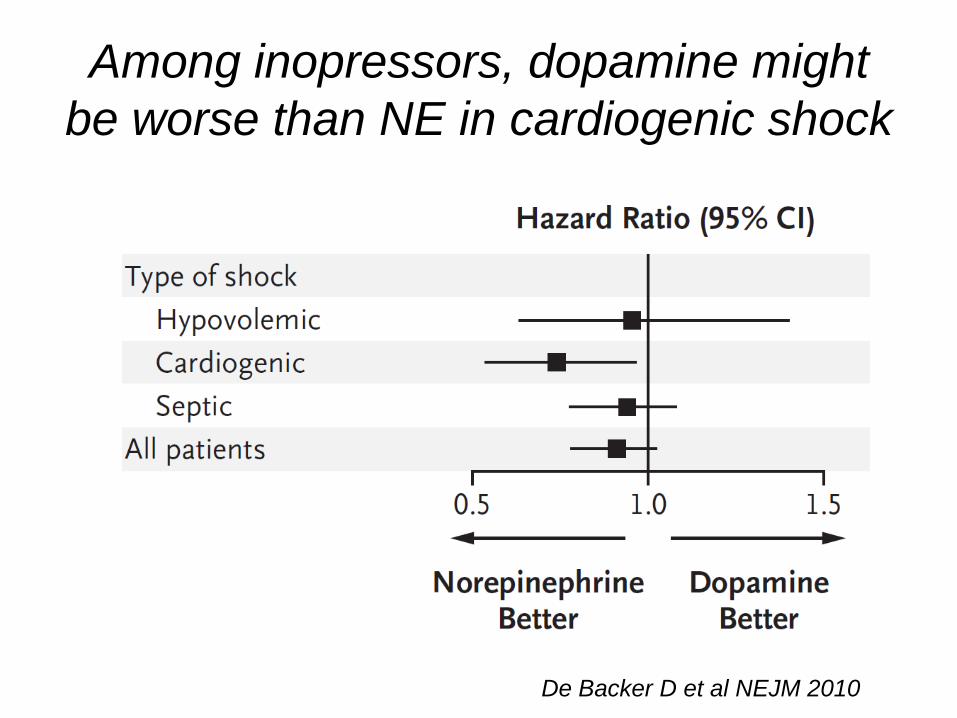
Among inopressors, dopamine might
be worse than NE in cardiogenic shock
De Backer D et al NEJM 2010
Pirracchio et al. PLOS one 2013
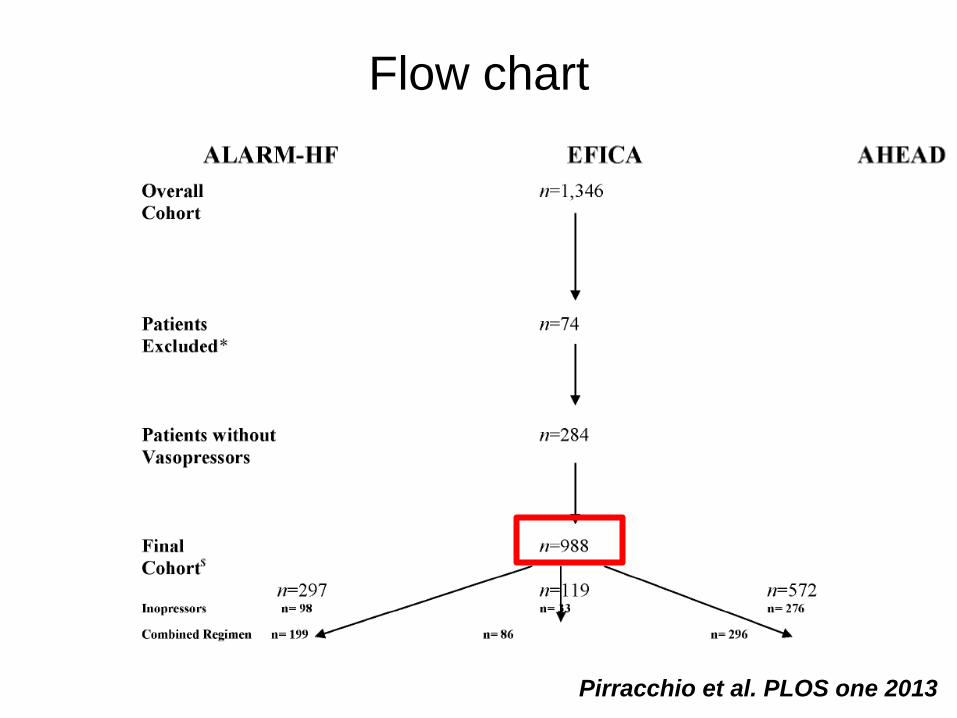
Flow chart
Pirracchio et al. PLOS one 2013
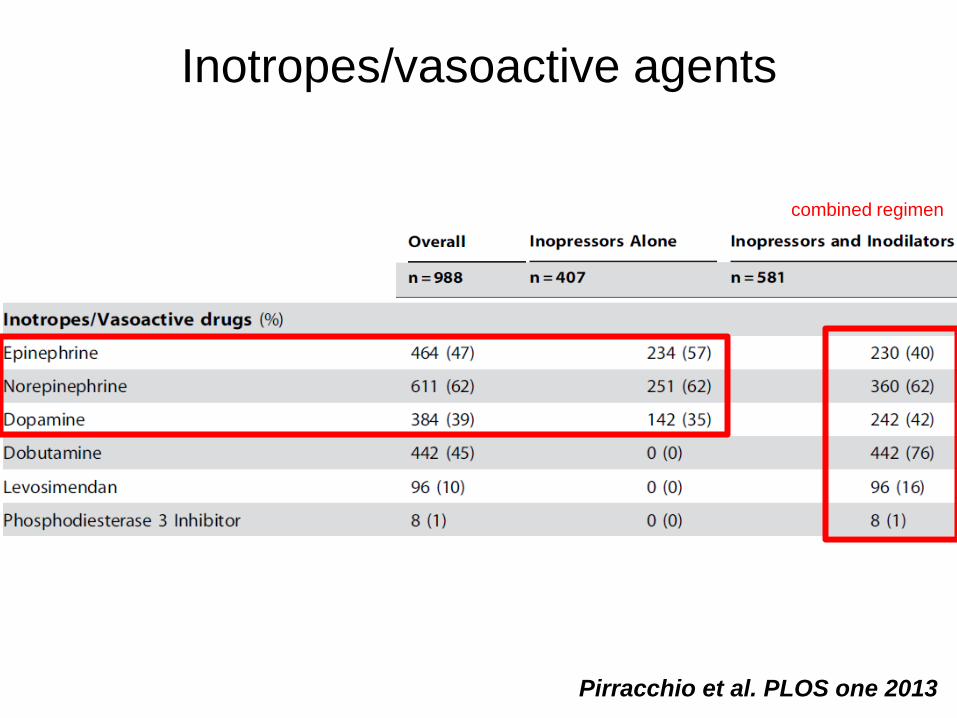
Inotropes/vasoactive agents
Pirracchio et al. PLOS one 2013
combined regimen
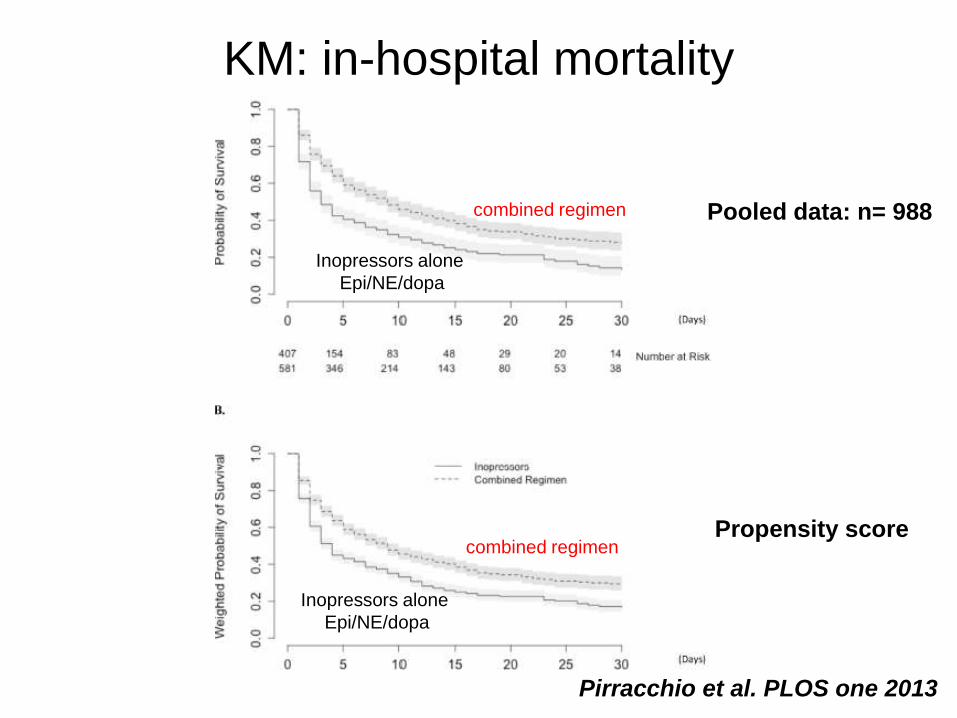
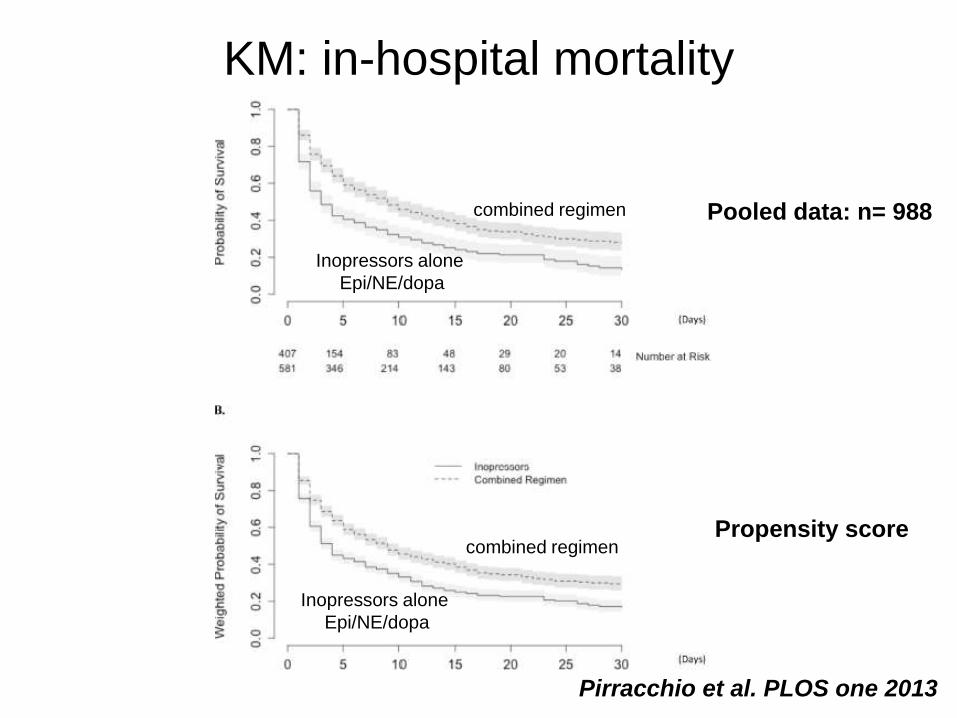
KM: in-hospital mortality
Pooled data: n= 988
Propensity score
combined regimen
Inopressors alone
Epi/NE/dopa
combined regimen
Inopressors alone
Epi/NE/dopa
Pirracchio et al. PLOS one 2013
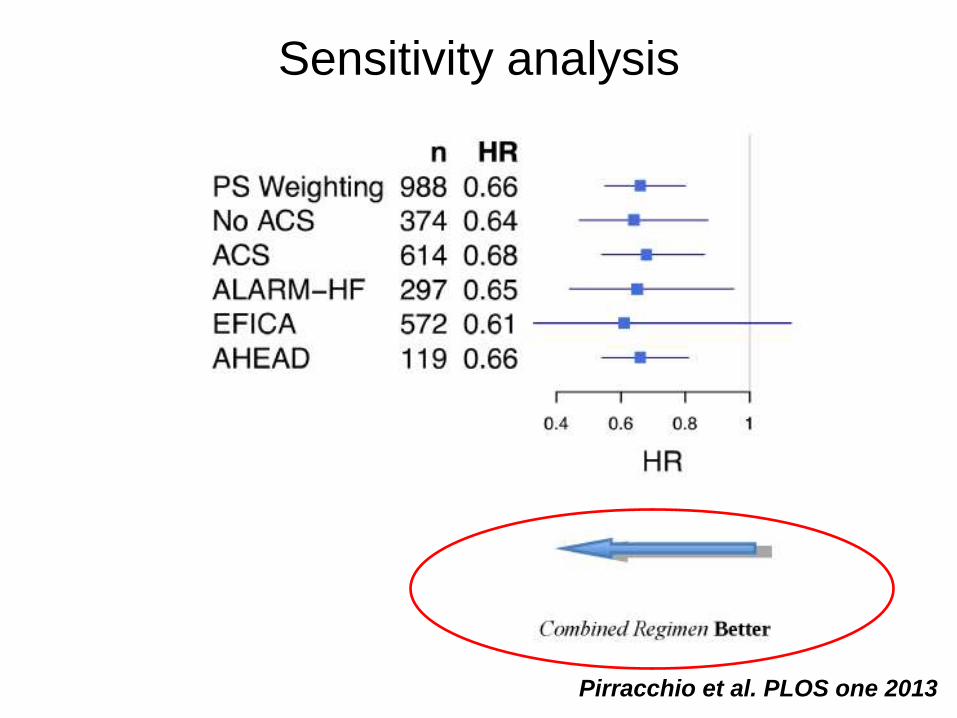
Sensitivity analysis
Pirracchio et al. PLOS one 2013
In summary
• We should better use the current agents in
cardiogenic shock:
less vasopressors alone, patient should
not only be managed with the objective to
improve blood pressure
• We need new inotropic agents that are
– active on both systolic and diastolic function
– much safer
– With a benefical long term effect
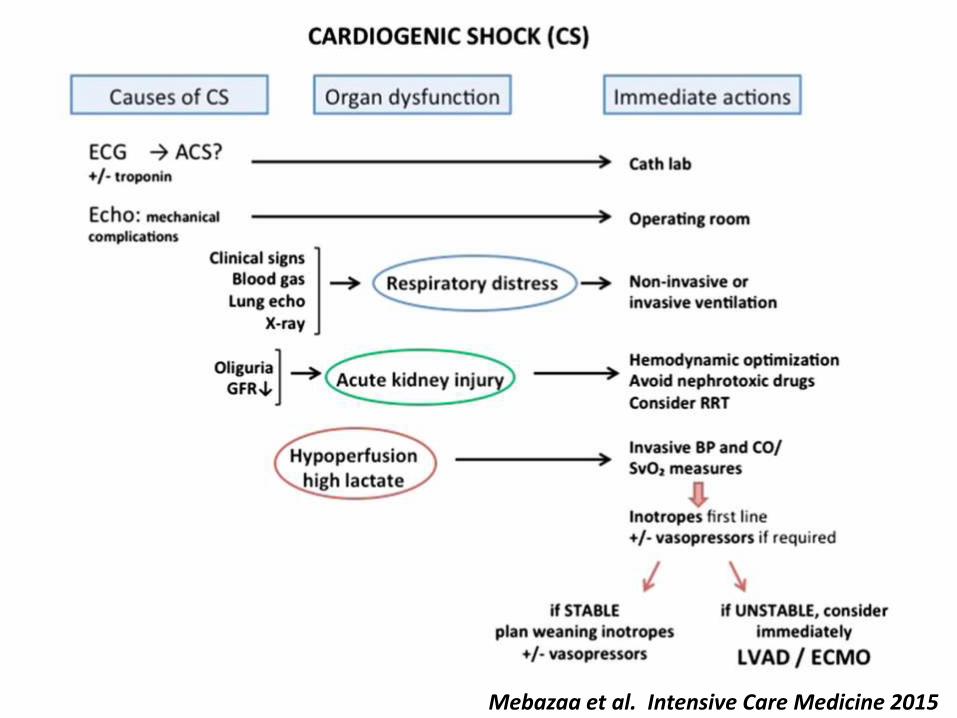
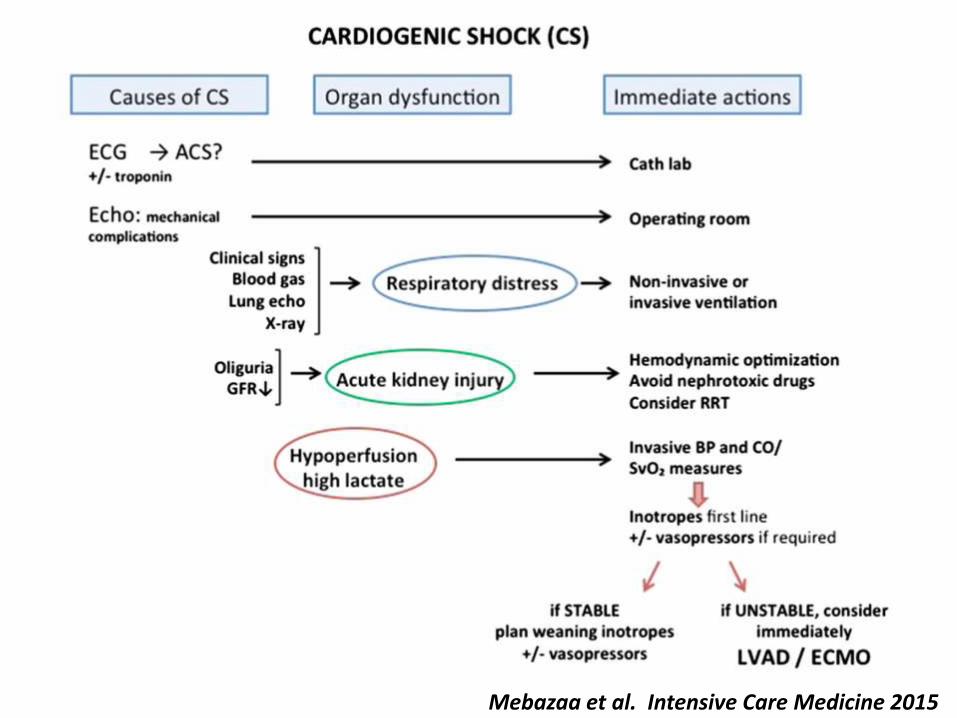
Mebazaa et al. Intensive Care Medicine 2015
Pirracchio et al. PLOS one 2013
The message is:
Vasopressors alone are harmful; better combine inotropes+vasopressors
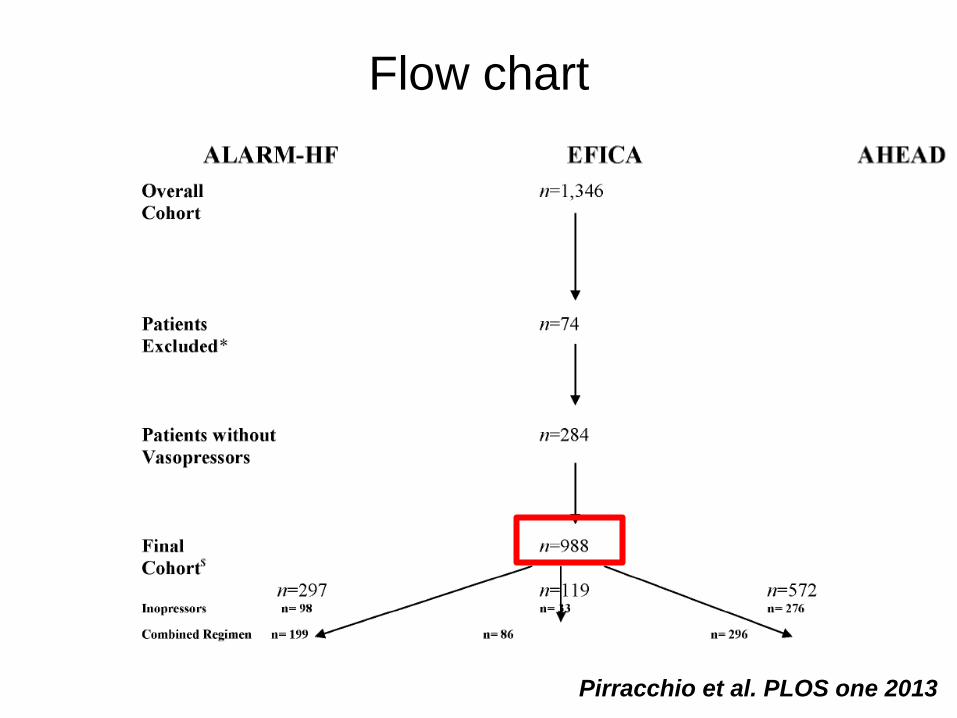
Flow chart
Pirracchio et al. PLOS one 2013
Inotropes/vasoactive agents
Pirracchio et al. PLOS one 2013
KM: in-hospital mortality
Pooled data: n= 988
Propensity score
combined regimen
Inopressors alone
Epi/NE/dopa
combined regimen
Inopressors alone
Epi/NE/dopa
Pirracchio et al. PLOS one 2013
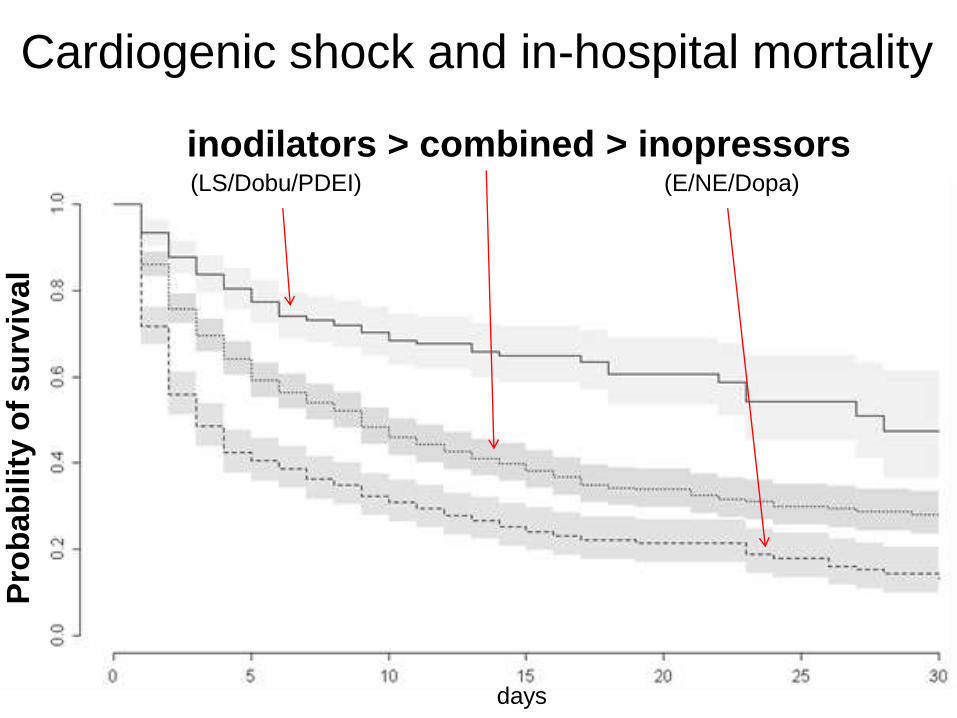
Cardiogenic shock and in-hospital mortality
days
Pro
bab
ilit
y o
f s
urv
ival
inodilators > combined > inopressors (LS/Dobu/PDEI) (E/NE/Dopa)
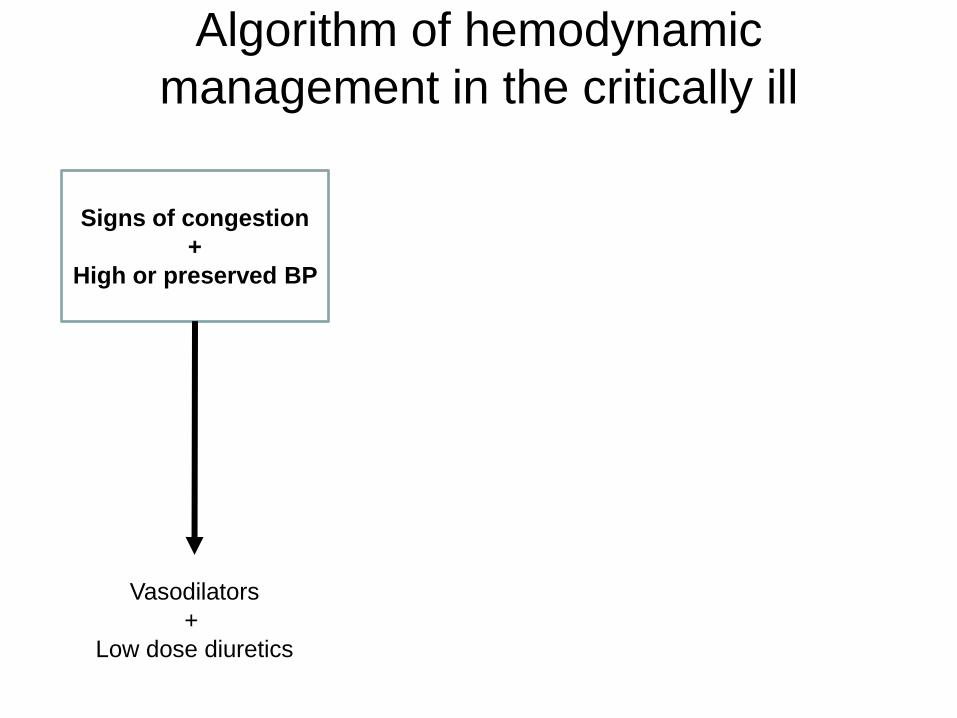
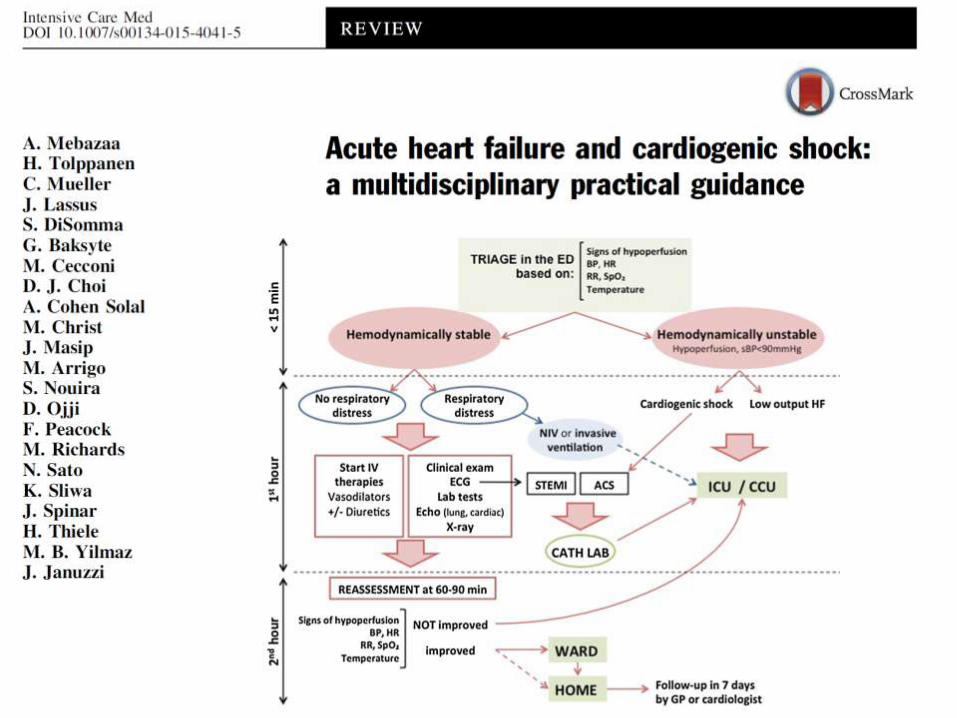
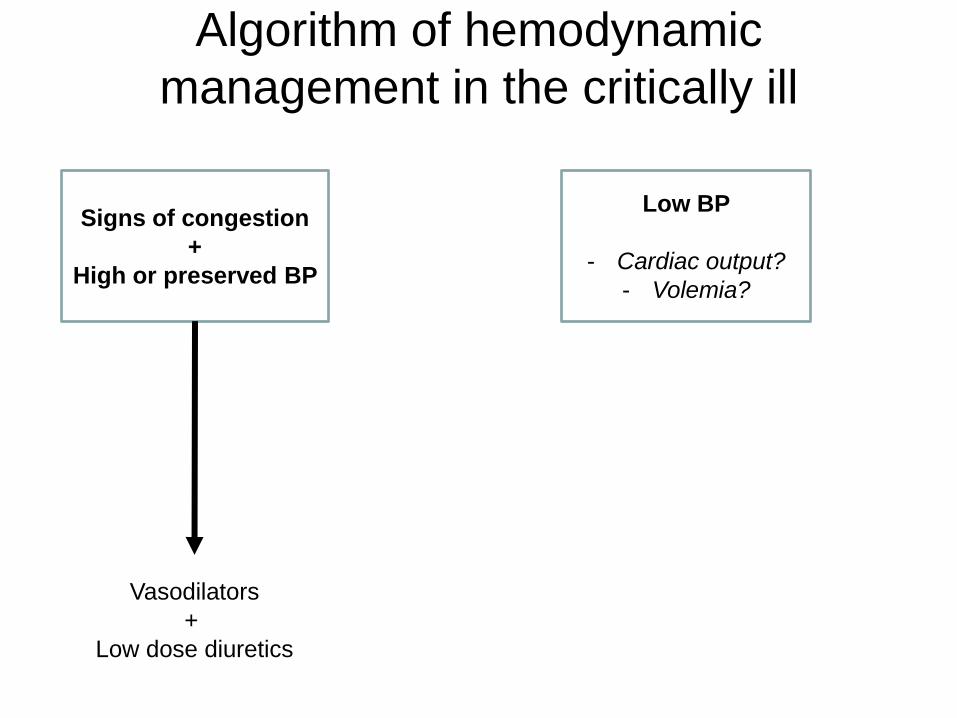
Algorithm of hemodynamic
management in the critically ill
Signs of congestion
+
High or preserved BP
Vasodilators
+
Low dose diuretics
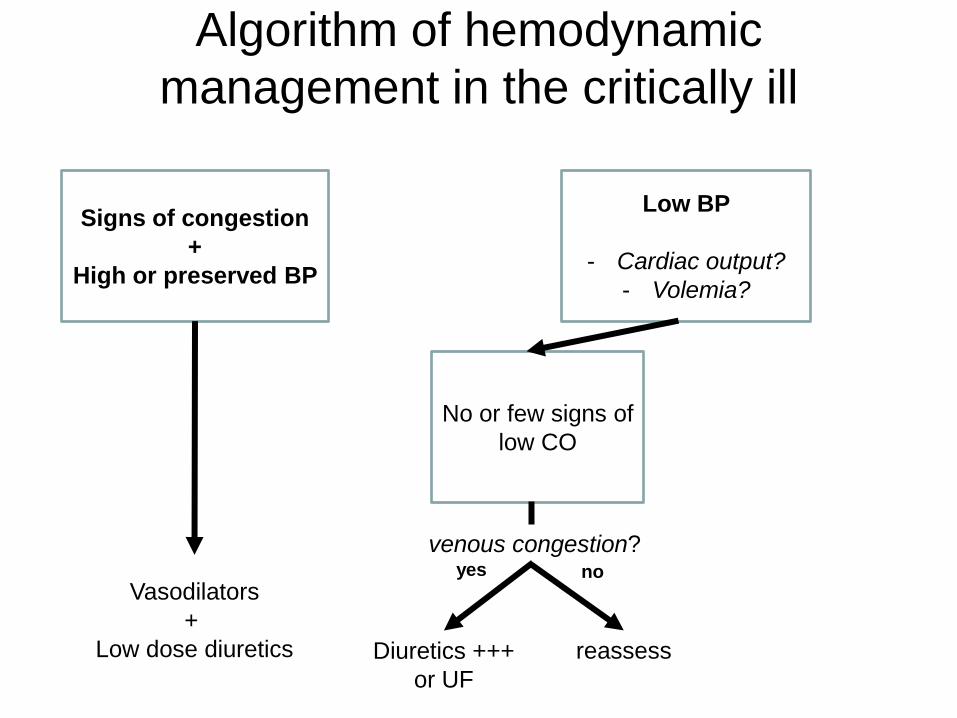
Algorithm of hemodynamic
management in the critically ill
Signs of congestion
+
High or preserved BP
Low BP
- Cardiac output?
- Volemia?
Vasodilators
+
Low dose diuretics
Algorithm of hemodynamic
management in the critically ill
Signs of congestion
+
High or preserved BP
Low BP
- Cardiac output?
- Volemia?
No or few signs of
low CO
Vasodilators
+
Low dose diuretics
venous congestion?
Diuretics +++
or UF
yes no
reassess
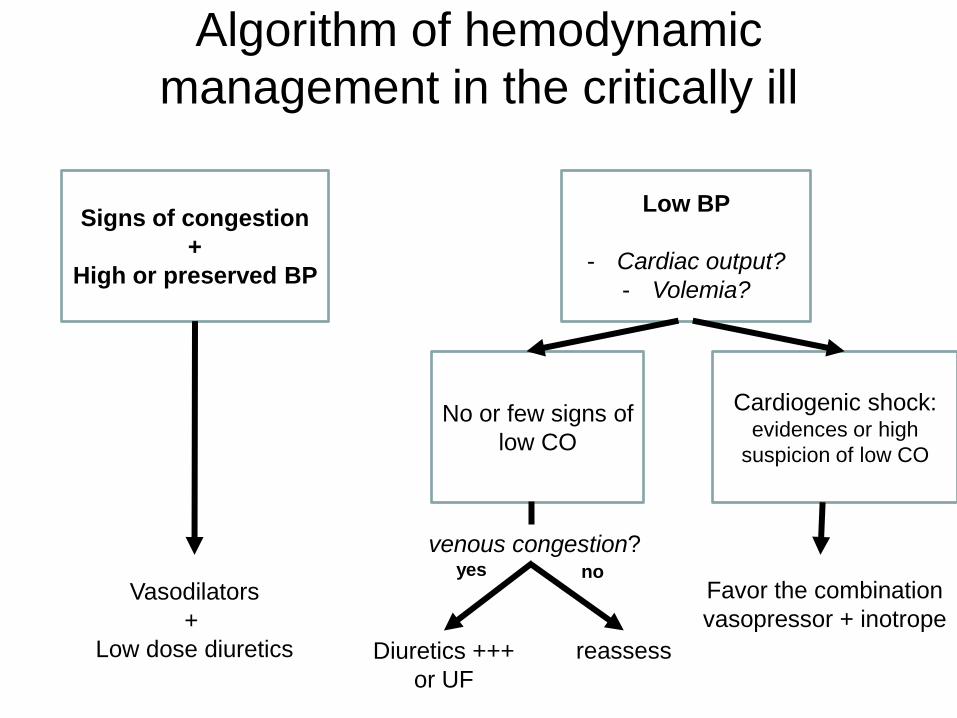
Algorithm of hemodynamic
management in the critically ill
Signs of congestion
+
High or preserved BP
Low BP
- Cardiac output?
- Volemia?
No or few signs of
low CO
Cardiogenic shock: evidences or high
suspicion of low CO
Vasodilators
+
Low dose diuretics
Favor the combination
vasopressor + inotrope
venous congestion?
Diuretics +++
or UF
yes no
reassess
Mebazaa et al. Intensive Care Medicine 2015
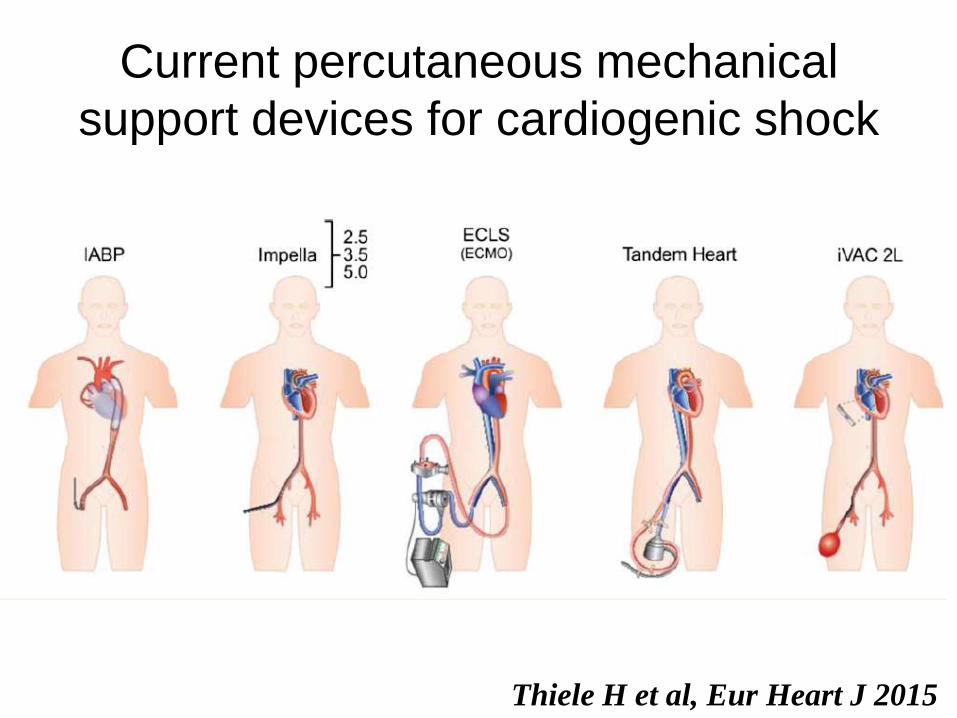
Current percutaneous mechanical
support devices for cardiogenic shock
Thiele H et al, Eur Heart J 2015
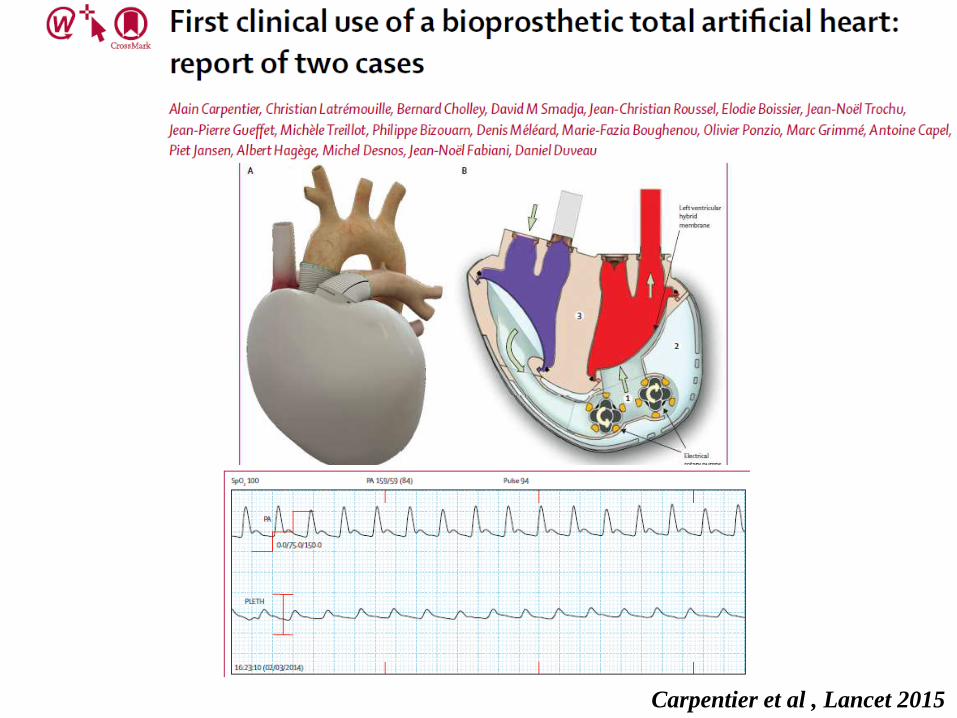
Carpentier et al , Lancet 2015
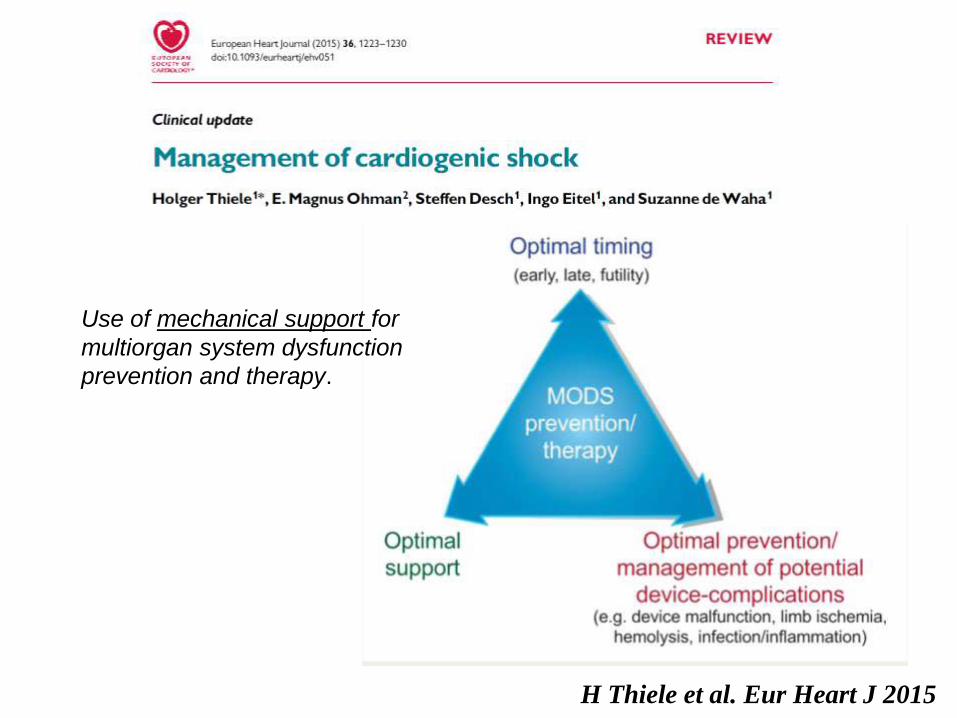
H Thiele et al. Eur Heart J 2015
Use of mechanical support for
multiorgan system dysfunction
prevention and therapy.
Inotropes and inodilatateurs
• Ils sont encore TROP utilisés en France et
dans le monde
• Ils ne doivent être utilisés que quand il y a
des signes patents de baisse de la
perfusion
• Leur durée d’utilisation doit être courte