gestion de l’anticoagulation orale en première ligne · status and hemostasis risk in...
TRANSCRIPT
Gestion de l’anticoagulation orale en première ligne
Par Caroline Brais, Pharm.D., M.Sc.
Pharmacienne CISSS Montérégie-Centre : Hôpital du Haut-Richelieu
28 octobre 2016
Conflits d’intérêt en lien avec cette présentation Aucun
Objectifs d’apprentissage
À la fin de cette présentation, vous devriez être en mesure de :
Différencier les caractéristiques des différents anticoagulants oraux
Identifier les patients qui bénéficieraient d’un NACO
Favoriser l’application de la loi 41 dans la gestion de l’anticoagulation orale d’un patient
Demande et interprétation de laboratoire, gestion du RNI
Gérer l’anticoagulation d’un patient avant une intervention chirurgicale
Abréviations ACO: anticoagulant oral
ACOD : anticoagulant oral direct (anciennement NACO, nouvel anticoagulant oral ou anticoagulants oraux non-vitamine K)
EP: embolie pulmonaire
FA: fibrillation auriculaire
HFPM: héparine de faible poids moléculaire
RNI: ratio normalisé international
Sgt: saignement(s)
TEV: thromboembolie veineuse
TVP: thrombose veineuse profonde
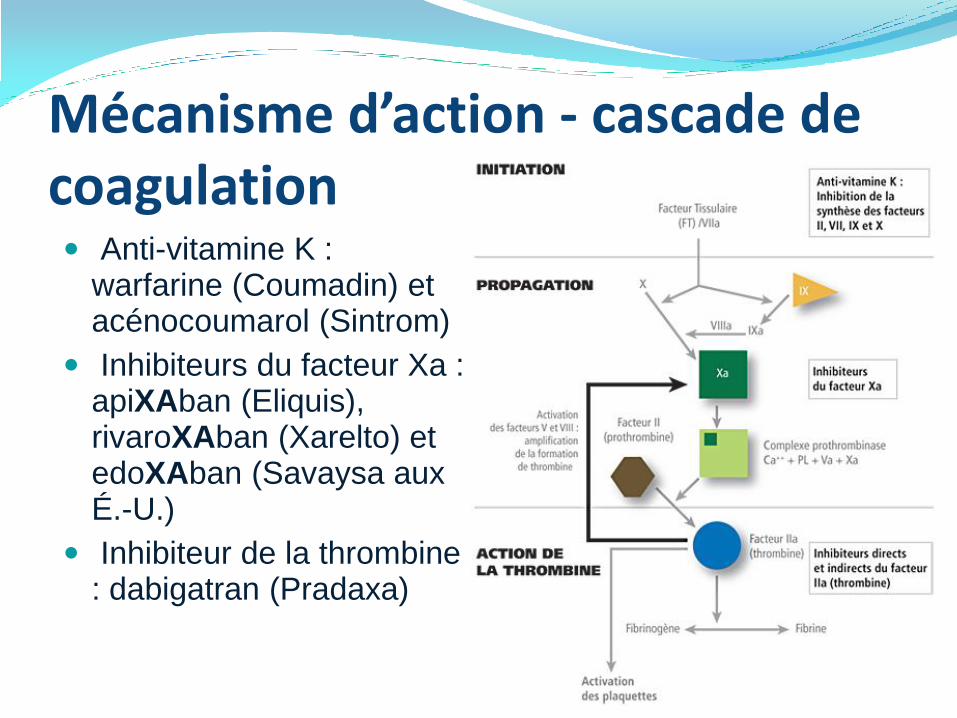
Anti-vitamine K : warfarine (Coumadin) et acénocoumarol (Sintrom)
Inhibiteurs du facteur Xa : apiXAban (Eliquis), rivaroXAban (Xarelto) et edoXAban (Savaysa aux É.-U.)
Inhibiteur de la thrombine : dabigatran (Pradaxa)
Mécanisme d’action - cascade de coagulation
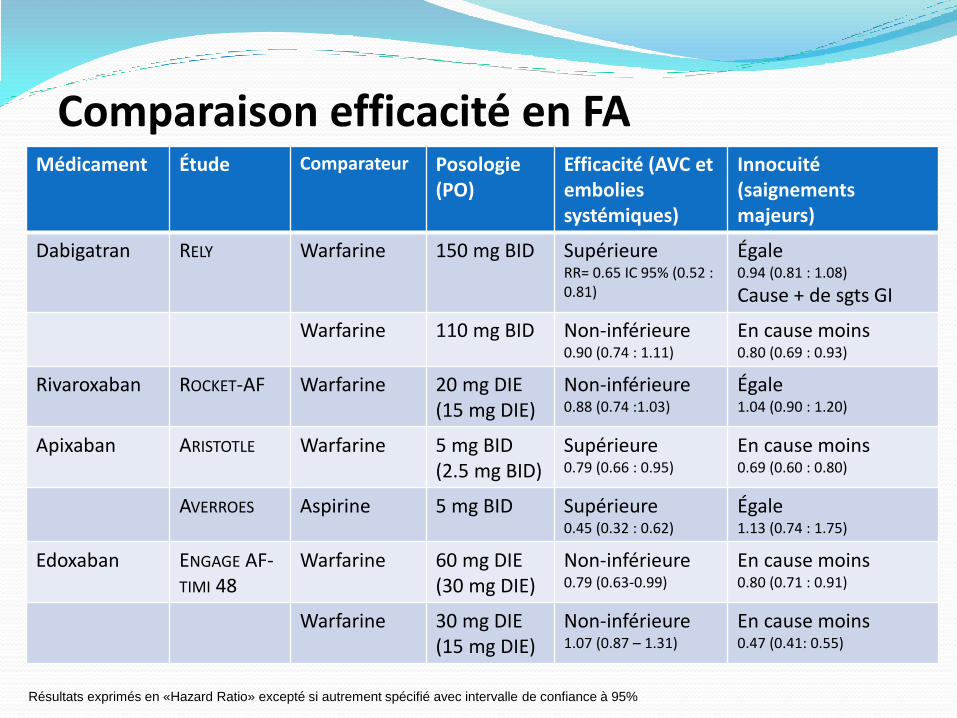
Comparaison efficacité en FA Médicament Étude Comparateur Posologie
(PO) Efficacité (AVC et embolies systémiques)
Innocuité (saignements majeurs)
Dabigatran RELY Warfarine 150 mg BID Supérieure RR= 0.65 IC 95% (0.52 : 0.81)
Égale 0.94 (0.81 : 1.08)
Cause + de sgts GI
Warfarine 110 mg BID Non-inférieure 0.90 (0.74 : 1.11)
En cause moins 0.80 (0.69 : 0.93)
Rivaroxaban ROCKET-AF Warfarine 20 mg DIE (15 mg DIE)
Non-inférieure 0.88 (0.74 :1.03)
Égale 1.04 (0.90 : 1.20)
Apixaban ARISTOTLE Warfarine 5 mg BID (2.5 mg BID)
Supérieure 0.79 (0.66 : 0.95)
En cause moins 0.69 (0.60 : 0.80)
AVERROES Aspirine 5 mg BID Supérieure 0.45 (0.32 : 0.62)
Égale 1.13 (0.74 : 1.75)
Edoxaban ENGAGE AF-TIMI 48
Warfarine 60 mg DIE (30 mg DIE)
Non-inférieure 0.79 (0.63-0.99)
En cause moins 0.80 (0.71 : 0.91)
Warfarine 30 mg DIE (15 mg DIE)
Non-inférieure 1.07 (0.87 – 1.31)
En cause moins 0.47 (0.41: 0.55)
Résultats exprimés en «Hazard Ratio» excepté si autrement spécifié avec intervalle de confiance à 95%
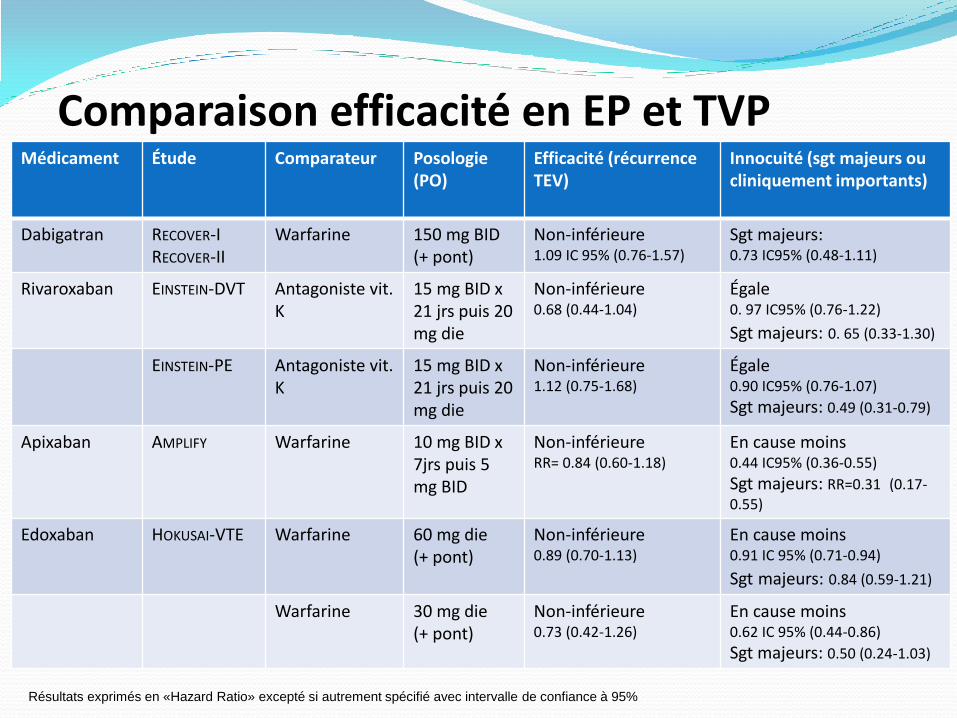
Comparaison efficacité en EP et TVP Médicament Étude Comparateur Posologie
(PO) Efficacité (récurrence TEV)
Innocuité (sgt majeurs ou cliniquement importants)
Dabigatran RECOVER-I RECOVER-II
Warfarine
150 mg BID (+ pont)
Non-inférieure 1.09 IC 95% (0.76-1.57)
Sgt majeurs: 0.73 IC95% (0.48-1.11)
Rivaroxaban EINSTEIN-DVT Antagoniste vit. K
15 mg BID x 21 jrs puis 20 mg die
Non-inférieure 0.68 (0.44-1.04)
Égale 0. 97 IC95% (0.76-1.22)
Sgt majeurs: 0. 65 (0.33-1.30)
EINSTEIN-PE Antagoniste vit. K
15 mg BID x 21 jrs puis 20 mg die
Non-inférieure 1.12 (0.75-1.68)
Égale 0.90 IC95% (0.76-1.07)
Sgt majeurs: 0.49 (0.31-0.79)
Apixaban AMPLIFY Warfarine 10 mg BID x 7jrs puis 5 mg BID
Non-inférieure RR= 0.84 (0.60-1.18)
En cause moins 0.44 IC95% (0.36-0.55)
Sgt majeurs: RR=0.31 (0.17-0.55)
Edoxaban HOKUSAI-VTE Warfarine 60 mg die (+ pont)
Non-inférieure 0.89 (0.70-1.13)
En cause moins 0.91 IC 95% (0.71-0.94)
Sgt majeurs: 0.84 (0.59-1.21)
Warfarine 30 mg die (+ pont)
Non-inférieure 0.73 (0.42-1.26)
En cause moins 0.62 IC 95% (0.44-0.86)
Sgt majeurs: 0.50 (0.24-1.03)
Résultats exprimés en «Hazard Ratio» excepté si autrement spécifié avec intervalle de confiance à 95%
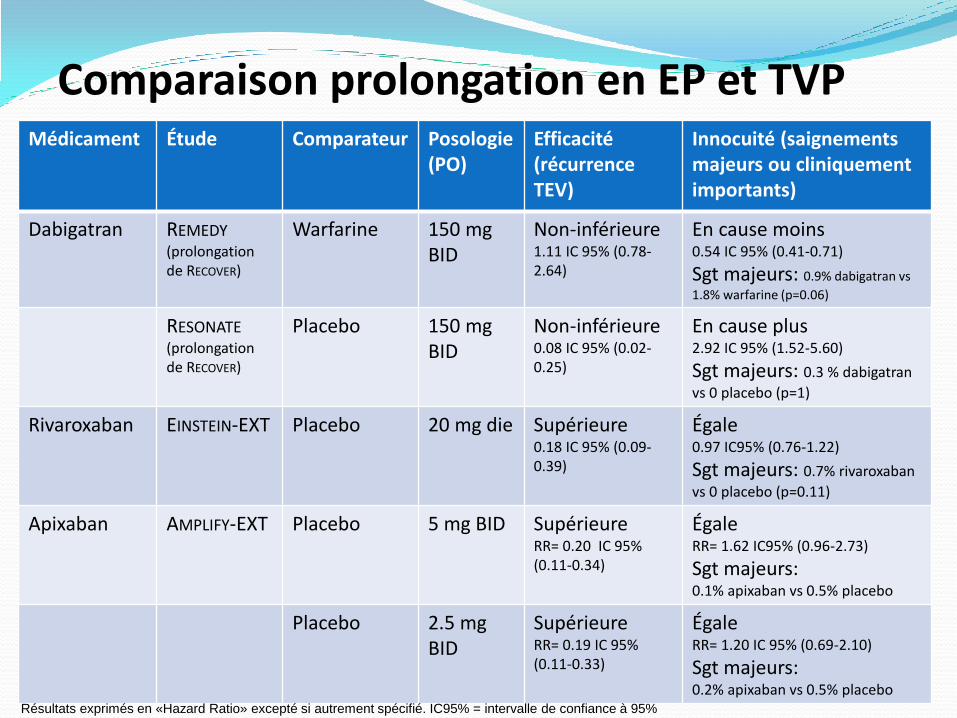
Comparaison prolongation en EP et TVP Médicament Étude Comparateur Posologie
(PO) Efficacité (récurrence TEV)
Innocuité (saignements majeurs ou cliniquement importants)
Dabigatran REMEDY (prolongation de RECOVER)
Warfarine 150 mg BID
Non-inférieure 1.11 IC 95% (0.78-2.64)
En cause moins 0.54 IC 95% (0.41-0.71)
Sgt majeurs: 0.9% dabigatran vs
1.8% warfarine (p=0.06)
RESONATE (prolongation de RECOVER)
Placebo 150 mg BID
Non-inférieure 0.08 IC 95% (0.02-0.25)
En cause plus 2.92 IC 95% (1.52-5.60)
Sgt majeurs: 0.3 % dabigatran
vs 0 placebo (p=1)
Rivaroxaban EINSTEIN-EXT Placebo 20 mg die Supérieure 0.18 IC 95% (0.09-0.39)
Égale 0.97 IC95% (0.76-1.22)
Sgt majeurs: 0.7% rivaroxaban
vs 0 placebo (p=0.11)
Apixaban AMPLIFY-EXT Placebo 5 mg BID Supérieure RR= 0.20 IC 95% (0.11-0.34)
Égale RR= 1.62 IC95% (0.96-2.73)
Sgt majeurs: 0.1% apixaban vs 0.5% placebo
Placebo 2.5 mg BID
Supérieure RR= 0.19 IC 95% (0.11-0.33)
Égale RR= 1.20 IC 95% (0.69-2.10)
Sgt majeurs: 0.2% apixaban vs 0.5% placebo
Résultats exprimés en «Hazard Ratio» excepté si autrement spécifié. IC95% = intervalle de confiance à 95%
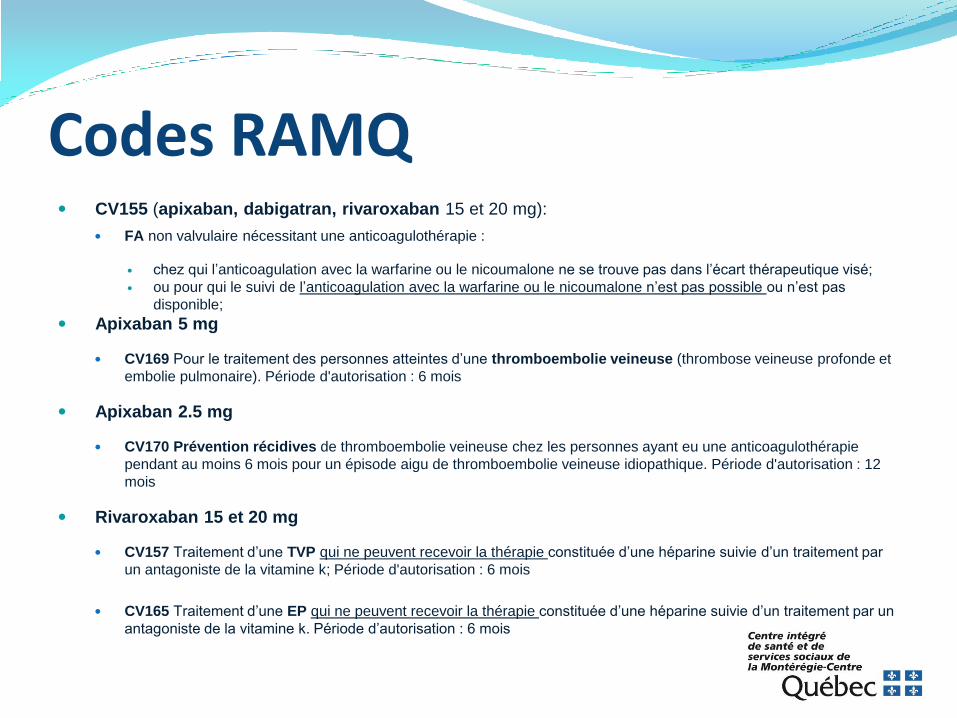
Codes RAMQ CV155 (apixaban, dabigatran, rivaroxaban 15 et 20 mg):
FA non valvulaire nécessitant une anticoagulothérapie :
chez qui l’anticoagulation avec la warfarine ou le nicoumalone ne se trouve pas dans l’écart thérapeutique visé;
ou pour qui le suivi de l’anticoagulation avec la warfarine ou le nicoumalone n’est pas possible ou n’est pas
disponible;
Apixaban 5 mg
CV169 Pour le traitement des personnes atteintes d’une thromboembolie veineuse (thrombose veineuse profonde et
embolie pulmonaire). Période d'autorisation : 6 mois
Apixaban 2.5 mg
CV170 Prévention récidives de thromboembolie veineuse chez les personnes ayant eu une anticoagulothérapie
pendant au moins 6 mois pour un épisode aigu de thromboembolie veineuse idiopathique. Période d'autorisation : 12
mois
Rivaroxaban 15 et 20 mg
CV157 Traitement d’une TVP qui ne peuvent recevoir la thérapie constituée d’une héparine suivie d’un traitement par
un antagoniste de la vitamine k; Période d'autorisation : 6 mois
CV165 Traitement d’une EP qui ne peuvent recevoir la thérapie constituée d’une héparine suivie d’un traitement par un
antagoniste de la vitamine k. Période d’autorisation : 6 mois
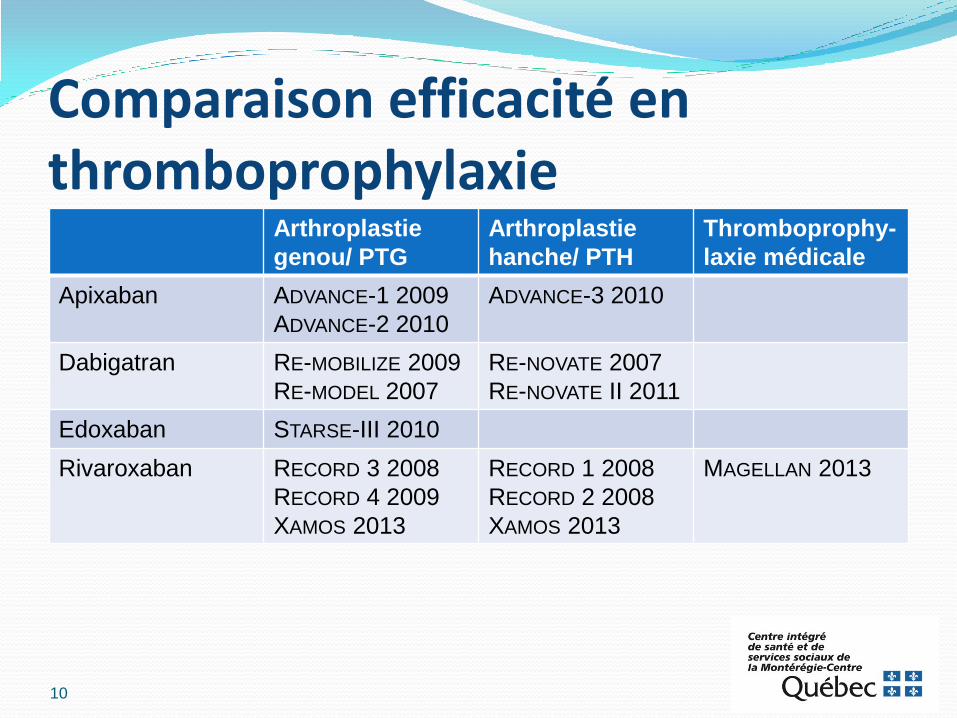
Comparaison efficacité en thromboprophylaxie
Arthroplastie
genou/ PTG
Arthroplastie
hanche/ PTH
Thromboprophy-
laxie médicale
Apixaban ADVANCE-1 2009
ADVANCE-2 2010
ADVANCE-3 2010
Dabigatran RE-MOBILIZE 2009
RE-MODEL 2007
RE-NOVATE 2007
RE-NOVATE II 2011
Edoxaban STARSE-III 2010
Rivaroxaban RECORD 3 2008
RECORD 4 2009
XAMOS 2013
RECORD 1 2008
RECORD 2 2008
XAMOS 2013
MAGELLAN 2013
10
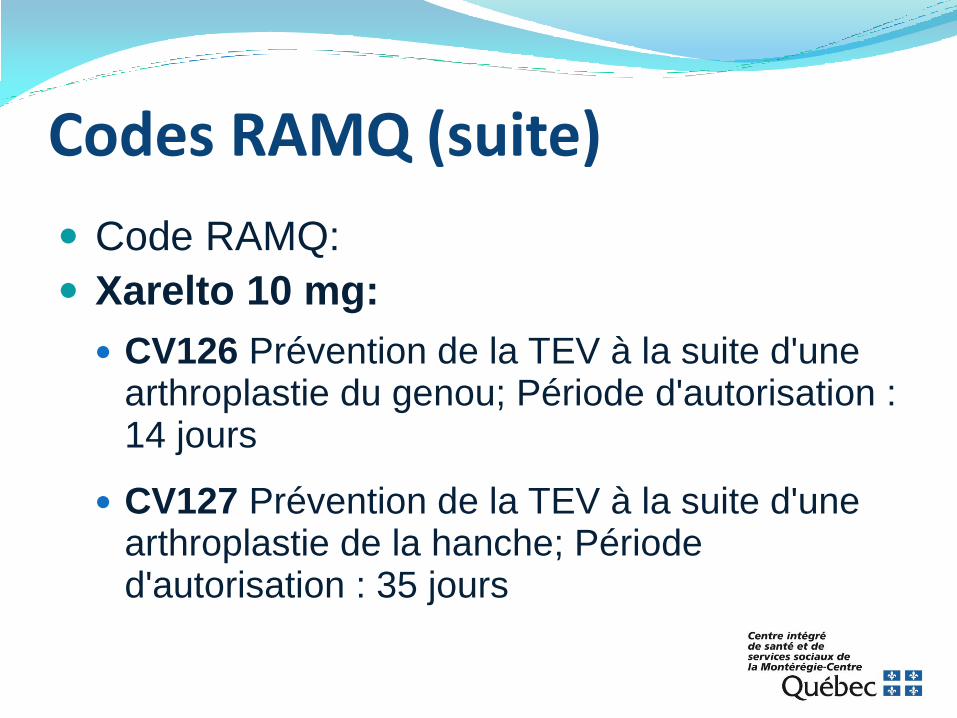
Codes RAMQ (suite)
Code RAMQ:
Xarelto 10 mg:
CV126 Prévention de la TEV à la suite d'une arthroplastie du genou; Période d'autorisation : 14 jours
CV127 Prévention de la TEV à la suite d'une arthroplastie de la hanche; Période d'autorisation : 35 jours
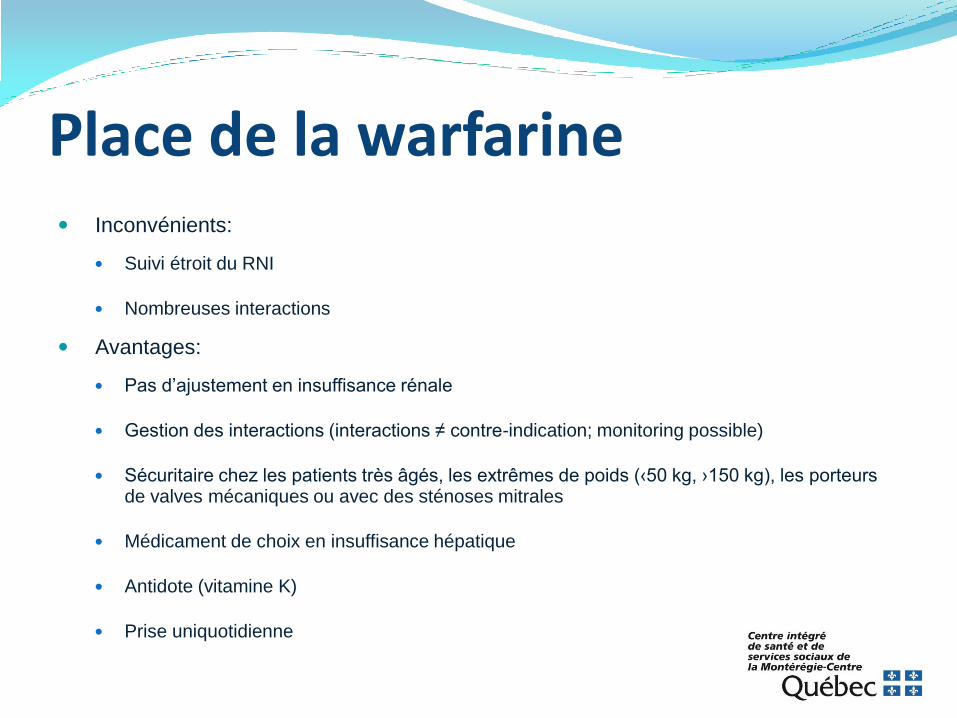
Place de la warfarine Inconvénients:
Suivi étroit du RNI
Nombreuses interactions
Avantages:
Pas d’ajustement en insuffisance rénale
Gestion des interactions (interactions ≠ contre-indication; monitoring possible)
Sécuritaire chez les patients très âgés, les extrêmes de poids (‹50 kg, ›150 kg), les porteurs de valves mécaniques ou avec des sténoses mitrales
Médicament de choix en insuffisance hépatique
Antidote (vitamine K)
Prise uniquotidienne
Cas-patient
Vous recevez le résultat du RNI d’une patiente de 76 ans sous warfarine pour FA. Son RNI est très labile et est actuellement supra-thérapeutique (3.52). Suite à une discussion avec votre patiente, vous réalisez que l’été étant fini, son potager ne lui fournit plus de brocolis. De plus, elle se plaint de la nécessité de faire des RNI fréquemment.
Cas-patient (suite)
Caractéristiques de la patiente:
Prend ses médicaments écrasés. Difficulté avec sa motricité fine.
Creat: 115 ClCr : 40 ml/min Poids: 70 kg
Choix de l’ACO: Lequel serait le mieux pour cette patiente?
Poursuivre la warfarine, diminuer légèrement la dose et recontrôler dans 1 semaine
Changer la warfarine pour le rivaroxaban 15 mg die
Changer la warfarine pour le dabigatran 150 mg BID
Changer la warfarine pour l’apixaban 2.5 mg BID
Gestion du RNI (Demande de labo) - Région Charles-Lemoyne
Gestion du RNI (Demande de labo)
Région Haut-Richelieu
Sera bientôt déposer avec les ordonnances collectives sur l’extranet de la Montérégie :
http://extranet.santemonteregie.qc.ca/affaires-medicales-professionnelles/ordonnances/index.fr.html
Trucs pour favoriser une gestion «facile» du RNI Prise de la warfarine le soir
Patient fait le RNI en avant-midi, permet d’avoir le temps de se réajuster avant la prochaine prise
Avoir un dossier complet
La loi 41 nous permet de gérer le RNI, mais elle ne nous permet pas d’initier une HFPM sans ordonnance d’un médecin. (Contactez MD pour avoir une Rx en attente au dossier si RNI devient sous-thérapeutique.)
Prévoir les interactions
Faire un RNI dans les 4-5 jours suivants l’ajout ou le retrait d’une interaction médicamenteuse.
Prévoir un contrôle plus rapproché si l’écart entre 2 RNI consécutifs est ≥ à 0.8
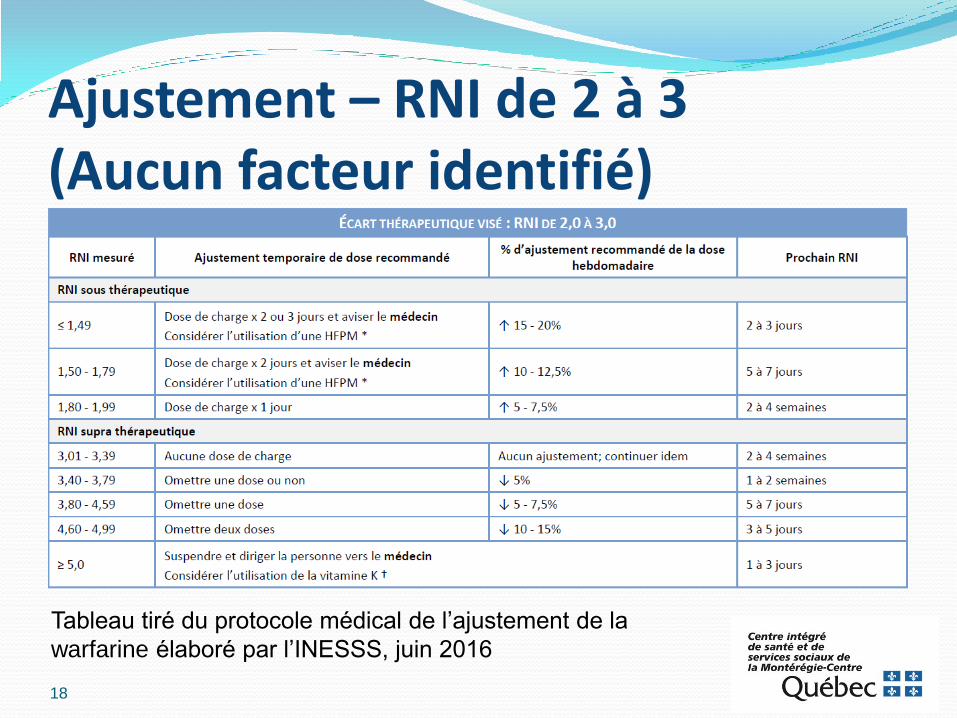
Ajustement – RNI de 2 à 3 (Aucun facteur identifié)
18
Tableau tiré du protocole médical de l’ajustement de la
warfarine élaboré par l’INESSS, juin 2016
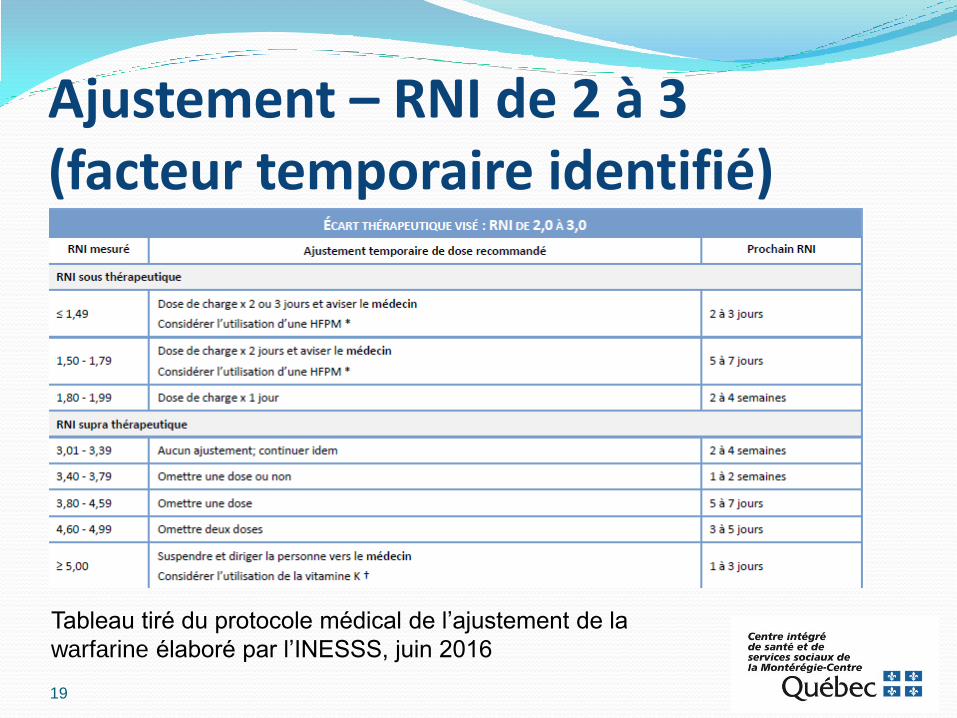
Ajustement – RNI de 2 à 3 (facteur temporaire identifié)
19
Tableau tiré du protocole médical de l’ajustement de la
warfarine élaboré par l’INESSS, juin 2016
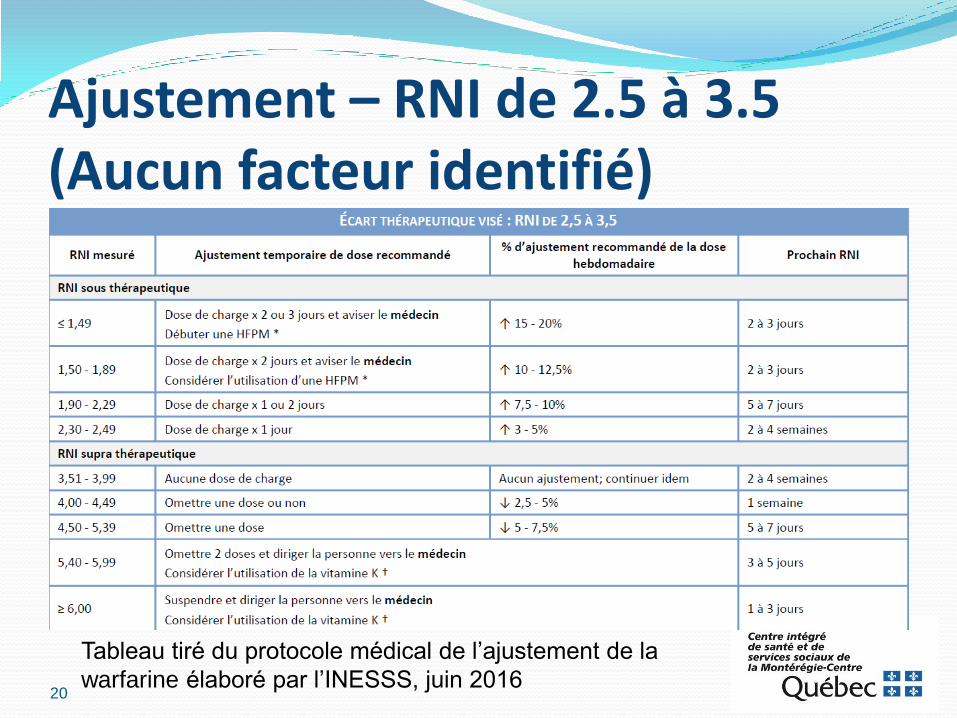
Ajustement – RNI de 2.5 à 3.5 (Aucun facteur identifié)
20
Tableau tiré du protocole médical de l’ajustement de la
warfarine élaboré par l’INESSS, juin 2016
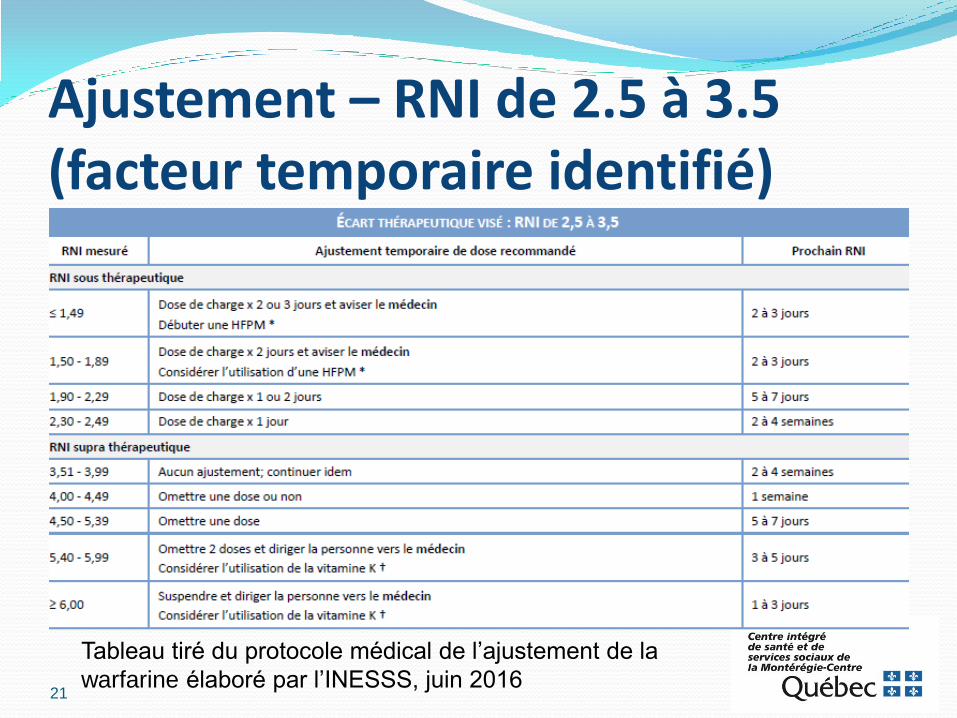
Ajustement – RNI de 2.5 à 3.5 (facteur temporaire identifié)
21
Tableau tiré du protocole médical de l’ajustement de la
warfarine élaboré par l’INESSS, juin 2016
Cas-patient
M. X se présente à la pharmacie car il doit
subir une opération au genou dans un peu
plus d’une semaine et vient chercher une
liste à jour de sa médication. Vous réalisez
qu’il prend de l’apixaban 5 mg BID et n’est
pas au courant si un arrêt est nécessaire.
Que faites-vous?
22
Cas-patient (Choix de réponse)
A- Fermez les yeux et faites comme si de rien n’était
B- Vérifiez la fonction rénale du patient
C- Contactez le MD pour faire cesser l’apixaban quelques jours avant
D- B et C
E- Toutes ces réponses
F- Aucune de ces réponses
23
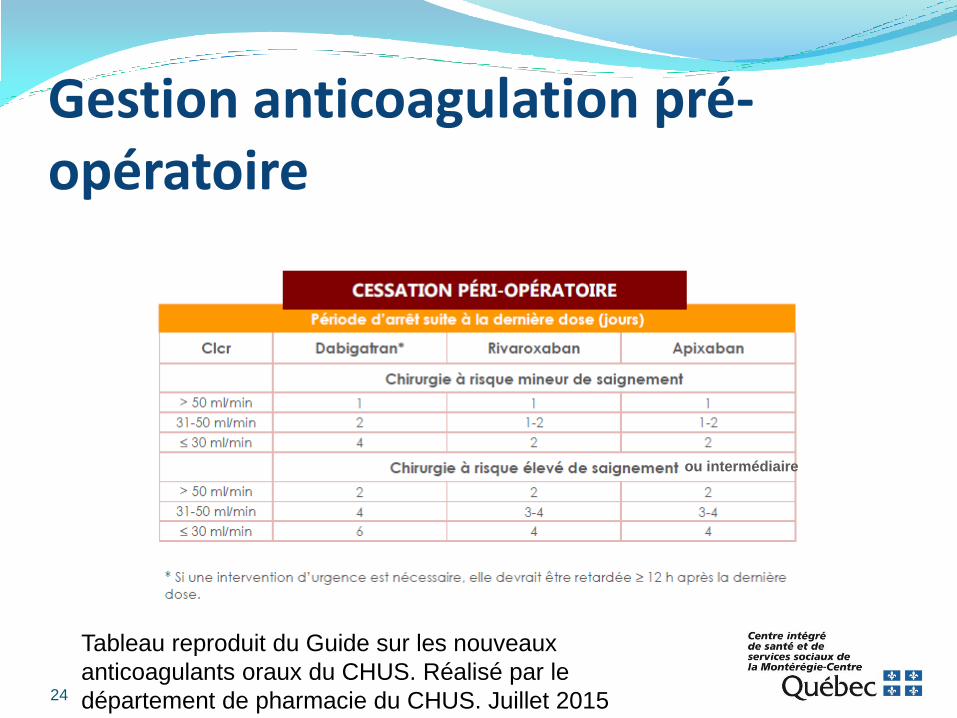
Gestion anticoagulation pré-opératoire
24
Tableau reproduit du Guide sur les nouveaux
anticoagulants oraux du CHUS. Réalisé par le
département de pharmacie du CHUS. Juillet 2015
ou intermédiaire
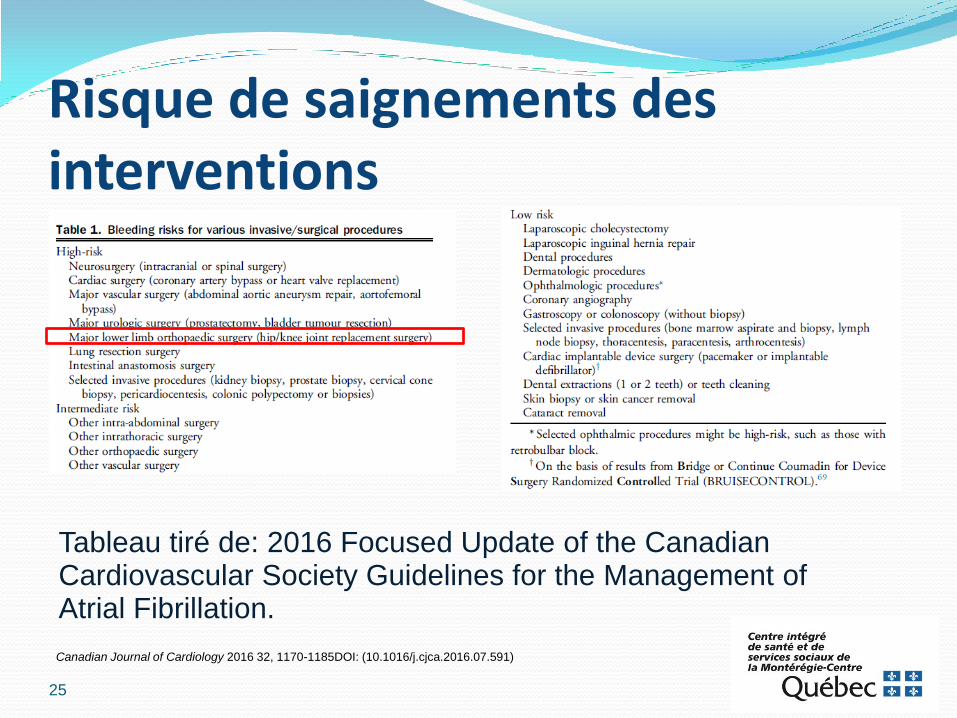
Risque de saignements des interventions
Tableau tiré de: 2016 Focused Update of the Canadian Cardiovascular Society Guidelines for the Management of Atrial Fibrillation.
25
Canadian Journal of Cardiology 2016 32, 1170-1185DOI: (10.1016/j.cjca.2016.07.591)
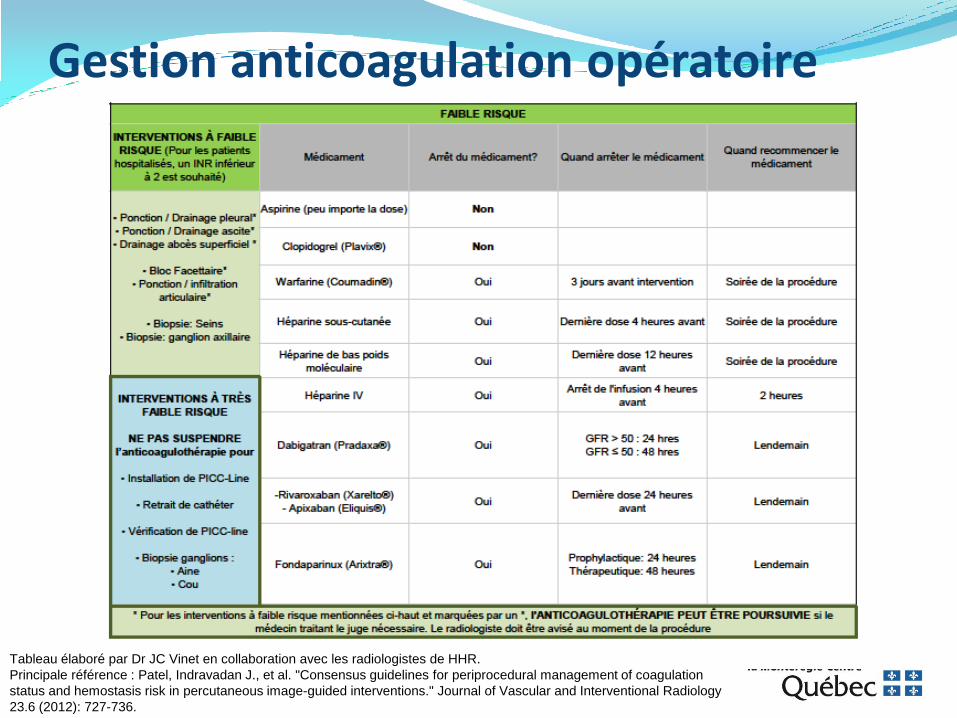
Gestion anticoagulation opératoire
Tableau élaboré par Dr JC Vinet en collaboration avec les radiologistes de HHR.
Principale référence : Patel, Indravadan J., et al. "Consensus guidelines for periprocedural management of coagulation
status and hemostasis risk in percutaneous image-guided interventions." Journal of Vascular and Interventional Radiology
23.6 (2012): 727-736.
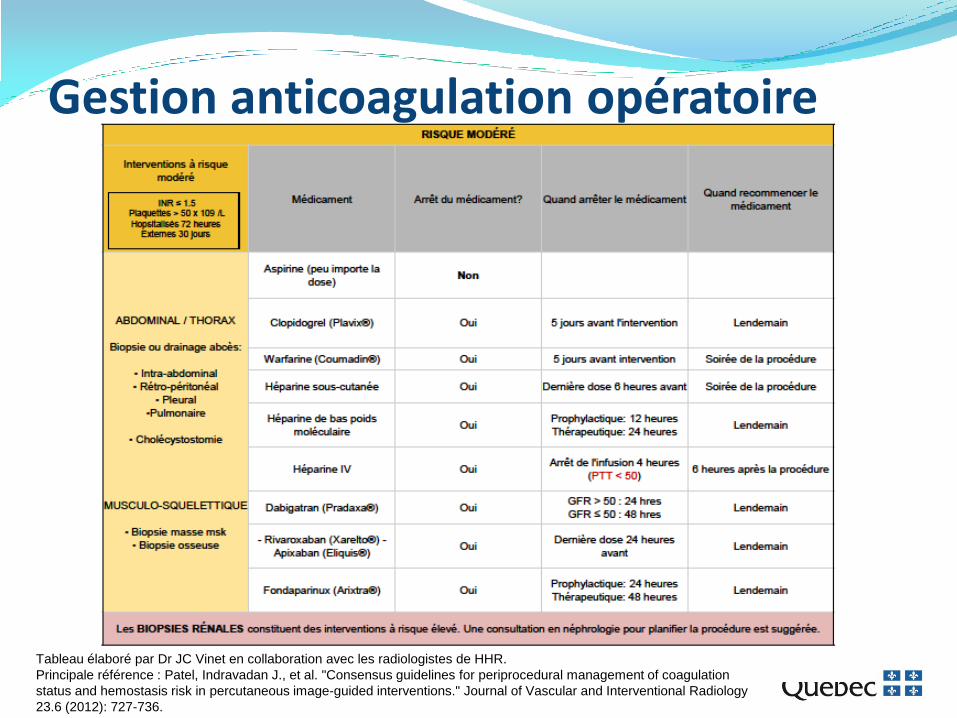
Gestion anticoagulation opératoire
Tableau élaboré par Dr JC Vinet en collaboration avec les radiologistes de HHR.
Principale référence : Patel, Indravadan J., et al. "Consensus guidelines for periprocedural management of coagulation
status and hemostasis risk in percutaneous image-guided interventions." Journal of Vascular and Interventional Radiology
23.6 (2012): 727-736.
Doit-on faire un pont? Étude BRIDGE (NEJM août 2015)
Étude chez patient en FA devant arrêter leur warfarine pour une procédure élective.
Groupe : Placebo vs Pont avec daltéparine 100 U/kg BID débuté 3 jours pré et poursuivi ad RNI thérapeutique (5-10 jrs post)
Efficacité: thromboembolie artérielle (AVC/ICT, embolie systémique) : 0.4% dans le groupe sans pont vs 0.3% dans le groupe avec pont (p=0,01 pour non-infériorité)
Innocuité: Saignements majeurs : 1.3% dans le groupe sans pont vs 3.2% dans le groupe avec pont (p=0.005 pour supériorité) NNH=53
Limites:
Peu de patients à risque élevé d’événements (CHADS moyen = 2)
Interventions à faible risque surtout (90%)
Les recommandations canadiennes suggèrent:
De ne pas faire de pont pour les patients sous NACO
De faire un pont pour les patients sous warfarine à haut risque thromboembolique
Gestion anticoagulation post-opératoire Quand l’hémostase est établie
Reprise habituelle entre 24-48h post-op (si
risque faible)
Reprise entre 48-72h post-op (si risque
intermédiaire à élevé)
Warfarine: doses prophylactiques
d’héparine ou HFPM pour les premières 24-
72h
Antidotes Warfarine : vitamine K
Dabigatran: idarucizumab (Praxbind)
Anticorps monoclonal qui se lie de manière préférentielle au dabigatran empêchant sa liaison à la thrombine
Étude REVERSE AD : chez des patients avec saignements importants ou nécessitant une procédure invasive urgente.
À venir:
Andexanet alfa (antidote antiXa)
Aripazine (ou ciraparantag) (antidote universel : héparine, HFPM, fondaparinux, inhibiteurs du facteur Xa et de la thrombine)
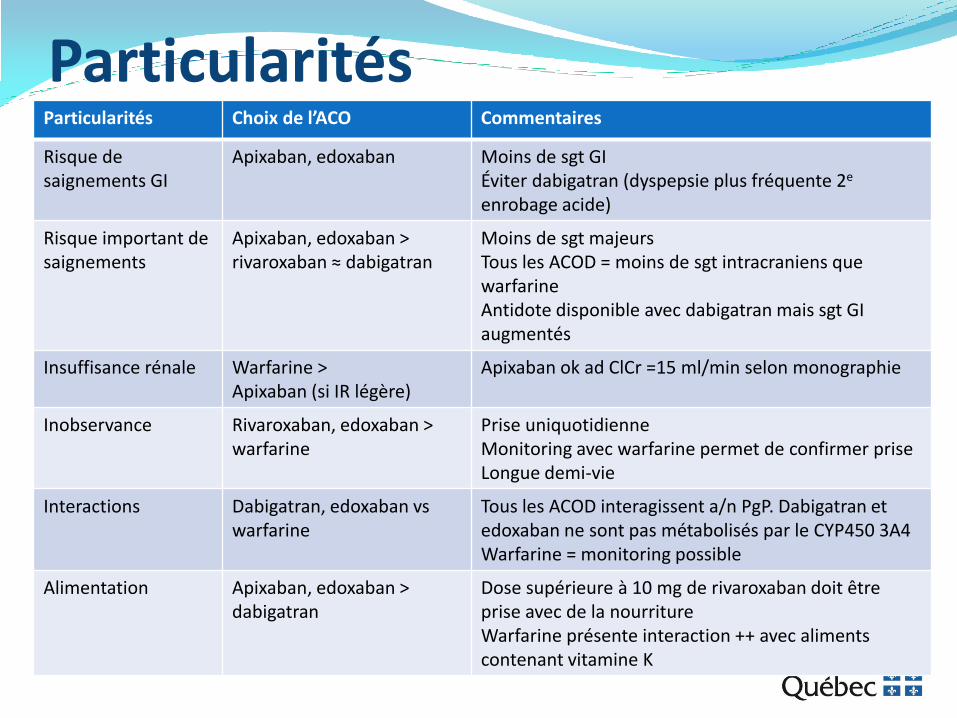
Particularités Particularités Choix de l’ACO Commentaires
Risque de saignements GI
Apixaban, edoxaban Moins de sgt GI Éviter dabigatran (dyspepsie plus fréquente 2e enrobage acide)
Risque important de saignements
Apixaban, edoxaban > rivaroxaban ≈ dabigatran
Moins de sgt majeurs Tous les ACOD = moins de sgt intracraniens que warfarine Antidote disponible avec dabigatran mais sgt GI augmentés
Insuffisance rénale Warfarine > Apixaban (si IR légère)
Apixaban ok ad ClCr =15 ml/min selon monographie
Inobservance Rivaroxaban, edoxaban > warfarine
Prise uniquotidienne Monitoring avec warfarine permet de confirmer prise Longue demi-vie
Interactions Dabigatran, edoxaban vs warfarine
Tous les ACOD interagissent a/n PgP. Dabigatran et edoxaban ne sont pas métabolisés par le CYP450 3A4 Warfarine = monitoring possible
Alimentation Apixaban, edoxaban > dabigatran
Dose supérieure à 10 mg de rivaroxaban doit être prise avec de la nourriture Warfarine présente interaction ++ avec aliments contenant vitamine K
Outils cliniques Mise à jour des lignes directrices canadiennes pour la prise en
charge de la FA 2016. Disponible en ligne seulement : http://www.onlinecjc.ca/article/S0828-282X(16)30829-7/abstract
Guide NACO du CHUS (Mélanie Gilbert) juill. 2015
Protocole médical de l’INESSS sur l’anticoagulothérapie juin 2016 (https://www.inesss.qc.ca/activites/ord-coll-et-prescription-infirmiere/ordonnances-collectives/anticoagulotherapie.html)
Document de l’INESSS (Pradaxa en FA, NACO en FA)
Résumé des études: http://www.anticoagulant-trials.eu/studies-a-z.html
Études AMPLIFY. Oral Apixaban for the Treatment of Acute Venous Thromboembolism. Agnelli et al. NEJM 2013
AMPLIFY-EXT. Apixaban for Extended Treatment of Venous Thromboembolism. Agnelli et al. NEJM 2013
ARISTOTLE. Apixaban versus Warfarin in Patients with Atrial Fibrillation. Granger et al. NEJM 2011
AVERROES. Apixaban in Patients with Atrial Fibrillation. Connolly et al. NEJM 2011
BRIDGE. Perioperative Bridging Anticoagulation in Patients with Atrial Fibrillation. Douketis et al. NEJM 2015
EINSTEIN-DVT et EINSTEIN-EXT. Oral Rivaroxaban for Symptomatic Venous Thromboembolism. NEJM 2010
EINSTEIN-PE. Oral Rivaroxaban for the Treatment of Symptomatic Pulmonary Embolism. NEJM 2012
ENGAGE-AF TIMI 48. Edoxaban versus Warfarin in Patients with Atrial Fibrillation. Giugliano et al. NEJM 2013
HOKUSAI-VTE. Edoxaban versus Warfarin for the Treatment of Symptomatic Venous Thromboembolism. NEJM 2013
RECOVER I. Dabigatran versus Warfarin in the Treatment of Acute Venous Thromboembolism. Schulman et al. NEJM 2009
RECOVER II. Treatment of Acute Venous Thromboembolism With Dabigatran or Warfarin and Pooled Analysis. Schulman et al. Circulation 2013
RELY. Connolly et al. NEJM 2009
REMEDY et RESONATE. Extended Use of Dabigatran, Warfarin or Placebo in Venous Thromboembolism. Schulman et al. NEJM 2013
ROCKET-AF. Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation. Patel et al. NEJM 2011
Etc.
Questions? Merci!
34
À venir COMPASS
Cardiovascular OutcoMes for People using Anticoagulation StrategieS (2013, ongoing)
PIONEER AF-PCI
Study exploring two strategies of rivaroxaban and one of oral vitamin K antagonists in patients with atrial fibrillation who undergo percutaneous coronary intervention (2013, ongoing)
VENTURE-AF
A study exploring two treatment strategies in patients with atrial fibrillation who undergo catheter ablation therapy (2013, ongoing)
X-PLORER
Exploring the efficacy and safety of rivaroxaban to support elective percutaneous coronary intervention (2013, ongoing)
X-VeRT
EXplore the efficacy and safety of once-daily oral riVaroxaban for the prevention of caRdiovascular events in subjects with non-valvular aTrial fibrillation scheduled for cardioversion (2013, ongoing)
Valves RE-ALIGN
Randomised, phase II study to Evaluate the sAfety and pharmacokinetics of oraL dabIGatran etexilate in patients after heart valve replacemeNt (2013)
In the dabigatran group, ischemic or unspecified stroke occurred in 9 patients (5%) and myocardial infarction occurred in 3 patients (2%), whereas there were no cases of stroke or myocardial infarction in the warfarin group. Major bleeding was seen in 7 patients (4%) and 2 patients (2%), respectively; and bleeding of any type occurred in 45 patients (27%) and 10 patients (12%), respectively (HR 2.45; p=0.01). All patients with major bleeding had pericardial bleeding n=168 dabi et n=84 warfarin
Dabigatran is not appropriate as an alternative to warfarin for the prevention of thromboembolic complications in patients who require anticoagulation after the implantation of a prosthetic heart valve. The use of dabigatran was associated with increased rates of thromboembolic and bleeding complications, thus showing no benefit and an excess risk
Combinaison avec antiplaquettaires? PETRO? (dabigatran + AAS)
RE-DEEM 2009 (dabi vs placebo en SCA sur bithérapie)
RUBY-1 2011 (darexaban en SCA sur AAS+/- Plavix)
EINSTEIN-PE
APPRAISE-2 (apixaban en SCA -> sgt +, arrêt prématuré)
WOEST : What is the Optimal antiplatElet & anticoagulant therapy in patients with oral anticoagulation and coronary stenTing? (2013)
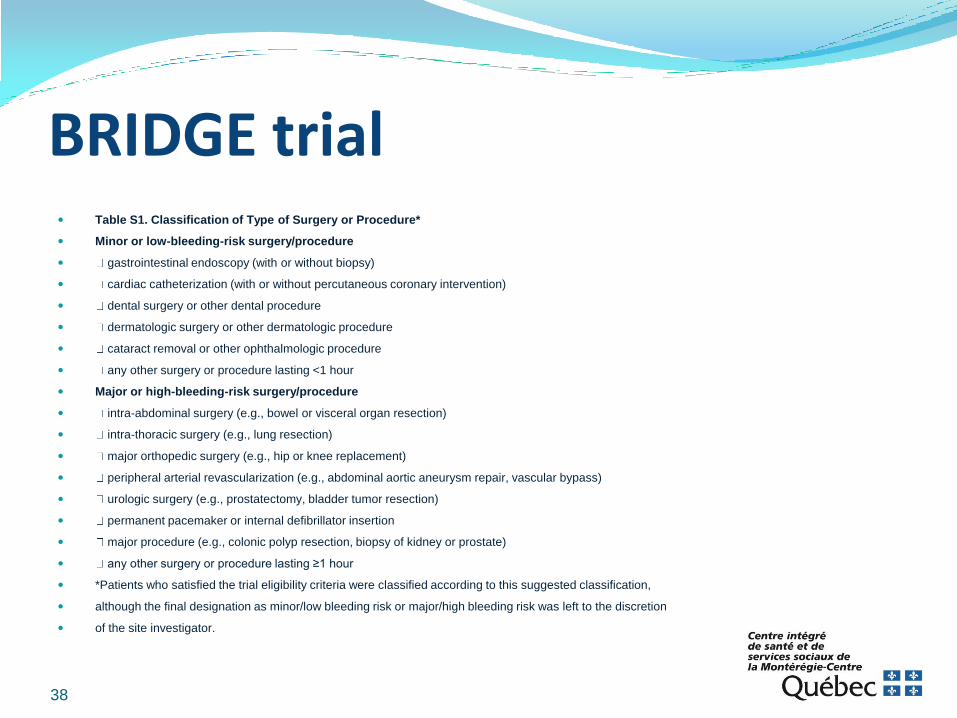
BRIDGE trial Table S1. Classification of Type of Surgery or Procedure*
Minor or low-bleeding-risk surgery/procedure
gastrointestinal endoscopy (with or without biopsy)
cardiac catheterization (with or without percutaneous coronary intervention)
dental surgery or other dental procedure
dermatologic surgery or other dermatologic procedure
cataract removal or other ophthalmologic procedure
any other surgery or procedure lasting <1 hour
Major or high-bleeding-risk surgery/procedure
intra-abdominal surgery (e.g., bowel or visceral organ resection)
intra-thoracic surgery (e.g., lung resection)
major orthopedic surgery (e.g., hip or knee replacement)
peripheral arterial revascularization (e.g., abdominal aortic aneurysm repair, vascular bypass)
urologic surgery (e.g., prostatectomy, bladder tumor resection)
permanent pacemaker or internal defibrillator insertion
major procedure (e.g., colonic polyp resection, biopsy of kidney or prostate)
any other surgery or procedure lasting ≥1 hour
*Patients who satisfied the trial eligibility criteria were classified according to this suggested classification,
although the final designation as minor/low bleeding risk or major/high bleeding risk was left to the discretion
of the site investigator.
38
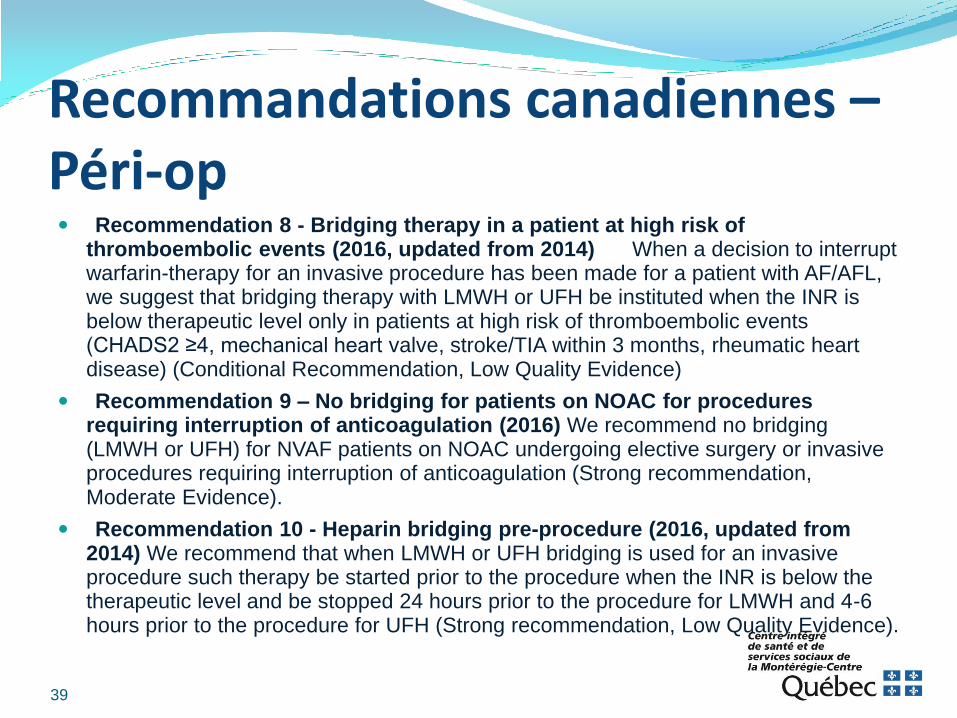
Recommandations canadiennes – Péri-op Recommendation 8 - Bridging therapy in a patient at high risk of
thromboembolic events (2016, updated from 2014) When a decision to interrupt warfarin-therapy for an invasive procedure has been made for a patient with AF/AFL, we suggest that bridging therapy with LMWH or UFH be instituted when the INR is below therapeutic level only in patients at high risk of thromboembolic events (CHADS2 ≥4, mechanical heart valve, stroke/TIA within 3 months, rheumatic heart disease) (Conditional Recommendation, Low Quality Evidence)
Recommendation 9 – No bridging for patients on NOAC for procedures requiring interruption of anticoagulation (2016) We recommend no bridging (LMWH or UFH) for NVAF patients on NOAC undergoing elective surgery or invasive procedures requiring interruption of anticoagulation (Strong recommendation, Moderate Evidence).
Recommendation 10 - Heparin bridging pre-procedure (2016, updated from 2014) We recommend that when LMWH or UFH bridging is used for an invasive procedure such therapy be started prior to the procedure when the INR is below the therapeutic level and be stopped 24 hours prior to the procedure for LMWH and 4-6 hours prior to the procedure for UFH (Strong recommendation, Low Quality Evidence).
39
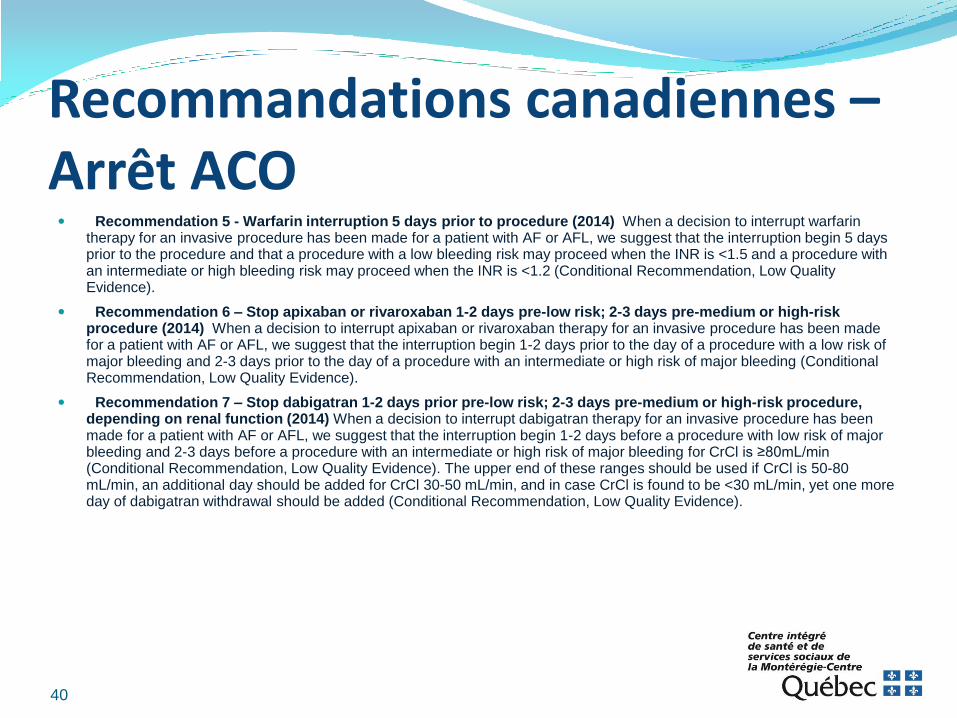
Recommandations canadiennes – Arrêt ACO Recommendation 5 - Warfarin interruption 5 days prior to procedure (2014) When a decision to interrupt warfarin
therapy for an invasive procedure has been made for a patient with AF or AFL, we suggest that the interruption begin 5 days prior to the procedure and that a procedure with a low bleeding risk may proceed when the INR is <1.5 and a procedure with an intermediate or high bleeding risk may proceed when the INR is <1.2 (Conditional Recommendation, Low Quality Evidence).
Recommendation 6 – Stop apixaban or rivaroxaban 1-2 days pre-low risk; 2-3 days pre-medium or high-risk procedure (2014) When a decision to interrupt apixaban or rivaroxaban therapy for an invasive procedure has been made for a patient with AF or AFL, we suggest that the interruption begin 1-2 days prior to the day of a procedure with a low risk of major bleeding and 2-3 days prior to the day of a procedure with an intermediate or high risk of major bleeding (Conditional Recommendation, Low Quality Evidence).
Recommendation 7 – Stop dabigatran 1-2 days prior pre-low risk; 2-3 days pre-medium or high-risk procedure, depending on renal function (2014) When a decision to interrupt dabigatran therapy for an invasive procedure has been made for a patient with AF or AFL, we suggest that the interruption begin 1-2 days before a procedure with low risk of major bleeding and 2-3 days before a procedure with an intermediate or high risk of major bleeding for CrCl is ≥80mL/min (Conditional Recommendation, Low Quality Evidence). The upper end of these ranges should be used if CrCl is 50-80 mL/min, an additional day should be added for CrCl 30-50 mL/min, and in case CrCl is found to be <30 mL/min, yet one more day of dabigatran withdrawal should be added (Conditional Recommendation, Low Quality Evidence).
40
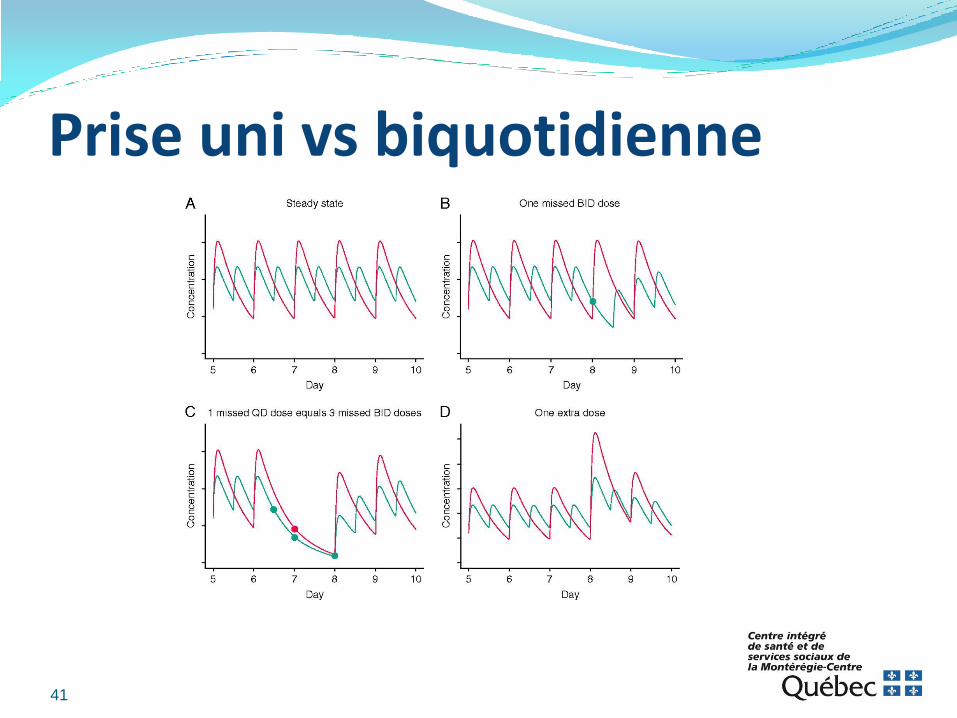
Prise uni vs biquotidienne
41
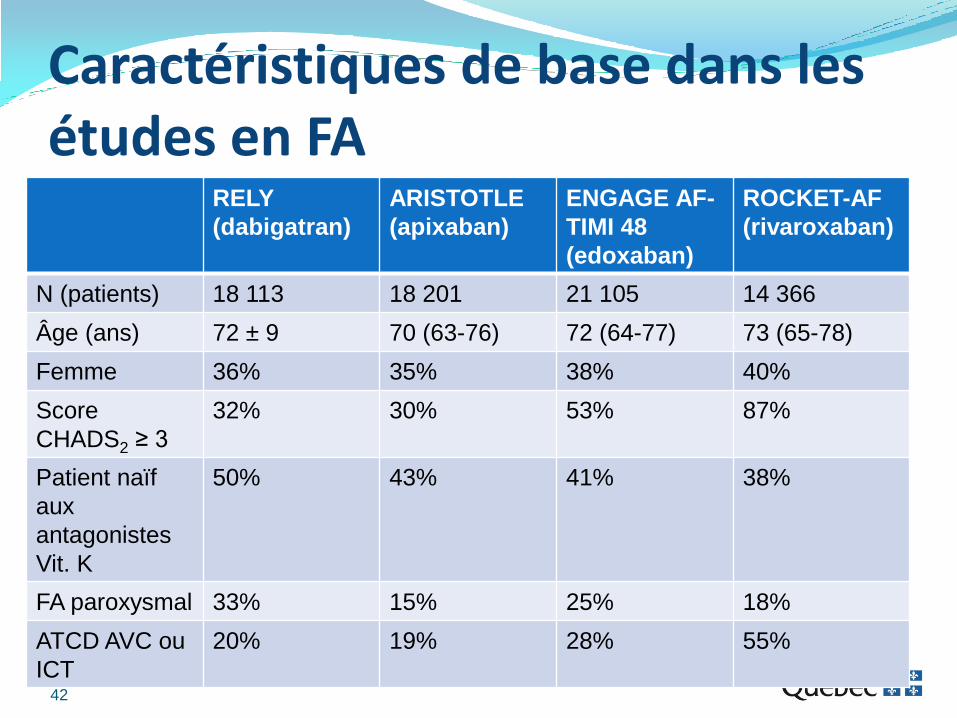
Caractéristiques de base dans les études en FA
RELY
(dabigatran)
ARISTOTLE
(apixaban)
ENGAGE AF-
TIMI 48
(edoxaban)
ROCKET-AF
(rivaroxaban)
N (patients) 18 113 18 201 21 105 14 366
Âge (ans) 72 ± 9 70 (63-76) 72 (64-77) 73 (65-78)
Femme 36% 35% 38% 40%
Score
CHADS2 ≥ 3
32% 30% 53% 87%
Patient naïf
aux
antagonistes
Vit. K
50% 43% 41% 38%
FA paroxysmal 33% 15% 25% 18%
ATCD AVC ou
ICT
20% 19% 28% 55%
42