trimestriel trimestral published by the … · un index des articles est publié tous les deux ans....
TRANSCRIPT
QUARTERLY TRIMESTRIEL TRIMESTRALVolume XIV Number 2 2007
Heal
th S
anté
Sal
ud
ISSN 1025 - 3823
Published by the International Union for Health Promotion and Education
English page 4 – Français page 42 – Español página 53
QUARTERLY
INTERNATIONAL JOURNAL OF HEALTH PROMOTIONAND EDUCATION
TRIMESTRAL
REVISTA INTERNACIONALDE PROMOCIÓN DE LA SALUDY EDUCACIÓN PARA LA SALUD
TRIMESTRIEL
REVUE INTERNATIONALEDE PROMOTION DE LA SANTÉET D’ÉDUCATION POUR LA SANTÉ
COMMUNITY HEALTH PROMOTION:CREATING THE NESSESSARYCONDITIONS FOR HEALTHTHROUGH COMMUNITYEMPOWERMENT AND PARTICIPATION

Promotion & Education, the International Journalof Health Promotion & Education, is an officialpublication of the International Union for HealthPromotion & Education (IUHPE). It is a multilin-gual journal, which publishes authoritative peer-reviewed articles and practical information for aworld-wide audience of professionals interestedin health promotion and health education. Thecontent of the journal reflects three strategic pri-orities of the IUHPE, namely, advancing knowl-edge, advocacy and networking.Promotion & Education publishes four regularissues a year, some of which are focused on spe-cific themes, and a selection of supplement issuesranging in scope and size. Articles are generallypublished in the original language and theabstract is translated in to the other two. Given therelevance of the article, it can also be published inone or two of the other languages than the origi-nal. An index of articles is published every twoyears.The views expressed in articles which appear inthis journal are those of the authors, and do not necessarily reflect those of the IUHPE.Any material published in Promotion & Educa-tion may be reproduced or translated providedcredit is given and copy sent to the address of theJournal.
Article submissionPlease refer to the Author Guidelines on theIUHPE website: www.iuhpe.org. Submissions orqueries on submissions should be addressed byemail to the Managing Editor at:[email protected]
SubscriptionAll members of the IUHPE automatically receivePromotion & Education. It is also available by sub-scription. For readers in Europe, North America,Northern Part of Western Pacific, South WestPacific: Ind. 71 €, Inst. 104 €. For readers in Africa, Eastern Mediterranean,South-East Asia, Latin America: Ind. 37 €, Inst.42 €. Individual copies of current and back issuesmay be ordered for 16 €.
To subscribe to Promotion & Education,write to:
Promotion & Education, la Revue internationalede Promotion de la Santé et d’Éducation pour laSanté, est une publication officielle de l’Unioninternationale de Promotion de la Santé et d’Édu-cation pour la Santé (UIPES). Il s’agit d’une revuemultilingue, contenant des articles de référencesur tous les aspects théoriques et pratiques de la promotion de la santé et de l’éducation pourla santé. Elle s’adresse à un public de profes-sionnels de toutes les régions du monde. Lecontenu de la revue reflète trois des priorités stra-tégiques de l’UIPES, à savoir, développementdes connaissances et compétences, plaidoyerpour la santé, et communication et travail enréseau.Promotion & Education publie quatre numérosréguliers par an, parmi lesquels certains sontconsacrés à des thèmes particuliers, ainsi qu’unesélection de numéros spéciaux de portée et detaille variables. Les articles sont généralementpubliés dans leur langue originale et leurs résu-més, dans les deux autres langues. Ils peuventaussi, en fonction de leur pertinence, être publiésdans l’une ou bien dans les deux autres langues.Un index des articles est publié tous les deux ans.Les opinions exprimées dans les articles de cetteRevue sont celles des auteurs et ne sont pasnécessairement celles de l’UIPES.Toute reproduction ou traduction des textes parusdans Promotion & Education est autorisée sousréserve de la mention de la source et de l’envoid’une copie à l’adresse de la Revue.
Soumettre un articlePour cela, référez-vous aux Directives pour lesAuteurs sur le site web de l’UIPES : www.iuhpe.orgLes soumissions ou les questions à propos dessoumissions doivent être adressées par e-mail àla Coordinatrice éditoriale : [email protected]
AbonnementTous les membres de l’UIPES recoivent automa-tiquement la revue Promotion & Education, et elleest aussi disponible par abonnement. En Europe,Amérique du Nord, Pacifique Occidental Nord, et Pacifique Occidental Sud : Ind. 71 €, Inst.104 €. En Afrique, Méditerranée Orientale, Asiedu Sud-Est, et Amérique Latine : Ind. 37 €, Inst.42 €. Il est possible de commander des numé-ros individuels de la revue : 16 € par numéro.
Pour s’abonner à Promotion & Education,veuillez contacter :
Promotion & Education, la Revista Internacionalde Promoción de la Salud y Educación para laSalud es la publicación oficial de la Unión inter-nacional de Promoción de la Salud y Educaciónpara la Salud (UIPES). Es una revista que incor-pora artículos revisados por una junta editora e incluye información práctica dirigida a unaaudiencia de profesionales interesados en loscampos de la promoción de la salud y educaciónpara la salud a nivel mundial. El contenido de larevista refleja las tres prioridades estratégicas dela UIPES, a saber, desarrollo de conocimientosy capacidades, argumentación en favor de lasalud y fortalecimiento de los intercambios y deltrabajo de redes.Promotion & Education publica cuatro númerosal año, alguno de ellos dedicados a temas espe-cíficos, y varios números extraordinarios cuyoalcance y tamaño varían. Por regla general, sepublican los artículos en el idioma original y unresumen de los mismos traducido los otros dos.Dependiendo de la relevancia del artículo, tam-bién es posible publicarlo en uno o dos idiomasmás, aparte del original. Cada dos años sepublica un índice de los artículos publicados.Las visiones y opiniones expresadas en la revistapor los autores de los artículos no reflejan nece-sariamente la visión institucional de la UIPES.Todo material publicado en la Revista Promotion& Education que sea reproducido o traducidodeberá ofrecer crédito a la revista y deberáenviarse copia a la dirección de la revista.
Solicitud de publicaciónde artículosLe rogamos lea las Instrucciones para los autoresen la web de la UIPES: www.iuhpe.org. Las solic-itudes o preguntas acerca de la publicación deartículos en la revista deberán dirigirse por correoelectrónico a la Coordinadora editorial a:[email protected]
SuscripciónTodos los integrantes activos de la UIPES reci-ben una copia de la revista como beneficio de sumembrecía a la organización. La revista tambiénestá disponible mediante suscripción. Para loslectores de Europa, Norteamérica, Pacífico occi-dental norte y Pacífico occidental sur, el precio dela revista es : Ind. 71 €, Inst. 104 €. Para los lecto-res de Africa, países del Mediterráneo oriental, delSureste de Asia y de América Latina, el precio dela revista es : Ind. 37 €, Inst. 42 €. Es posible soli-citar copias individuales de los números actuales yanteriores a precio de 16 € .
Para suscribirse a Promotion & Education,contactar :
42, boulevard de la Libération– 93203 Saint-Denis Cedex – France.Tel: +33 1 48 13 71 20 – Fax: +33 1 48 09 17 67 – E-mail: [email protected]
Founding Editor – Fondatrice – Fundadora:Annette Kaplun • Director – Directeur:Pierre Arwidson • Editorial Advisory Board–Conseil de Rédaction – Consejo Editorial:Hiram Arroyo (Puerto Rico), Dora Cardaci(Mexico), Juan-Manuel Castro (Mexico), ShaneHearn (Australia), Lloyd Kolbe (USA),Balachandra Kurup (India), Diane Levin (Israel),Gordon MacDonald (United Kingdom), DavidMcQueen (USA), Maurice Mittelmark (Norway),David Nyamwaya (Kenya), Michel O’Neill(Canada), Mihi Ratima (New Zealand), IrvingRootman (Canada), Becky Smith (USA), AlysonTaub (USA), Thomas Karunan Thamby (India),Keith Tones (United Kingdom), Pat Youri (Kenya)• Executive Editorial Board – Comité deRédaction – Comité Editorial : Editor in Chief - Rédactrice en Chef – Jefade redacción : Jackie Green • ManagingEditor – Coordinatrice éditorial –Coordinadora editorial : Martha Perry • Editorial assistant – Assistante de larédaction – Ayudante de la redacción: ClaraRachel Casseus-Eybalin • Translators –Traducteurs – Traductores: Marie-ClaudeLamarre, Ma. Asunción Oses, Martha Perry,Marie-Cécile Wouters • Graphic Design –Conception Graphique – Diseño gráfico:Frédéric Vion (01 40 12 27 41) • Printer –Imprimeur – Impresor: Imprimerie Landais –93160 Noisy-le-Grand (01 48 15 55 01)Commission paritaire n° AS 64681 du 14-09-8 Contributors – Contributeurs –Contribuidores: Mia Gardiner, Louise M.Gobron, Brick Lancaster, Philippe Lorenzo,Valéry Ridde, David A. Sleet

English section
Editorial Community Health Promotion- a step furtherS. Nishtar
Advancing KnowledgeReducing social inequalities in health: public health, community health or health promotion?V. Ridde
Lessons learned from the application of a participatory evaluation methodology to Healthy Municipalities, Cities and Communities Initiatives in selected countries of the AmericasM. Rice and M. C. Franceschini
Current health promotion practices in communities
AsiaAparajita OrissaA.Mukhopadhyay
Shejar KhojA. Mukhopadhyay
AustralasiaReorienting health services through community health promotion in Kwaio, Solomon IslandsE. Kekeubata and D. MacLaren
The Graniators support group programE. Sullivan and A. S. Duncan
Latin AmericaMotuca healthy municipality project: building together a better futureR. Mendes and F. Falvo
Empowered women from rural areas of Bolivia promote community developmentR. Ríos, C. Olmedo and L. Fernández
Promoting health and happiness in the Brazilian AmazonC. Scannavino and R. Anastacio
AdvocacyAdvocacy for appropriate health policy and effective health systemA. Mukhopadhyay
Cracking the nut of health equity: top down and bottom up pressure for action on the social determinants of healthF. Baum
Criteria and checkpoints for better community health promotionJ. E. Ritchie
Advocacy in actionCommunity health promotion in Pakistan: a policy development perspectiveK.A. Ronis and S. Nishtar
Abstracts
Showcasing networksNetwork of healthy communities of Rio de Janeiro, BrazilD. Becker et al.
Development of healthy cities networks in EuropeE. Goepel
EQUINET: Networking for equity in health in east and southern AfricaR. Loweson
Global equity gauge allianceA. Ntuli
Abstract
Contents – Sommaire – ÍndiceVolume XIV Number 2 2007

Dossier français
Editorial La Promotion de la santé communautaire- un pas en avantS. Nishtar
Développement des connaissancesRéduire les inégalités sociales de santé : santé publique, santé communautaire ou promotion de la santé ?V. Ridde
Abstracts
PlaidoyerDu témoignage au plaidoyer : l’expérience d’une ONG humanitaire
J. Ancien
Abstracts
Travail en reseauLe Réseau québécois des Villes et Villages en santé : un mouvement fort confronté à de nouveaux défisP.Simmard
Abstracts
Cuaderno español
Editorial La promoción de la salud comunitaria: un paso másS. Nishtar
Desarrollo de conocimientosResúmenes
AbogacíaEl Parque Saludable: una experiencia de prevención y promoción de la salud a nivel comunitario en un barrio marginal de laselva del Perú E. Peñaherrera Sánchez y W. Palomino
Resúmenes
Redes comunitariasResúmenes
Contents – Sommaire – ÍndiceVolume XIV Number 2 2007

5IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 2 2007
Editorial
This themed issue of Promotion & Edu-cation has received financial support fromthe United States’Centers for Disease Con-trol and Prevention (CDC), an Agency of theDepartment of Health and Human Services,under the Cooperative Agreement NumberU50/CCU021856 on Global Health Promo-tion and Health Education Initiatives. Theideas expressed in the articles are those ofthe authors and do not necessarily repre-sent those of the CDC and the IUHPE.
Community health promotion is ofstrategic significance in contemporaryhealth systems. The overarching context ofthis stems from the inability of most coun-tries with mixed health systems to deliverhealth as a public good; this coupled withthe emerging role of the market in healthand resource constraints at the social sec-tor level, particularly in the developingcountries, necessitate a visible role of thecommunities in health promotion in orderto achieve the equity objective in health.However, in contrast to its significance,community health promotion remains apoorly understood concept, which makesit difficult to advocate it to policy makers.These considerations therefore led theGlobal Consortium on Community HeathPromotion, after its creation in 2003 as a col-laborative initiative of the US Centers forDisease Control and Prevention (CDC) andthe International Union for Health Promo-tion and Education (IUHPE) to focus onbringing clarity to concepts and norms asa starting point for the scope of its work; andit is within this context, and as a step in thisdirection, that this special issue has builtfurther on the Statement of the Consortium(Nishtar et al., 2006).
The issue covers many aspects of com-munity health promotion from the elabo-ration of its interface with the principles ofequity and considerations of populationhealth to spot-lighting a series of case-stud-ies to enable a better understanding of whatcommunity health promotion involves andhow participatory empowering method-ologies can be used to harness communityassets and why. In addition, the issue alsofeatures articles of practical relevance withrespect to assisting countries and practi-tioners to examine whether their generalactivities in specific projects meet currentstandards of good community health pro-
motion practice, and providing guidance onparticipatory evaluation.
The Consortium’s Statement on whichthis issue further builds, defines commu-nity health promotion as a participatoryempowering equity focused process – onethat regards community participation asbeing essential to every stage of health pro-moting actions as well as one that leveragescommunity assets and knowledge to createthe necessary conditions for health. How-ever, as outlined by Rice in this issue (2007;p.), not all health promoting policies andactions conform to this definition. Theauthor uses lessons learnt from the appli-cation of participatory evaluation method-ologies to Healthy Municipalities, Cities andCommunities (HMC) Initiatives in selectedcountries of the Americas to highlight thepoint showing that most HMC initiativeshad not appropriately taken into accountkey health promotion principles, such asintersectoral collaboration and communityparticipation. The article by Baum delvesdeeper into the issue enabling an under-standing of the implications of not doing soby referring to the Ottawa Charter-gal-vanised health promoting policies andactions in Australia (2007; p.); these haveled to a significant impact at the populationlevel across a range of health outcomes, buthave remained unsuccessful in addressinginequities and reducing the existing gradi-ents. Such experiences underscore theneed to design health promotion policiesand actions with a strong equity lens, andit is here that the need to combine top-downpolitical commitment and policy actionwith bottom-up action from communitiesand civil society groups referred to byBaum in her article as the ‘Nutcracker effectfor health equity’, assumes importance.
Understanding the role of the communi-ties is therefore critical to health promotion.Within this context, a number of case stud-ies have been featured in this special issuefrom diverse developing country back-grounds to showcase relevant approaches.Each study used a structured format to high-light both the intervention as well as the les-sons that can be extrapolated from the expe-rience for wider application. Weaknesses intheir design and evaluation methodologiesnotwithstanding, the case studies yieldimportant process-related lessons.
Firstly, the collective message empha-sises the importance of understanding theentire process of community project man-agement and its instruments. Foremost isthe need to engage all development actorsin a locally-suited participatory model forplanning and governance; these includelocal government bodies, NGOs, interna-tional development partners, formallyestablished community organizations, localleadership and inter-community federa-tions. Participatory governance with a role,both for the public sector as well as thecommunities is relevant not only to the sus-tainability of grass roots initiatives, but alsoenables transferring successful social tech-nologies to other settings and the adoptionand integration of programmes as publicpolicies.
Secondly, the case studies bring to theforefront many considerations that shouldbe taken into account while structuringcommunity initiatives; these include gar-nering participation and ownership at allsteps; ensuring that voices are heard; fos-tering a sense of cohesion; ensuring that les-sons learnt are factored into decision mak-ing; allowing for flexibility with programdesign so that it can be shaped by locally rel-evant evidence as it emerges during thecourse of interventions; encouraging self-management and social control; using cul-turally appropriate and locally validatedtools of intervention and paying due atten-tion to the empowerment of women in deci-sion-making. These are regarded as beingimportant to the sustainability of grass rootsinterventions in general. More specifically,however, these also enable overcoming reli-gious, cultural and ancestral barriers toaccessing healthcare as is shown by thecase study from the Solomon Islands(MacLaren & Kekeubata, 2007; p.); in addi-tion, they can also assist in fostering theempowerment of the most isolated and dif-ficult to access groups, as is shown by theexample of the forest peoples, or the ‘cabo-clos’, in Brazil who live in rural, often iso-lated and difficult to access areas of theAmazon (Scannavino & Anastácio, 2007; p.).
Thirdly, most examples highlight theneed for intersectoral action within thelarger framework of social sector develop-ment rather than within the domain ofhealthcare. Examples of health interven-
Community Health Promotion – a step furtherSania Nishtar1,2
1. Guest Éditor2. SI, FRCP, Ph.D; Founder and President, Heartfile, Pakistan. Correspondence to: [email protected]

Editorial
tions cited herein have garnered supportfrom across various sectors such as hous-ing, education, youth services, and foodsecurity agencies rather than conventionalhealth systems to improve health out-comes. A local perspective within an inter-sectoral scope can also flag locally specificopportunities for health promotion; forexample, the case history from Orissashows that disaster proneness is one of thestrongest determinants of death and dis-ability in the cited region of India; the pre-dictability of disaster in this area thereforewarrants institutional capacity strengthen-ing for relief and rehabilitation operationsrather than the traditional public healthinterventions (Mukhopadhyay, 2007; p.).
And finally the case studies allude to thepotential value of networking both globallyin terms of promoting values of equity andsocial justice in health by facilitating shar-ing of experiences across countries, as inthe case of EQUINET (Loewenson, 2007; p.)as well as enhancing peoples’power overtheir health and well-being in local com-munity settings as was shown for the ‘Gra-niators’in Australia (Sullivan et al. p.).
The articles featured herein yield use-ful lessons for fostering community healthpromotion. Evidence of the effectiveness ofsuch initiatives underscores the need tomove beyond pilot and demonstration proj-ects to mainstream the participation androle of communities for improving healthacross a range of outcomes (IUHPE, 2000).This necessitates a range of complex inter-dependent actions and requires goingbeyond increasing the voice of communi-ties and frontline health workers tostrengthening the social policy fabric, shap-ing social welfare and health financingarrangements and moulding the regulatoryenvironment within country settings.Within the health sector, this also necessi-tates a number of other overarching meas-ures, such as, redistributing health budgetsfrom tertiary care to prevention and healthpromotion, and addressing budgetary andhealth personnel deployment imbalancesin favour of rural, informal urban and pri-mary care infrastructure and services.Existing and evolving public health pro-grammes present an opportunity, whereprevention, control and health promotioncan be integrated as was shown for the non-communicable diseases initiative in Pak-istan (Ronis & Nishtar, 2007; p.).
However, sustainable engagement ofcommunities in mainstream healthcare ismost feasible in countries with systems ofgovernance which involve decentralizationof administrative and political power to thelowest administrative units, such as munic-ipalities. These structures have institutionalmandate and responsibility for engaging
communities and channeling inputs bydevelopment actors to local developmentplans. The local government perspectivecan also enable the tying in of health inter-ventions to over-arching developmentgoals, cross-linking these with initiatives forlivelihood support, education, savings andcredit, given that these are critical to theprocess of development in general at thegrass roots level.
Spurring action at a social sector levelwithin countries along these lines is a pre-rogative of state institutions; however, mul-tilateral development initiatives such as theWHO’s Commission on the Social Determi-nants of Health can provide an impetus par-ticularly through WHO’s leverage in morethan 190 countries to encourage govern-ments to make public policy choices organ-ized around the active participation andinvolvement of communities as outlined inthese approaches. A strong state and pub-lic sector in health is important to improvepopulation health equitably – both by deliv-ering public good as well as regulating theprivate market and the role of communitiescan be critical to the success of both.
ReferencesBaum, F. (2007) “Cracking the nut of health equity:
top down and bottom up pressure for action onthe social determinants of health” Promotion &Education, XIV (2):
IUHPE (International Union for Health Promotion andEducation) (2000). The Evidence of healthpromotion effectiveness: Shaping Public Healthin a New Europe. A report for the EuropeanCommission. Paris: Jouve Composition &Impression.
Loewenson, R. (2007) “EQUINET: Networking for equity in health in east and southern Africa”Promotion & Education, XIV (2):
MacLaren, D. and Keukubata, E. (2007) “Reorientinghealth services through community healthpromotion in Kwaio, Solomon Islands” Promotion& Education, XIV (2):
Mukhopadhyay, A. (2007) ëAparajita Orissa” Promotion & Education, XIV (2):
Nishtar, S., Perry, M., Lamarre, M. C., Ritchie, J., et al.(2006) “Statement of the Global Consortium onCommunity Health Promotion.” Promotion &Education, XIII (1):7-8.
Rice, M. and Franceschini, C. (2007) “Lessons learned from the application of a participatoryevaluation methodology to Healthy Municipalities,Cities and Communities Initiatives in selectedcountries of the Americas” Promotion &Education, XIV (2):
Ronis, K.A. and Nishtar, S. (2007) “Community Health Promotion in Pakistan: a policydevelopment perspective” Promotion &Education, XIV (2):
Scannavino, C. and Anástacio, R. (2007) “Promotinghealth and happiness in the Brazilian Amazon”Promotion & Education, XIV (2):
Sullivan, E. et al. (2007) “The Graniators support group program” Promotion & Education, XIV (2):
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 20076

7IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 2 2007
Advancing knowledge
There has been much debate aroundthe definition of health practices. Someauthors have referred to vague and fluctu-ating definitions (Gagnon & Bergeron, 1999,p. 257), whereas others have managed toturn this controversy into a research area inand of itself (Fassin, 2000a). According toBourdieu (2001), it is perfectly normal forscientists working in the same field ofknowledge to be in perpetual disagreement.Traditionally, a dichotomy persists inexpert opinion discourse between publichealth and community health, with the for-mer being considered older than the latter.Health promotion emerged more recently,carrying a formal status since 1986. Addi-tionally, three expressions are commonlyemployed to describe health interventions:public health, community health, andhealth promotion.
Upon being invited to contribute to thisspecial issue on community health promo-tion, the author’s immediate reactions weretwo-fold. First of all, there was a desire todiscover how the Consortium managed todefine this new concept. The answer can befound at the beginning of this issue,although the communiqué issued by theConsortium at the beginning of 2006(Nishtar et al., 2006) still leaves one per-plexedi, and makes the present article allthe more pertinent. Secondly, the authorquestioned the relevance of introducing anew definition for health interventions,since no one has yet really succeeded indefining the three processes that alreadyexist. Introducing a new concept without
having ever really succeeded in clarifyingolder ones puts us at risk of being subjectedto critics’accusations, branded as ‘wind-bags’ (Fassin, 2000a, p.71). It can also leadto more confusion than clarification, as wasthe case in Canada when the term ‘popu-lation health’first appeared. The objectiveof this article is, therefore, to attempt to dif-ferentiate the three types of health prac-tices generally encountered in the literatureand in the field, in order to situate the term‘community health promotion’and demon-strate that health promotion must take thelead in the fight against social inequalitiesin health.
An attempt to differentiatepracticies:
Following the example of Rootman et al.(2001), it was considered useful whenattempting to establish definitions to dis-tinguish between the process and the goalof a practice. Examples drawn from theauthor’s personal experiences and knowl-edge of Canadian, French, and African prac-tices are used to support the arguments pre-sented here.
End Goal:
Public health and community healthgenerally share a common goal: improvingthe health status of people, taken as a groupand not individually. Many examples couldbe given of public policies from around theworld that share this objective. Curiously,and since it is rare enough to merit specificattention, the first health policy of Quebec
Reducing social inequalities in health: public health,community health or health promotion?Valéry Ridde1
Abstract: While the Consortium on’Community Health Promotion’is suggesting a definition of this new concept to qualify healthpractices, this article questions the relevance of introducing such a concept since no one has yet succeeded in really differenti-ating the three existing processes: public health, community health, and health promotion. Based on a literature review and ananalysis of the range of practices, these three concepts can be distinguished in terms of their processes and their goals. Publichealth and community health share a common objective, to improve the health of the population. In order to achieve this objec-tive, public health uses a technocratic process whereas community health uses a participatory one. Health promotion, on the otherhand, aims to reduce social inequalities in health through an empowerment process. However, this is only a theoretical defini-tion since, in practice, health promotion professionals tend to easily forget this objective. Three arguments should incite healthpromoters to become the leading voices in the fight against social inequalities in health. The first two arguments are based onthe ineffectiveness of the approaches that characterize public health and community health, which focus on the health system andhealth education, to reduce social inequalities in health. The third argument in favour of health promotion is more political innature because there is not sufficient evidence of its effectiveness since the work in this area is relatively recent. Those respon-sible for health promotion must engage in planning to reduce social inequalities in health and must ensure they have the meansto assess the effectiveness of any actions taken. (Promotion & Education, 2007, (2): pp)
Key words: social inequalities in health, public health, community health, health promotion, definition
1. Unité de Santé Internationale, Faculty of Medicine, University of Montreal. Correspondence to: Valéry Ridde, 3875, Saint Urbain St., Montreal, QC, Canada, H2W1V1 ([email protected])
(This article was commissioned from the author on July 3rd, 2006. Following peer review it was accepted for publication on February 1st, 2007.)
KEY POINTS
• Health promotion’s objective to reducehealth inequalities and the process ofempowerment distinguish it from pub-lic health and community health.
• Health promotion professionals mustengage in planning to reduce socialinequalities in health and ensure theyhave the means to assess their effec-tiveness.

Advancing knowledge
had a similar goal; however, it was framednegatively: the policy proposed 19 objec-tives to “reduce health problems” (Mini-stère de la santé et des services sociaux,1992). This was later revised based onnational public health priorities to “makesubstantial gains in health matters” (Mini-stère de la Santé et des Services sociaux,1997), which serves as a reminder of thedebate on the ‘positive’ versus the ‘nega-tive’ definitions of the concept of health.
The definition traditionally found in pub-lic health training manuals followsWinslow’s proposal from 1920 and definespublic health as the art and science of pro-moting health, preventing disease and pro-longing life (Fournier, 2003). This article,however, advocates a definition that goesbeyond the famous three ‘Ps’and focusesmore on process than on the goals of pro-motion, prevention and protection, whichwere the foundation of public health prior-ities in Quebec from 1997 to 2002. Thus,more in-depth reflection on the teleologicallevel is needed in order to understand theultimate purpose of health promotion activ-ities. A real paradigm shift is boldly pro-posed by affirming that health promotionseeks not only to improve the health of thepopulation, but above all to reduce the gapsin the health status among population sub-groups. Indeed, the Ottawa Charter statesthat, “Health promotion focuses on achiev-ing equity in health. Health promotionaction aims at reducing differences in cur-rent health status” (OMS, 1986). This para-digm shift also makes it possible to differ-entiate health promotion from previousendeavours to establish definitions, sinceConill and O’Neill (1984) proposed theobjective of community health to be theimprovement in the health status of thepopulation, making no mention of socialinequalities in health. This distinctionseems essential, since most interventionsthat do not specifically aim at reducing dis-parities almost always end up aggravatingthem, even when the goal of improving thehealth of the population is achieved(Fassin, 2000b, p. 33). This was the case forthe residents of Montreal (Lessard, 2003).Adopting this definition means questioningbeliefs, which are a central notion in theKhunian concept of a paradigm. Health pro-
motion is thus conceived as an undertakingwhose ultimate purpose is social change.If a new ‘new public health’ (Horton, 1998)needs to be created in order to achieve this,then so be it. Perhaps this may not be nec-essary, as will be explained below, since theOttawa Charter of the new public healthalready contains the objective of reducinginequalities.
Process:
In contrast to the view of Conill andO’Neill (1984) who believe that communityhealth can have two poles, one technocraticand the other participative, the authormaintains that these two poles actually con-stitute the distinction between the imple-mentation process in public health and theone in community health. The process ofimplementing public health interventionsseems to correspond to a technocratic top-down approach. If public health stake-holders agree with their counterparts incommunity health on, for example, encour-aging individuals to change their lifestylesor behaviour, the former will use morecoercion than the latter in attempting toachieve this change. Terms such as ‘risk fac-tor’and its corollary ‘victim blaming’(Lup-ton, 1995) are characteristic of publichealth, where the health system, healtheducation and prevention are the biggestbudget recipients. In France, the history ofpublic health (Abenhaim, 2003), as well asthe quarrels about the creation of theNational Institute for Prevention and HealthEducation (INPES), and the recent legisla-tion in 2004 on public health, are all veryindicative of this approach, which is cen-tred on prevention and the health care sys-tem, and is run by a centralized or decen-tralized administration. Epidemiology andan evidence-based approach are the cardi-nal tools of public health, with physiciansoccupying a central place in the system.There are some authors who directly referto the work of Weber and even maintainthat the only authority really known to pub-lic health is rational-legal, based on law (Jaf-fré & Olivier de Sardan, 1999, p. 364).Regardless of whether this is representativeof the history of public health, Fassin’sanalysis (2006) of the “double model of con-straint and normalization, authoritarian
control and moralizing intervention» inSouth Africa is the technocratic processparagon since «on many occasions publichealth has served the racist political proj-ect of South African authorities” (p.211). InAfrica, health promotion is a relativelyunknown concept (Nyamwaya, 2005); pub-lic health has the monopoly on words andpractices for numerous reasons whichwould take too long to explain here (Ridde& Seck, 2006).
Community health practitioners, on theother hand, place population participationat the centre of their interventions and theemic point of view is supported. Certainhealth centres in the United States were pio-neers in community medicine practices inNorth America in the 1960s (Lefkowitz,2007), as were those of social medicine incertain health centres in South Africa in the1940s (Fassin, 2006). There is recognition ofthe relationships between certain individ-ual practices and the triggering of particu-lar pathologies. At the same time, emphasisis placed on understanding the social andstructural conditions that can give rise tosuch practices. Members of the communityparticipate in defining the problem, findingsolutions and implementing them. Epi-demiology and statistical tools are notignored, but they are not the only methodsused, and the epistemological approach ismore constructivist. Planning models usingthis triangulation of methods (Green &Kreuter, 1999), such as the model appliedin Quebec from 1980-90 (Bergeron &Gagnon, 1994), and the one in Belgium(Bantuelle et al., 1998), are good examplesof the community health process.
Health promotion interventions arebased directly on the approach outlined inthe Ottawa Charter. Actors thus attempt toimplement a process that provides popu-lations with the means to ensure greatercontrol over and improve their own health(OMS, 1986). This is the concept of ‘empow-erment’, which is a guiding value in healthpromotion but will not be discussed herefor reasons of spaceii. Empowermentactions and interventions appear to pro-duce highly effective results in healthimprovement (Wallerstein, 2006). Evi-dently, this approach has its critics; in Lup-ton’s view (Lupton, 1995, p.60), the rheto-ric of empowerment serves to obscurepublic health professionals’investment andinterventions by persuading certain groupsto develop their competencies and exercisecontrol over their lives.
The attempt to differentiate these threetypes of practice is summarized in Table 1-again, this is only an attempt. The distinc-tions must not be perceived as being set instone and these characteristics are onlyhighlighted a priori in order to force the
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 20078
Process End Goal
Public health TechnocraticImprove population health
Community health Participatory
Health promotion Empowerment Reduce social inequalities in health
Table 1. Attempt to differentiate public health, community health, and healthpromotion
Source: Author

traits necessary for creating a Weberianideal type.
Health promotion must addresssocial inequalities in health3
In 1988, the Director General of the WHOwas already concerned that, “public healthhas lost its original link to social justice,social change and social reform” (Hancock,Labonte et al., 1999). Twenty years later, thisfact remains the same. Furthermore, healthpromotion must recover its original roleand challenge social inequalities in health.Stakeholders need to understand thathealth planning is not simply a technicalexercise, but can also be a tool for bringingabout social change. This responsibility foraction and advocacy must be entrusted tothose in the field of health promotion.Besides the fact that public health practice,which is several centuries old, has not beenable to eliminate the inequalities in health4
that persist to this day (Mackenbach, 2005)– and which have been measured statisti-cally ever since the 17th Century – threearguments, among others, may be used tosupport this case. The first two argumentsare based on the ineffectiveness of theapproaches that characterize public healthand community health, i.e. actions gener-ally centred on the health system andhealth education, for which effects are nowwell-known. The last argument in favour ofhealth promotion is more political in naturesince there is not yet sufficient evidence ofits effectiveness, due to the fact that work inthis area is very recent (Hills, Carroll et al.,2004).
The Health System:
For a very long time, and even today,people have believed that the health sys-tem is able to improve the health of the pop-ulation and reduce disparities in mortalityrates among sub-groups. The former FrenchMinister of Health thought that the duty ofpublic health basically involved nothingmore than modernizing the organization ofhealth services (Mattei, 2002). Section 2 ofthe Public Health Act, promulgated inFrance in 2004, states that the reduction ofinequalities in health may be achievedthrough health promotion and by develop-ing access to care and to diagnostics
Advancing knowledge
9IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
throughout the country, which no doubtexplains why 97% of the health budget isallocated to the care system (Abenhaim,2003). Budget allocation is not any betterin Quebec. The expression ‘health promo-tion’only appears in French legislationtwice: in the above-mentioned section andas a reminder of the mission of the INPES;the latter mention, however, has notresulted in the word ‘prevention’beingreplaced by’promotion’in the name of thispublic entity. According to Frenchresearchers, health policy essentially viewsthe reduction of social inequalities in healthin France from the angle of primary accessto care (Pascal, Abbey-Huguenin et al., 2006,p.118).
Nevertheless, numerous studies haveshown that if the health system and medi-cine can have an effect on the health of indi-viduals needing care, they have no or verylittle effect on population health. Due to lackof space, this subject cannot be developedhere, but readers are referred to the clas-sic references on the topic (McKinlay &McKinlay, 1977; Ashton et Seymour, 1988).Furthermore, the health system and medi-cine can also have harmful effects on thehealth of individuals. In France alone, it isestimated that 18,000 people die each yearfrom the side effects of medication (Aben-haim, 2003). In the United States, medicalerrors cause 98,000 deaths annually (Insti-tute of Medicine, 2000).
Given the limited evidence of the healthsystem’s effects on the population, whatevidence is there that the system reducessocial inequalities in health? Although workon this topic is rare, recent research carriedout in the province of Manitoba in Canadasheds some light on the subject. As is thecase elsewhere in Canada, the health sys-tem in Manitoba is largely funded andadministered by the public sector. A studyon the data of the hospital use from 1986 to1996 seems to show an equitable health sys-tem usage since the poorest, who a priorihave the greatest needs, spent 40% moredays in hospital and represented 30% moreof hospital admissions than the richest.This difference in use, which favoured thepoorest, remained constant over a periodof ten years. However, examining the dis-parities in mortality rates for this same
period shows that, not only does the situa-tion remain unfavourable for the poorest,but the gap has widened to their detriment(Table 2). In other words, although healthsystem usage has been equitable (in termsof need, rare evidence contradicts the«inverse care law»), social inequalities inhealth have not been reduced. There wasalso evidence that a 40% reduction in hos-pital beds has had no effect on populationmortality indicators.
Health Education:
The second argument concerns theimpossibility for health education alone tosuccessfully reduce social inequalities inhealth. Raising this issue is especially cru-cial for France and the United States, wherehealth education continues to play a dom-inant role in overall health strategies(O’Neill & Stirling, 2007). Developing inter-ventions that reduce inequalities in healthwould be no mean feat, and it could even beclaimed that this would constitute a logicalcontradiction. Rose (1985) explains theimportance for prevention activities to tar-get the population as a whole rather thanjust high-risk groups. He maintains thatwhen a risk factor is normally distributed ina population, reducing its influence willbring about greater change in the generalhealth status of the population than if inter-ventions are solely directed at high-riskgroups. Conversely, to complicate matterseven further, it is a known fact that wheninterventions targeting harmful healthbehaviours are directed at the populationas a whole, these interventions appear tohave a much greater impact on the mostfavoured social groups (Whitehead, 1995),thus contributing to increasing inequalities.Some specialists transpose Rose’s propo-sitions to social inequalities in health (Dou-glas & Scott-Samuel, 2001; Marmot, 2001).For these experts, the determinants of indi-vidual differences are dissimilar from thedeterminants of disparities among popula-tion sub-groups. Targeting interventions toincrease average life expectancy or toreduce disparities therefore remains tricky.Based largely on English research findings,Paquet and Tellier (2003) affirm that, evenif the whole population adopted healthylifestyle habits, overall life expectancywould increase, but the health gradientamong social classes would still persist. Insummary, on the one hand, in order forhealth education to be effective, it is betterto act on the population as a whole in orderto improve overall population health; this,however, carries the risk of increasinginequalities. On the other hand, interven-tions targeted directly at individuals or cer-tain sub-groups, rather than at the overallpopulation, can provoke increased feelings
Indicators 1986 1996
Number of days in hospital 1.40 1.38
Admission rate to hospital 1.31 1.32
Mortality rate from all causes 1.21 1.42
Pre-mature mortality rate 1.39 1.85
Table 2. Inequalities in the use of the health system and mortality in Manitoba,Canada
Source: Adapted from Ross et al. (2005)

IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 2 200710
Advancing knowledge
of exclusion and there are high risks ofstigmatization.
Health Promotion:
The third argument for reducing socialinequalities in health through health pro-motion is more political in nature than thetwo preceding arguments. The argument isinextricably linked to the commitment ofstakeholders working in the field of healthpromotion. The ineffectiveness of publichealth and community health in reducingdisparities in health can be partly explainedby the fact that neither one has been willingto take up this challenge, whereas the newpublic health has boasted of its novelapproach in taking all health determinantsinto consideration. Fassin argues about theexisting difficulty getting beyond the rheto-ric and refers somewhat harshly to wind-bags who do nothing (2000). According toGepkens and Gunning-Schepers (1996),interventions which were meant to reduceinequalities in health tended to be basedmore on the traditional and reductionistapproaches of health education than onnewer proposals of holistic action based onthe five pillars of health promotion. Now,almost twenty years later, health promotionmust reclaim its original role and becomea catalyst for raising questions about thepermanence and invisibility of socialinequalities in health, at least in France,claims Drulhe (2000). It appears that thismoral and ethical necessity is not yet reallybeing taken seriously (De Koninck &Fassin, 2004; Ridde, 2004a, 2004b; Bernier,2006). This would explain why publichealth and community health still takeprecedence over health promotion, as isevidenced by the call for experts of theFrench Public Health High Commission,which excludes specialists in health pro-motion.
Why should health promotion bear theburden of redressing inequalities in healthinstead of public health or communityhealth? Simply because the field of healthpromotion has judiciously ensured that ithas a charter which includes this objective,whereas the other two fields do not. In the1978 Declaration of Alma-Ata, inequalitiesin health were formally acknowledged, buttheir reduction was not an essential objec-tive: “Attainment of the highest possiblelevel of health” (Section 1) was affirmed,but not the reduction of inequalities inhealth (WHO, 1978). In contrast, the OttawaCharter affirms that, “Health promotionaction aims at reducing differences in cur-rent health status” (OMS, 1986). Thisrequires implementation of a process ofequity and social justice, one of the six prin-ciples underlying health promotion initia-tives (Rootman, Goodstadt et al., 2001). One
of the documents produced by WHOEurope, as part of the preliminary reflec-tions on the Ottawa Charter, clearly stipu-lates that reducing inequalities is an integralobjective of health promotion. A Europeantask force recently studied the question ofhealth promotion interventions that areeffective in reducing health inequalities,taking for granted that this is the role ofhealth promotion (VIG & ENHPA, 2001).
Attributing this role to health promotionappears to correspond to its mandate ofsocial change and strengthening citizenpower to take action on the determinants ofhealth, especially when it is conceded thathealth inequalities are the result of socialand political structures. However, this doesnot mean that health promotion activitiesmust all be held responsible for reducingdisparities in health; that is not an easy task.Through advocacy and the capacity toinfluence healthy public policy, health pro-motion must take leadership to advanceequity in health.
Conclusion:This attempt at differentiating the three
types of practice serves to underline thevital role of health promotion in reducingsocial inequalities in health through the car-dinal value of social justice and the use ofempowerment as a fundamental process.From a practical point of view, this meansthat questions need to be raised in twoareas. Firstly, health promotion plannersmust now examine the objectives they setto ensure these objectives are not aimedonly at improving the overall health of thepopulation. At best, this only replicatesinequalities and, at worst, it exacerbatesthem. Secondly, once the objective hasbeen reviewed and the actions initiated,there is a need to gather and evaluate theevidence of their effectiveness in reducingsocial inequalities in health; this will inresult open new theoretical, conceptual,and practical fields of work (Ridde,Delormier et al., 2007).
References:Abenhaim, L. (2003). Canicules. La santé publique
en question. Paris, Fayard.Ashton, J. et H. Seymour (1988). The new Public
Health. Buckingham, Open University Press.Bantuelle, M., J. Morel et D. Dargent (1998). La
participation et les acteurs. Bruxelles, ASBL« Santé, communauté, participation ».
Bergeron, P. et F. Gagnon (1994). La prise en charge étatique de la santé au Québec. Lesystème de santé au Québec. Organisations,acteurs et enjeux. V. Lemieux, P. Bergeron, C.Begin et G. Bélanger. Sainte-Foy, Les presses del’université Laval: 9-32.
Bernier, N. F. (2006). “Quebec’s Approach to Population Health: An Overview of Policy Contentand Organization.” Journal of Public Health Policy27: 22-37.
Bourdieu, P. (2001). Science de la science et réflexivité. Paris, Raisons d’agir.
Conill, E. M. et M. O’Neill (1984). « la notion de santé communautaire: éléments de comparaisoninternationale. » Canadian Journal of Public Health75: 166-175.
De Koninck, M. et D. Fassin (2004). « Les inégalités sociales de santé, encore et toujours. » Santé,Société et Solidarité 2: 5-12.
Douglas, M. et A. Scott-Samuel (2001). “Adressing health inequalities in health impact assessment.” JEpidemiol Community Health 55: 450-451.
Drulhe, M. (2000). Fin de siècle et inégalités sociales de santé en France: l’amorce d’undébat? Les inégalités sociales de santé. A.Leclerc, D. Fassin, H. Grandjean, M. Kaminski etT. Lang. Paris, Inserm - La découverte: 41-51.
Fassin, D. (2000a). « Comment faire de la santé publique avec des mots. Une rhétorique àl’œuvre. » Ruptures 7(1): 58-78.
Fassin, D. (2000b). Les enjeux politiques de la santé, Études sénégalaises, équatoriennes etfrançaises. Paris, Karthala.
Fassin, D. (2006). Quand les corps de souviennent. Expériences et politiques du sida en Afrique duSud. Paris, La Découverte.
Fournier, P. (2003). L’art et la science de la santé publique. Environnement et santé publique:fondements et pratiques. M. Gérin, P. Gosselin, S.Cordieret al. [St-Hyacinthe, Québec], [Paris],Edisem; Diffusion Éditions Tec & Doc: 39-57.
Gagnon, F. et P. Bergeron (1999). Le champ contemporain de la santé publique. Le systèmede santé québécois. Un modèle entransformation. C. Bégin, P. Bergeron, P.-G.Forest et V. Lemieux. Montréal, Les presses del’Université de Montréal: 229-258.
Gepkens, A. et L. J. Gunning-Schepers (1996). « Interventions to reduce socioeconomic healthdifferences: a review of the internationalliterature. » European Journal of Public Health 6:218-26.
Green, L. W. et M. W. Kreuter (1999). Health promotion planning: an educational andecological approach. Mountain View, CA, MayfieldPub. Co.
Hancock, T., R. Labonté et R. Edwards (1999). Indicators that count! - Measuring populationhealth at the community level: 182.
Hills, M. D., S. Carroll et M. O’Neill (2004). « Vers unmodèle d’évaluation de l’efficacité desinterventions communautaires en promotion de lasanté: compte-rendu de quelquesdéveloppements nord-américains récents. »Promotion & Education Spec no 1: 17-21, 49.
Horton, R. (1998). “The new new public health of risk and radical engagement.” Lancet 352 (9124):251-2.
Institute of Medicine (2000). To err is human: building a safer health system. Washington, D.C.,National Academy Press.
Jaffré, Y. et J.-P. Olivier de Sardan (1999). La construction sociale des maladies, les entitésnosologiques populaires en Afrique de l’Ouest.Paris, Presses Universitaires de France.
Lefkowitz, B. (2007) Community Health Centers. A Movement and the People Who Made It Happen.New Brunswick, New Jersey and London, RutgersUniversity Press.
Lessard, R. (2003). « Nouvelles perspectives sur la santé des Montréalais: une action commune pourréduire les inégalités. » Policy Options March2003: 41-45.
Lupton, D. (1995). The imperative of health: public health and the regulated body. London; ThousandOaks, Calif., Sage Publications.
Mackenbach, P. (2005). Health Inequalities: Europe in Profile. London, An independent expert reportcommissioned by and published under theauspices of the UK Presidency of the EU: 48.
Marmot, M. (2001). “Inequalities in health.” New England Journal of Medicine 345(2): 134-136.
Mattei, J.-F. (2002). Le devoir impérieux de santé publique en France et en Europe. Paris, Discoursauprès de l’Académie Nationale de Médecine, le1er octobre.
McKinlay, J. B. et S. M. McKinlay (1977). “The Questionable Effect of Medical Measures on theDecline of Mortality in the United States in theTwentieth Century.” Milbank Memorial FundQuarterly Health and Society (55): 405-28.
Ministère de la santé et des services sociaux (1992).La politique de la santé et du bien-être. Québec,Santé et services sociaux.
Ministère de la Santé et des Services sociaux (1997). Priorités nationales de santé publique1997-2002. Québec, MSSS.
Nishtar, S. et al. (2006). « Le Consortium mondial sur la promotion de la santé communautaire. »Promotion & Education 13(1): 53-54.
Nyamwaya, D. (2005). Trends and factors in the development of Health Promotion in Africa, 1973-2003. Promoting Health, Global Perspectives. A.Scriven et S. Garman. London, Palgrave: 167-178.
O’Neill, M. et A. Stirling (2007). The promotion of health or the health promotion: Getting ourconcepts straight. Health Promotion in Canada:Critical perspectives (2nd edition). M. O’Neill, A.Pederson, I. Rootman et S. Dupéré. Toronto,Canadian Scholars Press Inc.
OMS (1986). La charte d’Ottawa pour la promotion de la santé. Ottawa, OMS, Santé et Bien-êtresocial Canada, CPHA.
Paquet, G. et B. Tellier (2003). Les facteurs sociaux de la santé. Le système de santé au Québec.Organisations, acteurs et enjeux. V. Lemieux, P.Bergeron, C. Bégin et G. Bélanger. Québec, LesPresses de l’Université Laval: 65-89.
Pascal, J., H. Abbey-Huguenin et P. Lombrail (2006).« Inégalités sociales de santé: quels impacts surl’accès aux soins de prévention ? » Lien social etPolitiques 55(Printemps): 115-124.
Ridde, V. (2004a). « Agir contre les inégalités sociales de santé : tentative d’explications del’immobilisme des autorités de la santé publiquequébécoise. » Revue Canadienne de SantéPublique 95(3): 224-7.
Ridde, V. (2004b). « Une analyse comparative entre le Canada, le Québec et la France: l’importancedes rapports sociaux et politiques eu égard auxdéterminants et aux inégalités de la santé. »Recherches Sociographiques XLV(2): 343-364
Ridde, V. (2005). « Une triple interrogation à propos de la Charte de Bangkok. » Reviews of HealthPromotion and Education Online, 2005.URL:http://www.rhpeo.org/reviews/2005/9/index.htm.
Ridde, V., T. Delormier et L. Gaudreau (2007). Evaluation of Empowerment and Effectiveness:Universal Concepts? In press. GlobalPerspectives on Health Promotion Effectiveness.Volume I D. V. McQueen et C. M. Jones. NewYork, Springer Science & Business Media.
Ridde, V. et A. Seck (2006). Quelques défis de la mise en œuvre de la Charte de Bangkok enAfrique francophone. Charte de Bangkok:Ancrage pour de meilleures pratiques enpromotion de la santé? Collection Partage. E. vanSteenberghe et D. St-Amand. Montréal, REFIPS:pp 57-61.
Roos, N. P., M. Brownell et V. Menec (2005). Universal Medical Care and Health Inequalities:Right Objectives, Insufficient Tools. HealthierSocieties. From Analysis to Action J. Heymann,C. Hertzman, M. L. Barer et R. G. Evans. NewYork, Oxford University Press: 107-131.
Rootman, I., M. Goodstadt, B. Hyndman, D. V. McQueen, L. Potvin, J. Springett et E. Ziglio, Eds.(2001). Evaluation in health promotion: principlesand perspectives, WHO Regional Publications.European Series, No. 92.
Rose, G. (1985). “Sicks individuals and sick populations.” Int J Epidemiol 14(1): 32-38.
VIG et ENHPA (2001). Tackling social inequalities inhealth. The role of health promotion. Researchreport: 149.
Wallerstein, N. (2006). What is the evidence on effectiveness of empowerment to improve health?Copenhagen, WHO, Regional Office for Europe,Health Evidence Network: 37.
Advancing knowledge
11IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
Whitehead, M. (1995). Tackling inequalities: a reviewof policy initiatives. Tackling inequalities in health.An agenda for action. M. Benzeval, K. Judge et M.Whitehead, King’s Fund: 22-52.
WHO (1978). Declaration of Alma-Ata, International conference on Primary Health Care. Alma-Ata,USSR, WHO: 79.

The First International Conference onHealth Promotion in Ottawa, Canada, in1986 produced what has since becomeknown as the Ottawa Charter for Health Pro-motion (PAHO/WHO, 1986). Since then thehealth promotion strategy is accepted andutilized as a central element in communitydevelopment processes. As a result, in thelast 3 decades, governments and interna-tional organizations have significantlyincreased their investments in health pro-motion programs.
The concept of health promotion hasshifted from a focus on disease preventionin the 1970s, to the recognition of the needfor complementary interventions (such ashealthy public policies), to incorporateother sectors, and to create healthy envi-ronments in the 1980s and 90s. In the pastfew years, the concept of health promotionhas broadened to include the determinantsof health, global movements of socialchange and the need to invest andstrengthen leadership in health promotion.
Health promotion today focuses onaddressing the multiple determinants ofhealth. These determinants are both withinindividuals’control (such as personal prac-tices and behaviors and accessing serv-
ices), as well as outside it (such as physi-cal and social environments, education,income and social status, housing, accessto food, social support networks, and work-ing conditions, etc.). These determinantsdo not act in isolation of each other, butrather interact in very complex ways.
Creating a healthy and supportive set-ting, also known as the settings approach,continues to be one of the most widely usedhealth promotion strategies. The healthysettings approach is based on the premisesthat determinants of poverty and equity,and their influence on health, can beaddressed through creating sustainablepublic policies and laws, developing sup-portive environments, building public-pri-vate partnerships, strengthening networks,mobilizing means of communication, andpromoting an active role of municipal andlocal governments in health promotion anddevelopment.
The Healthy Municipalities, Citiesand Communities (HMC) Strategy
The HMC movement is an example ofthe application of health promotion princi-ples at the local level. The Pan AmericanHealth Organization (PAHO) developed
and introduced the HMC Strategy in the1990s to improve and promote local healthand development in the countries of theAmericas. This Strategy is being activelyimplemented in 17 of the 38 countries of theAmericas.
An HMC is one that ensures continuousimprovements in the conditions that affectthe health and wellbeing of its members.This is achieved by facilitating joint actionamong local authorities, community mem-bers and key stakeholders towards improv-ing their living conditions and quality of life.More than just addressing the conse-quences of disease, the HMC Strategyfocuses on the determinants of health, andsupports the processes that enable com-munity members to take control over theirown health and quality of life, and to par-ticipate in the development of an HMC(PAHO, 2002).
HMC is based on the premises that (1)various systems and structures governingsocial, economic, civil and political condi-tions, as well as physical environments, canimpact individuals’ and communities’health; and that (2) health is inherentlylinked to individuals’capacity to act in thecommunity and society to which they
IUHPE – PROMOTION & EDUCATION SUPPLEMENT 2 200712
Lessons learned from the application of a participatoryevaluation methodology to Healthy Municipalities, Cities andCommunities Initiatives in selected countries of the AmericasMarilyn Rice1 and Maria Cristina Franceschini1
Abstract: Health promotion has made significant strides in the past few decades in the Americas. Creating a healthy and sup-portive setting, also known as the settings approach, continues to be one of the most widely used health promotion strategies.Interest in evaluating the effectiveness of these strategies has been increasing greatly in the past few years. Participatory eval-uation holds great promise for helping to generate this evidence and promote understanding of the factors that affect, posi-tively or negatively, the advances of health promotion in the Region. During 2004-2006, a Participatory Evaluation methodol-ogy was introduced into several countries in the Americas through formal trainings conducted by the Pan American HealthOrganization (PAHO) in collaboration with country partners. This article summarizes the main lessons learned from the appli-cation of the participatory evaluation methodology in various countries in Latin America and the Caribbean. Factors affectingthe evaluation of the initiatives were identified at multiple levels (individuals, community, organizational, political, economic,etc.). Specific issues that were addressed included the political context, turnover of personnel in key institutions, concerns relatedto the effectiveness of participatory processes, and the existence of strong and sustained leadership at the country level.These factors are intertwined and affect each other in very complex ways, a fact that was reflected in the municipalities’experi-ences with participatory evaluation. Challenges included the ability to secure resources for the evaluation, the time needed toconclude the process, and working in an intersectoral manner. However, participating municipalities reported that the processof implementing a participatory evaluation and working with various stakeholders had an empowering effect: communities andstakeholders were more willing and interested in participating in health promotion initiatives in a sustained manner; alliances andintersectoral collaboration were strengthened; communication channels were opened; and municipalities were stimulated toreview their planning and implementation processes in order to more appropriately incorporate health promotion principles.The article concludes with recommendations to improve the planning and implementation process of participatory evaluationefforts. (Promotion & Education, 2007, (2): pp)
Key words: health promotion, healthy municipalities, communities, participatory evaluation
1. Health Determinants and Social Policies Unit, Area of Sustainable Development and Environmental Health, Pan American Health Organization/World HealthOrganization. Correspondence to Marty Rice: [email protected].
Résumé en français à la page #. Resumen en español en la página #.
Advancing knowledge

belong. HMC strives to create a synergybetween two premises: promoting individ-ual actions and societies that respond sup-portively. The ultimate goal is to supportprocesses that enable people to take con-trol over their own health while improvingequity, social participation, accountabilityand responsive local governance.
Evaluating HealthyMunicipalities, Cities andCommunities (HMC) Strategy
The evaluation of health promotionstrategies such as HMC has been recog-nized by the international community asnecessary in order to strengthen the capac-ity of institutions and communities to pro-mote measures that are coherent with theneeds and priorities of the population.Thanks to the HMC Strategy, countries ofthe Americas have gained considerableexperience with innovative ways of trans-lating health promotion into local action.However, there is little documentationabout these experiences and even lessabout the results achieved.
Health promotion strategies, such asHMC, generate real benefits for people andtheir environment. It is of particular impor-tance to be able to show these benefits todecision-makers so that they will be willingand motivated to set aside resources to sup-port health promotion programs and activ-ities. The evaluation offers many opportu-nities to create and disseminate evidencethat demonstrates strengths, weaknesses,consequences, and impacts resulting fromthe development and implementation ofthese strategies.
The evaluation of these initiatives willalso provide stakeholders with the oppor-tunity to better know their community andits resources, and to reflect on the progressof their efforts. This will, in turn, supportbetter design and management of healthpromotion initiatives in the context of com-munity health resources, as well as createaccountability related to what has been pro-posed and redirect efforts when needed.Given the intersectoral and interdiscipli-nary nature of health promotion, it is alsoexpected that the evaluation process willcreate opportunities for collaborationamong sectors, improve multidisciplinarydialogue and strengthen participatoryefforts within HMCs.
The participatory evaluation ofHMC initiatives
In very simple terms, evaluation meanscollection, analysis, interpretation andreporting of information, and using theresults for decision-making. Like health pro-motion, in the past few decades, the con-cept of evaluation has also greatly evolved.
Advancing knowledge
13IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
The goal of evaluating health promotionstrategies shifted from the evaluation andmonitoring of projects and interventions, tomore complex, thematic and interdiscipli-nary evaluations.
The implementation of health promo-tion programs highlighted the need formore flexible and participatory evalua-tions; ones that reflected health promotionprinciples as well as the complexity of localdevelopment and participatory experi-ences. This new approach required multi-ple measures and methods in order to eval-uate changes in areas such as governance,social participation, social impact, equity,sustainability, etc.
Instead of judging the success or failureof an intervention or a project, this newapproach focused on understanding localrealities and on continuous learning. Eval-uation, hence, shifted from something doneby «outsiders» to a collaborative and par-ticipatory endeavor.
It is in this context that the concept ofparticipatory evaluation develops. In a par-ticipatory evaluation, the key stakeholdersare involved in all phases of the process,including the design, implementation, man-agement, interpretation, and decision-mak-ing about the evaluation and its results. Aparticipatory evaluation implies more thanthe application of participatory techniquesto conventional approaches and method-ologies for monitoring and evaluation. Itrequires:• Participation of key stakeholders on all
phases of the process.• Negotiation and consensus about what to
evaluate and how results will be inter-preted and utilized.
• Continuous learning that results in capac-ity building and incorporation of lessonslearned in the decision-making process.
• Flexibility to adapt to a continuouslychanging environment.
Participatory evaluation is considered tobe the most appropriate methodology inthe context of HMC initiatives because itreflects the principles of the HMC strategy,recognizes the complexities of HMC as alocal development initiative, and facilitatesthe development of capacities, learning andempowerment. As such, participatory eval-uation stimulates autonomy and commu-nity self-determination as it allows commu-nities to improve their ability to resolvetheir own problems (PAHO, 2006).
It is expected that the implementation ofa participatory evaluation will create oppor-tunities and give voice to a broader range ofstakeholders, encouraging them to takeownership of the evaluation process. Whenconducted in a truly participatory manner,this type of evaluation promotes account-
ability and motivates continuous and activeparticipation from all stakeholders.Processes that are based on the commit-ment and dedication of all stakeholders arelikely to create a sense of common interestamong those involved and to produce pos-itive changes in their community.
However, the participatory evaluationmethodology presents some challenges. Aswith most collaborative and participatoryendeavors, participatory evaluation can betime-consuming, since the process requiresbringing together and building consensusamong people from various backgrounds,sectors, institutions and groups, that oftenbring to the table different, if not conflicting,needs, agendas and interests. This empha-sizes a need to clarify roles, responsibilitiesand the evaluation objectives andprocesses. The participatory evaluation alsorequires leadership from people with strongfacilitation skills as well as people with open-ness to collaborate, to listen and to take intoconsideration their colleagues’perspectives,needs and interests. Because it is an openand flexible process, participatory evalua-tion has no predetermined plan. As a result,this approach may be perceived as less effec-tive and objective and can be unsettling tothose who are used to working with tradi-tional evaluation settings.
PAHO’s participatory evaluationinitiative
In 1999, PAHO established a HealthyMunicipalities Evaluation Working Group,comprised of evaluation experts from vari-ous international institutions. The WorkingGroup agreed that specific evaluation tools,frameworks and evidence of effectivenesswere needed to support health promotionand similar initiatives. Building upon theserecommendations, the Evaluation WorkingGroup has developed a series of evaluationtools, among them, a Participatory Evalua-tion Guide for Healthy Municipalities, Citiesand Communities.
The Guide provides recommendationson evaluation processes and tools, as wellas a mechanism to showcase and docu-ment the rich, extensive, and varied expe-riences and results related to the HMC Strat-egy. It offers an evaluation framework thatincorporates essential HMC and health pro-motion elements such as intersectoral col-laboration, social participation, capacitybuilding, community capacity, among oth-ers. The methodology allows for the docu-mentation and analysis of changes andaccomplishments in terms of process, out-comes and results, and guides users onhow to act on the results to improve theirHMC initiative.
During 2004-2006, the Participatory Eval-uation Guide was introduced into several

Advancing knowledge
countries in the Americas through formaltrainings conducted by PAHO in collabora-tion with country partners. Participants inthese trainings included staff from the Min-istry of Health (MOH) and other key min-istries (such as education) at the nationalas well as state levels; representatives fromNGOs, universities, and funding agencies;health workers; municipal staff and author-ities; community organizations and mem-bers. Following the trainings, several com-munities in various countries of theAmericas applied the participatory evalu-ation methodology to their HMC initiatives.Follow-up questionnaires were sent toworkshop participants every 4 months dur-ing 2005-2006 to collect information aboutthe activities taking place as a result of thetraining received. During this period, coun-tries also submitted reports to PAHO and/orpublished their experiences with the appli-cation of the participatory evaluationmethodology.
Lessons learned from theapplication of the ParticipatoryEvaluation Methodology
This section presents the main lessonslearned from the application of the partici-patory evaluation methodology in Brazil,Dominican Republic, Honduras, Mexico,Peru and Trinidad and Tobago. This infor-mation was compiled from reports submit-ted by the countries to PAHO and from thefollow-up questionnaires completed byworkshop participants.
1. Take into account the political context
and timing
Given the strong emphasis of initiativessuch as HMC on the active involvement oflocal authorities and the public sector, thepolitical context and timing was by far themost important factor affecting the imple-mentation of participatory evaluation in theparticipating countries. Election periodsand political transitions often caused majordelays (if not termination) of initiatives,shortage/change of personnel and funds,and great uncertainty about the future ofthe initiatives, and their evaluation.
In Honduras, for example, plans to con-duct participatory evaluations that wereincorporated into the municipalities’strate-gic plans for 2006, were suspended after thelocal elections and the political changesthat took place in that year. Many of the peo-ple spearheading the process wereremoved from their posts. Workshops inthe participatory evaluation methodologyin municipalities were also suspended dueto administrative problems in State HealthSecretariats caused by this political transi-tion and the turnover of key personnel.
The political timing of the application of
the Participatory Evaluation Guide in theCampinas Region of the State of São Paulo,Brazil, was also reported as «sensitive»,since it occurred right before elections. Thisgenerated uncertainty about who wouldstill be present to follow-up on the initia-tives, or even if initiatives would be contin-ued (Sperandio et al. 2006).
The experience in the DominicanRepublic underscores this difficulty. Eventhough plans were in place to conduct theparticipatory evaluation in 10 municipali-ties during 2006, local elections took placeresulting in significant changes of municipalauthorities and staff. As a result, efforts hadto be redirected to introduce and seek sup-port for the HMC initiative and the partici-patory evaluation from the newly electedand re-elected officials.
These moments of political/administra-tive transitions can have considerableimpact on the work being conducted at thecommunity level. It causes delays andlosses (including financial) since the timenecessary to explain and get agreement onthe continuation of programs can belengthy. This has consequences for theevaluation of programs under implemen-tation, but especially for programs con-ducted by previous administration that donot continue under the new one.
These experiences demonstrate that thetransitory nature of local and national polit-ical contexts can weaken programs andpublic policies, particularly when there is achange in political parties. This emphasizesthe need to form a strong coalition amongall sectors of society to strengthen and sus-tain the HMC initiative and their evaluation(Sperandio et al, 2006). Having a strong andbroad base of support can provide conti-nuity and sustainability to HMC initiativesand their evaluation during these transi-tional periods.
2. Aim for a truly intersectorial process
Incorporating a variety of local partners(MOH, NGOs, universities, communitymembers and community-based organiza-tions, etc.) was important for the sustain-ability of the HMC initiative and its partici-patory evaluation in the countries. It iscrucial, however, to get buy-in from themain stakeholders in order to begin andsustain the implementation of the partici-patory evaluation methodology. Lack ofsupport from critical stakeholders, such asmunicipal program managers or key per-sonnel at public institutions can seriouslydeter or isolate the advancement of the ini-tiative.
In the experience of Vila Paciencia, inthe State of Rio de Janeiro, Brazil, it was dif-ficult to coordinate the activities with thepublic sector, due to the communities’«his-
torical social isolation and lack of citizen-ship rights», which was marked by «struc-tural oppression and violence.» (Becker etal., 2006). As a result, it was not possible toinclude a representative from the publicsector in the evaluation process, given itsdemonstrated lack of interest in the com-munity. In addition, a weak communityorganization could not ensure that the com-munity had a voice and, as a result, formalparticipation from the community associa-tion was weak. Even though this did notimpede the conduct of the participatoryevaluation by other stakeholders involvedin the community (NGOs, universities,etc.), it kept the process isolated from thebroader community context since it wasunclear whether the evaluation results andconclusions would be taken into consider-ation by all relevant stakeholders.
However, as the Vila Paciencia experi-ence reported, the implementation of a par-ticipatory evaluation methodology forcedthe group to confront these difficulties andto reflect on possible courses of action: «theparticipatory evaluation’s emphasis onintersectorial collaboration contributedgreatly to understanding local politics andthe role of different actors (public, private,community, etc.), thereby providing a ref-erence for discussions and decision-mak-ing.» (Becker et al, 2006)
Upon realizing the above, the groupdecided to create a new intersectoral groupfocused on the construction of a new com-munity kitchen. The new group includesrepresentatives from the local public sector(municipal education and social develop-ment, state’s social assistance), as well ascommunity members. The weak commu-nity participation also required concertedefforts focused on the process of getting thecommunity organized. The new actors havedemonstrated interest in participating in theevaluation process. It is expected that work-ing on the evaluation will help to strengthenthe work of the new intersectoral group andfavor the sustainability of the Vila Pacien-cia initiative (Becker et al, 2006).
3. Conducting a participatory evaluation
takes time, but it is worth it
All countries reported that the partici-patory evaluation process was lengthy andtime consuming due to various factors. It isnecessary to bring together and guaranteethe buy-in from people from various back-grounds, sectors and interests. These peo-ple bring to the table different perspectivesand paradigms. They often come from insti-tutions and organizations with rigid andbureaucratic structures and work cultures.
As it happens in processes that empha-size community and multi-sector participa-tion, the various levels of knowledge and lit-
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 200714

eracy among those involved have to betaken into account. Experiences in Brazil,Peru, Dominican Republic and Trinidadand Tobago all noticed that different levelsof education among the community leaderswas a challenge to implementing the eval-uation.
It is important to recognize the timeneeded for institutions, organizations andindividuals to adapt and accept a newmethodology and paradigm that can greatlychange how they function and work, suchas a participatory evaluation. In manycases, given the appropriate time and stim-ulation, people become motivated andapply dedicated efforts to implementingthese new programs and methodologies.
For example, the participatory method-ology was new to most of the health secre-tariats of the participating municipalities.This often generated an internal movementacross public institutions to discuss thenew concepts and assess degree of agree-ment among staff in order to incorporatethe new methodology into existing pro-grams, with particular emphasis on inter-sectorial collaboration and guaranteeingsocial participation in actions and decision-making processes. This is a slow process asit needs to take place through meetings,forums and discussion groups, andrequires linking various levels of adminis-tration, breaking existing paradigms, anddealing with individual and collectiveresistance (Sperandio, 2006).
Respecting the time needed to achievethis acceptance in public institutions andamong their staff was critical in order to putin place programs that were consistent withthe communities’expectations, making opti-mal use of resources, adopting approachesthat were more consistent with health pro-motion practices, and improving personalmotivation among public staff and otherstakeholders.
This initial process also served as anopportunity to strengthen alliances andtrust among participants and their institu-tions (for example, municipal managers,representatives from the community andNGOs). As reported by the experience ofcommunities in the Northeast of Brazil,these new alliances “encouraged an inno-vative way to promote local empowermentand equity.” (De Sá et al., 2006)
Since preparing for and using participa-tory processes takes time in order to workeffectively and even longer to demonstrateresults, often, due to political pressures andimpending changes in government, coun-tries will bring in evaluators external to thecommunity to conduct an outside and non-participatory evaluation. Although this pro-duces useful information and results, itdoes not have the same empowering and
Advancing knowledge
15IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
long-lasting impact of the more participa-tory processes. It also does not guaranteethat the information collected and analyzedand the lessons learned will be shared withthe community.
4. Set aside resources for the evaluation
Lack of sufficient resources have inmany cases limited or interrupted the par-ticipatory evaluation process. The alloca-tion of scarce community resources to con-duct a participatory evaluation was acommon problem. This was often the resultof a general lack of understanding about theeffectiveness and the usefulness of theresults generated on the part of programmanagers and others responsible for fund-ing and budget.
This underscores the importance of con-tinuously educating and raising awarenessof the importance of health promotion inpromoting equity and better health for all,and the need to establish adequate fundingand structures for its evaluation. Thisincludes the need to educate stakeholderson the benefits and the appropriateness ofparticipatory evaluation in producing keyinformation for decision-making at all lev-els.
Analysis of previous international expe-rience supports the allocation of a mini-mum of 10% of total program resources toensure the development and implementa-tion of evaluation in health promotion(PAHO, 2005). It is important to advocate forthe establishment of a fund for health pro-motion evaluation from the initial planningstages of any initiative (PAHO, 2005).
5. Reach consensus on the definition of
key concept
It was common for the participatingcountries and the stakeholders to report ageneral lack of understanding about theconcept of health promotion (often con-sidered an approach to disease prevention)and the participatory evaluation method-ology. This can have a direct impact on theplanning of the evaluation since how peo-ple understand key concepts will shape thedesign, data collection, analysis and pres-entation of results of the evaluation.
There were also doubts about the ben-efits of conducting a participatory evalua-tion, mostly related to the time it takes toconduct the process and the usefulness ofthe data it will produce. As a result, it wasnot uncommon to face resistance by thosein key institutions in applying a participa-tory evaluation methodology that, as theyunderstood it, did not emphasize resultsand project evaluation.
It is important to address these concernsand take into account the challenges facedby stakeholders coming from institutions
with rigid and bureaucratic structures, thatvery often do not have a policy to coordi-nate with other institutions or to work inan intersectorial manner, and who are oftenunwilling to share information.
6. Address concerns related to partici-
patory processes
Concerns about working with the com-munity also came up in some instances,often in the form of fears of receiving nega-tive comments about and prejudice againstactions taken with “too much” input fromcommunity members. Representativesfrom public sectors in some cases wereapprehensive that the process would gen-erate “unrealistic demands” on the part ofcommunity members or negative criti-cisms. This was particularly true of com-munities that were not well represented, inwhich, traditionally, programs andapproaches were implemented from thetop-down and truly representative and par-ticipatory mechanisms for community par-ticipation were scarce or non-existent.Often efforts had to be re-directed at organ-izing the community, and raising awarenessabout the real meaning of “participation”among the stakeholders.
7. Institutional context and individual
factors
Working with institutions with rigid andbureaucratic structures was also reportedas a major challenge for those engaged inconducting a participatory evaluation.Main complaints included lack of institu-tional support or excessive bureaucracy,lack of coordination among public sectorinstitutions, strict guidelines regarding theuse of funds, and conflicts between the dif-ferent actors involved (federal, state, munic-ipal).
Personal and professional interests, lowtechnical capacity of personnel, and con-cerns that participatory evaluation wouldonly lead to a heavier workload that wouldnot necessarily translate into «benefits» fortheir immediate work also affected people’sinterest in investing in the process.
Of all challenges, the high turnover ofpersonnel at all levels and institutions wasby far the most disruptive and difficult todeal with since it could seriously impair thecontinuity, feedback and appropriate appli-cation of the participatory methodology.Brazil, Peru, Mexico and Trinidad andTobago all indicated the difficulties facedwhen changes took place of key personnel(particularly within the Ministry of Health)involved with the health promotion initia-tives and their evaluation. Public sectorpersonnel are frequently transferred toanother State or unit/program within theirinstitutions and it is often the case that in

Advancing knowledge
their new posts they are no longer in a posi-tion to follow through with the initiatives forwhich they were previously responsible.
In Trinidad and Tobago, for example, aseries of training workshops in participa-tory evaluation were planned for MOH/Regional Health Authorities staff and com-munity members but had to be postponeddue to limitations caused by institutionalchanges. This activity is suspended untilfurther notice, until other national coun-terparts are assigned by the MOH. Changesin key personnel were also responsible forthe cancellation of participatory evaluationworkshops in Honduras.
On the positive side of working withinstitutions, the experience in Perureported that the process of participatoryevaluation has opened channels of com-munication with other levels and sectorsproviding valuable inputs into the annualevaluation of the Ministry of Health. Thishas resulted in an improved organizationalclimate and opened a space for exploringnew modes of intersectoral collaboration(Red de Municipios Saludables del Peru,2004).
Working with institutions also offers theopportunity to regularize processes andmethodologies within their work plans, pro-grams, etc. Given institutions’far-reachingstructure and linkages with other groupsand institutions, this has the potential topromote and support the implementationof health promotion activities, its evalua-tion and the allocation of resources forthese priorities. Another example is that ofthe San Marco University, a public institu-tion in Lima, Peru. The participatory eval-uation methodology was incorporated intothe curriculum of their health promotioncertificate program, which provides theopportunity to build capacities andincrease technical knowledge among pro-fessionals working in the field.
8. Strong leadership is central to the sus-
tainability of the evaluation initiative
A common determinant of successfulexperiences with the participatory evalua-tion in the countries was the existence ofstrong, sustained and dynamic leadershipto take the process forward. Active com-mitment and engagement from institutionsboth at the local and national levels is keyto the success of the initiative, as is collab-orative work among these institutions.
The role of national and regional HMCnetworks can be central in these efforts, giv-ing their potential far-reaching connectionsto municipalities throughout a country orregion, as well as their connection with keystakeholders that can support the evalua-tion process. Gaining the support and work-ing through national and regional HMC net-
works greatly supported the advancementand sustainability of the evaluation initia-tive in countries such as Brazil and Peru.In Peru, the AMARES Project, a programsupported by the European Union, thePeruvian Network of Healthy Municipalitiesand 7 regional Peruvian networks are col-laboratively developing a database of base-line data which, in turn is generating a greatdeal of baseline data that will be critical tosupport evaluation efforts in the future.
9. Conducting a participatory evaluation
can be an empowering process by
itself
There was an empowering effect ofapplying a participatory methodology –communities and stakeholders were morewilling and interested in participating andmaintaining this participation. The processof planning and implementing a participa-tory evaluation provided a very rich oppor-tunity to discuss, exchange and reflect oncountries’experiences with the HMC Strat-egy.
Most countries reported that these plan-ning discussions brought to light the vari-ous interpretations that participants gave tohealth promotion concepts and principles.Participants quickly realized the implica-tions of these differences for the planningand implementation of the evaluationmethodology and the importance of reach-ing consensus among the group members.This resulted in a productive and positivedialogue among participants to reach con-sensus on the various concepts and prin-ciples utilized in their evaluation processes.
This process also stimulated partici-pants to take into account different aspectsof health promotion that had been over-looked in previous evaluation efforts. Thisbrought up a “difficulty” since many real-ized that their HMC programs were not tak-ing into account some of the health pro-motion principles (for example, programswere not intersectoral). This is stimulatingmany municipalities to review their plan-ning and implementation processes inorder to more appropriately incorporatehealth promotion principles.
ConclusionsHealth promotion has made significant
strides in the past few decades in the Amer-icas. Interest in evaluating its effectivenesshas been increasing greatly in the past fewyears. Participatory evaluation holds greatpromise for helping to generate this evi-dence and promote understanding of thefactors that affect, positively or negatively,the advances of health promotion in theRegion.
The experiences described in this arti-cle highlight some of the various challenges
posed by the complex and multidimen-sional local and national contexts in whichthe participatory evaluation is introduced.Factors affecting the success of evaluationinitiatives were identified at all levels of real-ity (individuals, community, organizational,political, economic, etc.). It is also impor-tant to take into account that these factorsare intertwined and affect each other invery complex ways. This was reflected inthe municipalities’experiences in applyingthe participatory evaluation.
Even though the development of theParticipatory Evaluation Guide happenedas a direct response to requests from coun-tries implementing the HMC Strategy, oncethe methodology was made available andwas applied in such initiatives, the majorityof countries realized they «were not ready»to implement such an innovative approachto evaluation. This was mainly due to theirrealization that their HMC and health pro-motion programs and initiatives had notappropriately taken into account key healthpromotion principles (such as intersector-ial collaboration or community participa-tion).
This was an important contribution thatthe application of the participatory evalu-ation made to these initiatives: it shed lighton the gaps in their efforts and forced thoseinvolved to confront the problems andreflect on how to address them. As a result,the majority of community groups and insti-tutions involved in this initiative perceivedthe need to re-examine and thereby reori-ent their planning and implementationprocesses in order to effectively apply theparticipatory evaluation methodology inthe future. Thus, engaging in the participa-tory evaluation process has served as a cat-alyst to generate intersectoral and partici-patory processes essential to thedevelopment of HMC initiatives.
All countries involved in this evaluationinitiative reported that the process of engag-ing in participatory evaluation was highlymotivating and revitalizing, concretelyallowing those involved to evaluate theiractions more consistently, stimulating inter-est in the issue of evaluation and in-depthreflection on activities. The experiencestrengthened capacities among thoseinvolved, generated commitment to pro-mote health promotion principles, strength-ened alliances among key stakeholders,and emphasized the potential of the par-ticipatory evaluation as a decision-makingtool. These experiences demonstrate thatsupporting the implementation of partici-patory evaluation initiatives has the poten-tial to contribute to the advancement ofhealth promotion in the countries of theAmericas.
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 200716

ReferencesBecker D, Edmundo K, Nunes N, Mattos A, MarquesR, Bonato D (2006) “CEDAPS/Rio de Janeiro: ainiciativa de Vila Paciência” In Akerman M & MendesR (2006) Avaliação Participativa de Municipios,Comunidades e Ambientes Saudáveis: a trajetóriabrasileira – memória, reflexões e experiencia. MidiaAlternativa. São Paulo, Brazil.De Sá R, Viana V, Nishida M, Yuasa M (2006)“UFPE-NUSP/ Recife: Municipios Saudáveis noNordeste do Brasiol” In Akerman M & Mendes R(2006) Avaliação Participativa de Municipios,Comunidades e Ambientes Saudáveis: a trajetóriabrasileira – memória, reflexões e experiencia. MidiaAlternativa. São Paulo, Brazil.Pan American Health Organization/World HealthOrganization (2002) Healthy Municipalities andCommunities: Mayor’s Guide for Promoting Qualityof Life. Pan American Health Organization/WorldHealth Organization. Washington, DC.Pan American Health Organization/World HealthOrganization (2005) Healthy Municipalities, Citiesand Communities: Evaluation Recommendations forPolicymakers in the Americas. Pan American HealthOrganization/World Health Organization.Washington, DC.Pan American Health Organization/World HealthOrganization (2006) Guía de EvaluaciónParticipativa para Municipios y ComunidadesSaludables. Pan American HealthOrganization/World Health Organization. Lima, Peru.Red de Municipios y Comunidades Saludables delPeru (2004) Experiencia de Aplicación de la Guíade Evaluación Participativa en el Peru. Reportsubmitted to the PAHO Healthy MunicipalitiesEvaluation Working Group. Washington, DC.Sperandio AM, Correa C, Rodriguez E, Bueno RM(2006) A experiência de aplicação do Guia deAvaliação Participativa em uma Rede de Municipios:um processo em desenvolvimento. Report submittedto the Pan American Health Organization,Washington, DC.
Advancing knowledge
17IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007

IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 200718
Current health promotion practices in communities – Asia
Who we are?Aparajita can be described as a civil
society response to the devastating cyclonein Orissa, India, which occurred on October29, 1999, and completely shattered therhythm of people’s lives. More than 15 mil-lion people in 10 districts of Orissa weresaid to be affected with around a millionhouses damaged. The aftermath not onlyrevealed the extent of damages in terms ofmaterial and human loss but also the inad-equacies of individuals, communities andadministration vis-a-vis disaster prepared-ness. A number of individuals and institu-tions came together under aegis of the Vol-untary Health Association of India (VHAI)to provide relief to the cyclone affected peo-ple of Orissa. VHAI did not have disasterrelief or mitigation in its original mandate,but to turn its back on people’s misery anddistress was not an acceptable option.Hence VHAI’s response to the tragedy wasinstantaneous and spontaneous.
After three initial weeks of emergencyrelief and medical assistance by VHAI,Aparajita came into being as VHAI’sresponse to the perceived need of longterm rehabilitation.
The word «Aparajita» means the womanwith the indomitable spirit. It aptlydescribes the unconquerable spirit of thepeople who have survived the calamity.
What do we want to achieve?The main thrust of the rehabilitation has
been to strengthen the capacity of theaffected community and to minimize theirvulnerability to future emergencies.
VHAI recognizes the intrinsic connec-tion between disasters and development.The disaster traumatically brought to focusall the basic problems of the region. Thecyclone reduced all issues to their funda-mental level and highlighted the inherentweaknesses of the coastal areas of Orissa,
i.e. poverty, underdevelopment and poordisaster preparedness.
What are we doing?After providing the basic relief, the
teams stayed on in the affected areas tomake an assessment of the needs of thepeople and identify key partners for longterm relief and rehabilitation work. It wasdecided to focus operations in 3 blocks, inJagatsinghpur, Kendrapara and Puri dis-tricts.
How are we doing it?Micro-planning exercises, complete
damage assessment and vulnerability map-ping were done in the target areas toappraise and determine the needs of thecommunity.
Aparajita initially started with threeblocks with 15 gram panchayats1 (G.Ps)which later on expanded to 79 G.Ps in June2001. The main areas of intervention were:•• LLiivveelliihhoooodd ssuuppppoorrtt – Cash for work pro-
grammes, kitchen garden and agricul-tural support; fisher folk and post harvestsupport and artisan rehabilitation, suchas, providing raw materials, tools, train-ing and economic support to vulnerablewomen artisans for micro-enterprisesuch as pottery and bamboo basket mak-ing, mat and palm leaf weaving, hand-looms.
•• IInnffrraassttrruuccttuurree DDeevveellooppmmeenntt—restorationand renovation of individual housing,repair of village infrastructure, includingschools, roads, community buildings etc.
•• CCaappaacciittyy BBuuiillddiinngg—training of trainers,training of health workers, training of tra-ditional birth attendants and training rel-evant to treatment in camps.
•• SSaavviinnggss aanndd ccrreeddiitt— support to self helpgroups in dry fish, lime production, matweaving, bamboo crafts, basket makingand vegetable growing.
•• HHeeaalltthh IInntteerrvveennttiioonnss——first aid and cura-tive health services for common ail-ments, safe drinking water and sanitation,awareness generation on preventivehealth aspects, care of pregnant and nurs-ing mothers and referral linkages.
Right from the outset, the main thrust ofthe programme was to include the com-munity perspective in the developmentand implementation of the program; thisenabled community ownership of the pro-gram and contributed to its sustainabilityWith the help of micro planning and base-line survey, the target areas were assessed,beneficiaries were identified, groups andmarketing linkages were formed and withcommunity participation, activities andinterventions were planned and carried outsystematically.
Project implementation was assisted bya number of committees:• Project Coordination Committee• Village Committees• Advisory Committee• Technical Support Committee
Due to timely and effective implemen-tation of the programme, various healthand development interventions, startingfrom 1999 till date, have been carried outsuccessfully; these are outlined in Table 1.
Aparajita activities were monitored cen-trally as well as at the field level. Once amonth direct monitoring by VHAI’s ChiefExecutive and his team was done throughvisits to the operational blocks followed byregular staff meetings where team findings,achievements and constraints were dis-cussed and inputs were provided. The coreteam members undertook Field monitoringthrough field visits at least once a week toeach of the field offices and respective vil-lages. Field officers also send their reportson a regular basis. A field office was set up
Aparajita OrissaAlok Mukhopadhyay1
Abstract: Following the 1999 cyclone, which devastated important areas in the state of Orissa, India, the Voluntary Health Asso-ciation of India (VHAI) established Aparajita as the long-term aid and reconstruction programme. Aparajita aims at empower-ing the local community and building their capacity to recover from devastation and prepare for future natural disasters. Theprogramme operates in three main areas of the state: Jagatsinghpur, Kendrapara and Puri. After an assessment study of thedamage and the communities’socio-economic and health status, Aparajita focused its interventions on livelihood support,infrastructure development, capacity building, savings and credit, and health interventions. This programme has served to estab-lish the basis of a disaster management process, which includes two main components, preparedness and relief. Given the num-ber of natural adversities in India, there is a need to both empower the communities in the management process, as well asinfluence government to support and institutionalise initiatives like Aparajita. (Promotion & Education, 2007, (2): pp)
Key words: capacity building, disaster management, India
1. Chief Executive Officer, Voluntary Health Association of India. Correspondence to: [email protected]
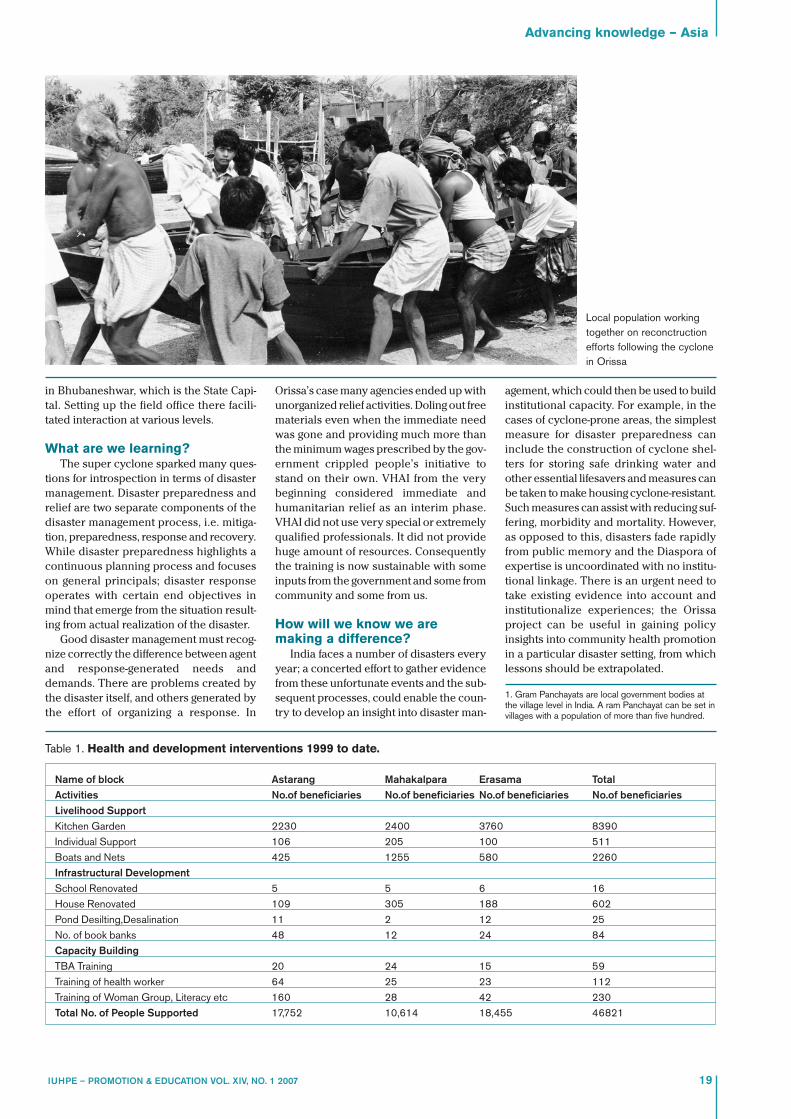
in Bhubaneshwar, which is the State Capi-tal. Setting up the field office there facili-tated interaction at various levels.
What are we learning?The super cyclone sparked many ques-
tions for introspection in terms of disastermanagement. Disaster preparedness andrelief are two separate components of thedisaster management process, i.e. mitiga-tion, preparedness, response and recovery.While disaster preparedness highlights acontinuous planning process and focuseson general principals; disaster responseoperates with certain end objectives inmind that emerge from the situation result-ing from actual realization of the disaster.
Good disaster management must recog-nize correctly the difference between agentand response-generated needs anddemands. There are problems created bythe disaster itself, and others generated bythe effort of organizing a response. In
Advancing knowledge – Asia
19IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
Orissa’s case many agencies ended up withunorganized relief activities. Doling out freematerials even when the immediate needwas gone and providing much more thanthe minimum wages prescribed by the gov-ernment crippled people’s initiative tostand on their own. VHAI from the verybeginning considered immediate andhumanitarian relief as an interim phase.VHAI did not use very special or extremelyqualified professionals. It did not providehuge amount of resources. Consequentlythe training is now sustainable with someinputs from the government and some fromcommunity and some from us.
How will we know we aremaking a difference?
India faces a number of disasters everyyear; a concerted effort to gather evidencefrom these unfortunate events and the sub-sequent processes, could enable the coun-try to develop an insight into disaster man-
agement, which could then be used to buildinstitutional capacity. For example, in thecases of cyclone-prone areas, the simplestmeasure for disaster preparedness caninclude the construction of cyclone shel-ters for storing safe drinking water andother essential lifesavers and measures canbe taken to make housing cyclone-resistant.Such measures can assist with reducing suf-fering, morbidity and mortality. However,as opposed to this, disasters fade rapidlyfrom public memory and the Diaspora ofexpertise is uncoordinated with no institu-tional linkage. There is an urgent need totake existing evidence into account andinstitutionalize experiences; the Orissaproject can be useful in gaining policyinsights into community health promotionin a particular disaster setting, from whichlessons should be extrapolated.
1. Gram Panchayats are local government bodies atthe village level in India. A ram Panchayat can be set invillages with a population of more than five hundred.
Name of block Astarang Mahakalpara Erasama TotalActivities No.of beneficiaries No.of beneficiaries No.of beneficiaries No.of beneficiariesLivelihood SupportKitchen Garden 2230 2400 3760 8390Individual Support 106 205 100 511Boats and Nets 425 1255 580 2260Infrastructural DevelopmentSchool Renovated 5 5 6 16House Renovated 109 305 188 602Pond Desilting,Desalination 11 2 12 25No. of book banks 48 12 24 84Capacity BuildingTBA Training 20 24 15 59Training of health worker 64 25 23 112Training of Woman Group, Literacy etc 160 28 42 230Total No. of People Supported 17,752 10,614 18,455 46821
Table 1. Health and development interventions 1999 to date.
Local population workingtogether on reconctructionefforts following the cyclonein Orissa

Who we are?Shehjar Khoj is a project established by
the Voluntary Health Association of Indiain Kashmir since 1999 with the aim ofimproving health interventions. When tur-moil and conflict began in Kashmir, therewas a collective numbness to respond, gen-erated by fear and unpredictability. Turmoiland conflict of any type and of any kind -social or political - affects every constituentof the society. No social fabric is strongenough to resist the undercurrents of con-flict; the resultant issues manifest them-selves in many ways ranging from dissatis-faction to violence.
It was envisaged that the situation inKashmir would gradually lead to poorerhealth outcomes particularly with state’sreluctance in enhancing the public medicalfacilities in the far off and remote areas andstreamlining the functioning of this sector.1
It was within this context that Shehjar Khojdeveloped a response to this growing crisis.The word Khoj stands for «Quest» or«Search»; Prefixed to Khoj, the word Sheh-jar means «Shade». It aims to define the«Shade of Health Awareness and HealthFacilities» that Khoj project strives to pro-vide to the people of Kashmir against thescorching heat of poverty, negligence anddisease.
What do we want to achieve?Shehjar Khoj has the following aims and
objectives:• Promotion of social justice, equality and
human rights in the provision and distri-bution of health services for all, with anemphasis on the less privileged.
• Strengthening people’s health movementin the state.• Advocating congenial policies and pro-grammes, aimed at improving the healthstatus and quality of life of the people.
What are we doing?In order to develop and achieve the
ambitious aims and objectives of the pro-gramme, the following strategies are imple-mented:• Initiating innovative grass root level sus-
tainable health and development.• Taking action in some of the least devel-
oped pockets of the state.• Capacity building of voluntary agencies
through non-formal orientation trainingand awareness building programmes.
• Influencing policies and programmes fora cost-effective, preventive, promotionaland economically sustainable healthcare system in the state.
How are we doing it?District Budgam was chosen as the first
area of operation. In consultation with thedistrict administration, five villages of TehsilChadoora with a population of over 9,000were identified. Work commenced in thesedistricts in 1999 by training local dais (tra-ditional birth attendants) and educatinggirls in community health, hygiene and san-itation. Inspired by the success of Shehjarproject, another project Shadab was startedin Wakharwan, a cluster of villages in Pul-wama district over 2000-01.By September2004, project activities were extended toanother five villages of Khan Sahib Block ofBudgam district under the banner of KhojProject.
The following activities were conductedin preparation for the interventions:• Meeting district administration, health
and education personnel to discuss plansand activities, areas of operation, andmodes of implementation.
• Establishment of Village DevelopmentCommittees (VDCs) constituted by rep-utable local villagers in order to enhancethe role of stakeholders in community
programmes, thus enhancing the accept-ability of programs.
• Identification of Village Health Workers(VHWs) and leveraging their potential todisseminate health information anddeliver certain health care services.
• Conducting baseline surveys2 to ascer-tain existing socio-economic conditionsand health status in selected villages. Thesurvey revealed that there was a seriouslack of health facilities with no antenataland post-natal arrangements, poor sani-tation, low literacy rates
3and a special
need for mental health programmes.Subsequently, the following interven-
tions were implemented:• Building capacity of traditional birth
attendants (TBAs) in modern methodsand techniques of delivery and repro-ductive health; distribution of Dai’s kit4 toconduct safe deliveries and the estab-lishment of a monthly training and reviewprogramme at Shehjar OPD clinic.
• Providing health services via house-to-house visits, setting up of outpatient facil-ities and sub-centers. Shehjar introducedthe yellow prescription card for its out-door patients; the card is widely recog-nized by all the hospitals in the valleyand allows patients access for referral.
• Organising mass health camps for pro-viding free treatment and medicines topatients with trained VHWs, TBAs andsupervisors assigned to monitor eachpatient for follow up.
• Organising Self Help Groups (SHGs) forfamilies involved in arts and craftsthrough income generation and assistingwith the establishment of Thrift andCredit societies5, which facilitate the dis-semination of health care information.
• Expert counseling, monitoring and treat-ment facilities for people with mental andpsychological problems.
IUHPE – PROMOTION & EDUCATION SUPPLEMENT 2 200720
Shehjar KhojAlok Mukhopadhyay1
Abstract: Turmoil and conflict whether social or political in nature, affects every constituent of the society. No social fabric isstrong enough to resist the undercurrents and dissatisfaction manifested violently or otherwise. The conflict in Kashmir is onesuch phenomenon. Realizing the need for effective health interventions in Kashmir, the Voluntary Health Association of India(VHAI) started Shehjar Khoj project in 1999. The project, among other, aims at promoting social justice and equity in the pro-vision of health services and improvement of the health status for all, with emphasis on the less privileged. The project cur-rently operates in four districts and has implemented numerous interventions, which involved training, motivating and encour-aging active participation of the community, including village opinion makers and health workers. Understanding people’s culturaland ideological beliefs has been a critical factor in enabling the development of locally suited programmes, and therefore theproject’s success. (Promotion & Education, 2007, (2): pp)
Key words: conflict, capacity building, India
1. Chief Executive Officer, Voluntary Health Association of India. Correspondence to: [email protected]
Résumé en français à la page #. Resumen en español en la página #.
Advancing knowledge – Asia

Notwithstanding the turmoil and thesubsequent devastation caused by theOctober 8, 2005 earthquake, several stepshave been taken to ensure sustainability ofthe project.
VHAI in collaboration with State Volun-tary Health Associations (SVHAs) througha Project Advisory committee has beeninvolved in this project at several levels -conceptualizing, monitoring and training.The Programme Coordinator is mandatedwith overall planning, monitoring andimplementation at the village level; theMedical officer is made incharge of healthservices and capacity building of field staff;and the Supervisor guides grass root levelworkers like VHWs, TBAs and volunteers inthe implementation and monitoringprocesses. An award in honor of SSoonnjjooyyGGoossee ––well-known social activist who diedin Assam– was conferred by the Govern-ment of India to Shehjar Khoj project inrecognition of its efforts.
What are we learning?During the turmoil, men became the vic-
tims of their male identity, as a result of thedirect association with their counterpartsin the struggle. The woman suffered fore-most, on the pretext of their female iden-tity as mothers, sisters or wives; sufferingthe emotional and financial repercussionsof the phenomenon. In such situation offear and turbulence the first casualty isalways loss of trust and community spirit.In order to achieve its aims and objectives,every programme has had to build rapport
Advancing knowledge – Asia
21IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
and deep understanding of community’spsyche to fill up its wounds and provide cul-turally appropriate responses.
How will we know we aremaking a difference?
Shehjar Khoj firmly stands on the con-cept of community motivation through thecreation of a “chain” of ever increasing vol-unteers from the grass-root level. In Kash-mir, Shehjar Khoj has overcome the ortho-dox and conservative attitudes of people,while it managed the sociopolitical conflict,
which had created «ideologically oppositegroups» amongst the population. The teamspirit, community motivation and partici-pation garnered by the project are the keyto its success to improve access to healthand the health status of the population,which needs to be maintained by the proj-ect in the future. However over the longterm, it is also imperative to sustain, impro-vise and expand the project targets andareas of operation.
1. Editorial in The Greater Kashmir, June 13, 2001.2. Baseline Survey was conducted in 5 villages of
Shehjar Project by the project team comprising ofTraditional Birth Attendants and Village HealthWorkers (VHWs) to ascertain the existing healthscenario for the reference year 1999-2000.Besides providing information about basicpopulation and other vital statistics of the villages,the survey facilitated the project team in gettingfamiliar with the villagers.
3. See Annexure - 14. Dai’s kit is used by Trained Birth Attendants in
home delivery. The kit contains a soap piece,gauze piece, disposable gloves, sterilized razorblade (cord cutting instrument) and clean cordties.
5. A cooperative society that makes loans to itsmembers at low interest rates.
Project activities Beneficiaries Beneficiariescovered covered Total2000-05 2005-06 2000-06
No. of patients examined and treated 10,927 1729 12656No. of ANCs examined and treated 923 129 1052No of ANCs (high risk) cases referred 112 15 127Immunization of Children 2642 723 3365Village meetings for health awareness 232 60 292Health Education Training for VHWs\TBAs 521 57 578No. of SHGs formed 14 14 28Children treated in School Health Programme 1317 648 1965Total 16,688 3375 20,063
Table 1. Shehjar Khoj Project District Budgam
Name of the village Literacy Rate Sex Ratio (per 1000 male persons)
Male Female TotalZoohama 62.23 35.20 49.01 958Dadompora 46.40 24.54 36.04 901Hanjoora 65.32 37.73 51.90 947Surayar 42.18 23.11 32.92 844Nowhar 43.23 19.35 32.11 880
Annexure 1. Baseline Data (1999-2000) Findings
Training village women in Kashmir through the Shehjar Khoj project

Current health promotion practices in communities – Australasia
Who are we?The Kwaio people are one of the 12 lan-
guage groups on the island of Malaita,Solomon Islands. This group is unique giventhat almost half of the ten thousand Kwaiopeople uphold traditional ways of life in thetropical rainforest clad mountains andretain customary religious beliefs andancestral culture. This is in contrast to 95%of their fellow Solomon Islanders who haveaccepted Christianity. Health services inKwaio were established in the 1950s and1960s by the colonial government and Chris-tian churches; these failed to incorporatelocal understanding or concepts of health inplanning, policy or the delivery of curativeor preventive services. Little changed foralmost four decades. As a result, Kwaio peo-ple faced a stark choice when in need ofhealth services – relinquish fundamentalprecepts of Kwaio culture and religion byaccessing health services or remain true toKwaio beliefs and stay away. Many continueto choose the latter.
This is of particular concern at AtoifiHospital, established by a Christian Churchin 1965 with no Kwaio participation in plan-ning or policy development. Hospital serv-ices are delivered in a single building whichincludes a two-story section. Maternityservices are delivered within the building.This causes problems for many Kwaio whoconsider the entire building a woman’s areaand taboo for men to enter. In addition, thetwo story section allows women to be phys-ically above men – an anathema in Kwaioculture. Thus to enter the building contra-venes fundamental precepts of Kwaio cul-ture, causing the spirits of the ancestors toallow misfortune or illness to befall the indi-vidual or their family. The implication is not
only for clinical curative services, but pre-ventative services including antenatal serv-ices, immunization and other communityhealth initiatives. Atoifi is one of the bestequipped and most respected providers ofhealth services in the Solomon Islands withpeople traveling from across the country toutilize the services it provides. The Kwaiodo not experience the benefits of havingarguably the most respected health serviceon their land. Because Atoifi is the primaryprovider of curative and preventativehealth services for Kwaio, the exclusionthey face causes inequalities in health andcreates antagonism between the commu-nity and Atoifi’s service providers.
Since the establishment of Atoifi Hospi-tal, Kwaio community leaders have wantedaccess to services at the hospital throughmeans that do not cause cultural offence orrequire the relinquishment of ancestral val-ues. However, because of the colonial andChristian paradigm, which has informedthe attitude and practice of many of the hos-pital administrators and deemed Kwaiowho retained ancestral culture and religionas ‘backward’, ‘primitive’and ‘heathen’,requests were not taken seriously. In 2000we (the two authors, a community healthworker, born and raised in the Kwaio moun-tains, and the current chairman of theKwaio Fadanga, i.e. the Kwaio Council ofChiefs, and an Australian public healthresearcher having worked with Atoifi andthe Kwaio since 1992) worked with com-munity groups to document a list of barri-ers faced by Kwaio wishing to access healthservices at Atoifi
1. This was written in Eng-
lish, the language used by hospital admin-istrators as most do not speak Kwaio lan-guage. The list was presented to
administrators with a recommendationfrom the community that a facility be estab-lished at Atoifi Hospital specifically forKwaio people unable to access mainstreamservices. Administrators agreed to pursuea facility on the hospital campus specifi-cally for Kwaio unable to access main-stream services. In 2002, a ParticipatoryAction Research process began, facilitatedby the authors, with the community andhospital staff to collaboratively review thesituation, design and build the facility andcreate relevant policy and procedures.
How are we doing it?A group named the Atoifi Support Com-
mittee comprising community and hospitalleaders was formed to discuss communityhealth issues and plan for the future. Thegroup acted as a conduit for informationfrom the community to hospital leaders andfrom the hospital to community leaders.The culturally appropriate facility was con-ceptualized, designed and driven forwardby members of the Atoifi Support Commit-tee through 2002 with technical assistanceprovided by external agencies. The processof collectively conceptualizing, planningand implementing plans to develop a cul-turally appropriate health service at Atoifiwas the first time leaders from both the com-munity and hospital had collectively sattogether in a mutually respectful way to dis-cuss community health promotion initia-tives for the future. A series of parallel meet-ings were facilitated by the authors withcommunity groups and hospital staff toinform the planning process and providefeedback. This participatory process wasrespectful of all social, cultural and religiousknowledge and responsive to new knowl-
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 2 200722
Reorienting Health Services through Community HealthPromotion in Kwaio, Solomon Islands.David MacLaren1 and Esau Kekeubata2
Abstract: When ethnic minorities adhere to cultural practices which mark them as unique, structural impediments within healthservices can deny access and significantly add to the burden of disease. This is particularly pertinent if the development of healthservices is not done in partnership with all population groups in the area. This is the case at Atoifi Hospital, which structureprevents certain Kwaio people (Solomon Islands) from receiving benefits of hospital services and maintaining cultural beliefsat the same time. A Participatory Action Research process was used to collaboratively work with health service providers andcommunity groups to review the situation, design and build a health facility with both medically and culturally appropriate poli-cies and procedures. The Participatory Action Research process of collectively looking, thinking, planning and acting towardsreorienting health services to become more culturally appropriate at Atoifi was the first time leaders, from both the communityand hospital, had collectively sat together in a mutually respectful way to discuss community health promotion initiatives. Theproject was complete in 2006 with collaboration and dialogue between both groups proving vital to its success. Numerousindicators are present that the culturally appropriate health facility is making a difference, not only in terms of the hospitalusage by all, but also for the feeling of “community ownership.” (Promotion & Education, 2007, (2): pp)
Key words: dialogue, minority groups, participatory action research, culturally appropriate
1. Kafurumu Health Centre c/o Atoifi Hospital, East Kwaio, Malaita Province, Solomon Islands ([email protected]).2. School of Public Health, Griffith University, Australia. Correspondence to [email protected]

edge created through the process. Thisprocess was occurring through a particu-larly tumultuous time in Solomon Islandshistory. The years 1998-2003 saw civil unrestbetween the peoples of Malaita and Gudal-canal Islands known as the ‘Ethnic Tension’.This included the overthrown of the demo-cratically elected government in June 2000by rebel elements of the Royal SolomonIslands Police and a militant group calledthe Malaita Eagle Force. This resulted in thecrumbling of law and order and almost totalcollapse of government services, includinghealth services. Being a non-governmenthealth service, Atoifi was one of the onlyhospitals in the country offering full serv-ices. In Early 2003 just months before thePacific Islands Forum initiated the RegionalAssistance Mission to Solomon Islands(RAMSI), a multinational force made up ofAustralian, New Zealand and Pacific Islandmilitary and police got involved to re-estab-lish law and order and the machinery of gov-ernment violence, which also affectedAtoifi. In May 2003, the Australian businessmanager of the hospital was murdered. Thiscaused most of the staff to flee the hospitalcampus, where most resided. This resultedin a near collapse of the organization andnew projects, including the culturally appro-priate health facility, were postponed untilthe situation stabilized.
Given the community engagement strate-gies used in the PAR process, the authorswere requested and participated in theprocess to facilitate dialogue betweenchurch and hospital administrators andcommunity groups to address the uncertainand volatile situation. In late 2004, after staffreturned, a RAMSI police post was estab-lished at Atoifi and some stability returnedand the process to establish the culturallyappropriate facility was re-started. Planswere made and construction began in 2005.All building materials were either donateddirectly by community members or pur-chased from community contributions. Twobuildings were constructed of local materi-als, one for the general community and onefor women’s services (including antenatalservices). They were officially opened inJune 2006. Both are now used by Kwaiowithout causing cultural offence or relin-quishing religious beliefs.
What are we learning?Numerous lessons have been learned
through the Participatory Action ResearchProcess, which resulted in culturally appro-priate health services for the Kwaio at AtoifiHospital. One of the key lessons was theimportance of participation.. It was onlythrough participation and dialogue that hos-pital administration and community leadershad mutual understandings of important
Advancing knowledge – Australasia
23IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
issues to each group. Prior to this projectthere was no process through which com-munity leaders and hospital administrationcould engage in meaningful dialogue. Theresult of which was historical mistrust, sus-picion, stereotyping and misinformedassumptions. Through the process of engag-ing in meaningful dialogue as equals work-ing towards a common goal, both groupsbecame aware of the social, cultural, spiri-tual and economic complexities the otherfaced in planning health services. Under-pinning this participation was the impor-tance of flexibility. To be flexible, both interms of the approach adopted and theresponse to unexpected events allowed theproject to continue through a dynamic andvolatile period of history. Having the capac-ity to deal with complexity allowed allinvolved to acknowledge, respond, valueand incorporate complex changes in theproject rather than trying to ‘control’them.This enabled the project to ultimately cometo fruition. We learned that if the project wastruly community owned and driven it wouldbe able to adapt to complex and dynamicsocial, cultural, political, religious and eco-nomic situations. This required periodichalts in progress, but was critical to the pro-ject’s long term successes. The role of theresearcher/facilitator being a catalyst wasalso an invaluable lesson learned. Althoughthis community health promotion projectwas run as a Participatory Action Researchproject in collaboration with an Australianpublic health researcher, the researcheralways saw himself as a facilitator of thechange process, rather than an external‘expert’directing the project. Researchersinvolved always strove for the process to bewith and by persons, not on or to them.Being true to this process allowed theresponsibility for the project’s successes andsustainability to lie with the hospital andcommunity, not the researcher/facilitator.A final major lesson learned throughout theproject was the importance of local leader-ship.. The reality of a culturally appropriatehealth facility would never have been real-ized without visionary leadership in theKwaio Council of Chiefs. As community lead-ers they exemplified how oppressed peo-ples can articulate the situations of oppres-sion in which they live and take actions totransform such oppressive situations.
How will we know we aremaking a difference?
Change at several levels show that theculturally appropriate health facility isindeed making a difference. Firstly, theKwaio people are using the facility. Priorto the official opening in June 2006, a seniorchief who was ill sought treatment at thefacility. He was admitted there for several
weeks. This was a powerful signal of sup-port by senior community leadership andopened the way for others to use the facil-ity after its official opening. Subsequently,there has been ongoing ‘community own-ership’and a feeling of having a facility thatis ‘in and of Kwaio’on the hospital campusfor the first time. An outcome of this strongfeeling of ownership by the community isthat relatives of people admitted there arestaying for several days, often sleeping inthe facility, as is normal in a village setting- of course, this brings a new set of chal-lenges for hospital administrators. The con-struction of the facility has created a feelingof partnership and goodwill between thecommunity and hospital leadership andhas stimulated ongoing debate for the needto provide more culturally appropriatehealth services for all sectors of the com-munity that address the social and culturaldeterminants of health for all. This includesthe limitations of such initiatives andchange in policy and practice that isneeded to reorient health services. Giventhe strong medical, religious and cultural
paradigms present, this will be an ongoingchallenge. A doctoral thesis has been pro-duced that outlines the intricate historical,political, cultural and religious contexts inwhich health services operate in Kwaio anda detailed description and analysis of theParticipatory Action Research process andoutcomes2. This document is being used asa basis for further collaboration and evalu-ation of the facility by Atoifi Hospital, KwaioCouncil of Chiefs and university collabora-tors. A final indicator of the difference beingmade by this community health promotionproject is the numerous requests theauthors have received to present theprocess, experiences and reflections atlocal, national and international forums.
1 MacLaren, D. (2000) Kastom and Health: A Studyof Indigenous Concepts of Custom, Health andAppropriate Health Care within Kwaio, Malaita,Solomon Islands. 2 MacLaren, D. (2006) Culturally Appropriate HealthCare in Kwaio, Solomon Islands. An Action ResearchResponse. PhD thesis. Griffith University.

Who are we?Murri Grannies (Aboriginal grandmoth-
ers) in a regional town in northern NewSouth Wales are considered the backboneof the community. Many find themselves inthe role of primary caregiver and discipli-narian to their grandchildren and greatgrandchildren, meeting their physical,financial and social needs. This is on topof their need to care for themselves. Nev-ertheless, they take on the role willinglybecause they want their grandchildren tothrive and to reach their full potential. Notsurprisingly, the Grannies’own needs areoften neglected and they become stressedand anxious.
In early 2004, the Counselor at the localAboriginal Medical Service (AMS) noticedthat many of the Murri Grannies who cameto see her suffered from stress and anxietyassociated with their care-giving role. Oth-ers were distressed by the lack of respectthat Murri kids in the community showedthem as elders. The Counselor talked aboutthis with Aunt
1Shirley, the Aboriginal Men-
tal Health Worker at the AMS and a Grannieherself. Together, they initiated an eight-week program for the Grannies called Relaxto the Max. It involved relaxation sessionsand discussion on how to care for them-selves mentally, emotionally and spiritually,as well as including a bit of pampering, suchas a visit to the hair salon. The program hadan overwhelmingly positive response andtogether, the Grannies with the Counselorand Aunt Shirley decided to start a supportgroup for themselves.
The name given to the Support Group,‘the Granitators’, was chosen as it identifiedthe strength and determination of theGrannies. Led by Aunt- Shirley, the group
IUHPE – PROMOTION & EDUCATION SUPPLEMENT 2 200724
The Graniators support group programEmily Sullivan1, Ilse Blignault1, Aunt Shirley Duncan2 and Lisa Jackson Pulver1.
Abstract: Aboriginal grandmothers (grannies) in many communities throughout Australia are considered the backbone of thesocial structure. This is the case for the Murri1 Granies in a town in regional eastern Australia. Many of these women are alsotheir grandchildren’s primary caregivers and disciplinarians, and sometimes this role is detrimental to their own care and well-being. As a response to this stress, the local Aboriginal Medical Service (AMS), which includes a comprehensive primaryhealth care facility, began promoting the program Relax to the Max to the Grannies as part of the holistic care they offer. Sincethese humble beginnings some three years ago, the group has grown to become the Graniators support group. In addition totheir initial work of supporting each other, the group extended their field of action to the entire community to address social issues,particularly those around youth and children. To complement and strengthen their initiative, the Graniators partnered withother organizations in the community including the police, the municipal council, and the state government’s department of hous-ing, the local primary school, and a special youth service group. The program’s evaluation has proved to be extremely positivein providing others in the community a clear and positive formula for driving change at a grass roots level. (Promotion & Edu-cation, 2007, (2): pp)
Key words: Aboriginal grandmothers, youth, partnership
1. Muru Marri Indigenous Health Unit, School of Public Health and Community Medicine, UNSW. Correspondence to Emily Sullivan: [email protected]. Mental Health Team, Pius X Aboriginal Medical Service, Moree, NSW, Australia.
Résumé en français à la page #. Resumen en español en la página #.
Advancing knowledge – Australasia
decided to meet once a fortnight for aboutfour hours, on an ongoing basis, providinga support network and social outlet forabout 25 Murri Grannies in the local area.
What de we want to achieve?The initial aim of the Group was for the
Grannies to support each other in address-ing the daily issues they faced. As time wenton, the Grannies realised they had a com-mon desire in wanting to reach out and todo something about the problems affectingtheir grandchildren, families and commu-nity. In early 2005 the Grannies visited the‘Linking In’project in another regional townthat ran activities to support young peoplein the community. This was a significantevent as it provided them with the motiva-
tion and inspiration to expand their ownfocus. From this point, the Graniators’aimgrew to include assisting the community toaddress social issues, particularly aroundyouth.
What are we doing?Every second Tuesday, the Grannies
meet at a place organised by the AMS. AuntShirley sometimes organises guest speak-ers and at other times invites the Granniesto follow the Relax to the Max tape. Thismeeting provides the Grannies with time-out to relax away from the grandkids, anda chance to reminisce about the old days onthe Christian mission station together.Building friendships and trust amongst thegroup has been an important aspect of the
meeting as it has enabled the Grannies toshare their stories and problems with eachother and they now feel comfortable turn-ing to one another to both offer and receiveadvice and support.
As well as partnering with the AMS, theGraniators have established partnershipswith several organizations in the commu-nity including the police, the municipalcouncil, and the state government depart-ment of housing, the local primary school,and a special youth service group. With thesupport of these organisations, they holdthe Brekkie Club every weekday for up to30 school children where the Grannies takeit in turn to prepare breakfast. Once amonth the Grannies assist the local policewith a movie night for the families of thecommunity. In addition, the Grannies areoften invited to contribute to communityactivities such as the Croc Eisteddfod andCarols by Candlelight.
What are we learning?At the end of 2005 the Graniators’pro-
gram was formally evaluated as part of alarger project to provide on-site training andcapacity-building for AMS staff in serviceplanning and evaluation. Aunt Shirley and
Advancing knowledge – Australasia
25IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
the Grannies were involved in the evalua-tion of their own project and in compilingthe community report2.
The evaluation documented positivechanges in both the Grannies themselvesand in the community. The Grannies havegained strength and confidence and act asnew role models for the community. Sev-eral informants commented on the way theGraniators are raising the spirit of the com-munity.
Many people have benefited from theGraniators’work. For example, the Grannieshave built friendships and mutual supportwithin the group, and formed new and pos-itive relationships with the police. Kidsfrom the Brekkie Club not only have a nutri-tious meal in the morning and get to school,but also now know they have more thenone Granny to love them.
Most importantly, the Grannies havenew learnings such as:• The importance of the friendship and
bond between them in achieving successout in the community and to their con-tinuing as a support group for each other.
• The value of taking small steps and work-ing within their own limits.
• The usefulness of having frequent and
regular meetings where they focus ontheir initial aim of supporting each otherto avoid ‘burn out.’
• The worth of building partnershipswithin and outside the Murri communityin the town and working together toachieve shared goals.
• The fact that challenges can be over-come. In facing the challenges, they havelearnt new skills such as networking, andhave grown stronger.
How will we know we aremaking a difference?
Thinking and talking about the issuesand reflecting on what others said about theGraniators allowed the Grannies to seemore clearly where they come from, howthings are going, and how they might workmore effectively in the future. The Granniesare proud of them, and are keen to sharetheir success with others.
1. MacLaren, D. (2000) Kastom and Health: A Studyof Indigenous Concepts of Custom, Health andAppropriate Health Care within Kwaio, Malaita,Solomon Islands.
2. MacLaren, D. (2006) Culturally Appropriate HealthCare in Kwaio, Solomon Islands. An ActionResearch Response. PhD thesis. Griffith University.
Current health promotion practices in communities – Latin America
Who we are?Motuca Healthy Municipality project
was set up in 2002 for a total duration ofthree ears by the Ministry of Health in col-laboration with the Municipality of Motucaand the School of Public Health, Universityof Sao Paulo. The main objective was to cre-ate a new managing system with a partici-patory approach to improve the quality oflife of the population.
The municipality of Motuca is located inthe Northwest part of São Paulo State, Brazilcovering an area of 230 square kilometerswith a total population of 3,872 inhabitants.According to the Brazilian Institute of Geog-raphy and Statistics (IBGE), the populationincreased by 12.47% during the period 1993-2000... Majority of the population (63%)lives in the urban areas, where social andcommercial services are available and
Motuca healthy municipality project: building together abetter futureRosilda Mendes1 and Fabio Falvo2
Abstract: The Brazilian Ministry of Health in collaboration with the Municipality of Motuca and the School of Public Health atthe University of Sao Paulo set up in 2002 the Motuca Healthy Municipality project with the aim of improving the population’shealth and quality of life. The project used a participatory and holistic approach, which addressed the social determinants andstructural inequities, and called for strategies of community empowerment, social participation, intersectoral networking andgood governance. All local and public actors from rural and urban areas were consulted and participated in the project to col-lect information on the living conditions and challenges to better well-being. This participatory methodology allowed in turn devel-oping cultural and socially appropriate initiatives to improve local governance and standards of living on a long-term basis.Although there is still the challenge to maintain the momentum and reenergize the efforts, the project serves as a model for fur-ther efforts to evaluate the effectiveness of participatory intervention and research methodologies to promote health and well-being in communities. (Promotion & Education, 2007, (2): pp)
Key words: participatory methodology, empowerment, health promotion
1. CEPEDOC Healthy Municipalities, Faculty of Public Health, São Paolo University, São Paulo, Brazil2. Secretary of Health, Motuca, São Paulo, Brazil
small industries exist. Four groups of set-tled-out landless people represent 37% ofthe population. This high population in therural area is different from the rest of Brazilwhere, in general, usually only 18% of thepopulation lives rurally. In the 1980’s theregional government allotted ownership ofgovernment-owned land to these people,which is where they now grow sugar caneand other agricultural products.

Advancing knowledge – Latin America
mental, housing, economic, recreational,and public services aspects. Through thesethe broad dimensions of the city were elab-orated. For instance, it enabled an under-standing of distribution of illiteracy, whichcontrary to popular belief, was in the urbanareas. Currently, the Committee is priori-tizing problems and defining participatoryevaluation.
What did we learn?To-date, three Municipality Conferences
have been held with the overall objectiveof presenting the process-related findingsand other related information to the popu-lation, specifically, and to other cities in theregion, in general.
This process has examined differentinterests and abilities that shape politicalagendas, and the possibility of creatingalliances and networks to strengthen localgovernance to improve living conditions.The challenge now is to reenergize theseefforts, to think through the problemstogether focusing on improving polices andinstitutions that better serve the needs andinterests of the population. Empowermentof the groups can be considered the great-est lesson learned.
How do we know we can makedifference?
This Project serves as a model for fur-ther efforts to evaluate methodologies inparticipatory intervention and research.Process and outcome data are necessary inorder to establish the effectiveness ofhealth promotion initiatives. The questionof who conducts the evaluation is impor-tant. It must include all the social actors.Linking intervention in the planning, imple-mentation and evaluation can be useful tocontribute to the capacity to promotehealth and ensure continuation of the inter-vention. It means we have established away to better understand the facilitatorsand barriers in the initiative, and to betterplan for sustainability of efforts withinchanging political contexts.
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 200726
The economy of the municipality isbased on a large local sugar cane process-ing plant. In the period between March andNovember each year the processing plantalso employs 1440 local workers. Cultivationof oranges and the production of carnaubawax contribute to the local economy as well.Additionally, there is a factory which pro-duces hand-woven carpets and rugs.
In terms of health, the main strategy forstrengthening primary health care is theHealth Family Program, which is run by theState of São Paulo in collaboration with theFederal Ministry of Health. The municipal-ity provides other primary health care serv-ices in addition to this and takes responsi-bility for transporting patients in need foradvanced care to a neighboring city -Araraquara, which is 40 kilometers away.
What did we want to achieve?In its broadest definition, this project
encompassed a holistic approach whichaddressed the social determinants andstructural inequities, and called for strate-gies of community empowerment, socialparticipation, intersectoral networking, andgood governance. Through interactionsbetween government and civic represen-tatives, policies and social conditions,which promote good governance at a locallevel, were constructed. Technical and edu-cational cooperation created an enablingenvironment in which all the participantsfocused on the needs of the future.
How did we do it?Participatory governance strategies
were created in order to involve differentsocial actors. Initially, four workshopscalled Oficinas de Sensibilização - two in theurban area and two in the rural area- wereconducted; based on these workshops, acollective vision for the city was developed:«our city nowadays» and «our city in thefuture». Collecting and analyzing the infor-mation from these groups allowed a betterunderstanding of the potential for and bar-riers to local governance to improve thestandard of living on a long term basis. Sec-ondly, a Healthy Municipality Committeewas established with representation fromthe professional community, decisionsmakers and community members. A par-ticipatory approach was used to integratethe local committee in order to create acommon vision for the city and to involvethe settled-out landless people, previouslyexcluded from local policies.
Other methods included recognizing thehistorical context of the city. More than 500historical photos were exhibited in a localcommunity center; in addition, communitythematic maps were created for the ruraland urban areas, representing environ-
27IUHPE – PROMOTION & EDUCATION SUPPLEMENT 2 2007
What is this initiative about?The United States Agency for Interna-
tional Development in Bolivia (USAID/Bolivia) created a Health Project in Septem-ber 2002, with the overall aim of improvingthe health of the Bolivian population to beimplemented by PROSALUD, a Bolivian NGOwho is being working in the health sectorsince 1986. The project is entitled Partners forDevelopment (PfD), which comprises threecomponents: small grants, technical assis-tance, and management of data base sys-tems. The small grants component wasdesigned to benefit the public sector, NGO’sand Grass-root Community Organizationsthrough a competitive process.
In the beginning (2003), USAID/Boliviathrough the Integral Health Project PROSIN,and since 2005 through the PfD via its smallgrants component, supported a Commu-nity Participation Strategy (CPS) projectover a three year period (April 2003 – June2006) in 35 municipalities as follows:
Number of interventionsDepartment Rural Municipalities Sub-urban Beni 3 1Chuquisaca 5La Paz 11Pando 1 1Potosí 9Tarija 3 1
The project was led by a psychologistwith expertise in working with communi-ties and was implemented by 15 nurses.
The project aims to increase health serv-ice utilization with a particular emphasis onempowerment of women, strengthening oflocal organizations and increasing thehealthy practices and demand for healthservices. The total contribution to this proj-ect by USAID/PfD was US $ 280,000.
What is the approach used?The Community Participation Strategy
has been implemented in the first stagethrough 73 community based educationalsub-projects including basic project mana-gerial training to selected women, someoffice furniture and materials, basic kitchentools for community based organizationsand equipment for strengthening healthservices.
Each sub-project comprises two five-dayworkshops to train women health promot-ers as cascade trainers. Then, the healthpromoters replicate the knowledge in 19sessions three hours each to the women incommunity workshops. The training isrelated to reproductive health and familyplanning in the following themes: contra-ception, pregnancy and delivery, sexualorgans infections, women reproductive andsexual rights, self-esteem among others.Women from indigenous cultures, likeAymara1, Quechua2 and others wereinvolved in this process.
As an output, 219 women from commu-nity based organizations have been trainedin basic project management; another 1080women have been trained as health pro-
moters, which in cascade replicated whathave learned to about 30,000 women of thecommunities who have received training inreproductive health and family planning(RH/FP).
In relation of the educative materials,the ones developed by the NGO ““MMaannuueellaaRRaammooss (Lima, Perú)”” served as the tools ofintervention for this project; these wereadapted to the local setting and validated.
In the second stage, as three new sub-projects, the Community Participation Strat-egy trained the women health promoters,in different but related themes as a contin-uation of first stage, including leadership,negotiation, small projects management,advocacy, and community participation.
As another result, six active networks ofwomen health promoters have been estab-lished as well as committees of sexual andreproductive rights defenders were estab-lished; these networks and committeesgained insight into community needs, nego-tiated community requests with respectivemunicipalities’governments and developedconjoint action plans for quality of healthservices improvement.
SSuucccceessss hhiissttoorryy:: The women health pro-
moters’network of sub-urban area in
Bermejo, Tarija (38,000 people munici-
pality) negotiated with the local Munici-
pal Government in November 2005, the
young people orientation center imple-
mentation, which is giving today orienta-
tion in RH/PF in coordination with local
health services. In average, every month
Empowered women from rural areas of Bolivia promotecommunity developmentRoxana Ríos1, Catón Olmedo2, and Luis Fernández3
Abstract: The United States Agency for Development in Bolivia (USAID/Bolivia) created in 2002 PROSALUD- Partners forDevelopment Project (PfD) with the aim of improving the population’s well-being. The project used three components: smallgrant scheme, technical assistance and database system management. Through the small grants scheme, the PfD supporteda Community Participation Strategy (CPS) project over a three year period. The project involved the rural areas of six Boliviandepartments and sub urban areas of three Bolivian cities. The main objective was to increase health service utilization with aparticular emphasis on empowerment of women, strengthening of local organizations and increasing the demand for health serv-ices. Women from both the urban and rural areas, and from different indigenous groups, were trained in project management,health promotion, reproductive health and family planning, advocacy and community participation. Participatory methodolo-gies have allowed empowering women in decision making and capacity building throughout the entire project process. The expe-rience shows that it is important to work with formally established grass-root community organizations and strengthen leader-ship within them. Additionally, the sub-projects demonstrated that interventions are more successful when promoters speak andwrite native languages, women are more motivated and empowered, projects are designed to be responsive to daily necessi-ties identified by the communities and health services are culturally suitable. A preliminary evaluation, in both quantitative andqualitative terms, shows an overall improvement in health knowledge and practice, and utilization of health services. (Promo-tion & Education, 2007, (2): pp)
Key words: empowerment, participatory methodology, women
1. Psychologist, Community Participation Strategy Coordinator2. M. Sc., Qualitative and quantitative project impact Researcher3. MD, Partners for Development Project Director
Résumé en français à la page #. Resumen en español en la página #.
Advancing knowledge – Latin America

Advancing knowledge – Latin America
around 80 young people seek the services
of the orientation center. In addition,
women health promoters offer orienta-
tion in contraception and sexual/repro-
ductive rights to the post delivery women
at local hospital services.
After the project conclusion, the pro-moters of the CPS, are also raising fundsfrom different donors for the implementa-tion of new local development projects.This can be stated as another result like“local capacity built”.
How are we doing this?This project employs participatory
methodologies for the empowerment ofwomen in decision making and builds theircapabilities in the whole project process:from problem analysis and identificationto the design and implementation of localsolutions. Specific areas of focus include:situational analysis, communities’selectionfor intervention, self diagnosis, project pro-posal elaboration, management and evalu-ation. This enables an understanding of thewhole process of community project man-agement and its instruments.
What are we learning?Implementation of the project has
enabled an understanding of communityhealth promotion in a specific setting. Theexperience shows that it is important towork with formally established communitybased organizations and strengthen lead-ership within them. The results of such anintervention are directly proportional to thecapacity of the promoters; however, betterresults can be gained if promoters speakand write native languages, when motiva-tion amongst women is higher, when sub-projects are designed to be responsive today to day necessities identified by com-munities, when health services are cultur-ally suitable and with the participation ofGrass-root Community Organizations, par-ticularly women have better relations interms of negotiations with local authorities.
How do we know we are makingthe difference?
A quantitative, qualitative and costrelated study to evaluate the effectivenessand empowerment of CPS was conductedin the 2005. Results of the qualitative com-ponent of the study showed an increase inante natal care, PAP screening and familyplanning methods provision, and decreasein the gap between the health services andcommunities, having in mind the sexualand reproductive women rights. Resultsalso showed that the local authorities weremore likely to provide financial support toimplement the process. In addition a visi-
ble change was observed in knowledge, atti-tude and practice of couples with respectto negotiating for and exercisinghuman/reproductive rights.
The quantitative component of the eval-uation yielded the following results:
Effectiveness average of 37%3, with thefollowing variables: 73.5% of the womanshowed willingness to use RH services, 11%women accepted and used family planningmethods (FP), 11.8% assisted ante natal careand delivery services, 27.6% reported gen-der equity relationships with their couples,and 55.8% reported gender and family rela-tions without violence.
Empowerment average of 31.4% with thefollowing variables: 50.9% realized healthypractices, 39% had knowledge about pre-vention of intra-family violence, 27.6%referred to improving communication withtheir couples; in addition, the demand forRH services have increased by 9.7% in rela-tion to previous year (2004).
The average training cost in this projectper woman was US $ 24.
Implications for broaderapplication
The two phases of the CPS strategyinclude training (including the selection ofproject intervention areas), advocacy andlocal activities and consolidation; the latteralso includes strategies to establish finan-cial sustainability. Consolidation of theRH/FP component of the program also pro-vides an opportunity to integrate other ele-ments such as environmental interven-tions. The methodology has shown modestsuccess in Bolivia and can be adapted toother settings, with careful attention to spe-cific characteristics of each country such ascultural and working practices, health serv-ices accessibility, and the regulatory envi-ronment.
1. The Aymara are a native ethnic group in theAndes and Altiplano regions of South America;about 2.3 million live in Bolivia, Peru, NorthernChile, and Northeastern Argentina (in particular inSalta Province). They lived in the region for manycenturies before becoming a subject people ofthe Inca, and later of the Spanish in the 16thcentury. (Wikipedia, free internet encyclopedia).
2. Quechua (Runa Simi; Kichwa in Ecuador) is aNative American language of South America. Itwas the language of the Inca Empire, and is todayspoken in various dialects by some 10 millionpeople (Quechuas) throughout South America,including Peru, South-western Bolivia, southernColombia and Ecuador, north-western Argentinaand northern Chile. It is the most widely spoken ofall the languages of the Indigenous peoples of theAmericas. (Wikipedia, free internet encyclopedia).
3. By means of Net Aggregation Method:% Effectiveness = ((% measured in ex postevaluation - % base line) / (100 - % baseline)*100.
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 200728

29IUHPE – PROMOTION & EDUCATION SUPPLEMENT 2 2007
Who we are?We hear much about the Amazon and its
natural resources, but little is said of itsinhabitants, especially the forest peoples,the majority of which are ‘caboclos’–descendents of Indians who live in rural,often isolated and difficult to access areas.
These people partly subsist on hunting,fishing, the collection of forest products,growing manioc and other regional crops,but no longer manage to guarantee theirown subsistence due to the impacts ofdeforestation in the Amazon.
Amthough public services offered byrespective municipalities are improving,there still appears to be a major shortfall.This is evidenced by some of the key socialsector indicators of the region; 60% of thepopulation is under 18 years of age, ofwhich only 7.5% manage to complete sec-ondary education. Health is one of the keychallenges in the social sector domain atthe community level. Preventable diseaseslead to significant mortality and morbiditydue gaps in the delivery of primary healthcare services (Gusmao, 2002). Infant mor-tality is high and Infant deaths account for15.7% of all deaths in the community; this isreflective of regional health disparities inBrazil given that this is almost double thenational average of 8% (Gusmao, 2002). Themajority of these deaths are the result ofpreventable diarrhoeas or infectious dis-eases.
The population lives in a regionextremely rich in natural resources,; how-ever at the same time, they suffer fromincreasing impoverishment. This is mostlydue to the lack of investment in the popu-lation’s own potential. However, thesegroups still maintain a strong sense of com-
munity, solidarity and self initiative and areable to effectively mobilize and worktogether to resolve their own problems, ifand when given the opportunity.
The Health and Happiness Project (PSA)was created in 1987, taking the local realityof these populations as a starting point, theproject is grounded in the belief that a crit-ical component of safeguarding the Ama-zon, relates to guaranteeing living condi-tions for the forest peoples. PSA is anot-for-profit organisation, which works topromote integrated and sustainable com-munity development in riverside locationson the banks of the rivers Tapajós, Ama-zonas and Arapiuns in the West of Pará,Brazil.
PSA further built on the work of a med-ical doctor and an art-educator who hadexperience working with riverside com-munities in the municipality of Santarémbetween 1984 and 1985. They created a non-governmental organisation, PSA, to guar-antee the continuity of the actions in abroader and more independent mannerand without party-political connections.
In 1987 cooperation agreements securedby BNDES- Banco Nacional de Desenvolvi-mento Econômico e Social, from FederalGovernment, which permitted the work tocommence with16 pilot communities. TheParticipatory Planning highlighted healthas one of the biggest challenges and fromhere, the other programmes of the Healthand Happiness Project were developed.
How are we achieving our aim?Education and community participation
were key elements of the project’s actionsand brought immediate results for thewhole population, taking advantage of
resources from the region itself. Commu-nity leaders, health workers, traditionalmidwives, rural producers, women, teach-ers, children and young people built theircapacity through training to become train-ers. The project invested in basic sanitation(chlorine, filters, toilets, wells and adaptedwater systems). Community events pro-moting the health of the children, withthree-monthly vaccination campaigns wereinitiated. Rural farmers received technicalassistance to increase the availability offood stuffs produced using agro-ecologicalpractices. Groups of women were involvedin activities to promote reproductive healthand combat malnutrition with the con-sumption of local plants of high nutritionalvalue. In the schools, teachers and childrenparticipated in health and ecology work-
Promoting health and happiness in the Brazilian AmazonCaetano Scannavino1 and Rui Anastácio1
Abstract: With the motto«Health, happiness of the body. Happiness, health of the soul», the Health and Happiness Project (PSA)works to promote integrated and sustainable community development in parts of the Brazilian Amazon. PSA grew out of localworkers’personal experience in collaborating with communities and the need for sustainable actions for their future develop-ment. It was established as a not-for-profit organization in 1987. PSA started off by implementing strategies that would increasethe health status of the population, which was identified as the biggest challenge, to then extend to other areas of develop-ment. Education, training and community participation were key elements of the project’s actions, which included basic sani-tation, reproductive health and child health, technical assistance in agricultural practices and youth empowerment through com-munications, among others. Once the health structure was established, the work moved on to new priorities related to education,economic production, protection of the environment and community management in the medium and long terms. The project’ssuccess has helped to institutionalize the practices and today it reaches a total of approximately 5,000 families distributed across150 rural communities in the mid- and low-Amazon region. (Promotion & Education, 2007, (2): pp)
Key words: health promotion, community health, development
1. Projeto Saúde & Alegria, Brazil. Correspondence to Caetano Scannavino, Project Coordinator: Rua Mendonça Furtado, 3979, Santarém-PA, Cep 68040-050, Brazil.([email protected])
Résumé en français à la page #. Resumen en español en la página #.
Advancing knowledge – Latin America
Mobile Health Unit (Abaré): monthly visits tothe communities to promote primary healthcare for 2.500 families in the municipalities ofSantarém, Belterra and Aveiro, a consortiumbetween PSA and the Municipal Councils.

Advancing knowledge – Latin America
shops. A communication network wasdeveloped with the youth, where they weretrained as reporters allowing them to pro-duce, exchange and disseminate educa-tional materials via community newspa-pers, radios and videos.
The project tries to take a positive in-takeon promoting health, instead of disease-ori-ented, which is where the term «happiness»comes into play in the organization’s name.As a main strategy when visiting communi-ties, team members and community mem-bers use the Great Mocorongo Circus. Therepresentations of the circus include music,poetry, educational and cultural sketches topromote healthy behaviors, such as, breastfeeding, the use of oral re-hydration therapyand hygiene, among other.
What are we learning?These simple and culturally appropriate
education methods had a very positiveimpact on the communities, who not onlybegan to change their health practices, butalso became more stimulated to actively par-ticipate and influence other areas of theirdevelopment. Once the health structure wasestablished, the work could move on to newpriorities related to education, economicproduction, protection of the environmentand community management in the mediumand long terms. PSA with the community’sinvolvement in the planning and implemen-tation created integrated development pro-grams, as shown in Figure 1.
How do we know we are makinga difference?
The lessons learned made it possible todevelop exemplar and culturally-adaptedsocial development technologies, whichare low in cost, high in impact and replica-ble in other regions and contexts. Conse-quently, in 1999, PSA started to graduallyincrease the communities it worked in.
Faced with a larger scale program, cer-tain principles for successful project devel-opment were established, i.e.:• working in partnership with government
bodies and other existing developmentactors to transfer social technologies;
• programmes are readapted in order to beintegrated as public policies;
• training trainers is prioritized;• the concept of territorial communities is
reinforced to encourage self-managementand social control, focusing on strength-ening inter-community federations.
As reflected in Figure 2, over the yearsit has been possible to significantly improvethe quality of life indicators in partner com-munities, according to comparative databetween areas served and those not servedby PSA (Souza Lemos, 2000.)
At present, PSA works directly in three
municipalities – Santarém, Belterra andAveiro – reaching a total of approximately5,000 families distributed across 150 ruralcommunities in the mid- and low-Amazonregion. PSA is also increasingly consulted bygovernmental and non-governmental bodies,from the Amazon and beyond, to provideadvice on the replication of its experiences.
ReferencesGusmão, Joana Buarque, (2002) Pesquisa de
Saúde Comunitária, Centro de Informação ePesquisa/PSA.
Souza Lemos, Jose de Jesus (2000) DIAGNÓSTICO AMBIENTAL, SOCIAL EECONÔMICO NAS ÁREAS DE ATUAÇÃO DOPROJETO SAÚDE E ALEGRIA NOSMUNICÍPIOS DE SANTARÉM E BELTERRA,PARÁ (Environmental, Social and EconomicDiagnosis in the Areas Assisted by Health &Happiness Project at the Municipalities ofSantarém and Belterra, State of Pará Researchpaper. Federal University of Caera, Brazil.
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 200730
Mocorongo Grand Circus: a small mambembe traveling theatre presented by rural residents withmusic, poetry, educational and cultural skits, communicating the content in the communities’ownlanguage
Mocoronga network: youth’s communicationinitiative for education- radio communicationsand programmes and internet access points
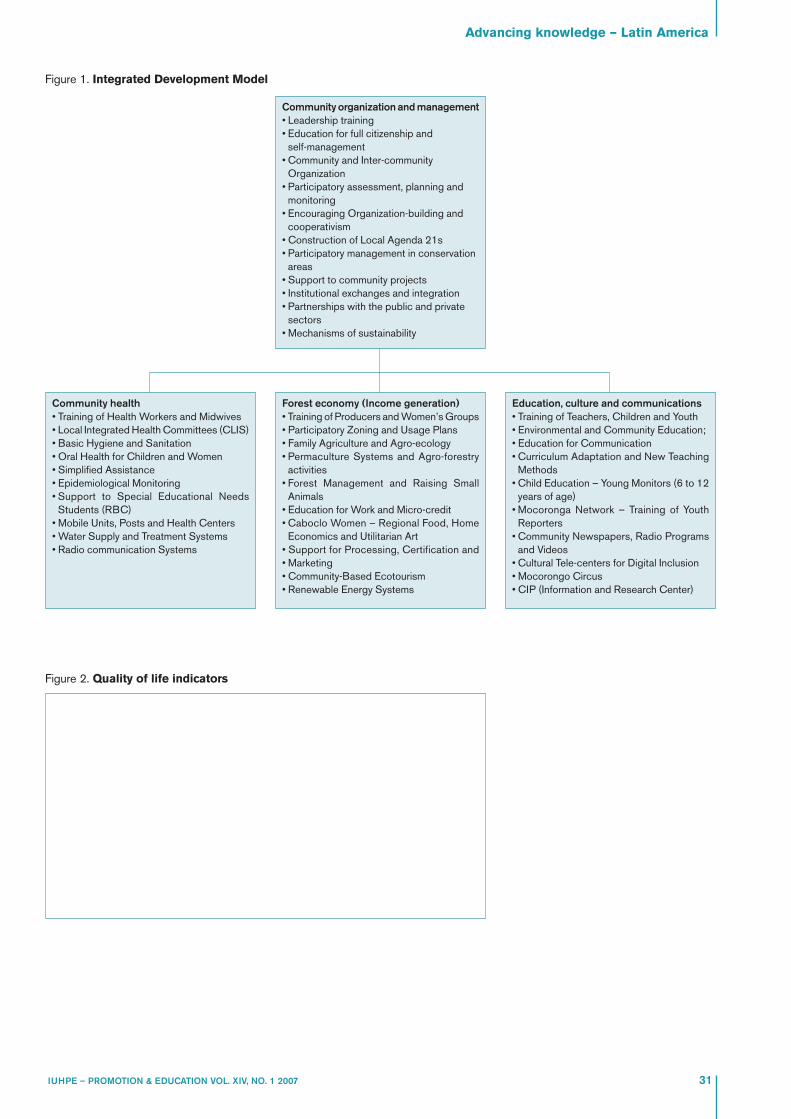
Figure 1. Integrated Development Model
Advancing knowledge – Latin America
31IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
Community health• Training of Health Workers and Midwives• Local Integrated Health Committees (CLIS)• Basic Hygiene and Sanitation• Oral Health for Children and Women• Simplified Assistance• Epidemiological Monitoring• Support to Special Educational Needs
Students (RBC)• Mobile Units, Posts and Health Centers• Water Supply and Treatment Systems• Radio communication Systems
Forest economy (Income generation)• Training of Producers and Women’s Groups• Participatory Zoning and Usage Plans• Family Agriculture and Agro-ecology• Permaculture Systems and Agro-forestry
activities• Forest Management and Raising Small
Animals• Education for Work and Micro-credit• Caboclo Women – Regional Food, Home
Economics and Utilitarian Art• Support for Processing, Certification and• Marketing• Community-Based Ecotourism• Renewable Energy Systems
Community organization and management• Leadership training• Education for full citizenship and
self-management• Community and Inter-community
Organization• Participatory assessment, planning and
monitoring• Encouraging Organization-building and
cooperativism• Construction of Local Agenda 21s• Participatory management in conservation
areas• Support to community projects• Institutional exchanges and integration• Partnerships with the public and private
sectors• Mechanisms of sustainability
Education, culture and communications• Training of Teachers, Children and Youth• Environmental and Community Education;• Education for Communication• Curriculum Adaptation and New Teaching
Methods• Child Education – Young Monitors (6 to 12
years of age)• Mocoronga Network – Training of Youth
Reporters• Community Newspapers, Radio Programs
and Videos• Cultural Tele-centers for Digital Inclusion• Mocorongo Circus• CIP (Information and Research Center)
Figure 2. Quality of life indicators

Advocacy
Over decades, the State has played a sig-nificant role in health sector. With the grow-ing process of Globalization and the influ-ence of New Economic Policy, there istremendous pressure to replace thisarrangement and put the social sector inmarket place. There can be little doubt thatthe greatest economic force now sweepingthrough the health care system worldwideis that of the market. Health is a vital humangood and Medicare plays a key role in pro-moting it. Totally commercializing it evenfor the sake of choice and efficiency runsa potent risk of submitting it to the market-forces. The integrity of medicine itself is atstake. Thankfully for the poor in most devel-oping countries the State still remains prin-cipal provider in Health Sector. We need toappreciate the importance of advocacy forpeoplecentered health from this backdrop.
Health policies need to grow, developand be continually creative to meet thechanging needs of the situation. This under-lines the importance of sustained advocacyon health policy, to ensure that it is peo-pleoriented and relevant. Viable options forhealth system must be technically feasible,consistent with public sector capacity, andcapable of commanding sufficient socialand political support to be sustainable. Thisis particularly true for the developingworld, where a large section of the popula-tion does not have well-defined and strongenough platform to air their frustrationagainst inadequate social policies.
VHAI, the largest network of voluntaryagencies in health sector in a massive, com-plex and heterogeneous country like India,
plays significant role in this area. A largesection of the population of India is totallydependant on the Government health sec-tor since they do not have the financialmeans to buy services from the market.Several studies conducted by us show thatwhen the public health infrastructures donot work, the health expenditure becomesone of the major contributors for indebt-edness of the poor.
In India, the state health policy is out-dated. The critical services and facilities aregetting frayed due to growing population,non-optimal use of existing facilities andincreasing pressure of global financial insti-tutions for dilution of the role of Public Careand to abandon holistic, people-centeredcommunity health care and to replace itwith a selective «magic bullet» orientedhealth care. The situation is further com-plicated by the fact that the large privatesector usually does not provide qualityservices at a reasonable cost. Outreach ofthe voluntary sector is limited due toabsence of more enabling atmosphere. We,therefore, felt that it is important to worktowards a new Health Policy to respond tothe current situation adequately.
Plans and policy options should beguided by an ambitious vision of whatshould be accomplished, but they mustalso be informed by the realities of the pres-ent. Despite the rhetorical vision of a healthsystem with a universal, vertically inte-grated, publicly provided system, India hasnot provided funds to make that vision areality. Raising additional governmentfinance has its own complexities. Any pol-
icy that proposes a significant expansion inthe low level of publicly mobilizedresources devoted to health needs to pro-vide an explicit proposal for how the addi-tional costs will be financed.
These realties are not immutable. Theycan be changed through institutionalreforms and strong political commitment,but one cannot simply assume that they willdisappear. Ultimately changing the shape ofthe health system depends on politicaldecisions made at national, state and locallevels. An explicit approach to policy for-mulation and implementation must ensurethat the health system is improving thehealth of all in an equitable, accountableand affordable manner. For developing anappropriate and sustainable health caresystem, the health policy must promoteGovernment, Public and Private Partner-ships; an inter-sectoral coordination alongwith the Decentralisation of the health sys-tem, tempered with effective supervision.
Our advocacy effort begins at the grass-roots by not only trying to understand peo-ple’s health & development problems, butto work with them to learn how to developthe alternative approach. This experience-based learning gives us very essential cred-ibility to talk about important health issueswith conviction. The knowledge aboutexciting innovations to address criticalissues of health care being taken up in largemetropolitan towns or institutions of devel-oped countries reach all corners of theworld within days, but similar effort at theremote rural areas of the developing coun-tries hardly attracts anybody’s attention.
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 2 200732
Advocacy for appropriate health policy and effectivegovernance of health systemAlok Mukhopadhyay1
Abstract: Health policies supported by sustained advocacy efforts need to continually grow and develop to respond to theincreasing pressures of macro-economic policies of globalization, liberalization and privatization. VHAI, the largest network ofvoluntary agencies in health sector is playing a critical role at both macro and micro levels. Its health advocacy efforts emergefrom the grassroots with an understanding of their health and development problems as well as the strategies adopted to addressthem. The process, of strengthening an upward mobilization of information, towards formulation of an effective health policy, isbacked by serious macro research on various policy dimensions of health, done by the Independent Commission on Healthand Development in India (ICDHI), set up in 1995 by VHAI. These key policy documents, prepared are both reflective and pre-scriptive and are presented to the highest state authorities along with a discussion at various levels with varies groups. One ofthe recent successes was at getting the giant tobacco companies withdrew from Cricket sponsorship with an association inthe formulation of comprehensive Bill by the Union Government to prevent this in future. Various well-researched policy docu-ments have been put together by the organisation based on its micro and macro level work and persistent advocacy. Appro-priate public health and development policies with their effective implementation are the cornerstones to realize the fundamentalvalues of Ala Ata. The health care system needs to be removed from the current bio-medical model and closer to a socio-polit-ical and spiritual model where health care again becomes an organic part of community care as it once was in the traditionalsociety. (Promotion & Education, 2007, (2): pp)
Key words: Global health advocacy; State health policies; Grassroots.
1. Chief Executive Officer, Voluntary Health Association of India. Correspondence to: [email protected]

We feel that the process of strengtheningupward mobilization of information is animportant factor towards appropriate direc-tion of an effective health policy. Experi-ence of our grassroots effort is backed byserious macro research on various policydimensions of health, involving respectedprofessionals, academics, policy makersand activists. While preparing documentsto influence the health policy, we not onlyrely on primary and secondary data, butthey are usually backedup by focusedgroup discussions with stakeholders andpublic hearings of beneficiaries and round-table with concerned professional groups.
We keep the major political parties, keyofficials and the media fully informed aboutthe endeavour and often they are invited toparticipate in some of these events. Thedocuments finalized through this partici-patory process are not just critique ofhealth policies, but are prescriptive. Weclearly outline viable solutions to the majorpublic health problems and documentexamples of successful micro experiences.This elaborate and rigorous process pro-vides the alternative policy documentslegitimacy and the desired credibility.Preparation of key policy document is cor-nerstone of a successful advocacy effort.We ensure that the policy document is for-mally presented to the highest possibleauthority of the land. Our policy documentfor an alternative health policy was pre-sented to the Prime Minister and the Pres-ident in an elaborate function widely cov-ered by the media. This was followed bydiscussion with elected representatives ofvarious political parties and ParliamentaryStanding Committee on Health. These highprofile events create an overall empatheticatmosphere for policy change.
Often the groups working on policy mat-ters loose their steam by sheer demand ofpreparing the policy document. It is impor-tant to ensure that sufficient finance andhuman resources are available for advo-cacy related work. Persistent and doggedfollow-up is key «mantra» in advocacy.
During our recent successful work for acomprehensive bill to debar tobacco com-panies from sponsoring sports, we receivedtremendous support from Cricketers andCricket Control Boards of other countriesand sporting public. This was backed byour Public Interest Litigation against theIndian Cricket Control Board in the HighCourt. Eventually the giant tobacco com-pany withdrew from the sports sponsor-ship due to our dogged advocacy and thesuccessful Public Interest Litigation. TheGovernment is now drafting a comprehen-sive Bill to prevent this in the future. We areplaying an active role in the finalization ofthe content of this Bill. Similarly, the revised
Advocacy
33IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
Health Policy is in the final stage of redraft-ing with substantial input from the reportproduced by us. We are also Members ofthe Steering Committee for drafting the NewHealth Policy.
We should remember that adoption ofan appropriate public policy by the Gov-ernment is not an end by itself because themajor task of effective implementation ofthe policy is an equally important issue.Advocacy groups have to play dynamic roleof monitoring the implementation of thepublic policy closely, particularly in the ini-tial years. Our grassroots level projects playa very important role of providing us feed-back on the effectiveness of the implemen-tation process at the grassroots. The feed-back is regularly conveyed to theauthorities to enable them to fine-tune themechanism of implementation.
The importance of urgent and sustainedglobal advocacy for restoration of funda-mental values of Alma Ata – people-cen-tered, holistic and sustainable health carecannot be overstressed. The challenge tohealth in the new millennium will be to rec-ognize that in no country in the world theprivate sector has been the answer to healthproblem of the population. Even in theUnited States, forty seven percent of thepopulation is without health insurance cov-erage. Secondly, there is an imperative needto acknowledge that health improvement isless an outcome of medical technology thanof living standards. Health improvementsbased on narrow technical interventions arebound to be chimerical. Thirdly, the macro-economic policies of globalization, liberal-ization and privatization, which are increas-ing the exploitation of low-income countriesand communities around the globe, havehad profoundly deleterious effects. Finally,it is simply not true that we do not haveresources to pay for health for all. It is esti-mated that the cost of providing basic healthcare to be world’s population will amount to25 billion dollars. This is about what West-ern Europe spends on cosmetics, and a frac-tion of the 400 billion dollars that the worldspends on armaments annually.
We obviously need a new paradigm ofhealth care far removed from the currentbio-medical model and closer to a socio-political and spiritual model. Currently,health care has become a commodity thatcan be bought and sold in the market; it isno longer an organic part of communitycare as it once was in traditional society.The ‘germ theory’needs to be replaced bya model where the human being isregarded as central and helped to regener-ate a sense of well-being and fitness in hisor her life situation. Interestingly, most ofthe traditional systems approach healthfrom this holistic perspective.
ReferencesBanerjee, D. (1983). ‘National Health Policy and its
Implications’. Economic and Political Weekly. 22January, Pp. 105-108.
DAC Guidelines and Reference Series (2003): Poverty and Health, OECD & WHO
Dugal, Ravi and Sucheta, Amin. (1987) ‘Cost of Health Care’. Mumbai: Foundation for Research inCommunity Health
Gwatkin R. Davidson (2001) ‘The need for equity oriented Health Sector Reforms’, InternationalJournal of Epidemiology. pp-720-723
Gopalan, C. (1995) ‘Towards India’s Food and Nutrition Security’. Keynote address at theNational Symposium on Food Security for thePoor, organized by the FAO and the IndianAssociation for the Advancement of Science, 4October.
Jain, L.C. (1993) Panchayats – Window to a Million Possibilities. New Delhi: People’s Action, Vol. 8,No. 2.
Jeffery, Roger. 1988. The Politics of Health in India. Berkeley: University of California Press.
Report of the Independent Commission on Health in India. (1998). VHAI, New Delhi.
Sachs D., Jefferey (2005) ‘The end of poverty; how we can make it happen in our lifetimes’.
State of India’s Health, (1992) Voluntary Health Association of India, New Delhi.
The Silver Lining – A Document on People CenteredHealth Initiatives in South East Asia. (1997).VHAI, New Delhi.
Wagstaff, Adam. (2002) ‘Poverty and Health sector inequalities’, Bulletin of the World HealthOrganization. pp-97-105.

When the late Dr. Lee, Director Generalof the World Health Organisation,announced the formation of the Commis-sion on the Social Determinants of Healthat the World Health Assembly in May 2004he commented:
“The goal is not an academic exercise,but to marshal scientific evidence as alever for policy change — aiming towardpractical uptake among policymakersand stakeholders in countries”
This paper focuses on factors that arelikely to encourage and initiate practicalaction on the social determinants of healthinequities. It will include discussion of theneed for both evidence and knowledgetogether with understanding and a com-mitment to equity. Consideration will begiven to the importance of the «nutcracker»effect which describes the power of thecombination of top down and bottom upaction on health equity. The argumentsarticulated herein demonstrate that soci-eties, which focus on linking social capital(as defined by Szreter & Woolcock(2004)and discussed in detail below) are morelikely to be committed to and effective intaking action on the social determinants ofhealth than those with low levels of linkingsocial capital.
Powerful combination ofevidence, knowledge,understanding and values
Knowledge and evidence are clearlyimportant to achieving action on healthequity. The CSDH has established a knowl-edge network on Evidence and Measure-ment. The first paper from this network(Kelly et al, 2006) argues strongly in favourof methodological pluralism and epistemo-logical variability in approaches to studyingthe social determinants of health and health
inequity. They note «Humans use differentforms of knowing and different forms ofknowledge for different purposes. There isno necessary hierarchy of knowledgeinvolved until we need to discriminate onthe basis of fitness to purpose» (Kelly et al,2006 p. 8). An understanding of the com-plexity of factors that contribute to the socialdeterminants requires an insight into manydifferent disciplines and the use of a rangeof methods. However, the most useful qual-itative research methodology involves inter-views of key informants to ascertain ways inwhich social, economic and political struc-tures shape individual experiences. Forexample longitudinal epidemiological stud-ies that enable the determination of causallinks between exposure to certain socialand economic conditions and diseases orpolicy studies of the outcome of differentsystems of social welfare. Such knowledgeis often context specific and contingent onpolitical and economic circumstances. Thecomplexities of this process and the broadrange of knowledge on social determinantsis often envisaged to be an impediment tothe uptake of the knowledge in this area.Commenting on the challenging of gettingknowledge to inform policy and practice,Speller (2001) used Stacey’s (1996) Agree-ment & Certainty Matrix to demonstrate thathealth promotion and public health initia-tives often fall into a zone of complexity thatleads to uncertainty about what works andso consequently to a lack of agreementamong policy makers and practitioners.Stacey stresses the need for non-linear andcreative thinking when organisations areworking at the edges of chaos and dealingwith complex information to obviate issuesemerging from lack of consensus. It is envis-aged that such situations often arise whenorganizations attempt to address the socialdeterminants of health. Thus it will take a
particular combination of commitment tojustice, understanding of complexity andthe ability to lead organisations through thechange necessary to cope effectively withcomplexity in order to lead to the actions,which the Commission envisages lendingimpetus to.
Evidence on health inequities has beenavailable in many developed countries forsometime; however this has not ensuredthe institutionalization of remedial action.Most notably, the «Black Report» in theUnited Kingdom (Townsend and Davidson,1992) was rejected by the incomingThatcher Government despite the com-pelling information it presented on the exis-tence of inequities and the possible reasonsfor their existence. This and many otherexamples show that while evidence oninequities is necessary it is certainly not suf-ficient to ensure action. Policy makers alsoneed to know what can be done to reduceinequities and need to work from a valuesbase that emphasises the pursuit of socialjustice as crucial to society. Knowing whatis to be done requires coming to grips withthe range of choices that lie inside and out-side the health sector.
The international health promotionmovement has come a long way in the pasttwenty years. In the 1970s and 1980s, behav-iour change using pamphlets and marketingcampaigns was the overriding tool of healthpromotion. Subsequently, the concept ofhealth promotion was revolutionarized bythe Ottawa Charter for Health Promotion(WHO, 1986), which established that whilechanging behaviours was indeed a crucialaim of health promotion, bringing change atthat level involved a complex interplay ofpolicy and strategy, creating supportiveenvironments, encouraging communityaction and reorienting health services. TheOttawa Charter was instrumental in galva-
IUHPE – PROMOTION & EDUCATION SUPPLEMENT 2 200734
Cracking the nut of health equity: top down and bottom uppressure for action on the social determinants of health.Fran Baum1
Abstract: The Commission on the Social Determinants of Health was established to advise on ways in which understandingof the social determinants of health can affect practical action to improve population health equitably. This paper considers thefactors that are necessary to encourage governments to adopt policies that aim at doing this. It argues that knowledge, whileessential, is insufficient. Governments need a commitment to the values of fairness and justice and an ability to cope with thecomplexity of responding to social determinants beyond exhorting individuals to change their behaviour. The role of civil soci-ety is crucial in advocating for governments to do this. The presence of linking social capital is also crucial to creating a socialand political environment in which fairness is promoted. A case study of the poor health status of the Aboriginal peoples inAustralia is used to illustrate the importance of social capital. (Promotion & Education, 2007, (2): pp)
Key words: Social determinants of health, linking social capital, Aboriginal health.
1. Department of Public Health, Flinders University. Correspondence to: GPO Box 2100, Adelaide 5001 ([email protected])
Résumé en français à la page #. Resumen en español en la página #.
Advocacy

nizing action in many countries. In Aus-tralia, for example impact at the populationlevel was clearly evident and manifesteditself as reduction in prevalence of smokingand smoking related morbidity, decrease inroad accident-related fatalities, reduction insuicide rate and decline in the rate of skincancer (Baum, 2002). Each of these hasbeen achieved not through single measuresbut through a battery of self reinforcingmeasure. While these are significant publichealth gains, they have done little toaddress inequities and reduce the existinggradients. Here it is important to recognizethat unless designed with a very strongequity lens, health promotion can act toincrease the difference between groupsrather than reduce them even if theyimprove population health as a whole. Forexample, there is evidence that people inhigher socio-economic groups are morelikely to be successful in quitting smoking(Osler and Prescott, 1998; Barbeau, Krieger,Soobader, 2004). In Australia over theperiod 1998-2004 while there has been a 9%decline in smoking among the lowest quin-tile the rate of change for the highest socio-economic quintile is 35% (see Table 1). Areasonable conclusion is that anti-smokingmessages have been more successful withbetter off people and, at least temporarily,have increased inequality.
Further complicating our message is thefact that health inequities do not reflect adichotomy between a disadvantaged groupat the bottom of the social advantage pileand the rest sharing equal health status. Thework of Sir Michael Marmot (Chair of theCommission on the Social Determinants ofHealth) and colleagues (see summary inMarmot, 2004) has shown that the distribu-tion of health in communities is in the formof a gradient. This gradient is also illustratedin Table 1 where the percentage decline insmoking across socio-economic quintiles isin the form of a gradient from high to low.This has great significance for the strategieswe adopt to bring about equity. The gradientin health suggests that we need populationwide universalist strategies as well as thosetargeted at the most disadvantaged. Againthis is a more complex argument to advo-cate to policy makers than the one which
Advocacy
35IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
focuses on the need to target those at thebottom of the pile.
Taking action on the social determinantsof health to reduce health inequity will alsorequire politicians and policy makers toresist what Kickbusch (2006) has called «thedoability of medicine». Modern medicineoffers individuals considerable possibilities.But many of its interventions will not havea discernable impact on population health(as opposed to the health of a few individ-uals, usually towards the end of their life).Perhaps this is the hardest lesson for pol-icy makers and politicians to grasp. Yet it isalso the most important lesson to grasp if weare to have the understanding necessary tobring about a real determination to improvehealth across populations. Rose (1985) hasset this lesson out most clearly. He pointsout that treating high risk or diseased indi-viduals does not have much impact on pop-ulation health levels overall, but changinga risk factor across a whole population byjust a small (and often clinically insignifi-cant) amount can have a great impact on theincidence of a disease or problem in thecommunity. For example reducing saltintake in manufactured food by a small pro-portion across a population (at a level indi-viduals would not notice) would reduceblood pressure levels and in time reducedeath rates from cardio-vascular disease.Add to this the need to implement popula-tion-wide strategies in a way that is equitableand the extent of complexity of knowledgeand concepts is considerable. Rose’s mes-sage about population health is counterintuitive and the difficulties of grasping iteffectively is, in all likelihood, the reasonwhy we face challenges in shifting ourhealth care system to a focus on prevention,health promotion and social determinantsof health, despite so many WHO and Gov-ernment sponsored reports that have calledfor this reorientation (Benezeval, 2003; Inde-pendent Inquiry into Inequalities in Health,1998; Stahl et al, 2006; Stegeman and Cos-tongs, 2003; WHO, 1978; WHO, 1986; Wilkin-son and Marmot, 2003).
Understanding of Rose’s dictums on pre-ventive medicine are likely to be heededmore easily in those who have a more col-lective mind set rather than those more
committed to a strong individualism. Thisfact was point out by Tesh (1988) when shepointed to the strong individualism thatunderpins public health policy in theUnited States. A strong ethos of individual-ism is likely to lead to victim blamingassumptions (Crawford, 1977). Such an atti-tude is obvious in the following commentby an Australian federal health minister,Tony Abbott (2005) on a television programon childhood obesity:
“No-one is in charge of what goes intomy mouth except me. No one is incharge of what goes into kid’s mouthsexcept their parents. It is up to parentsmore than anyone else to take this mat-ter in hand……..if their parents are fool-ish enough to feed their kids on a dietof Coca Cola and lollies well they shouldlift their game and lift it urgently”.Tesh (1988) points out that the very
research questions we ask are shaped bycore values. Thus a focus on individualismwould lead to questions about why indi-viduals are over weight and explore theirmotivations while a more collective ideol-ogy would explore questions about why itis that obesity levels in all high incomecountries have increased in the pastdecade and consider what features of thesociety have encouraged this. The assump-tion that changing behaviour is about per-sonal motivation is very common despitethe evidence that people need supportiveenvironments in which to make healthychoices and that pressures from socialmores, advertising and constraints of healthfood availability are likely to have stronginfluences on the choices people are ableto make (Baum, 2002). There are many fac-tors that reinforce ideologies of individual-ism. These include the fact the ideology isless threatening to many vested interests,especially commercial interests, the phi-losophy of some political parties aregrounded in a strong belief in the individualrights even when these are at the expenseof the common good and the fact that pro-tecting the rights of individuals has oftenbeen a guard against the excesses of totali-tarian regimes. Consequently public healthis often viewed as being aligned with a‘nanny state’ that seeks extreme measuresthat restrict rights. This view has beenvoiced during campaigns to introducetobacco control, enforce seat belt legisla-tion, restrict the ownership of firearms,restrict the advertising of junk food andenforce sun protection in schools.
The fact that many of the determinantsof health of health lay outside the formalhealth sector also complicates the tasks ofimplementing action on the social determi-nants of health. In the past twenty years theimportance of cross sectoral action has
1998 2001 2004 % Change1st Lowest 30.0 25.8 27.3 -9%2nd 27.0 25.1 23.6 -13%3rd 28.4 23.7 21.7 -16%4th 25.8 23.6 18.2 -29%5th Highest 23.1 18.4 15.1 -35%
Table 1. Percentage Smoking and Percentage change by five socio-economicquintiles Australia, 1998-2004
Source: Data derived from Adhiknit and Summerhill, 2000; Australian Institute of Health and Welfare 2002 & 2005.

Advocacy
been repeatedly reinforced and put intopractice. Through the Healthy Cities proj-ects, the need to integrate government ini-tiatives in the intersectoral domains wasdemonstrated, particularly with referenceto road injuries, substance abuse, andpoverty (Ashton, 1992; Baum 2002; WHO,2007).. European Union’s current focus on‘Health in All Policies’is testimony to theacceptance of this message (Stahl et al,2006). The crucial task now remains toensure that this intersectoral action hap-pens effectively and as a matter of courseand is implemented with a strong focus onreducing equity.
The messages of modern health promo-tion then are complex. They involve under-standing the factors that impact on popu-lation and the existence of a healthgradient, the limitations of most medicaltherapy as a means to make significant
improvement to population health, andunderstanding that while behaviour changeis the aim of health promotion achievingthis effectively is not about simply tellingpeople to do so but in creating supportiveenvironments which will require actionfrom multiple agencies. The task of equityhealth promoters would be much easier ifthere were a simple message to pitch topoliticians and senior policy makers. Butthe reality of the situation makes equity ahard nut to crack. The following sectionconsiders the social and political environ-ments in which equity is more likely tomake it to the policy agenda.
The “Nutcracker” EffectThe “nutcracker” effect is illustrated in
Figure 1. It demonstrates the value of com-bining top down political commitment andpolicy action with bottom up action from
communities and civil society groups. Gov-ernment commitment to taking action onthe social determinants of health equity islikely to result from a belief in social justiceand an understanding of the complexitiesof health promotion as detailed in the pre-vious section. If a government reflects apolitical commitment to individualism andis wary of a overly interventionist ‘nannystate’then the pursuit of equity is unlikelyto be on it’s social policy agenda to anyextent. In this situation it will be hard to findmuch pressure exerted on the top of thelever. Such was clearly the case inThatcher’s Britain. Action on health equityonly resulted when Blair Labour Govern-ment was elected on a platform thatincluded a strong commitment to pursuingequity. By contrast a government driven bya belief in social justice is likely to imple-ment policies designed to reduceinequities; the Nordic welfare states haveprovided a strong example of such govern-ments. A powerful influence on govern-ment’s desire to be socially just is the pres-sure from the more socio-economicallybetter off in a society to do so. The existenceof this pressure has been described as link-ing social capital and is described in moredetail below. The other crucial part of thenutcrackers effect is the bottom up actionfrom civil society.
Civil society actionOne way in which governments can be
persuaded to take action is through bottomup pressure. This is a consequence of grow-ing iniquities as a result of which commu-nities prefer governments who state a com-mitment to reduce such inequities. Withinthis context, history provides numerousexamples of the role of civil society in bring-ing about change. Outstanding examplesare the suffragettes in ensuring votes forwomen; the civil rights movement in theUSA in stopping sanctioned segregation;and the anti-apartheid movement in bring-ing democracy to South Africa; and thegreen movement in putting environmentalissues on national and international agen-das and the land rights movement in Aus-tralia. (See Burgmann, 2003 for a discussionof these various social change mouve-ment). In each case years of grass rootsactions led to irresistible pressures forchange. In recognition of the important rolethat the civil society may play in arguing foraction on the social and economic deter-minants of health the Commission on theSocial Determinants of Health has estab-lished a stream of work on the role of civilsociety which has involved many civil soci-ety players. The report from the June 2006meeting of the Commission (Commissionon the Social Determinants of Health, 2006)
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 200736
Figure 1: The Nutcracker effect: top down and bottom up action for health equity

notes that the Commissioners recognisedthe distinctive contribution of civil societyin country level action on the social deter-minants of health including direct engage-ment with national governments andnational commissions on social determi-nants such as those in Kenya and Brazil.They also noted the importance of massmobilization such as the Indian People’sHealth Assembly and the crucial role oflabour organisations and trade unions(Commission on the Social Determinants ofHealth, 2006, p. 22). Civil society groupsmay also play a major role as advocates ofequity. Globally the People’s Health Move-ment (PHM) has played such a role since itsformation at the first People’s HealthAssembly. The movement has organizedtwo People’s Health Assemblies to date(intended as alternative World HealthAssemblies) from which two key docu-ments have emerged – the Peoples’HealthCharter written in 2000 and the Cuenca Dec-laration (2005) (see PHM, 2006 for copies)have made powerful statements about theneed to reduce global inequities. Manyhealth promotion and public health asso-ciations around the world make similarcalls. Locally community-based health pro-moters also play crucial advocacy roles forhealth equity. It can therefore be arguedthat collectively, civil society is a crucial tobring the bottom up political pressure tobear on politicians and policy makers sothat they are willing to take action on healthequity. Civil society can be oppositional togovernments and in extreme situations canbring about social and political change bycontributing pressure for a change of gov-ernment. In other situations progressivecivil society can work through advocacyand incremental change and will be oppor-tunistic about chances to influence policyagenda.
Linking Social CapitalSo far we have seen that bringing about
action on health equity will reflect a com-plex mix of sufficient evidence, good under-standing of what changes populationhealth, a political elite committed tochanges and active civil society pressurefor that change. But we are still left with thequestion of how is it that some societies aremore inclined towards taking action toreduce health inequities than others. Someclues can be found in the notion of linkingsocial capital. Szreter & Woolcock(2004,p.655) define linking social capital as«norms of respect and networks of trustingrelationships between people who areinteracting across explicit, formal or insti-tutionalised power or authority gradients insociety». What does this mean in practice?A society high in linking social capital is
Advocacy
37IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
likely to be characterised by the followingfeatures:• High trust in formal institutions• Fair and transparent public policy
processes• Commitment to redistribution by the bet-
ter off people in society• Commitment to activities of State (e.g. low
taxation evasion)• Opportunities for people from different
groups to interact in a respectful manner
There are indications that many of thesefactors are declining rather than increasing.Trust in institutions has declined signifi-cantly in the past two decades in most coun-tries where this is measured (Eckersley,2004). While transparency and fairness areupheld as hallmarks of democracy in prac-tice there have been significant challengesto this. The extent of commitment to redis-tribution varies around the world from theNordic countries where it is high to otherswhere taxation policy is moving away fromredistribution, Australia and the USincluded (Stretton, 2005). Many corpora-tions and very rich individuals seek toavoid tax and show little commitment to thecountry in which they operate, preferringto avoid tax whenever possible (Korten,2006). A society high in linking social capi-tal would have its richest corporate andindividual citizens committed to supportinga strong taxation base. This base wouldmake possible redistributive measures. Inthe Australian context Stretton (2005) haspointed out that under the conservativeMenzies government in the 1950s the topmargin tax rate was far higher than it is inAustralia today. Finally, what opportunitiesare there for people to interact respectivelyacross class and ethnic difference? Thedegree to which this can happen variesfrom society to society but in societiesmarked by considerable inequity it hap-pens less. The consequence is that thereare less common bonds and less under-standing. Linking social capital implies thatthere is a sense of obligation from power-ful institutions in society towards the lesspowerful. Bourdieu’s (1986) conception ofsocial capital makes it clear that the net-works and reciprocities involved inexchanges most commonly work to thebenefit of the already well-off and morepowerful groups. They do this by givingpeople pathways by which they gain accessto educational, cultural and employmentopportunities. Policies aimed at reducinginequities should, as an aim, work towardsensuring that benefits that accrue to certainclasses in society are made available toother less powerful and privileged groupsas well, on the premise that a society thatsupports and encourages such policies is
likely to be characterised by high linkingsocial capital. The importance of this notionof linking social capital is best illustrated bya case example articulated herein, whichfocuses on a case study of the absence oflinking social capital between AustralianAboriginal and non-Aboriginal peoples.The case shows how the absence of link-ing social capital can have profound impacton health and illustrates how the presenceof strong linking social capital has thepotential to encourage government com-mitment to equity. .
Australian case study of the lackof linking social capital
The case of the relationship betweennon-Indigenous Australians and IndigenousAustralians illustrate the importance of theconcept of linking social capital to the like-lihood of effective intervention to reducehealth inequity. Indigenous people in Aus-tralia have been described as second classcitizens in Australia (Chesterman and Gilli-gan, 1997). In the early days of settlementthere is solid evidence (Hunter 1993;Reynolds 1998) that they were subjectedto considerable violence. In the twentiethcentury much Indigenous experience wasshaped by the welfare policies purported tobe in the best interests of Indigenous peo-ple. In fact, it controlled their lives to theextent that children were removed fromtheir families and the law dictated whoIndigenous people could and could notmarry. The experience of the «stolen gen-eration» has been well-documented in theBringing Them Back Home Report (HumanRights and Equal Opportunity Commission1997). It demonstrates the significant impactthat these experiences have had on thehealth and well-being of the Indigenouspeople caught up in this shameful period ofAustralian history. Clearly one of the seque-lae of these experiences is a legacy of deepmistrust that the Indigenous people havetowards mainstream institutions of the non-Indigenous society such as the police,health and welfare systems and schools.Clearly, very little linking social capital wasevident in this area.
Non-Indigenous Australians often proj-ect negative views of Indigenous Aus-tralians that reflect purely on their currentbehaviour and situation without taking intoaccount the impact of the historical expe-rience of Indigenous peoples. Indigenouspeople are far more excluded from thesocial and economic mainstream of Aus-tralian life than are other Australians (Trud-gen 2000). They are also subjected to sig-nificant racism (Hunter, 1993) and live in aworld which is dominated by invisible andlargely unacknowledged assumptions ofwhiteness (for further details of concept of

Advocacy
‘whiteness’see Riggs 2004; Fein et al. 1997).The history of Australia since the invasionby white people shows that a number of fac-tors have worked to determine the health ofthe indigenous people; these include: theway society has been organized, the degreeand nature of interaction between Indige-nous and other Australians, the levels oftrust between the two groups and the extentof care extended to Indigenous Australiansby the wider society. Limited attempts havebeen made to bridging the social capitalbetween Indigenous and non IndigenousAustralians and therefore the scope for link-ing social capital to development has sadlybeen lacking in Australian society. This hasled to the exclusion of the Australian Indige-nous people from mainstream economic,educational and social life in Australia.Some insights into the likely impact of socialexclusion on health can be gained from therecent literature debating the impact ofincome inequality across populations.Wilkinson (2005) has argued that a keydeterminant of population health outcomesis the extent to which societies distributedtheir income equally with more equal soci-eties achieving higher population healthoutcomes. He theorised that part of theexplanation for this pattern was that coun-tries with less equal distribution of incomealso had lower levels of social capital. Heargues that this link exists because unequalsocieties are characterized by individualswith increased anxiety and low social sup-port institutions and by higher levels of vio-lence and disrespect between citizens. Hiswork has been strongly criticized for underplaying the role of access to material factors(especially employment and housing) thatunderpin inequalities (see for example,Lynch et al 2000). However it gains supportfrom the work of Michael Marmot and col-leagues (Marmot et al. 1991; Brunner & Mar-mot 1999) who explain health status gradi-ents in populations through the stresspeople experience from not being at the topof hierarchies and the consequent absenceor loss of autonomy over one’s life, workingand neighbourhood environment. Appliedto the experiences in the Australian con-text, it is evident that racism and economicinequity have led to lack of control on partof the indigenous people, over their life interms of its direction, culture and traditionalways and the ownership of land. This hasled to extreme stress for Indigenous peo-ples; Marmot’s work indicates that it islikely to have a very significant impact onhealth. The situation principally resultsfrom the lack of supportive policies frommainstream Australia – the lack of linkingsocial capital. Szreter and Woolcock (2004)argue that consideration of the relationshipof the state in terms of the initiation and sus-
taining of networks, trust and social struc-tures is crucial. They show, with illustra-tions from a case study from nineteenthcentury England, that states (local and cen-tral) can create and encourage the condi-tions in which linking social capital canoperate. They can do this by ensuring thatresources flow from more powerful to lesspowerful groups. Szreter and Woolcock’s(2004) argument leads to the conclusionthat greater linking social capital in Aus-tralia can lead to increased empathy aboutthe dispossession suffered by Aboriginalpeople, and increase in the level of concernwith respect to improving the material con-ditions and facilities and services availableto Aboriginal people; this will contribute toadvancing the common commitment to agoal of a society of mutually respecting cit-izens. While there have always beenaccounts of some sympathy and empathyand desire to link with Indigenous peoplesfrom those more powerful, this has rarelybeen from other than a small minority(Reynolds, 1998).
Theories on linking social capital sug-gest that it is most evident at times whennetworks and trust develop betweengroups. Over the last fifty years, the Aus-tralian history does suggest that there hasbeen a growing movement in which Indige-nous peoples in Australia have been able toassert their rights more than in the past(Burgmann, 1993). Their endeavours havebeen supported by non-Indigenous peopleas was seen in the referendum on consti-tutional rights for Indigenous peoples andduring the reconciliation marches of 2000.The early 1990s held promise of being aperiod in which linking social capitalbetween Indigenous and non-IndigenousAustralians might take root, as evidencedby Prime Minister’s Paul Keating’s 1993 Red-fern speech:
And, as I say, the starting point might beto recognise that the problem starts withus non-Aboriginal Australians. It begins, Ithink, with the act of recognition. Recog-nition that it was we who did the dispos-sessing. We took the traditional lands andsmashed the traditional way of life. Webrought the disasters. The alcohol. Wecommitted the murders. We took the chil-dren from their mothers. We practiseddiscrimination and exclusion. It was ourignorance and our prejudice. And ourfailure to imagine these things being doneto us. With some noble exceptions, wefailed to make the most basic humanresponse and enter into their hearts andminds. We failed to ask - how would I feelif this were done to me?Paul Keating (then Prime Minister ofAustralia)– Redfern Speech December1992
This political will received strong sup-port from an active reconciliation move-ment that reached a height with a reconcil-iation walk involving 250,000 Australiansacross Sydney Harbour Bridge in May 2000.But recent events with the promotion ofmore punitive policies suggest any linkingsocial capital has been on the decline inrecent years. Recent policy directions suchas the imposition of «Shared ResponsibilityAgreements» which demand certain behav-iours from Indigenous people as a condi-tion for receiving social security benefitshave acted to reduce the autonomy ofIndigenous peoples and have been inter-preted as a return to more paternalistic pol-icy days (Collard et al 2005; Anderson,2006). Our knowledge of the importance ofcontrol to health status (Marmot, 2004) sug-gests that policies should aim to encourageself-determination supported by resourcesthat can make a difference. Linking socialcapital suggests a policy approach, whichis trustful of communities, encourages themto do the right thing for their children andprovides them with the infrastructure tocreate a health promoting environment.
ConclusionThis article has examined the factors that
are important for encouraging practicalaction on social and economic factors thataffect population health and healthinequities. It has argued that knowledge iscrucial but insufficient and that in order tocrack the nut of inequity, practical action isneeded both from governments as well asthe civil society. Civil society is constitutedby a rich array of groups, many of whomremain concerned about promoting justiceat a local level and lobby and advocate forequity-oriented policies. Their actions canboth encourage governments to take actionas well as can develop popular constituen-cies to support action initiated by the gov-ernment. Governments need to recognizethat taking effective action would be reflec-tive of their commitment to equity and jus-tice and will enable them to deal with thecomplexity of evidence and devising com-plex responses. These responses need to bebased on strategies that go beyond blamingindividuals to those that focus on creatinghealth and equity promoting environments.However, the exact process by which suchcommitment comes about differs from onecontext to another. Notwithstanding, it islikely to emanate from a society in whichgovernments and their agencies have boththe ability to deal with complex evidenceand devise solutions that deal with this com-plexity leveraging social capital. This formof social capital ensures that the better off ina society are prepared to support andencourage action to improve the health in
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 200738

a way that reduces inequity. Thus when theCommission on the Social Determinants ofHealth reports in May 2008 a crucial legacywill include improved knowledge on howaction on social and economic determi-nants can be used by governments toimprove population health equitably; exam-ples of governments who are successfullytaking such action; a strengthened civil soci-ety with a louder voice about the impor-tance of this action and improved under-standing of the processes (such as linkingsocial capital) by which societies adopt fair-ness and justice as the basis of their socialand health policies.
AcknowledgementsThe author is a member of the Commission onthe Social Determinants of Health. This paperdoes not, however, represent the views of theCommission and are those of the author.The nutcracker cartoon was drawn by SimonKneebone ([email protected])
ReferencesAbbott, T. ABC 4 Corners TV program on Childhood
Obesity Generation O transcript from DVD:Sydney ABC, 2005.
Adhikari P, & Summerill A (2000) 1998 National Drug Strategy Household Survey: Detailedfindings. AIHW cat. no. PHE 27. Canberra: AIHW (Drug Statistics Series No. 6) pp 11
Ashton, J., ed. (1992). Healthy Cities. Milton Keynes,Open University Press.
Australian Institute of Health and Welfare (2002) 2001 National Drug Strategy Household Survey:detailed findings.
Australian Institute of Health and Welfare AIHW cat. no. PHE 41. Canberra: AIHW (Drug StatisticsSeries No.11) pp 24
Australian Institute of Health and Welfare AIHW (2005) 2004 National Drug Strategy HouseholdSurvey: Detailed Findings. AIHW cat. no. PHE66. Canberra: AIHW (Drug Statistics SeriesNo.16) pp 23
Anderson, I. (2006) Mutual obligation, shared responsibility agreements and Indigenous healthstrategy, Australian and New Zealand HealthPolicy, 3:10http://www.anzhealthpolicy.com.contents/3/1/10accessed 18th October 2006
Benzeval M. (2003) The final report of the tackling inequalities in health module: the nationalevaluation of the health action zones. London:University of London, Queen Mary College,Department of Geography
Baum, F. (2002) The New Public Health. Chapter 24 Healthy Cities. Oxford University Press:Melbourne.
Bourdieu P.(1986) The forms of capital. In: Richardson JG, editor. The Handbook of Theoryand Research for the Sociology of Education.New York: Greenwood Press. p. 241-258.
Brunner, E. Marmot, M. (1999) Social organization, stress and health. Chapter 2 in Marmot, MWilkinson, R G (eds.) Social Determinants ofHealth, Oxford: Oxford University Press.
Burgmann V.(1993) Power and Protest. Movements for Change in Australian Society. Sydney: Allenand Unwin.
Chesterman, J. Galligan, B (1997) Citizens without Rights: Aborigines and Australian Citizenship,Melbourne: Cambridge University Press.
Commission on the Social Determinants of Health (2006) Summary of Proceeding: Fifth Meeting of
Advocacy
39IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
the Commission on the Social Determinants ofHealth. Nairobi Kenya 26-30th June. Geneva:WHO (available athttp://www.who.int/social_determinants/en/accessed 15th October, 2006)
Crawford R. (1977)’You are dangerous to your health’: the ideology and politics of victimblaming. International Journal of Health Services7, 4, 663-80.
Eckersey R. (2004) Well and Good. How We Feel and Why it Matters. Melbourne: Text Publishing.
Fine, M., Weir, L., Powell L.C. and Mun Wong, L. (eds.) (1997) Off White: Readings on Race,Power and Society. New York: Routledge.
Human Rights and Equal Opportunity Commission (1997) Bring Them Home: Findings of theNational Inquiry into the Separation of Aboriginaland Torres Strait Islander Children from TheirFamilies. Sydney: Human Rights and EqualOpportunities Commission.
Hunter, E. (1993) Aboriginal Health and History: Power and Prejudice in Remote Australia,Melbourne: Cambridge University Press
Independent Inquiry into Inequalities in Health (1998). Independent Inquiry into Inequalities inHealth Report (The Acheson Report). London:Stationery Office.
Kelly, MP, Bonnefoy J, Morgan A, Florenzano F. (2006) The Development of the Evidence Baseabout the Social Determinants of Health,Geneva: WHO. Available athttp://www.who.int/social_determinants/knowledge_networks/measurement/en/index.html Accessed19th October 2006.
Keating, P. (1992) Redfern Speech on the occasion of Australian Launch of the International Year forthe World’s Indigenous People. Available athttp://apology.west.net.au/redfern.html Accessed28th April, 2006.
Kickbusch I. Health and economic and social development. Paper presented at Health in AllPolicies High Level Expert Conference underFinland’s EU Presidency, Kuopio, Finland 21stSeptember 2006.
Korten D.(2006) The Great Turning. San Franciso: Berrett-Koehler Publishers Inc.
Marmot M. (2004) The Status Syndrome. How Social Standing Affects Our Health andLongevity. New York: Times Book. Henry Holt andCompany.
Lynch, J. Davey Smith, G. Kaplan, G. House, J S. (2000). Income Inequality and Mortality. BritishMedical Journal, vol. 320, pp. 1200-1204.
Marmot. M.G., Davey Smith, G. Stansfeld, S. A. et al (1991) Health inequalities among British CivilServants: the Whitehall 11 study. Lancet 337,1387-93.
Riggs, D (ed.) (2004) Why Whiteness Studies? Borderlands e-journal, 3, 2http://www.borderlandsejournal.adelaide.edu.au/issues/vol3no2.html Access 21st December 2005.
Reynolds, H. (1998) This Whispering in our Hearts. St. Leonards: Allen and Unwin
Speller, V. (2001) “The next challenge - getting evidence into practice” Promotion & EducationSupp. (1) pp: 20- 23.
Stacey RD. Complexity and Creativity in Organisations. San Francisco: Berrett Koehler,1996.
Stahl T, Wisma M, Ollia, E, Lahtinene E, Leppo K. (2006) Health in All Policies. Prospects andPotentials. Helsinki: Ministry of Social Affairs andHealth
Stegeman I, Costongs C. (2003) Health, Poverty and Social Inclusion in Europe: literature reviewon concepts, relations and solutions. Brussels:EuroHealthNet
Stretton H. (2005) Australia Fair. Sydney: University of New South Wales Press
Szreter, S. Woolcock, M. (2004) Health by Association? Social Capital, social theory, and thepolitical economy of public health. InternationalJournal of Epidemiology, 33, 650-667.
Tesh, S. (1988) Hidden Arguments: Political
Ideology and Disease Prevention Policy. NewBrunswick, NJ: Rutgers University Press.
Townsend P, Davidson N. (1992) Inequalities in Health. The Black Report, 2nd Édition, London:Penguin.
Trudgen, R. (2000) Why warriors lie down and die: towards an understanding of why the Aboriginalpeople of Arnhem Land face the greatest crisis inhealth and education since European contact,Djambatj Mala, Aboriginal Resource andDevelopment Services Inc., Darwin
Wilkinson R. (2005). The Impact of Inequality. New York: The New Press.
Wilkinson R, Marmot M. (eds.)(2003) The Solid Facts. 2nd Édition. Copenhagen: Regional Officefor Europe of the World Health Organization.
World Health Organization (1978) Primary Health Care. Report of the International Conference onPrimary Health Care, Alma –Ata, USSR, 6-12September. Geneva: WHO.
World Health Organization. (1986) The Ottawa Charter for Health Promotion, Health Promotion. 1(4); i-v.
World Health Organization. European Healthy Cities Web site http://www.euro.who.int/healthy-cities/introducing/20050202_4 accessed 9thApril 2007.

Members of the CDC and IUHPE GlobalConsortium on Community Health Promo-tion have been wrestling with two questionsin their work together over the term of thisConsortium. These questions are: ‘Howbest can community health promotionpractitioners check out whether their gen-eral activities and specific projects meetcurrent standards of good communityhealth promotion practice? And, where dopractitioners start, whether working aloneor in a team, in order to make certain theyare working most effectively?’
To address these questions, the Con-sortium members decided to compile a sim-ple list of criteria and checkpoints to assistpractitioners in appraising their projectactivities step by step. Although this is def-initely an early work-in-progress, we havedecided to place the initial draft in the pub-lic domain so as to encourage practition-ers to provide us with feedback since thelist will only able to be verified after field-based testing of these suggested steps.
The values outlined in the Statement ofthe Global Consortium published in theprevious edition of this journal (Nishtar etal, 2006), need to be read in conjunctionwith these criteria and checkpoints as thesevalues form the foundation on which thislist has been compiled. The most pertinentof these values and principles in relationto this checklist is the recognition that«community participation … must driveevery stage of health promoting actions»(Nishtar et al, 2006, p 7). The term ‘com-munity health promotion’refers here tohealth promotion action initiated with com-munity members, by community membersand for community members. Working inpartnership with communities throughoutall activities is the essence of good com-munity health promotion.
Two existing works-in-progress haveserved to lay the foundations for this check-list and the Consortium gratefully acknowl-edges these contributions. The Centre forCommunity Health Promotion Research,University of Victoria, Canada has donesome far-reaching work in developing aframework to assess the effectiveness ofcommunity health promotion interventions,and this Centre has been very generous insharing their developing material with us.
The Western Pacific Region of the WorldHealth Organization has in recent yearsdeveloped regional guidelines for imple-menting a Healthy Islands approach to pro-moting health (WHO WPRO, 2001), with aspecial focus on checking out progress ininitiating and implementing communityhealth promotion action. This developmentin particular has occurred through exten-sive consultation with communities acrossthe Pacific island countries.
The criteria and checkpoints for com-munity health promotion practice are hereset out in two stages: Stage I: ‘Getting Start-
ed’and Stage II: ‘On the Go’. We hope thatdespite not yet being tested in the field, theycan be refined with your feedback, andeventually offer real value to practitioners.
ReferencesNishtar, S., Akerman, M., Amuyunzu-Nyamongo, M.,
Becker, D., Carroll, S., Goepel, E., Hills, M.,Lamarre, M-C., Mukhopadhyay, A., Perry, M.,Ritchie, J. (2006) «The statement of the GlobalConsortium on Community Health Promotion.»Promotion & Education, XIII (1).
WHO WPRO (2001) The Vision of Healthy Islands for the 21st Century: Regional ImplementationGuidelines. Manila: WHO Western PacificRegional Office.
IUHPE – PROMOTION & EDUCATION SUPPLEMENT 2 200740
Criteria and checkpoints for better community health promotionJan E. Ritchie1
1. Conjoint Associate Professor, School of Public Health and Community Medicine, University of New South Wales, Australian. Regional Director, IUHPE South WestPacific Region. Correspondence to: [email protected]
Résumé en français à la page #. Resumen en español en la página #.
Advocacy
Stage I: Getting StartedCriteria for initiating community health promotion action
As you beginInvite the community to identify and prioritise the issues they want addressed by health pro-moting action.• Outline the issue to be addressed• State the population concerned• Describe how the community context – physical environment, and/or social, cultural, political,
economic or gender aspects – has influenced the issue in the first place• Indicate source and amount of specific funding, if available.
‘Starting’: Collaborative Planning and OrganisationHow does the community want to take this action forward?Which other key persons have an interest or stake in addressing the nominated issue? Howcan they come to agree on appropriate action?What is the goal of community health promotion action in this instance?What strategies can be harnessed to meet this goal?In partnership with the community, consider: What steps need to be taken to implement thisaction?• Identify the issues important to the community in starting this action• Identify key stakeholders, reflecting the full diversity of views and recognising the power differ-
ent ones hold• Provide opportunities for different views to be aired and discussed• Plan discussions to work towards developing a common vision• Document the shared vision• With community, determine leader responsibilities• Identify community leader• With community, implement structures for relevant data collection and management• With community, implement structures for regular forums for reflection on progress• With community, determine health promotion goal to address this issue• With community, determine health promotion strategies to meet this goal
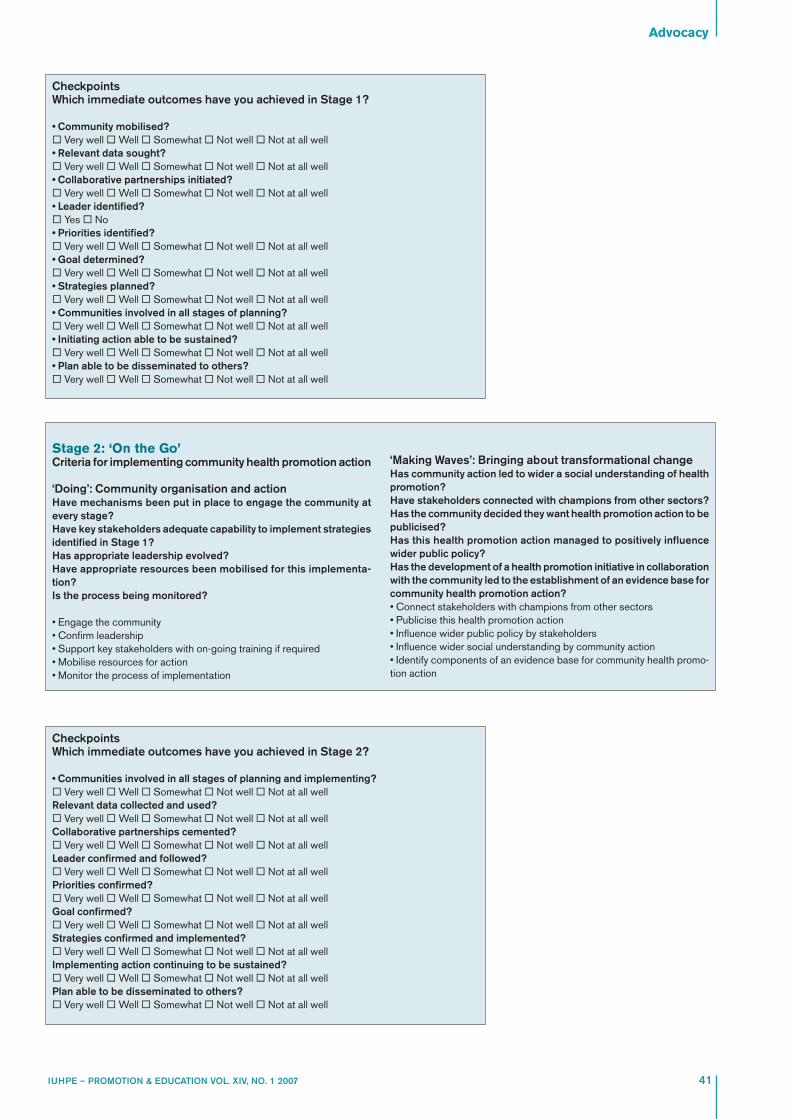
Advocacy
41IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
CheckpointsWhich immediate outcomes have you achieved in Stage 1?
• Community mobilised?� Very well �Well � Somewhat � Not well � Not at all well• Relevant data sought?� Very well �Well � Somewhat � Not well � Not at all well• Collaborative partnerships initiated?� Very well �Well � Somewhat � Not well � Not at all well• Leader identified?� Yes � No• Priorities identified?� Very well �Well � Somewhat � Not well � Not at all well• Goal determined?� Very well �Well � Somewhat � Not well � Not at all well• Strategies planned?� Very well �Well � Somewhat � Not well � Not at all well• Communities involved in all stages of planning?� Very well �Well � Somewhat � Not well � Not at all well• Initiating action able to be sustained?� Very well �Well � Somewhat � Not well � Not at all well• Plan able to be disseminated to others?� Very well �Well � Somewhat � Not well � Not at all well
CheckpointsWhich immediate outcomes have you achieved in Stage 2?
• Communities involved in all stages of planning and implementing?� Very well �Well � Somewhat � Not well � Not at all wellRelevant data collected and used?� Very well �Well � Somewhat � Not well � Not at all wellCollaborative partnerships cemented?� Very well �Well � Somewhat � Not well � Not at all wellLeader confirmed and followed?� Very well �Well � Somewhat � Not well � Not at all wellPriorities confirmed?� Very well �Well � Somewhat � Not well � Not at all wellGoal confirmed?� Very well �Well � Somewhat � Not well � Not at all wellStrategies confirmed and implemented?� Very well �Well � Somewhat � Not well � Not at all wellImplementing action continuing to be sustained?� Very well �Well � Somewhat � Not well � Not at all wellPlan able to be disseminated to others?� Very well �Well � Somewhat � Not well � Not at all well
Stage 2: ‘On the Go’Criteria for implementing community health promotion action
‘Doing’: Community organisation and actionHave mechanisms been put in place to engage the community atevery stage?Have key stakeholders adequate capability to implement strategiesidentified in Stage 1?Has appropriate leadership evolved?Have appropriate resources been mobilised for this implementa-tion?Is the process being monitored?
• Engage the community• Confirm leadership• Support key stakeholders with on-going training if required• Mobilise resources for action• Monitor the process of implementation
‘Making Waves’: Bringing about transformational changeHas community action led to wider a social understanding of healthpromotion?Have stakeholders connected with champions from other sectors?Has the community decided they want health promotion action to bepublicised?Has this health promotion action managed to positively influencewider public policy?Has the development of a health promotion initiative in collaborationwith the community led to the establishment of an evidence base forcommunity health promotion action?• Connect stakeholders with champions from other sectors• Publicise this health promotion action• Influence wider public policy by stakeholders• Influence wider social understanding by community action• Identify components of an evidence base for community health promo-tion action

Historical background to healthpromotion policies in Pakistan
In 1978, Pakistan became one of the ini-tial signatories to the World Health Organi-zation’s (WHO) Alma Ata Conferencewhich laid the foundation and target forHealth for All by the Year 2000 (WHO, 1978).One of the five principles to emerge fromAlma Ata focuses on disease prevention,health promotion, and curative and reha-bilitative services. Policies to address thisprinciple in Pakistan did not appear until1990 when the Pakistan Governmentlaunched its first National Health Policy(Ministry of Health, Government of Pak-istan, 1990). From a public health andhealth promotion perspective this policyfocused on school health services; familyplanning; nutrition programs; malaria con-trol programs; control of communicable dis-eases (e.g. tuberculosis and infective hep-atitis); sanitation and safe drinking water.
In 1997, the second National Health Pol-icy (Ministry of Health, Government of Pak-istan, 1997) was launched and health pro-motion and health education received aprominent place under priority health pro-grams and non-communicable diseasessuch as cardiovascular disease, cancer anddiabetes were highlighted for preventionand control measures. The focus for healthpromotion was «health education» and thefive principles of the Ottawa Charter forHealth Promotion (WHO, 1986) as a guidingframework per se were not alluded to.
The most recent National Health Policy(Ministry of Health, Government of Pak-
istan, 2001) was launched in 2001 and omitsthe prevention and control aspect of non-communicable diseases; it does not specif-ically refer to health promotion and in rela-tion to public health the main goal is …tocreate mass awareness in public healthmatters with a major focus on the use ofmulti-media to disseminate information.
In 2003, a Pakistani non-governmentorganization (NGO) by the name of Heart-file (http://heartfile.org) approached Pak-istan’s Ministry of Health and lobbied forthe development (implementation andevaluation) of a public health/ health pro-motion policy that specifically addressednon-communicable diseases from a pre-vention and wellbeing perspective. A tri-partite partnership was formed betweenthe Ministry of Health, the World HealthOrganization and Heartfile, a unique com-bination of public-private sectors workingtogether to support national health goals(Nishtar et al, 2005).
In 2004, the National Action Plan for Pre-vention and Control of Non-communicableDiseases and Health Promotion in Pakistan(NAP-NCD) (Ministry of Health, WHO andHeartfile, 2004) was launched and the firstplanning phase for implementation was ini-tiated. This public health/health promotionpolicy is both a policy and an implementa-tion document and is Pakistan’s firstnational policy devoted specifically to theprevention and control of non-communi-cable diseases and health promotion andtherefore is a milestone in public health/health promotion policy development.
What policy development cycledid the NAP – NCD follow?
In the absence of a Pakistani PolicyCycle reference, the Australian PolicyCycle (Bridgman and Davis, 2004) has beenutilized to analyze the development of theNAP – NCD policy as seen in figure 1.
Bridgman and Davis (2004) state thatmuch policy begins with iiddeennttiiffyyiinngg iissssuueessand during the initial planning phase of theNAP - NCD, there was the identification thatnon-communicable diseases such as car-diovascular disease, lung disease, diabetesand cancer contribute significantly to the ill-ness of the Pakistani population; secondlythese diseases are very costly in their treat-ment (incurred on the health system) andthirdly, if there are significant numbers ofpeople affected by morbidity then thisaffects the social and economic productiv-ity of a nation (Heartfile, 2003a).
In addition to the identification of theimpact that the afore mentioned diseaseshave on the Pakistani society they do notfeature prominently in Pakistan’s NationalHealth Policy and are not addressed in aprevention and control paradigm (Heart-file, 2003a). According to Bridgman andDavis (2004) sometimes an existing policyproves no longer effective and requires anoverhaul…. and with this new publichealth/health promotion policy, Heartfileidentified the fact that the current nationalhealth policy did not give due coverage ofthese non-communicable diseases andcommunity health promotion therefore anew strategic framework was needed.
IUHPE – PROMOTION & EDUCATION SUPPLEMENT 2 200742
Community health promotion in Pakistan: a policydevelopment perspectiveK. A. Ronis1 and S. Nishtar2
Abstract: Pakistan was one of the initial signatories to the Alma Ata Declaration in 1978, however, it was not until 2004 thatthe first policy dedicated solely to public health and health promotion was launched. The National Action Plan for Preventionand Control of Non-communicable Diseases and Health Promotion in Pakistan has gained a prominent place on the nation’shealth agenda competing for resources with traditional health policies that focus on treatment, cure and evolving technology.From a health promotion perspective the action plan was unique in that it focused on the community setting through two majorbehavioral communication change initiatives – one through the media and the other by integrating non-communicable diseaseprevention into the work plan of the Lady Health Workers.The development phase of this inaugural public health/health promotion policy follows closely the pathway of the AustralianPolicy Cycle and celebrates a comprehensive consultation process. Its strength comes from the tripartite partnership betweenthe Government, the World Health Organization and a Non-Government Organization, Heartfile who lent impetus to the creationof the initiative. This public-private partnership greatly facilitated the process of policy development and continues to supportresearch, implementation and evaluation.This paper endeavors to analyze the development of the National Action Plan with a focus on community health promotion.(Promotion & Education, 2007, (2): pp)
Key words: community health promotion, policy cycle, partnerships and non-government organizations
1. Senior Public Health Officer, Heartfile, Pakistan. Correspondence to: [email protected]. Founder and President, Heartfile, Pakistan.
Résumé en français à la page #. Resumen en español en la página #.
rubrique

Heartfile successfully identified theissues and put non-communicable dis-eases, prevention and community healthpromotion on the agenda for considerationby the Federal Government.
According to Bridgman and Davis(2004), ppoolliiccyy aannaallyyssiiss, is often - though notalways - the work of the public service,drawing on broader debates among spe-cialists in a policy field. In the developmentof the NAP - NCD, decision makers wereprovided with a situational analysis byHeartfile about the policy problem (i.e. non-communicable diseases and health pro-motion) so the decision makers could makean informed decision and provide infor-mation/data for debate. Heartfile provideda situational analysis due to their technicalexpertise in the area which examined pro-grams and policies within Pakistan toreview existing prevention and controlrelated efforts and to identify gaps relatedto policy, implementation and research.The action plan was led by Heartfile untilthe time of its development and launch.
Policy analysis leads to identification ofappropriate ppoolliiccyy iinnssttrruummeennttss (Bridgmanand Davis (2004) and with this publichealth/health promotion policy, the instru-ment selected was a national action planwith an Integrated Framework for Action.The dual approach provided a guide for thepolicy maker and bureaucrat and was sci-entifically written to appeal to the publichealth/health promotion community.
Bridgman & Davis (2004) state that…through ccoonnssuullttaattiioonn, policy proposals areimproved, ideas tested and, appropriate,support gathered. One of the majorstrengths in the development phase of theNAP - NCD is related to the wide consulta-tion which started with the tripartite col-laboration of the Ministry of Health, Gov-ernment of Pakistan; WHO and Heartfile.In addition to the three main partners, otherrelevant players or actors were consulted,for example: the scientific community; pub-lic health practitioners; related organiza-tions; other stakeholders, key leadershipand staff.
In an Australian policy cycle context, theccoo--oorrddiinnaattiioonn element of the cycle requiresdiscussions with treasury about availablefunding and to consider the relationbetween a new proposal (in this examplethe NAP - NCD) and overall governmentdirection (in this example Pakistan’sNational Health Policy). The developmentof the NAP – NCD was well situated withinthe overall direction of the government’shealth policy and availability of resourceswas discussed. Heartfile successfully lob-bied the Ministry of Health to allocate fund-ing to the action plan and transform it intoa program.
rubrique
43IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 2007
The ddeecciissiioonn pphhaassee in the policy cyclemeans consideration by cabinet or otherrecognized authority and in this case acommittee of the Ministry of Health and thePlanning Commission had the mandate totake such a decision. According to Bridg-man & Davis (2004)…iimmpplleemmeennttaattiioonn mustfollow, in which policy is given expressionthrough legislation or a program, in pursuitof the goals agreed by ministers. With theNAP - NCD an Integrated Framework forAction was included to prioritize and directthe implementation of the policy.
Under a formally approved PlanningCommission 1 (PC 1) (Ministry of Health,Planning Commission, 2003) allocationshave already been made to support twomajor community health promotion initia-tives namely the media focused behavioralchange communication strategy and a com-munication campaign at the grass rootslevel utilizing the Lady Health Workers ofthe National Program for Family Planningand Primary Health Care (2nd Goal) (Heart-file, Ministry of Health, WHO and 2004).
According to Bridgman and Davis (2004)…eevvaalluuaattiioonn is essential so government cangauge the effects of a policy and adjust orrethink policy design as appropriate. Simi-larly, partners that have supported a pol-icy development such as WHO and Heart-file also need to know the effectiveness ofthe policy and to assess the viability of con-tinuing as a partner both in terms of timecommitment and other resources (e.g.funding). In addition evaluation can help inredesigning or fine tuning communityhealth promotion programs in response toprocess, impact and outcome evaluationfindings.
In conclusion, the development of Pak-istan’s first National Action Plan for Pre-vention and Control of Non-communicableDiseases and Health Promotion adhered toa comprehensive and well planned policycycle; its implementation in the communitysetting aimed at promoting health and well-being has been initiated and ongoing mon-itoring reports indicate a supportive pub-lic – private partnership approach.
References:Bridgman, P. and Davis, G. (2004). The Australian
Policy Handbook. Allen and Unwin. Australia.Heartfile: http://heartfile.orgHeartfile. (2003 a) Planning Process: National
Action Plan for the prevention and control ofNon-Communicable Diseases in Pakistan. Asummary document.
Heartfile. (2003 b) Memorandum of Understanding: National Action Plan for Prevention, Control andHealth Promotion in Pakistan.http://heartfile.org/napmou.htm
Ministry of Health, Government of Pakistan (1990). National Health Policy. Government of Pakistan.
Ministry of Health, Government of Pakistan (1997). National Health Policy. Government of Pakistan.
Ministry of Health, Government of Pakistan (2001).National Health Policy. Government ofPakistan.
Ministry of Health, Government of Pakistan (2003) Planning Commission (Health) PC-1: NationalAction Plan for Prevention and Control of Non-Communicable Diseases and Health Promotionin Pakistan, F.NO.25-21/2003-Planning.Islamabad, Pakistan. Government of Pakistan.
Nishtar, S. (2004) National Action Plan for Non-Communicable Disease Prevention, Control andHealth Promotion in Pakistan. Ministry of Health,World Health Organisation and Heartfile;Islamabad, Paksitan.
Nishtar S, Bile, K.M., Ahmed, A., Faruqui, A.M.A., Mirza, Z., Shera, S., Ghaffar, A., Minhas. F.A.,Khan, A., Jaffery, N.A., Rajput, M., Aslam, M. andRahim, E. (2005) “Pakistan’s National Action Planon Chronic Diseases - Process, Rationale andInterventions.” Prev Chronic Dis. 2006 Jan; 3(1):A14. Epub 2005 Dec 15.
World Health Organization (1978). Declaration of Alma Ata. Geneva, WHO.
World Health Organization. (1986) Ottawa Charter for Health Promotion. Geneva, WHO.
Identify issues � policy analysis � policyinstruments� consultation� co-ordination� decision� mplementation� evaluation� identify issues etc.
Figure 1

Advocacy – Abstracts
From testimony to advocacy: a humanitarian NGO’s experienceJ. Ancien
Doctors of the World France (Médecins du Monde, MdM) is an international humanitarian aid NGO working to support access tohealth care to vulnerable populations of the world excluded from these services. MdM has fixed two strategies to «cure and give witness,»especially in light of the flagrant injustices lived by the populations they work with. Based on the need to improve the situation of thesepopulations, and using the Anglo-Saxon model, the association wanted to take their strategy one step further by progressively devel-oping advocacy actions in partnership with other organizations. This case study shows the different success obtained through advo-cacy actions in two campaigns: one against the World Bank’s promotion of health systems’privatization in 1993 and another one forthe increase in training of health care workers in the South in 2006.
A healthy park: the case of a prevention and community health promotion programme in amarginalised area in the Peruvian forest E. Peñaherrera Sánchez and W. Palomino
The healthy park initiative is an example of a prevention and health promotion programme in a community affected by high levels ofdrug use. It was developed through a strategic partnership with local actors (such as community leaders and youth groups), publicinstitutions (Health and Education Ministries and the local police) and private sector institutions (NGOs, local commerce). The com-munity involvement was essential throughout the project’’s entire process of design and implementation. Community members wereempowered through direct responsibility for carrying out the project and its follow-up, through advocacy initiatives and financial account-ing with the funding agency, the Belge Technical Cooperation group. The key programme outputs include the creation of a frameworkfor community coexistence and a community development plan, which allowed not only to plan and distribute responsibilities amongthe neighbours for the park’’s care and maintenance, but also to coordinate an increase in services and development opportunitieswith the local authorities.
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 2 200744

45IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 2 2007
Showcasing networks
BackgroundThe Network of Healthy Communities of
Rio de Janeiro is a social initiative for pro-moting health and equity, especiallythrough community development. Theapproach was inspired by the internationalHealthy Cities movement, which waslaunched in 2005 by 59 communities, withthe support of the Dreyfus Health Founda-tion, the Brazilian Ministry of Health, theRio de Janeiro Municipal Health Secre-tariat, the Pan-American Health Organiza-tion (PAHO), the Ford Foundation, severaluniversities and NGOs.
Poor communities (favelas) in Rio deJaneiro suffer from serious problems, suchas poor housing and environmental condi-tions, unemployment, lack of recreationand cultural life, and restricted access tobasic services such as health and educa-tion. In addition, they are severely affectedby violence from organized crime and thestate police.
Public policies directed towards low-income communities in Brazil are scarceand almost always implemented withouttaking local needs into account; therefore,they fail to harness the potential of local tal-ent. Residents have limited opportunities toparticipate and contribute to the develop-ment of these policies. As a result, the effec-tiveness, sustainability and ownership ofsocial interventions are reduced.
It is thus crucial to increase opportuni-ties for community participation in thedevelopment and implementation of socialsector community projects. Networking ofcommunity groups can increase their col-lective political strength and enable themto operate autonomously. Networking canalso enable the building of capacity in low-
income communities thus enabling them toparticipate in decision-making relevant toprograms that affect them.
Besides, poor communities have manyuntapped resources. These include: socialnetworks, solidarity, celebration and cul-ture, businesses, informal activities on edu-cation, recreation, religion, politics andmuch more. There are men and womenthat even in the midst of extreme poverty,violence and lack of services, break the iso-lation of their homes and become agentsof a social action that benefits their com-munities. Capacity building and networkingcan strenghten this potential.
Given better opportunities to developtheir skills and potentials, with betterchances of interaction with the civil societyand the state, community members canincrease their contribution to the eco-nomic, social, and cultural development oftheir communities.
It was within the context of these real-izations that the initial goals of the Net-work were formulated; these are to:• strengthen and empower each commu-
nity group through capacity building,planning and systematization of actions,meetings and exchange of experiencesand opportunities;
• improve the collective power, tostrengthen the capacity of communitiesto defend their right to health and to nego-tiate programs and public policies;
• increase social participation, so to influ-ence local governance and open avenuesfor communities to become stakeholdersin health (and other) public policies;
• increase visibility of positive actions infavelas, fighting prejudice and stigma.
The Network of Healthy Communitiespresently compromises 106 members -groups and associations that work for devel-opment and health promotion in poor com-munities in the State of Rio de Janeiro.According to a recent survey, the total pop-ulation of those territories is over 1.4 millionpeople. 68% of leaders are women, and 75%are African-Brazilian. 92% use their ownresources (including personal finances) fortheir work. They engage in all kinds offorums and committees to obtain resourcesto their communities and to voice theirproblems and needs. Their work reachesdirectly 130,000 people and many moreindirectly.
The Rio de Janeiro-based non-govern-mental organization Center for Health Pro-motion (Cedaps, 2007) acts as a technicaland political reference for support, chan-neling its resources, projects, and institu-tional partnerships to the Network. Cedapsbuilds the capacity of organizations to planstrategically and develop local actions,helps them to produce educational mate-rial and activities, articulates integratedactions and events, promotes partnershipsand strengthens the capacity to negotiatewith the government and the private sector.
To reach these goals, CEDAPS uses an empowerment-oriented methodology,“Shared Construction of Solutions” (Cedaps,2007), based on the Problem Solving for Bet-ter Health (PSBH) program, developed bythe Dreyfus Health Foundation, based inNew York, in more than 30 countries world-wide (Dreyfus Health Foundation, 2002).,and on additional elements from wellknown methodologies: Healthy Cities; Car-los Matus’Strategic Planning (Azevedo,1992); Local Development (Becker et al.,
Network of healthy communities of Rio de Janeiro – BrazilDaniel Becker1,2, Katia B. Edmundo1, Wanda Guimarães1, Maria S. Vasconcelos1, Daniella Bonatto1, Nilza R. Nunes1
and Ana Paula Baptista1
Abstract: Poor communities in Rio de Janeiro, which are known as favelas, suffer from various problems related to poor hous-ing, poverty, unemployment, violence and organized crime, and lack of access to basic services, such as health care and edu-cation. In order to tackle these determinants, and inspired by WHO’s international Healthy Communities/Cities movement, theNetwork of Healthy Communities of Rio de Janeiro was formed in 2004. The Network is coordinated by the Center for HealthPromotion (CEDAPS) and now includes more than 100 community groups and organizations in the state of Rio de Janeiro. Theiraim is to promote health, community development and equity through community empowerment, participation, capacity build-ing and advocacy. The paper describes the work that has been done since the Network’s inception and the challenges whichthey face to reach their goals in the context of a country like Brazil. The Network represents an important landmark of how poorpopulations can organize themselves in a collective, participatory and constructive way to influence public policy and strive forbetter conditions of life in disadvantaged settings, like the favelas. (Promotion & Education, 2007, (2): pp)
Key words: poor communities, empowerment, health promotion, equity
1. Centro de Promoção da Saúde (Center for Health Promotion) - CEDAPS, Rio de Janeiro, Brazil. Correspondence to Daniel Becker ([email protected]). 2. Instituto de Estudos em Saúde Coletiva, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brasil
Résumé en français à la page #. Resumen en español en la página #.

Showcasing networks
2005), Paulo Freire’s Popular Education(Freire, 2000) and others).
This social ‘technology’creates an oppor-tunity for the direct participation of commu-nity leaders and groups, enabling them tocontribute in problem solving, through indige-nously derived solutions that harness avail-able resources and partnerships. Thisenables mobilization of the community andits resources and a network of social projects,with solutions that have the potential to gen-erate direct impacts. The people who sufferwith the problems become problem solvers,active stakeholder,. acting to change the socialdeterminants of health. The collective con-struction systematizes and organizes localactions, promoting ownership and sustain-ability to the development process initiated.
Community-based interventions havecontributed to tackling issues such asdomestic and street violence, lack of cul-tural and sport activities, prevention ofHIV/Aids and other infectious diseases,adolescent pregnancy, income generation,environmental and sanitation problems,smoking, hypertension and diabetes andcommunity organization.
Meeting the challengesA major challenge of the network is how
to evaluate and demonstrate changes andbenefits of such a program, which workswith so many intangible variables; andtherefore, systematizing and collectingthese results is very important. Many of themember communities have been workingwith CEDAPS for more than 10 years to doso. Some of the results achieved at aprocess and output level are as follows:• 13 HIV/Aids community managed Pre-
vention Centers;• Almost 400,000 condoms distributed
every year;• More than 1,200 educational events and
activities yearly;• Several health promotion activities devel-
oped by community leaders;• Creation of innovative educational strate-
gies and material;• 700 adolescents in 11 communities have
participated in education programs thatpromote autonomy, self-esteem, andsocial entrepreneurship; 80% of themexpress better understanding of citizen-ship, better self care, social responsibil-ity, and better perspectives for the future;
Local development programs thatengage residents since the diagnosticsphase, creating integrated networks of com-munity projects in health, environment,leisure, education, and income generation.
Another important challenge consistson broadening those results into the col-lective perspective of a network organiza-
tion. In addition to strengthening localactions, it is also important to break the iso-lation and engage people in collective andsolidarity actions. Some indicators reflectthis empowerment process (Wallerstein,2006), such as, the leaders, who:• Learn to develop projects, to speak in
public, to organize their actions and phys-ical space;
• Establish partnerships, circulate in aca-demic and political environments;
• Negotiate and co-manage social pro-grams;
• Support the actions of their peers, dis-seminate information and opportunities,exchange experiences, get organized tofight for collective causes;
• Obtain media coverage and campaigns,gain visibility and break the segregationof favelas;
• Broaden their horizons, participating inforums, meetings, conferences, andcouncils.
A third challenge is to effectivelyincrease social participation in public poli-cies in a country like Brazil. In this area,changes have started to emerge. The Net-work is directly involved in partnershipswith public policies, in Primary Health Careprograms, the Pan-American Games in Riode Janeiro, groups that fight social violenceand others. In this regard, Cedaps is work-ing to improve the Network capacities inadvocacy and social control of publicresources.
The forth challenge is sustainability.CEDAPS doesn’t have a direct line of fund-ing for the Network’s activities, and it isstruggling to obtain resources that allow forintensifying the collective and capacitybuilding activities. In the long term, weexpect that cooperation with public policymakers will help to sustain the program.
Finally, there is also the challenge of howto disseminate this experience and facilitatean exchange. CEDAPS is constantly seekingfor such opportunities. As part of the Drey-fus Health Foundation’s global PSBH com-munity (with 30 countries), we plan to inte-grate other initiatives into an internationalnetwork of communities. Cedaps has pub-lished several articles about the Network, itis co-creating the Brazilian Network ofHealthy Communities and Municipalities,and has joined IUHPE’s Global Consortiumfor Community Health Promotion and theKnowledge Network for Urban Settings ofWHO’s Commission for Social Determi-nants of Health. Our next goal is to partici-pate in South-South cooperative programs.
PerspectivesThe Network of Healthy Communities
represents an important step in the ability
of poor populations to obtain better publicpolicies. Our work recognizes that there arecommunity leaders and groups that strivefor better conditions of life in favelas, andthat their work must be reinforced.
The Network is demonstrating that anorganized movement, created in a collec-tive, participatory, and constructive way,can reinforce the effectiveness of eachgroup, and create collective power forbroader and more ambitious achieve-ments. We hope that it will represent a land-mark for health promotion in communities.
We all seek utopia – an integrated, equi-table, and healthy city. As Mário Quintana,a Brazilian poet, used to say, «certain thingscannot be achieved, but this is not a rea-son to give up seeking them». The Networkof Healthy Communities wants utopia andworks to achieve it.
ReferencesAzevedo, C. da S. Planning and Management in the
Strategic-Situational Approach of Carlos Matus.Cad. Saúde Públ., Rio de Janeiro, 8 (2): 129-133,abr/jun, 1992.
Becker D, Edmundo K, Nunes NR, Bonatto D, de Souza R. An innovative geographical approach:health promotion and empowerment in a contextof extreme urban poverty. 1: Promot Educ. 2005;Suppl 3:48-52.
Center for Health Promotion / Centro de Promoção da Saúde (2007). - Network of HealthyCommunities of Rio de Janeiro – Brazil URL:http://www.cedaps.org.br/4010
Dreyfus Health Foundation (2002). Problem Solving for Better Health. Disponível no website:http://www.dhfglobal.org/psbh/psbh_2.html. NewYork: Dreyfus Health Foundation
Edmundo, K. 2003. A experiência do Centro de Promoção da Saúde nas comunidades popularesdo Rio de Janeiro. P.116-147. In Passarelli, C.A.;Parker, R.; Pimenta, C.; Terto jr., V. Aids eDesenvolvimento: interfaces e políticas públicas.Rio de Janeiro: ABIA.
FREIRE, Paulo. Pedagogia da autonomia: saberes necessários à prática educativa. 15. ed. SãoPaulo: Paz e Terra, 2000. p 36-37
Laverack, G., Labonte, R. (2000). A planning framework for community empowerment goalswithin health promotion. Health Policy andPlanning, 15(3), 255-62.
Kemenade, S. (2002). Social Capital as a Health Determinant - How is it Defined? AppliedResearch and Analysis Directorate; HealthCanada - Policy Research Communications Unit.URL: http://www.hc-sc.gc.ca/iacb-dgiac/arad-draa/english/rmdd/wpapers/engsocial.pdf
Tsouros, A. D. (1995) The WHO Healthy Cities Project: State of the art and future plans. HealthPromotion International, 10, 133–141
Rifkin, S.B. (2003). A Framework Linking CommunityEmpowerment and Health Equity: It Is a Matter ofCHOICE. Journal of Health, Population andNutrition, 21 (3), 168-180.
Wallerstein N. (2006) What is the evidence on eff ectiveness of empowerment to improve health?Copenhagen: WHO Regional Offi ce for Europe(Health Evidence Network Report). URL:www.euro. who.int/Document/E88086.pdf.
Westphal, M.F. (2000). O movimento Cidades / Comunidades Saudáveis: um compromisso coma qualidade de vida. Ciência e Saúde Coletiva,5(1), 39-51.
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 200746

47IUHPE – PROMOTION & EDUCATION SUPPLEMENT 2 2007
The founding role of the WHOEuropean Region
The Healthy Cities project was launchedin Europe in 1987 by the WHO RegionalOffice for Europe. It was clearly inspired bythe Ottawa Charter and the «Health for All»strategy. The public response revealed thatthe initiative was timely in a Europe, whichwas undergoing a political transition, espe-cially in the East. Besides the organization ofa formal WHO-led European Healthy CitiesNetwork, which has so far implemented overfour, 5-year phases of structured and goal-ori-ented collaborative activities with a limitednumber of especially committed cities, anopen process of regional and national net-working of interested cities and counties hasalso been stimulated.
The movement quickly spread and, aftertwo years, in 1989, more than 350 cities inEurope had declared themselves membersof a national healthy city network and manymore expressed their interest in joining toaddress the public concerns related tourban health and living conditions. Todaymore than 1300 cities, districts and countiesare members in more than 30 national net-works; however the motivational impetusto these efforts is clearly on the decline andneeds new political commitment to takethis process successfully into the future.
During the last 20 years the importanceof the urban dimension of living conditionsand the key role of local governance for theplanning of appropriate health services andand of sustainable living conditions hasbecome widely recognized . The Europeanregion has experienced enormous politicaland constitutional changes during thelast20 years . Between 1989 and 1996, 27 statesin the eastern part of the Region adoptednew constitutions with the overall trend to
decentralize and democratize politicalprocesses. Municipal governments havebeen delegated more responsibility andautonomy to set priorities and decide poli-cies in areas such as education, social serv-ices, health services, community care, envi-ronment, and health and urban planning.
During this process of change, a paral-lel process of dramatic decline of publicfinancial resources took also place andimposed severe constraints for political ini-tiatives at the local level. Under these cir-cumstances, the development of activitiesat the local level and the organization ofnational networks varied considerably inthe different countries and regions . Thestructure of national health systems, theexistence or lack of supportive national andregional policy frameworks for «Health forAll» or for sustainable development in thecontext of the Local Agenda 21, as well asthe distribution of responsibilities andresources for service delivery betweenlocal governments, regional structures andthe national governments, heavily influ-enced the potential for common actions.
During the first years of the EuropeanHealthy Cities network the WHO mainlyhelped to share information and to facilitatetraining and resource development for thenetworks. Later, in addition, it tried tostrengthen the organizational and strategiccapacity of the national networks and urgednational governments to recognize them asimportant structures and players in urbanand public health. Coordinators and politi-cal leaders from national healthy cities net-works met regularly and cooperateddirectly with WHO in a special Europeanforum for networks. An important achieve-ment of this cooperation has been the adop-tion of a common set of minimal standards
for a Healthy City and an action framework,which aspired to raise the professional stan-dards of healthy cities activities in the dif-ferent networks and their constituent cities.
As a new working method, city health pro-files or health development plans were intro-duced. These techniques were originallydeveloped by piloting within the WHO Euro-pean Healthy Cities network. The profilesshould provide a basis for a city to developan intersectoral plan for joint actions with itspartners derived from a quantitative andqualitative analysis of social, environmentaland health data, as well as the actual experi-ence of citizens. In some countries, membercities have undertaken population surveyswith the aim of spotlighting community pri-orities and citizens’views on health and envi-ronmental development.
National institutes of public health, uni-versities and other research organizationshave become increasingly important part-ners for many networks, since they cansecure a sound methodological approachfor core tasks, such as the city health pro-file. National networks and the improve-ment of international communication haveencouraged many cities to move away froma culture of organizing single events to a cul-ture of producing strategic health plans, inwhich promoting health through intersec-toral cooperation becomes an aim for allcity departments. The employment ofhealth promotion specialists at the munic-ipal level has fostered these innovativeprocesses in public bureaucracies.
Different surveys and assessments car-ried out in the European Region indicatethat long-established healthy cities net-works showed a clear potential to:• provide a testing ground for new partici-
patory health policies and citizen
Development of Healthy Cities networks in EuropeEberhard Goepel1
Abstract: The Healthy Cities network in Europe was inspired by the Ottawa Charter for Health Promotion when it was launchedin 1987. The networking process was initiated by the WHO Regional Office for Europe, but developed its own dynamics in differentEuropean countries during a time marked by fundamental political transformations in many of the countries of Eastern Europe.The networks then connected with the ‘Local Agenda 21’and the ‘Sustainable Cities and Towns Campaign’to create a new andbroader programmatic agenda at the local level. City Health Profiles and participatory policies, which can contribute to newforms of urban planning and local governance. In particular, the «Aalborg plus10 – commitments» of local governments in 2004have the potential to inspire a new phase of participatory and sustainable policies at the level of local communities in Europe.However the extent to which these initiatives will influence the macro-politics of the European Union towards a proclaimed“Europe of Citizens” remains to be watched carefully during the coming years. (Promotion & Education, 2007, (2): pp)
Key words: healthy cities, Europe, sustainability
1. Professor, University of Applied Sciences Magdeburg-Stendal, Dept. of Social and Health Care. Correspondence to: Breitscheidstr.2. D – 39114 Magdeburg,Germany ([email protected])
Résumé en français à la page #. Resumen en español en la página #.
Showcasing networks
Showcasing networks
involvement;• generate and disseminate knowledge and
new ideas through cooperation, confer-ences, newsletters, websites and organi-zational development;
• promote best practices by setting stan-dards, giving guidance and consultation,providing training and supporting theprofessional development of health pro-motion specialists;
• strengthen local capacities in adoptinggood governance approaches based onthe principles of «Health for All» and theLocal Agenda 21;
• inform national policy developments bycondensing and advocating local needs.
Opening towards sustainabledevelopment and health in aglobal context
During the last 10 years a number ofattempts have been made in Europe to link
the Healthy Cities networks with urbanplanning and sustainable local develop-ment initiatives.
The following principles were seen askey for healthy urban planning (Barton etal., 2003):• Human health as a key facet of sustain-
able development• Cooperation between planning and
health agencies• Cooperation between the public and the
private sectors• Community consultation and empower-
ment• Political commitments at the highest level• Health integrated plans and policies• Health integration at all scales from
macro to micro• A comprehensive approach to determi-
nants of health• Evidence-based planning for health
WHO Regional Office for Europe hasmade healthy urban planning a core devel-opmental theme of the fourth phase (2003-2007) of the European Healthy Cities Net-work.
Common programmes at the level of theEuropean Union have been launched,which led in 1994 to the Sustainable Citiesand Towns Campaign to integrate healthinto the broader sustainability discourse.
The national Healthy Cities networks inEurope rarely reached the level of commongoal setting with regard to local policydevelopment. The Sustainable Cities andTowns Campaign, conversely, initiallyobtained 80 European local authorities tosign up to the Aalborg Charter on ‘Euro-pean cities and towns towards sustainabil-ity’and committed themselves to its objec-tives. This document was then renewed in2004 with the “Aalborg plus 10 – commit-
ments” including a common vision that“cities and towns are inclusive, prosperous,creative and sustainable, and provide agood quality of life for all citizens andenable their participation in all aspects ofurban life.” (Aalborg Commitments, 2004)The amended document takes into accountthe challenges faced with globalization andthe revolution in technology, as well as theother social, economic, environmental andpolitical determinants; and underlines thatworking with all the spheres of governmentis central to combat the determinants.
The next European conference of theSustainable Cities and Towns Campaign inSevilla (Spain) in 2007 will reveal the extentto which the ambitious commitments laidout by the Charter have gained substantialsupport by the different European govern-ments and the European Commission onthe route towards a proclaimed “Europe ofCitizens”.
References:Aalborg Commitments (2004) “Aalborg+10 Inspiring
Futures” Available:http://www.aalborgplus10.dk/media/finaldraftaalborgcommitments.pdf
City planning for health and sustainable development.1997. European Health andsustainable development series 2,Copenhagen:WHO Regional Office for Europe
Hugh Barton, Claire Mitcham, Catherine Tsourou . 2003. Healthy urban planning inpractice:Experience of European cities.Copenhagen: WHO Regional Office for Europe
Sustainable Cities and Towns Campaign www.sustainable-cities.eu
World Health Organization, Regional Office for Europe. Healthy cities and governance.http://www.euro.who.int/healthy-cities
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 200748

49IUHPE – PROMOTION & EDUCATION SUPPLEMENT 2 2007
EQUINET was formed to promote andrealize shared values of equity and social jus-tice in health. It involves people working ingovernment, civil society, research, Parlia-ment and other institutions in east and south-ern Africa (ESA) (www.equinetafrica.org).
We have since 1998 used and supportedresearch and policy analysis, held forumsfor skills development, analysis, dialogue,learning and engagement, strengthened net-works and formed alliances towards achiev-ing health equity. These activities jointlyhave contributed to an affirmative visionof the health systems that we would want tobuild to deliver on equity goals.
The lessons learned indicate thatachieving equity, while demanding techni-cal and public policy choices, is centred ona strong state and public sector in health,organised around the active participationand involvement of communities. As foundin other regions, rising investment in healththrough the public sector is necessary tosupport the universal health systems andredistributional policies necessary forimproved health outcomes (UNDP HDR2003; EQUINET SC 2000).
Different areas of work in EQUINET thusfeed into an understanding of how toachieve this, with research, capacity build-ing, policy dialogue and informationexchange to:• Support the strengthening of ppeeooppllee’’ssppoowweerr ffoorr hheeaalltthh,, including the power andability that people have to make and imple-ment choices over health inputs. Work inthe network is informing parliamentary andcivil society processes and building skillsfor participatory methods in health sys-tems. EQUINET supported research high-lights that public participation in health canhave a positive impact on health outcomesand the performance of health systems,particularly when linked to mobilisation
around collective action to realise socialand economic rights (Loewenson et al 2005;Ngulube et al 2005; London 2004). • Provide iinnccrreeaasseedd ffaaiirr,, ssuussttaaiinnaabbllee aannddeeqquuiittaabbllee ffiinnaanncciinngg for health at national,regional and global level. This includesexploring options for increasing resourcemobilization through mechanisms that pro-vide for universality (like taxes and socialhealth insurance), and that protect house-holds against the impoverishing effects ofhealth costs. This complements work doneon mechanisms for allocating publicresources fairly between geographicalareas, in reflection of health need (McIntyreet al 2005). • EEnnssuurree tthhaatt hheeaalltthh wwoorrkkeerrss aarree vvaalluueedd,,mmoottiivvaatteedd aanndd rreettaaiinneedd wwiitthhiinn oouurr hheeaalltthhssyysstteemmss.. Responding to the outflow ofskilled health workers from public sectordistrict health systems to high incomecountries, work is underway with theRegional health secretariat in east, centraland southern Africa to review and supportimplementation of incentives to retainhealth workers and to identify and proposeoptions to manage the costs and benefitsof health worker migration. (EQUINET,TARSC, HST, UNAM 2006)• CChhaalllleennggee ttrraaddee lliibbeerraalliizzaattiioonn aannddeennccrrooaacchhmmeenntt oonn hheeaalltthh, through identi-fying ways of protecting health in tradeagreements, and exploring how health sys-tems can promote nutrition in ways thatsupport household control of food pro-duction, particularly for women farmers(Bond 2006, Chopra 2005).
Challenges to equity actionsAs in many networks, EQUINET faces
challenges of communicating across differ-ent constituencies, and of spreading skillsand capacities across the region in a con-text of under-resourced institutions facing
multiple demands. While universal accessto life-saving antiretroviral medicines (ART)is now recognized as a policy goal, treat-ment access is still affected by constraintswithin health systems. This calls for ‘learn-ing while doing’ approaches that shareknowledge and experience while imple-menting change (Makwiza et al 2005). Weare challenged to learn not only about whatmeasures and processes will enhancehealth equity, but also how to advanceequity-oriented change in policy and prac-tice in ways that strengthen local capabili-ties and autonomy.
“I learned that learning participatoryapproaches starts with three days andtakes three decades”Participant at an EQUINET training work-shop, Tanzania 2006
We do this in a process of globalizationthat is unequal in its distribution of costs andbenefits, weak in regulating and managingits social costs and promoting market ledreforms within the health sector that wideninequalities in health (UN WCSDG 2004;EQUINET SC 2004) . As the health costs ofsuch polarization visibly increase, so toodoes the gain from networking across coun-tries to protect equity in health in the region.
EQUINET: Networking for equity in health in east andsouthern AfricaRene Loewenson1
Abstract: This short report outlines the perspectives and motivations for the work of the Regional Network for Equity in Health ineast and southern Africa (EQUINET). It presents key areas of work on health equity being implemented to strengthen the stateand public sector in health, organised around the active participation and involvement of communities. This includes work on strength-ening people’s power for health, on increased fair financing; on retaining health workers and challenging trade policies that encroachon health. Such work faces challenges that can be met through increased regional networking to exchange experience, informa-tion and expertise, particularly given the demand for ìlearning by doingî. (Promotion & Education, 2007, (2): pp)
Key words: health equity; Africa; networks
1. Regional Network for Equity in Health in east and southern Africa (EQUINET). Correspondence to Equinet Secretariat: Training and Research Support Centre, BoxCY2720, Causeway, Harare, Zimbabwe ([email protected])
Résumé en français à la page #. Resumen en español en la página #.
Showcasing networks

Showcasing networks
Acknowledgements:This article outlines work of institutions inEQUINET more fully described and published at. EQUINET is governed by a steering commit-tee involving institutions leading work in the net-work in east and southern Africa, ie Training andResearch Support Centre, Peoples HealthMovement Tanzania ; Community WorkingGroup on Health, University of Zimbabwe,CHESSORE, Centre for Health Policy Wits Uni-versity, Health Economics Unit University ofCape Town, Tanesa Tanzania; Malawi HealthEquity Network; ; Health Systems Trust, Uni-versity of Namibia, University of Cape Town; Uni-versity of Western Cape; Health SciencesResearch Council South Africa and Southernand east African Trade and Information Negoti-ations Institute, Southern and east African asso-ciation of parliamentary committees on healthand REACH Trust Malawi.
ReferencesBond, P (2006) The dispossession of African
wealth at the cost of African health EQUINETDiscussion paper 30, Ideas studio, South Africa:
Chopra M (2004) Food Security, Rural DevelopmentAnd Health Equity In Southern Africa, EQUINETdiscussion paper Ideas studio, South Africa
EQUINET SC (2004) Reclaiming the state: Advancing people’s health, challenging injustice,Policy paper 15, Hunyani printers, Zimbabwe
EQUINET; TARSC; Health Systems Trust; Universityof Namibia (2006) ìReport of regional planningmeeting: Retention and migration of healthpersonnel in southern Africa, 3 April 2006,Lusaka Zambia,î EQUINET meeting report.EQUINET: Harare.
Loewenson R, Rusike I, Zulu M (2005) ìThe impact of Health Centre Committees on health outcomesin Zimbabwe,î Plenary paper presented at GlobalForum for Health Research, Forum 9: Poverty,equity and health research Conference, MumbaiIndia, 12-16 September 2005.
London L. (2004) How can human rights serve as a tool for health equity? Third InternationalConference of the International Society for Equityin Health (ISEqH), Durban, South Africa, June 10-12, 2004
Makwiza, I; Nyirenda, L; Bongololo, G; Loewenson, R; Theobald, S (2005) ìMonitoring equity andhealth systems in the provision of Anti-retroviralTherapy (ART): Malawi Country report,î EQUINETDiscussion paper 24. EQUINET: Harare.
McIntyre D, Gilson L, Mutyambizi V (2005). Promoting equitable health care financing in theAfrican context: Current challenges and futureprospects. EQUINET Discussion Paper 27.Harare: Health Economics Unit, Centre for HealthPolicy, Ideas Studio, South Africa
Ngulube TJ, Mdhluli L, Gondwe K, Njobvu CA (2004) Governance, participatory mechanismsand structures in Zambia’s health system:EQUINET Discussion paper 21: Mimeo, Zambia
UNDP (2003) Human Development Report, Oxford University Press, New York
UN World Commission on the Social Dimension of Globalisation (WCSDG) (2004) A fairGlobalisation: Creating opportunities for all, ILO,Geneva 2003.
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 200750

51IUHPE – PROMOTION & EDUCATION SUPPLEMENT 2 2007
The Global Equity Gauge Alliance(GEGA) is an international network ofgroups in developing countries that facili-tate processes designed to confront andmitigate inequities in health. In 1999 and2000, a series of meetings involvingresearchers and activist NGOs noted that,despite the 1978 Alma Ata Declaration,which emphasizes the importance of equityfor the attainment of good health, inequitiesstill, prevailed and continued to grow world-wide. The concern that few countries weregiving adequate attention to measuring andmonitoring equity in health, healthcare,and the underlying determinants of health,culminated in the establishment of anorganized consortium of eleven (nowgrown to fifteen) health equity projects,called Equity Gauges, based in Asia, Africaand Latin America.
Equity Gauges focus on disparities thatare unjust and unfair, and place healthequity squarely within the larger frame-work of social justice. Their focus goesbeyond the monitoring of inequities. EquityGauges aim to contribute towards the sus-tained decline in inequities in both thebroad sociopolitical determinants of healthas well as inequities in the health system.On the understanding that socio-politicaland health inequities are mediated by dif-ferentials in power, the Equity Gauge strat-egy includes an explicit set of activitiesdesigned to empower those who are mar-ginalised and disempowered as an essentialelement of improving health equity. Thisactive approach to equity is supportedthrough three broad spheres of action,called «pillars» of the Equity Gauge. TheMeasurement and Monitoring pillar isfocused on monitoring and measuring pop-ulation health, and identifying socioeco-
nomic and other determinants at work;advocacy for pro-equity policy aims tomotivate action by policy makers and toincrease accountability; and, the commu-nity empowerment pillar aims to amplifythe voices of marginalised communitiesand plays a critical role in creating a sus-tainable culture of expectation for equity insociety.
Equity Gauge teams are varied in theirmembership and include representationfrom Ministries of Health, Education, Waterand Sanitation, local governments, legisla-tors, policy makers, community organisa-tions, public and private research and pol-icy institutions, universities, internationalNGOs and other social groups. Thesediverse groupings utilize the three pillarapproach to formulate individual countryor local area activities that promote theinteraction between research and evidencebased policy formulation and implementa-tion, and interaction between the commu-nity and policy makers.
Research conducted by Equity Gaugeshas been influential in the inclusion ofequity indicators in some national infor-mation data sets, has strengthened meas-urement capacities at country level, andhas pointed to the need for regular moni-toring of inequities in health. In SouthAfrica, the Cape Town Equity Gaugedemonstrated the unfair allocation of finan-cial and human resources between healthdistricts serving those who are rich andthose serving poor communities in the met-ropolitan council and their work led to pol-icy changes in human resource allocations.Need reference here
Some of the success of the Gauges hasbeen attributed to the inclusion of politicalrepresentatives and senior health man-
agers in the steering committee of the proj-ect. The inclusion of parliamentarians ascore Equity Gauge team members has pro-moted the use of research to assist them inmonitoring the implementation of pro-equity policies. An additional benefit hasbeen the strengthening of participating par-liamentarians appreciation of the differencebetween «pro-poor» and «equity oriented»activities and policies.
Reliable and valid information gatheredfrom the measurement process forms astrong basis for evidence based policy rec-ommendations and raising of public aware-ness. Equity updates emanating fromequity studies are disseminated throughpublications, newsletters, newspaper arti-cles, conferences and seminars with policymakers and training workshops. TheChilean, Nairobi and Zambian Gauges haveheld Equity workshops for journalists toensure that concepts of health equity filterinto the public domain. These platformsprovide advocacy opportunities in whichthe potential of evidence gathered locallyfor pro-equity policy development isdemonstrated.
Evidence gathered by Gauges assists inidentifying communities affected by unjustresource allocation. Equity Gauges collab-orate with affected communities to makeinformation available and accessible and toadvocate for pro-equity changes. This col-laborative and empowering effort has attimes resulted in the development of thecommunity’s own monitoring processesand the recognition of the right of the com-munity to participate in the planning, imple-mentation and management of health andother social services.
The Pakistan Equity Gauge facilitatedthe process of understanding fairness in
Global Equity Gauge AllianceAntoinette Ntuli1
Abstract: The lack of attention to equity in health, health care and determinants of health is a burden to the attainment of goodhealth in many countries. With this underlying problem as a basis, a series of meetings took place between 1999 and 2000,culminating in the creation the Global Equity Gauge Alliance (GEGA). GEGA is an international network of groups in developingcountries, mainly Asia, Africa and Latin America, which develop projects designed to confront and mitigate inequities in health,know as Equity Gauges. Equity Gauges aim to contribute towards the sustained decline in inequities in both the broad sociopo-litical determinants of health, as well as inequities in the health system. Their approach is based on three broad spheres of action,known as «pillars»: 1) measurement and monitoring, 2) advocacy, and 3) community empowerment. Through a series of exam-ples from local or national level gauges, this paper showcases their work promoting the interaction between research and evi-dence based policy formulation and implementation, and the interaction between the community and policy makers. (Promo-tion & Education, 2007, (2): pp)
Key words: equity, determinants of health, empowerment
1. Chair, Global Equity Gauge Alliance (http://www.gega.org.za/) Correspondence to: [email protected]
Résumé en français à la page #. Resumen en español en la página #.
Showcasing networks

Showcasing networks
health and included participation of menand women from a rural district, health careproviders from public service, NGOs, andelected representatives. In twenty three vil-lages men and women conducted an equityanalysis separately and prioritized dispari-ties that would receive immediate attention.A joint workshop attended by villagers,local government, civil society and com-munity members resulted in the develop-ment of an advocacy plan aimed at influ-encing stakeholders to work on theidentified disparities.
In Zambia, a series of in-depth work-shops at the local level involving commu-nity representatives and health workers ledto joint action that improved the quality ofcare, strengthened skills for local monitor-
ing and assessment, increased the com-munities’capacities to influence local deci-sion making, and amplified communityvoices at national level.
Many of the Equity Gauges originatedin research and tertiary institutions with an«expert» role in research. This has provedto be a limiting factor for implementing thecommunity empowerment pillar whichrequires specific sets of technical abilitiesand which can be time consuming. Thischallenge is being overcome throughcapacity development of the Gauges them-selves and through collaboration with localorganisations recognised for their expertisein community development.
GEGA has also been active at the globallevel. Concern with unjust international
political and economic frameworks andpolicies has resulted in GEGA partneringwith health activist organizations, includingthe People’s Health Movement and Medact,to produce the Global Health Watch, evi-dence based analysis of the political econ-omy of health and health care.
GEGA’s shared vision and approach hasbenefited Alliance partners and hasenabled:• Sharing of lessons learnt and experiences
between the different Gauges• The creation of critical mass of experience
to enable evaluation of the Equity Gaugestrategy and to develop a proof of concept
• Sharing of skills and expertise betweenGauges
• Country Location of Equity Gauges
IUHPE – PROMOTION & EDUCATION VOL. XIV, NO. 1 200752
Showcasing networks – Abstract
The Quebec Healthy Cities and Towns Network: a powerful movement faced with newchallengesP. Simard
After twenty years serving its members, the Quebec Healthy Cities and Towns Network (QHCTN) faces several challenges. Thereare currently many changes being made in the local organization and the administration of services. The Network, through its capacityto mobilize the different municipalities, is the best placed to advocate and support a coordinated approach to government initiativesand also to encourage partnerships with other institutions (education, health, socio-economic) and communities. There is, nonethe-less, a need to rethink its direct support to members, especially in terms of communication and networking among them.
Country Location of Equity Gauges