intoxication au co et aux fumees...
TRANSCRIPT

mathieucoulangeap-hmfr
Meacutedecine Hyperbare Subaquatique et Maritime Pocircle Reacuteanimation Urgences SAMU Hyperbarie CHU Marseille
Institut de Meacutedecine et de Physiologie en Milieu Maritime et en Environnement Extrecircme - PHYMAREX
Centre National de Plongeacutee de Secours Nautique amp de Survie ECASC SDIS04
UMR MD2 Dysoxie Tissulaire Aix Marseille Universiteacute
Socieacuteteacute Nationale de Sauvetage en Mer - SNSM
INTOXICATION AU CO ET AUX FUMEES DrsquoINCENDIEDESC MEDECINE DrsquoURGENCE ndash MARSEILLE ndash 06022017
Intoxication CO ndash 050106
bull 400 deacutecegraves (1egravere cause par intox)
bull 8000 cas an en France
bull 30 drsquoerreurs diagnostics
bull Seacutequelles agrave long terme
2
1 Bref rappel sur la physiopathologie
2 Deacutemarche diagnostique et filiegravere de soins
3 Speacutecificiteacutes de la fumeacutee drsquoincendie
O2
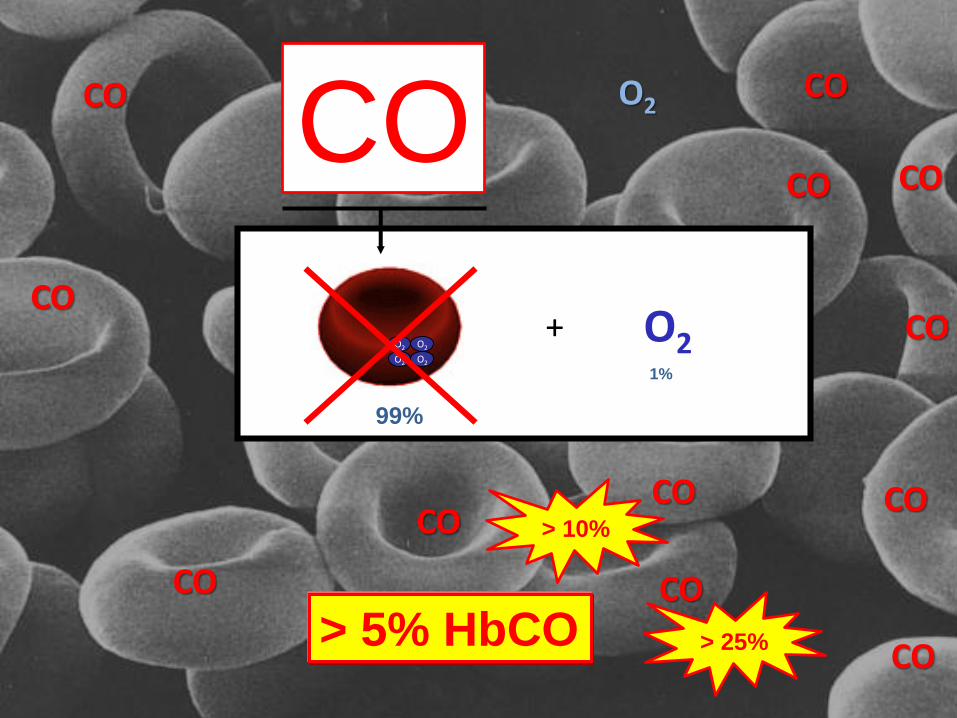
CO
5
O2 O2
O2 O2O2+
99
1
CO
CO
CO
CO
CO
CO
CO O2
CO
CO
CO
CO
COCO
gt 5 HbCO
gt 10
gt 25
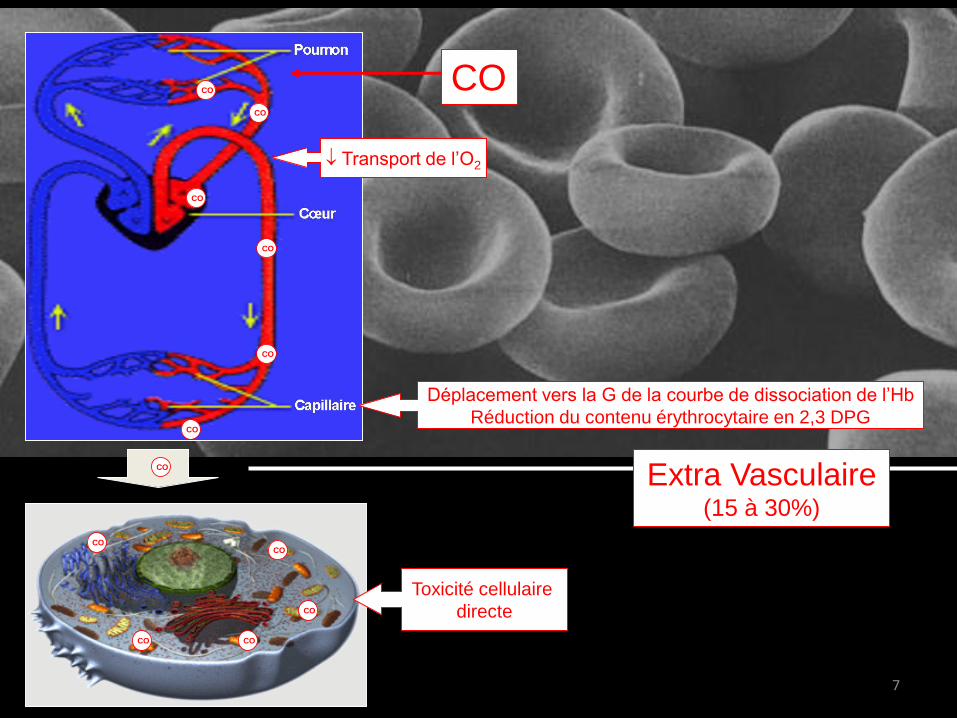
Transport de lrsquoO2
CO
CO
CO
CO
CO
CO
CO
CO
CO CO
CO
COCO
Toxiciteacute cellulaire
directe
Extra Vasculaire(15 agrave 30)
Deacuteplacement vers la G de la courbe de dissociation de lrsquoHb
Reacuteduction du contenu eacuterythrocytaire en 23 DPG
7
Transport de lrsquoO2
CO
CO
CO
CO
CO
CO
CO
CO
CO CO
CO
COCO
Toxiciteacute cellulaire
Directe
Extra Vasculaire(15 agrave 30)
Deacuteplacement vers la G de la courbe de dissociation de lrsquoHb
Reacuteduction du contenu eacuterythrocytaire en 23 DPG
8
9
bull Interrogatoire +++
bull Polyvictimes animaux domestiques
bull Soudaineteacute et variabiliteacute dans le tempshellip
DIAGNOSTIC POSITIF 10
Peu speacutecifiqueInfection virale
Intox alimentaire
Grossesse
Coronaropathie
Consommation de toxique
Patho neurovasculaire ou psy hellip
CLINIQUE = DIAGNOSTIC DE GRAVITE
SOURCE
COMBUSTION
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
INCOMPLETE
13
COMBUSTION INCOMPLETE
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
50
14
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
Intoxication CO ndash 050106
bull 400 deacutecegraves (1egravere cause par intox)
bull 8000 cas an en France
bull 30 drsquoerreurs diagnostics
bull Seacutequelles agrave long terme
2
1 Bref rappel sur la physiopathologie
2 Deacutemarche diagnostique et filiegravere de soins
3 Speacutecificiteacutes de la fumeacutee drsquoincendie
O2
CO
5
O2 O2
O2 O2O2+
99
1
CO
CO
CO
CO
CO
CO
CO O2
CO
CO
CO
CO
COCO
gt 5 HbCO
gt 10
gt 25
Transport de lrsquoO2
CO
CO
CO
CO
CO
CO
CO
CO
CO CO
CO
COCO
Toxiciteacute cellulaire
directe
Extra Vasculaire(15 agrave 30)
Deacuteplacement vers la G de la courbe de dissociation de lrsquoHb
Reacuteduction du contenu eacuterythrocytaire en 23 DPG
7
Transport de lrsquoO2
CO
CO
CO
CO
CO
CO
CO
CO
CO CO
CO
COCO
Toxiciteacute cellulaire
Directe
Extra Vasculaire(15 agrave 30)
Deacuteplacement vers la G de la courbe de dissociation de lrsquoHb
Reacuteduction du contenu eacuterythrocytaire en 23 DPG
8
9
bull Interrogatoire +++
bull Polyvictimes animaux domestiques
bull Soudaineteacute et variabiliteacute dans le tempshellip
DIAGNOSTIC POSITIF 10
Peu speacutecifiqueInfection virale
Intox alimentaire
Grossesse
Coronaropathie
Consommation de toxique
Patho neurovasculaire ou psy hellip
CLINIQUE = DIAGNOSTIC DE GRAVITE
SOURCE
COMBUSTION
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
INCOMPLETE
13
COMBUSTION INCOMPLETE
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
50
14
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
1 Bref rappel sur la physiopathologie
2 Deacutemarche diagnostique et filiegravere de soins
3 Speacutecificiteacutes de la fumeacutee drsquoincendie
O2
CO
5
O2 O2
O2 O2O2+
99
1
CO
CO
CO
CO
CO
CO
CO O2
CO
CO
CO
CO
COCO
gt 5 HbCO
gt 10
gt 25
Transport de lrsquoO2
CO
CO
CO
CO
CO
CO
CO
CO
CO CO
CO
COCO
Toxiciteacute cellulaire
directe
Extra Vasculaire(15 agrave 30)
Deacuteplacement vers la G de la courbe de dissociation de lrsquoHb
Reacuteduction du contenu eacuterythrocytaire en 23 DPG
7
Transport de lrsquoO2
CO
CO
CO
CO
CO
CO
CO
CO
CO CO
CO
COCO
Toxiciteacute cellulaire
Directe
Extra Vasculaire(15 agrave 30)
Deacuteplacement vers la G de la courbe de dissociation de lrsquoHb
Reacuteduction du contenu eacuterythrocytaire en 23 DPG
8
9
bull Interrogatoire +++
bull Polyvictimes animaux domestiques
bull Soudaineteacute et variabiliteacute dans le tempshellip
DIAGNOSTIC POSITIF 10
Peu speacutecifiqueInfection virale
Intox alimentaire
Grossesse
Coronaropathie
Consommation de toxique
Patho neurovasculaire ou psy hellip
CLINIQUE = DIAGNOSTIC DE GRAVITE
SOURCE
COMBUSTION
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
INCOMPLETE
13
COMBUSTION INCOMPLETE
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
50
14
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
O2
CO
5
O2 O2
O2 O2O2+
99
1
CO
CO
CO
CO
CO
CO
CO O2
CO
CO
CO
CO
COCO
gt 5 HbCO
gt 10
gt 25
Transport de lrsquoO2
CO
CO
CO
CO
CO
CO
CO
CO
CO CO
CO
COCO
Toxiciteacute cellulaire
directe
Extra Vasculaire(15 agrave 30)
Deacuteplacement vers la G de la courbe de dissociation de lrsquoHb
Reacuteduction du contenu eacuterythrocytaire en 23 DPG
7
Transport de lrsquoO2
CO
CO
CO
CO
CO
CO
CO
CO
CO CO
CO
COCO
Toxiciteacute cellulaire
Directe
Extra Vasculaire(15 agrave 30)
Deacuteplacement vers la G de la courbe de dissociation de lrsquoHb
Reacuteduction du contenu eacuterythrocytaire en 23 DPG
8
9
bull Interrogatoire +++
bull Polyvictimes animaux domestiques
bull Soudaineteacute et variabiliteacute dans le tempshellip
DIAGNOSTIC POSITIF 10
Peu speacutecifiqueInfection virale
Intox alimentaire
Grossesse
Coronaropathie
Consommation de toxique
Patho neurovasculaire ou psy hellip
CLINIQUE = DIAGNOSTIC DE GRAVITE
SOURCE
COMBUSTION
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
INCOMPLETE
13
COMBUSTION INCOMPLETE
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
50
14
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
O2 O2
O2 O2O2+
99
1
CO
CO
CO
CO
CO
CO
CO O2
CO
CO
CO
CO
COCO
gt 5 HbCO
gt 10
gt 25
Transport de lrsquoO2
CO
CO
CO
CO
CO
CO
CO
CO
CO CO
CO
COCO
Toxiciteacute cellulaire
directe
Extra Vasculaire(15 agrave 30)
Deacuteplacement vers la G de la courbe de dissociation de lrsquoHb
Reacuteduction du contenu eacuterythrocytaire en 23 DPG
7
Transport de lrsquoO2
CO
CO
CO
CO
CO
CO
CO
CO
CO CO
CO
COCO
Toxiciteacute cellulaire
Directe
Extra Vasculaire(15 agrave 30)
Deacuteplacement vers la G de la courbe de dissociation de lrsquoHb
Reacuteduction du contenu eacuterythrocytaire en 23 DPG
8
9
bull Interrogatoire +++
bull Polyvictimes animaux domestiques
bull Soudaineteacute et variabiliteacute dans le tempshellip
DIAGNOSTIC POSITIF 10
Peu speacutecifiqueInfection virale
Intox alimentaire
Grossesse
Coronaropathie
Consommation de toxique
Patho neurovasculaire ou psy hellip
CLINIQUE = DIAGNOSTIC DE GRAVITE
SOURCE
COMBUSTION
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
INCOMPLETE
13
COMBUSTION INCOMPLETE
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
50
14
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
Transport de lrsquoO2
CO
CO
CO
CO
CO
CO
CO
CO
CO CO
CO
COCO
Toxiciteacute cellulaire
directe
Extra Vasculaire(15 agrave 30)
Deacuteplacement vers la G de la courbe de dissociation de lrsquoHb
Reacuteduction du contenu eacuterythrocytaire en 23 DPG
7
Transport de lrsquoO2
CO
CO
CO
CO
CO
CO
CO
CO
CO CO
CO
COCO
Toxiciteacute cellulaire
Directe
Extra Vasculaire(15 agrave 30)
Deacuteplacement vers la G de la courbe de dissociation de lrsquoHb
Reacuteduction du contenu eacuterythrocytaire en 23 DPG
8
9
bull Interrogatoire +++
bull Polyvictimes animaux domestiques
bull Soudaineteacute et variabiliteacute dans le tempshellip
DIAGNOSTIC POSITIF 10
Peu speacutecifiqueInfection virale
Intox alimentaire
Grossesse
Coronaropathie
Consommation de toxique
Patho neurovasculaire ou psy hellip
CLINIQUE = DIAGNOSTIC DE GRAVITE
SOURCE
COMBUSTION
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
INCOMPLETE
13
COMBUSTION INCOMPLETE
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
50
14
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
Transport de lrsquoO2
CO
CO
CO
CO
CO
CO
CO
CO
CO CO
CO
COCO
Toxiciteacute cellulaire
Directe
Extra Vasculaire(15 agrave 30)
Deacuteplacement vers la G de la courbe de dissociation de lrsquoHb
Reacuteduction du contenu eacuterythrocytaire en 23 DPG
8
9
bull Interrogatoire +++
bull Polyvictimes animaux domestiques
bull Soudaineteacute et variabiliteacute dans le tempshellip
DIAGNOSTIC POSITIF 10
Peu speacutecifiqueInfection virale
Intox alimentaire
Grossesse
Coronaropathie
Consommation de toxique
Patho neurovasculaire ou psy hellip
CLINIQUE = DIAGNOSTIC DE GRAVITE
SOURCE
COMBUSTION
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
INCOMPLETE
13
COMBUSTION INCOMPLETE
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
50
14
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
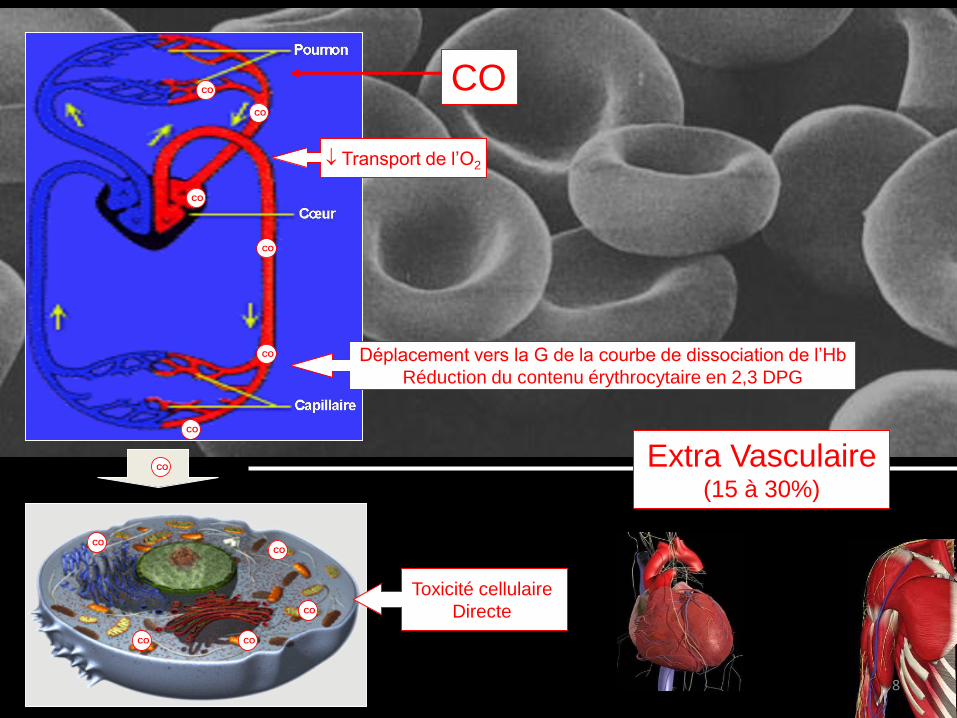
9
bull Interrogatoire +++
bull Polyvictimes animaux domestiques
bull Soudaineteacute et variabiliteacute dans le tempshellip
DIAGNOSTIC POSITIF 10
Peu speacutecifiqueInfection virale
Intox alimentaire
Grossesse
Coronaropathie
Consommation de toxique
Patho neurovasculaire ou psy hellip
CLINIQUE = DIAGNOSTIC DE GRAVITE
SOURCE
COMBUSTION
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
INCOMPLETE
13
COMBUSTION INCOMPLETE
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
50
14
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
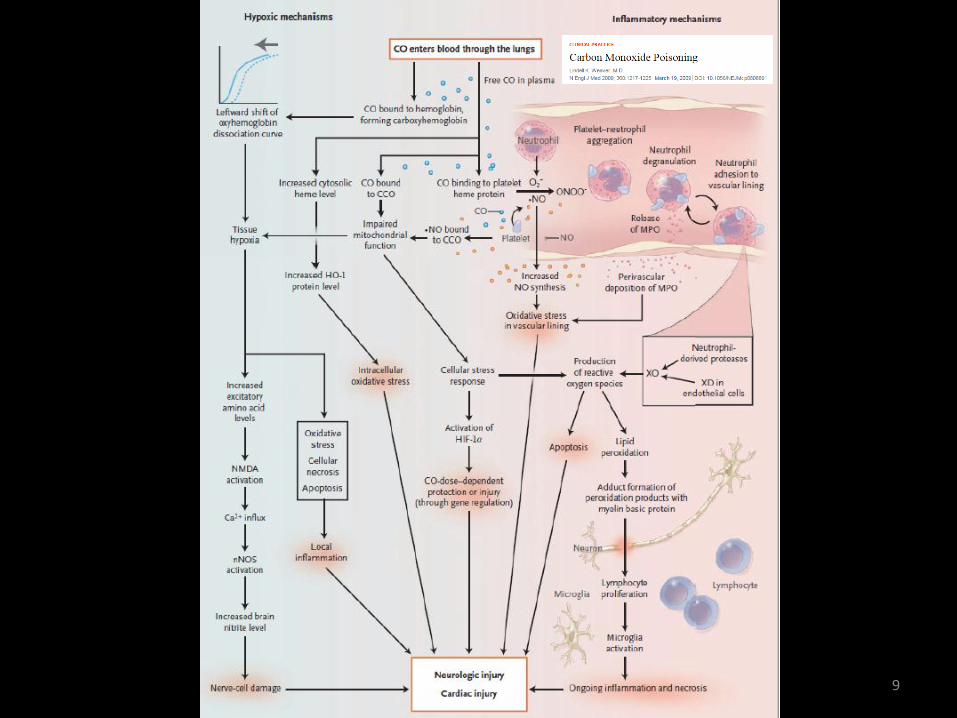
bull Interrogatoire +++
bull Polyvictimes animaux domestiques
bull Soudaineteacute et variabiliteacute dans le tempshellip
DIAGNOSTIC POSITIF 10
Peu speacutecifiqueInfection virale
Intox alimentaire
Grossesse
Coronaropathie
Consommation de toxique
Patho neurovasculaire ou psy hellip
CLINIQUE = DIAGNOSTIC DE GRAVITE
SOURCE
COMBUSTION
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
INCOMPLETE
13
COMBUSTION INCOMPLETE
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
50
14
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
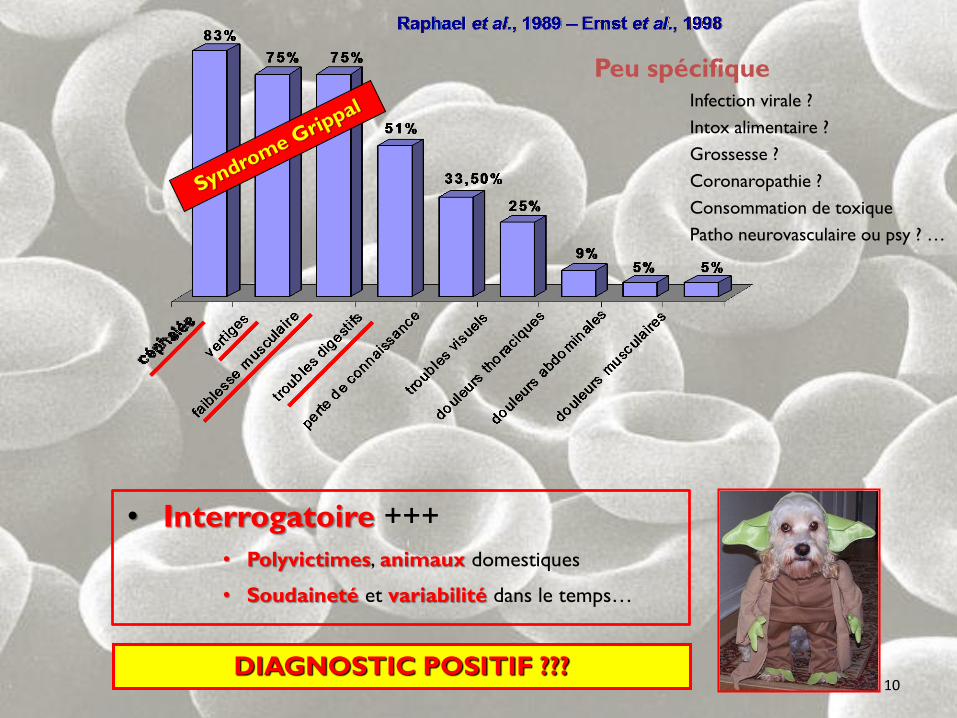
CLINIQUE = DIAGNOSTIC DE GRAVITE
SOURCE
COMBUSTION
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
INCOMPLETE
13
COMBUSTION INCOMPLETE
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
50
14
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
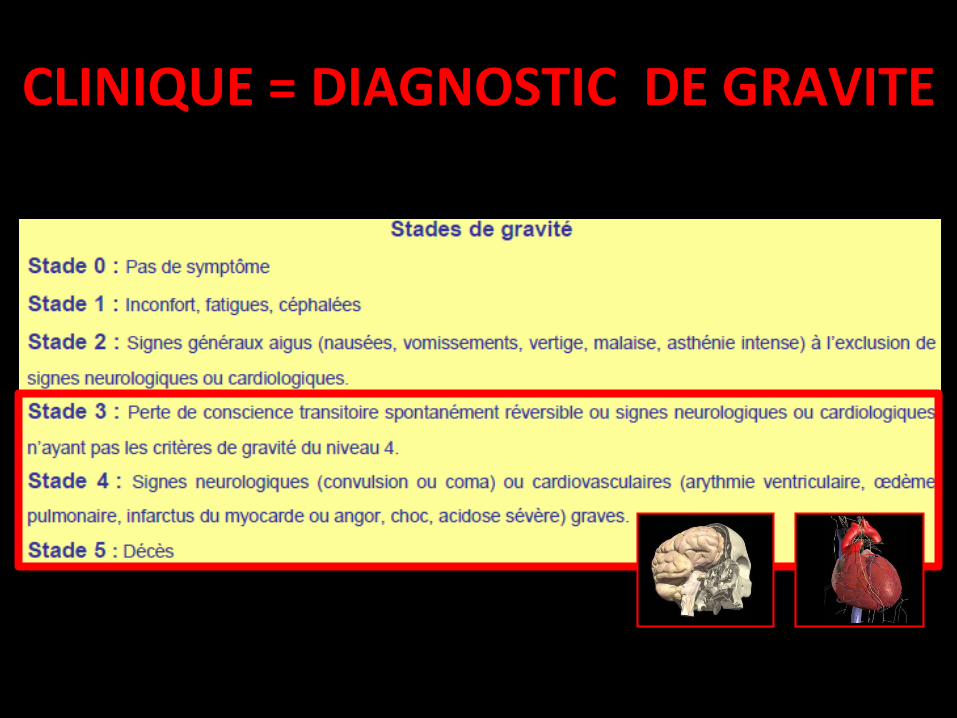
SOURCE
COMBUSTION
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
INCOMPLETE
13
COMBUSTION INCOMPLETE
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
50
14
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
COMBUSTION
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
INCOMPLETE
13
COMBUSTION INCOMPLETE
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
50
14
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
COMBUSTION INCOMPLETE
C + O2 rarr H2O + CO2
C + frac12 O2 rarr H2O + CO
50
14
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
17
18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

18
DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

DETECTER
Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

Dans lrsquoATMOSPHERE gt 50 PPM
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
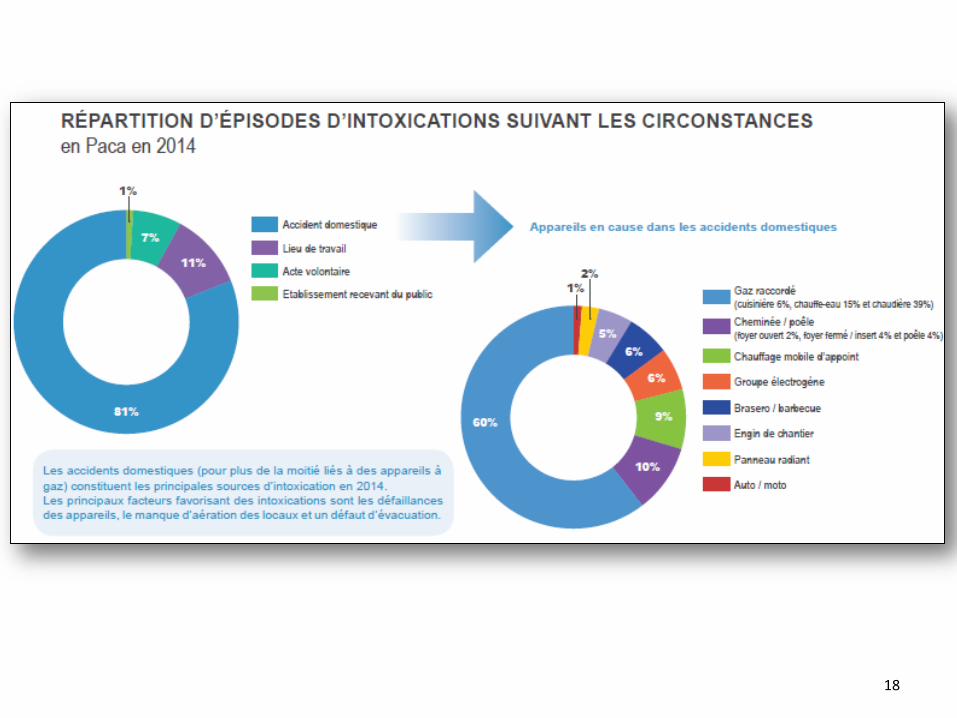
LEVEE DE DOUTE bull DOAGE
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
Dans le GAZ EXPIRE
bull Instantaneacute sur les lieux (triage +++)
bull HbCO calculeacutee en (80 ppm =10 HbCO)
bull Interfeacuterence possible (OH CO2 cyanure)
bull Difficile chez lrsquoenfant ou le patient inconscient
1 Ne pas hyperventiler
2 Une inspiration normale
3 Deacutebuter lrsquoexpiration
4 Bloquer
5 Terminer lrsquoexpiration dans le circuit de
mesure sans faire drsquoexpiration forceacutee
FAISABILITE
MODE DEGRADE
23
Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

Dans le SANG
bull Rapide
bull Invasif
bull Spectrophotomeacutetrie HbCO = hellip drsquoHb totale
bull Cineacutetique de dissociation du CO (laquo tube heacuteparineacute raquo techniqueacute lt 30rsquo)
REFERENCE
ACCESSIBILITE
24
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
NON INVASIF
NON
SpO2 peut ecirctre normale
26
NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

NON INVASIF
bull Pleacutethysmographie + Spectrophotomeacutetrie drsquoabsorption
bull HbCO = hellip drsquoHb totale [1 agrave 40]
bull En pratique
DOSAGE DELOCALISE
27
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
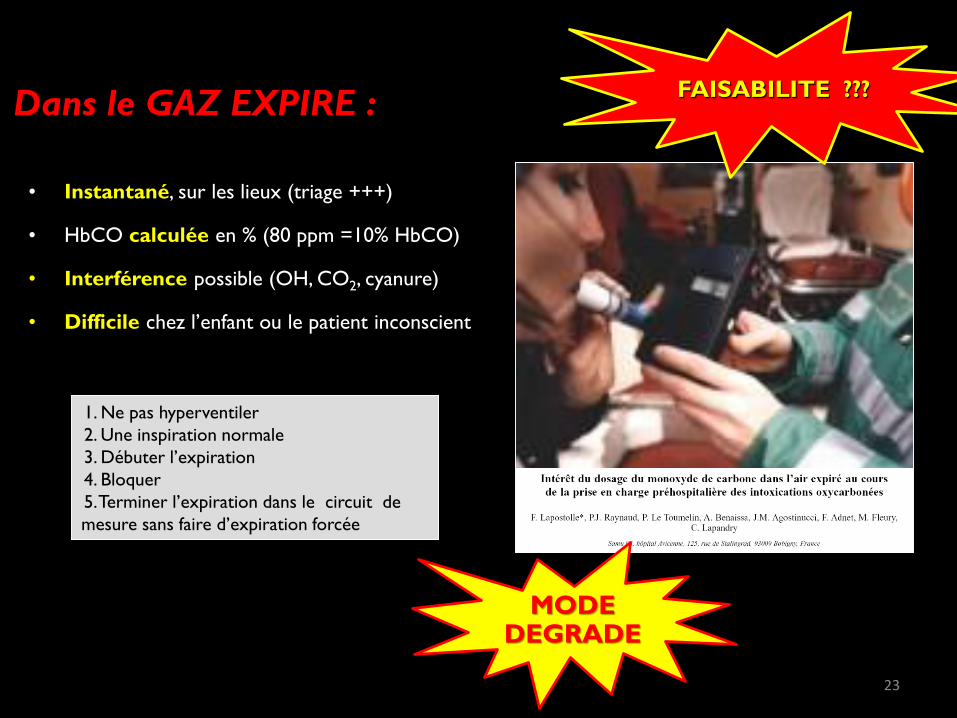
hellip et J Desola et al (n=58) M Sebbane et al (n=94) C Cazenave et al (n=86)
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
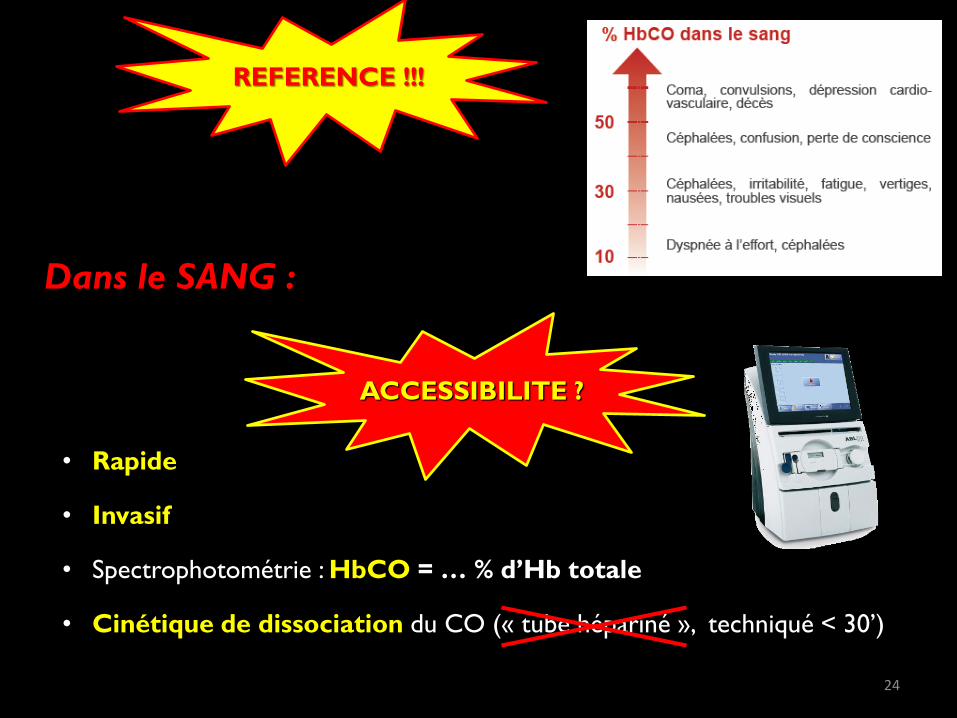
REGLES DE BONNE PRATIQUE
29
BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

BILAN
COMPLEMENTAIRE
TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

TRAITER
34
CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

CO
CO
CO
CO
O2
CO
CO
CaO2 =O2 O2
O2 O2O2
+
ONB
20 mL100mL
FiO2 = 100
DETOXIFICATION
12Hlaquo Demi vie de HbCO en ONB = 90 min raquo
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
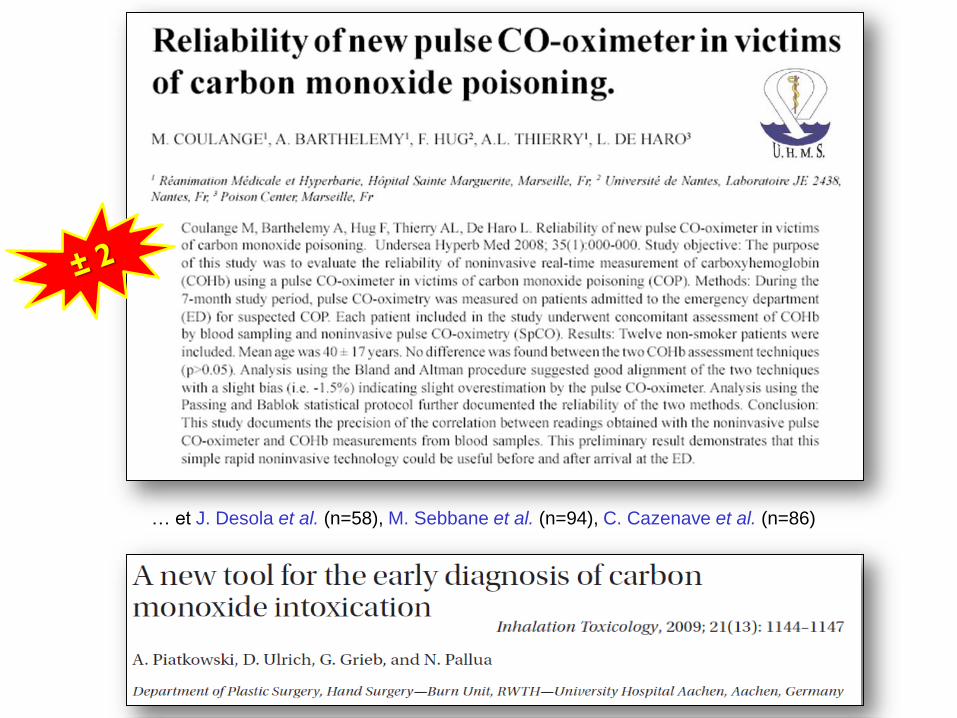
O2O2 O2
CO
CO
CO
CO
O2O2
O2 O2 O2
O2
O2
O2 O2 O2
CaO2 =O2 O2
O2 O2O2
+
6 mL100mL
SUFFISANT
OHB
EFFET
DE SUPPLEANCElaquo Suffisant pour garantir le meacutetabolisme
cellulaire raquo
100 x 25 b
20 mL100mL
DETOXIFICATION
2Hlaquo Demi vie de HbCO en ONB = 20 min raquo
X30
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
37
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
HbCO
Intox gt 24 h
gt 25
Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

Confeacuterence Europeacuteenne de Consensus 2004
1 Troubles de la conscience signes neuro cardiaques
respiratoires ou psychiques (haut risque) doivent beacuteneacuteficier
drsquoune OHB quel que soit le taux d rsquoHbCO type 1
2 Femme enceinte quels que soient les signes cliniques et le
taux d rsquoHbCO type 1
3 Intox mineures choix entre ONB pendant 12 heures vs OHB
dans l rsquoattente de reacutesultats d rsquoeacutetudes randomiseacutees type 3
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
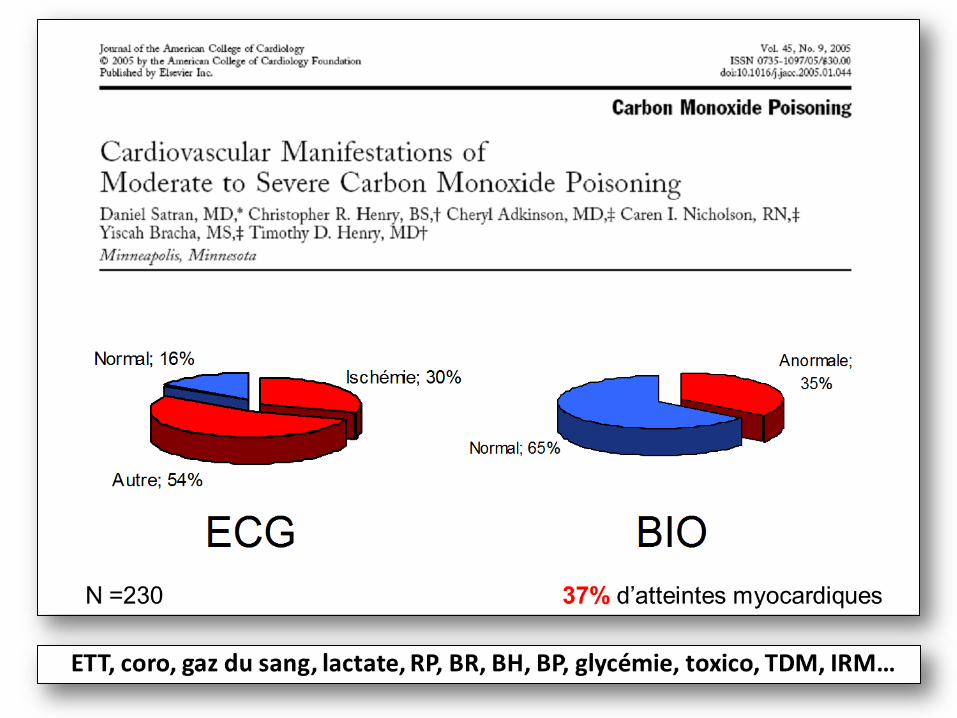
N= 1041 - 26 SAU ndash 2009 agrave 2010
M Coulange et al SFMU 2012
41
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
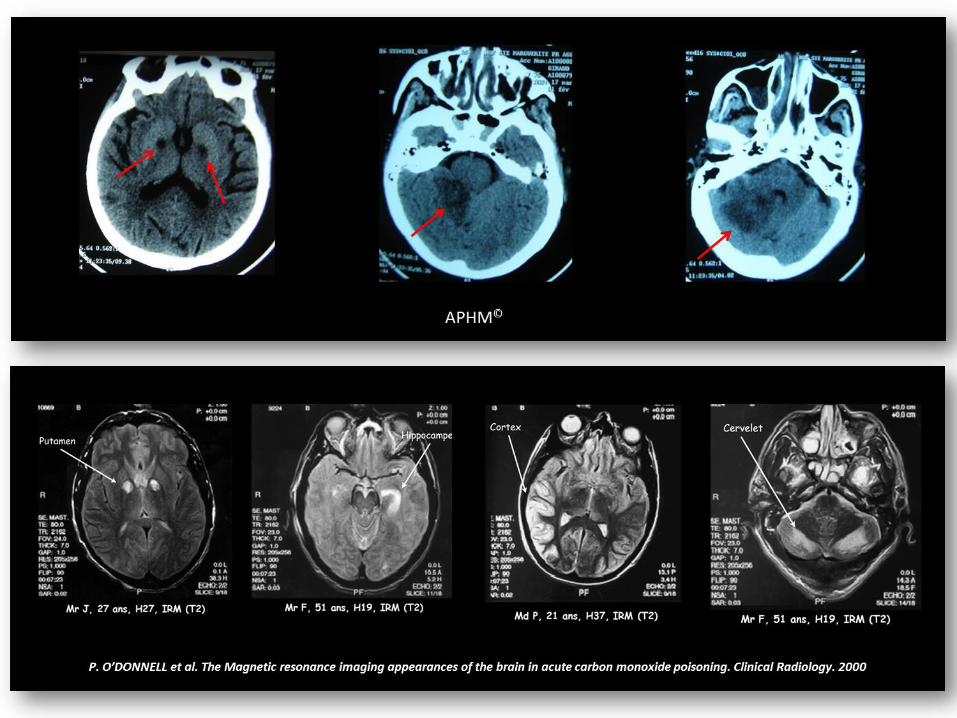
EXCLUSION DES CAS LES PLUS GRAVES
TRAITEMENTS HETEROGENES
SUIVI NEURO A TROP COURT TERME
ABSENCE DE SUIVI CARDIOLOGIQUE
43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

43
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
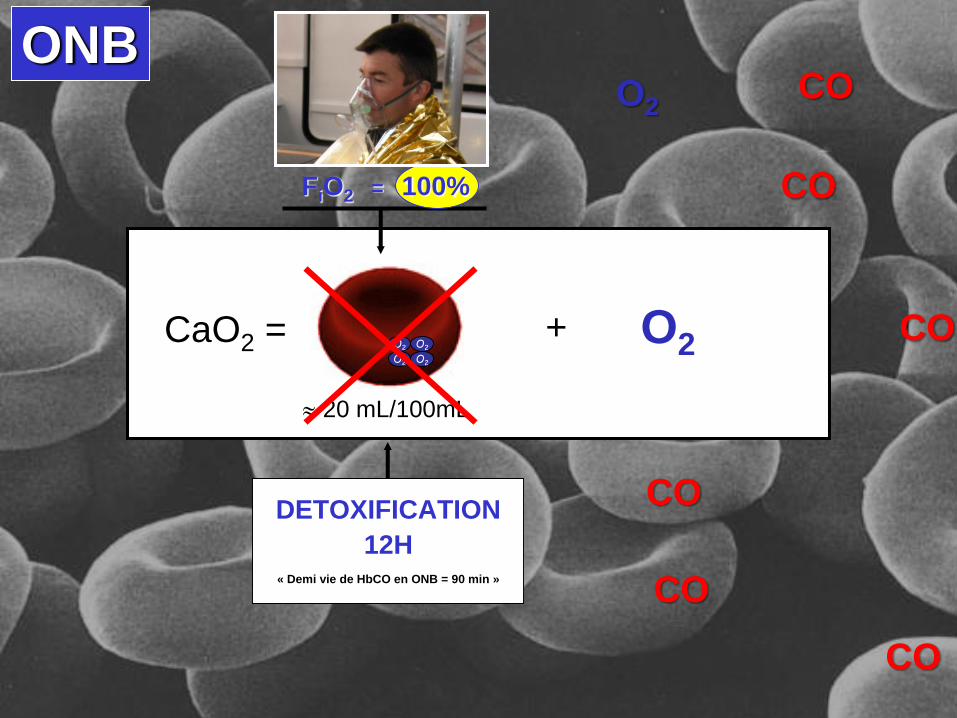
45
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
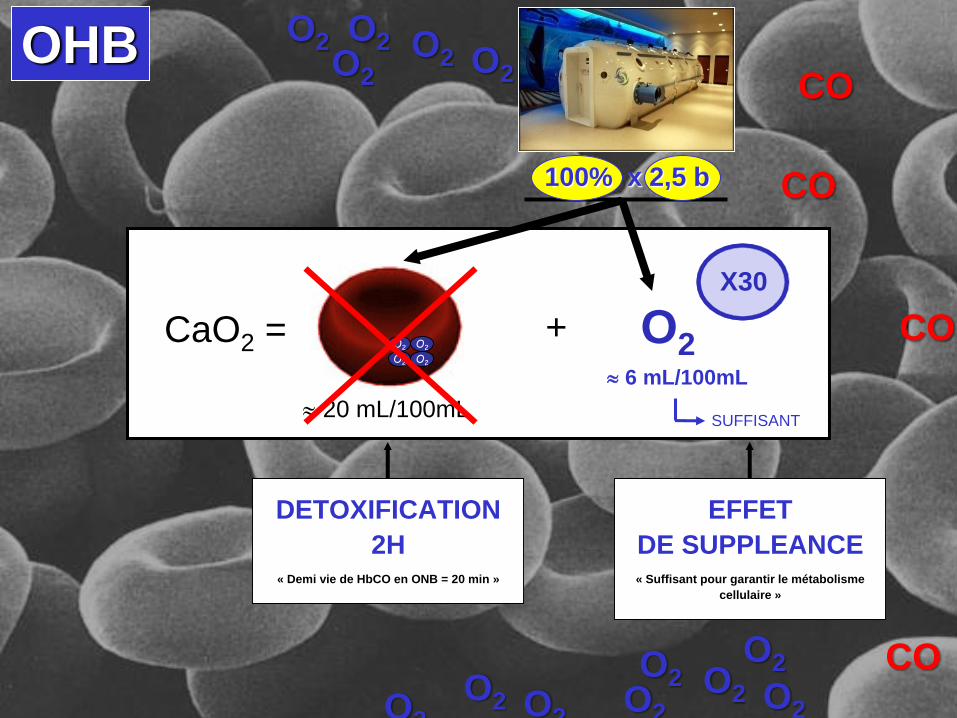
46
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
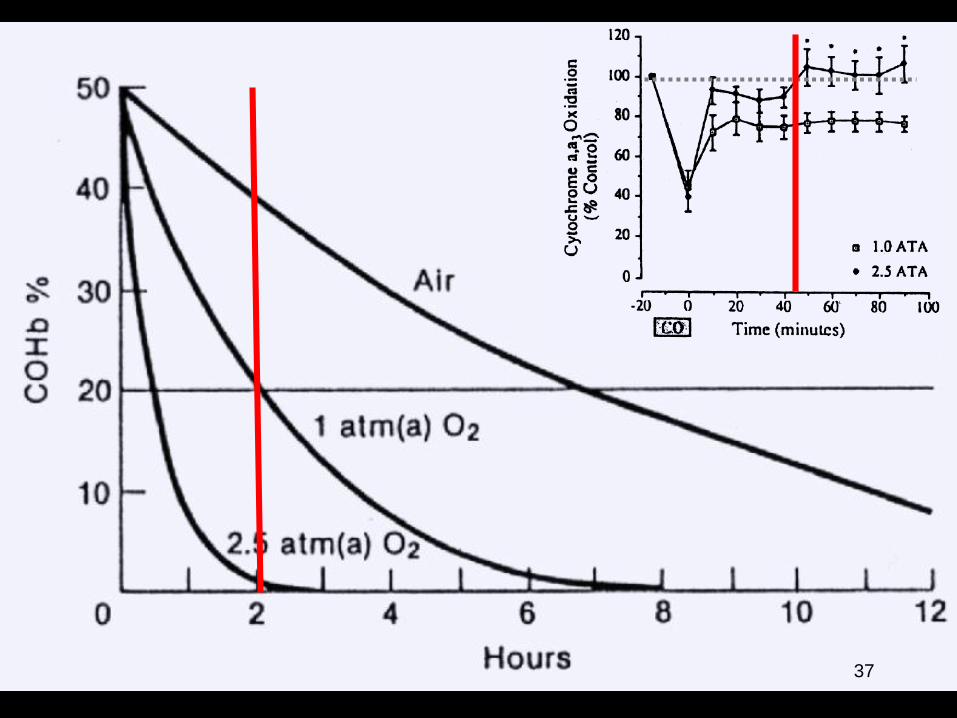
47
Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

Bull Acad Natl Med 2013 Mar197(3)677-94 discussion 695-7[A 25-year study (1983-2008) of childrens health outcomes after hyperbaric oxygen therapy for carbonmonoxidepoisoning in utero][Article in French]Wattel F Mathieu D Mathieu-Nolf MAbstractCarbon monoxide (CO) poisoning during pregnancy can be fatal for the fetus or cause bone malformations orencephalopathy depending on the stage of pregnancy at which the poisoning occurs Fewer cases of death andencephalopathy have been reported since the adoption of maternal hyperbaric oxygen (HBO) therapy in this settingbut these childrens long-term psychomotor development and growth remains to be documented A prospectivesingle-center cohort study spanning 25 years (1983 - 2008) included all pregnant women living in the Nord-Pas-de-Calais region of France who received HBO for CO poisoning and who gave birth to a living child A descriptive analysisof the women and children was performed first A control group of children was created by matching withanonymous files from local authorities The results of the childrens compulsory health amp development assessmentswere used to compare the two groups 406 women were included in the study of whom 6 were expecting twins Thepsychomotor development of 412 children was monitored up to the day 8 assessments in 388 cases the year 2assessments in 276 cases and the year 6 assessments in 232 cases Sixty children have not yet reached the age of 6years No significant differences in psychomotor or heightweight criteria (p gt 005 for both) were found between theexposed and unexposed children No malformations were reported These findings support the use of HBO therapyfor all expectant mothers exposed to CO poisoning No specific follow-up of the children is necessary if theirneonatal status is normal
48
Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

Intoxication CO ndash 050106
LES FUMEEShellip
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
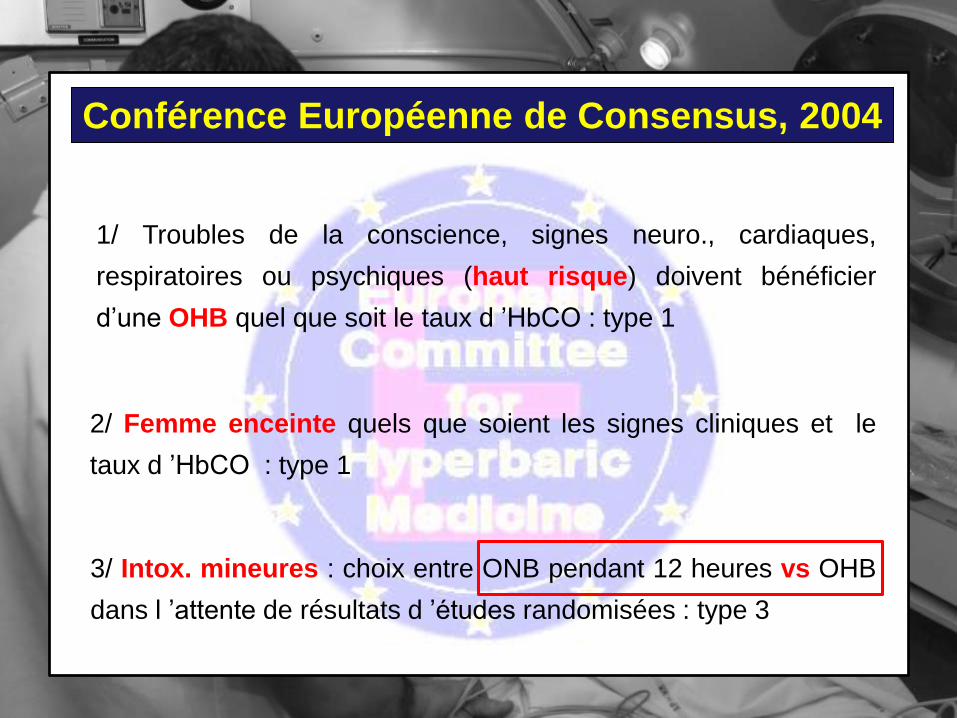
80 des deacutecegraves en relation avec lrsquoinhalation de fumeacutees
Birky et al 1981 Bull N Y Acad Med
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
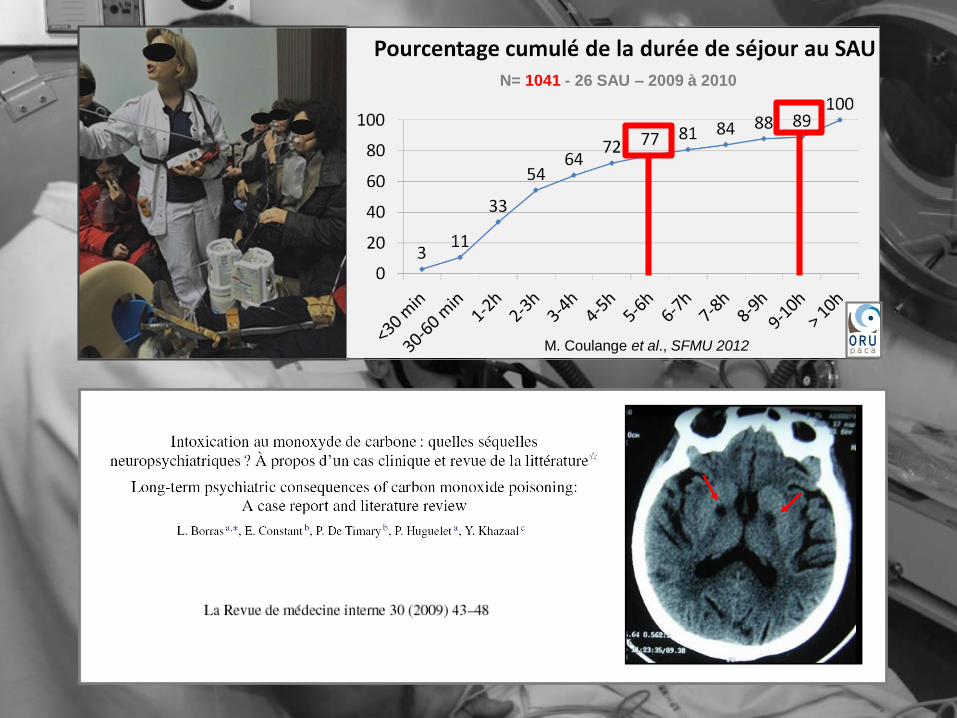
Intoxication CO ndash 050106
Purser DAThe evolution of toxic effluents in fires and the assessment of toxic hazardToxicol Lett 1992 Dec64-65 Spec No247-55
HCNCO
Meacutelange complexe et heacuteteacuterogegravene composeacute drsquoune phase gazeuse (composeacutee de plus de
150 moleacutecules) et drsquoune phase particulaire (suie et vapeur drsquoeau)
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ATTEINTE TOXIQUE
SYSTEMIQUE
SYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
53
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
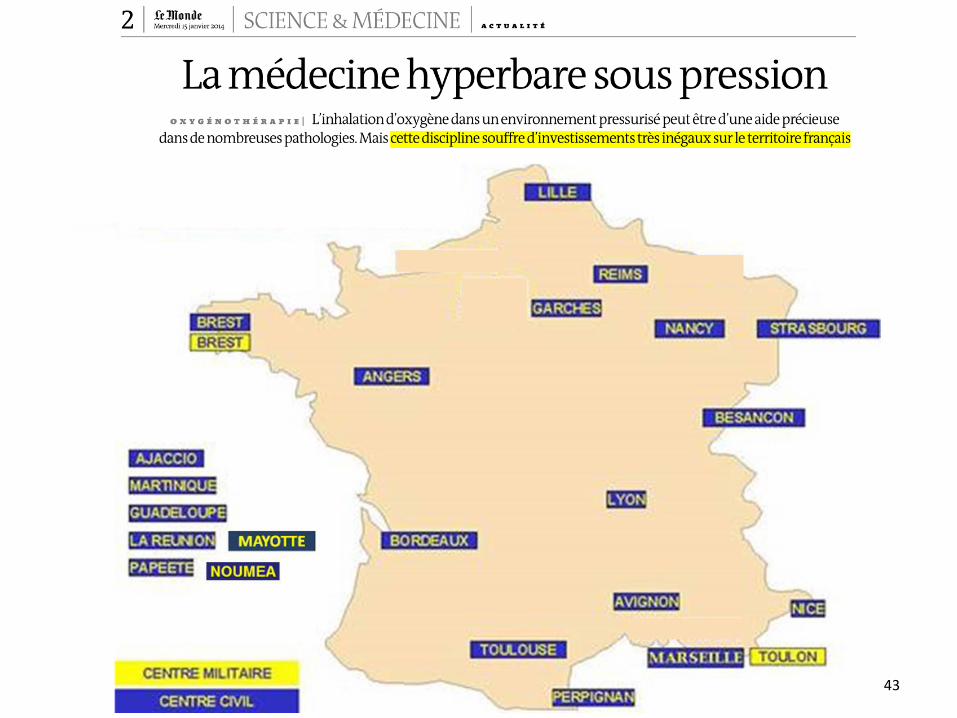
HCN
54
CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

CO
+90 min12 h
55
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
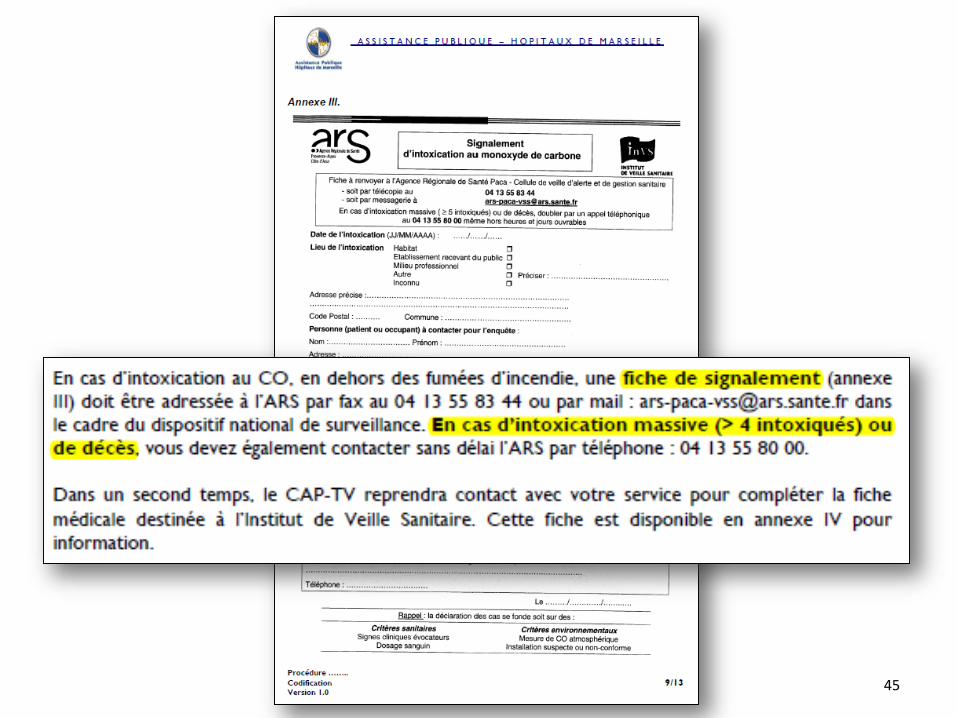
EN CONCLUSION
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
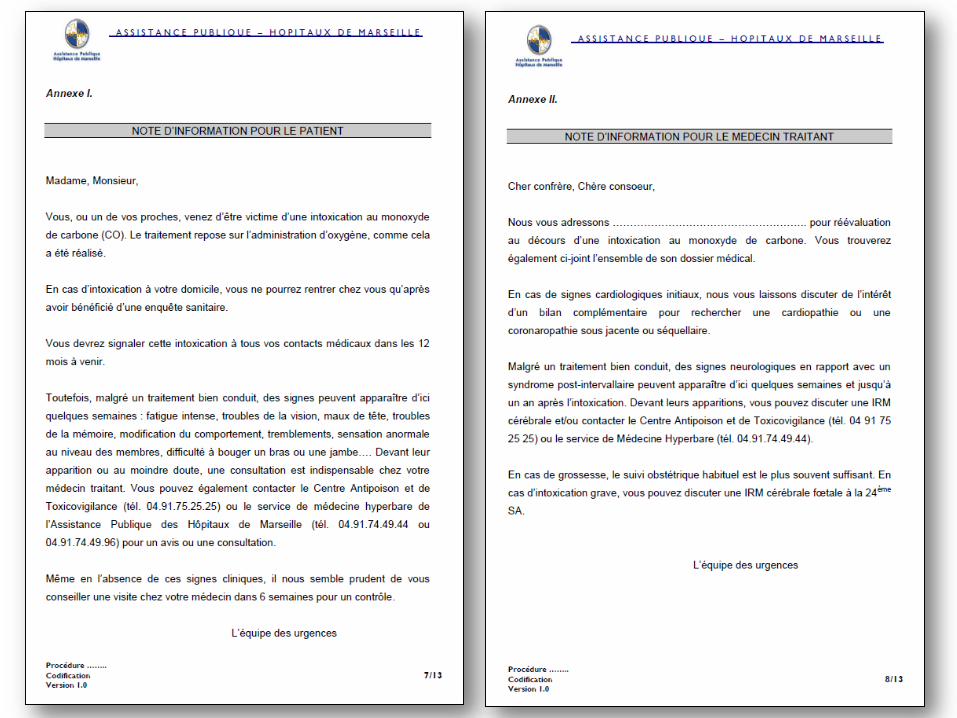
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
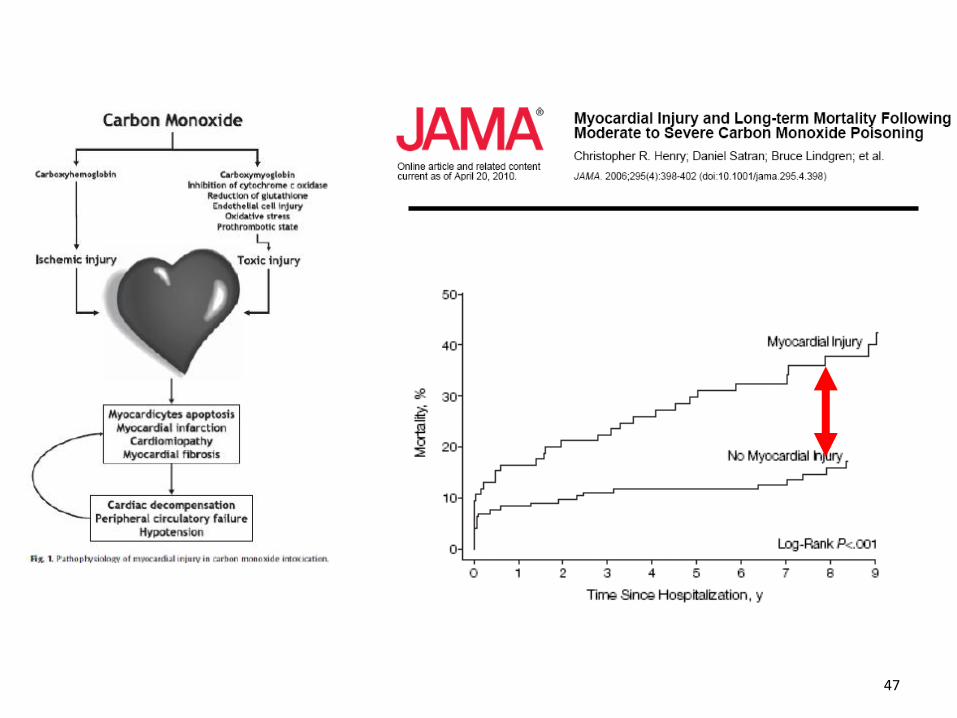
ANALYSE DE CAShellip
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
Intoxication CO ndash 050106
COMADIARRHEE
VOMISSEMENTASTHENIE
Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr

Intoxication CO ndash 05010661
PDC INITALE
COMA
CONVULSION
ENCEINTENAUSEE
ASTHENIE
ASTHENIE
DIARRHEE FA
VOMISSEMENT
CEPHALEE
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
Intoxication CO ndash 050106
ASTHENIE
ASTHENIE
DIARRHEE
VOMISSEMENT
CEPHALEE
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
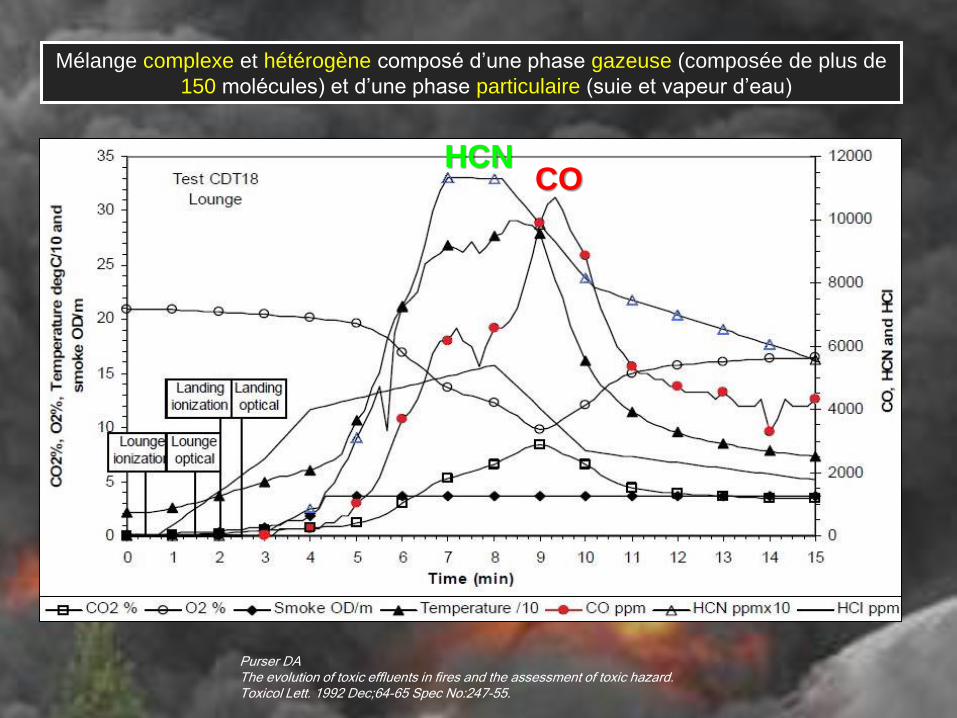
PROMPT SECOURS
bull Homme 53 ans HTA inconscient
bull CO atm = 200ppm exposeacute pd 3 h
bull Bilan
ndash G = 5 TA = 106 FC = 110 SpCO = 39
ndash Sd drsquoinhalation + heacutemodynamique preacutecaire
ndash ECG
SMUR
RDU
bull J1
ndash SDRA
ndash Adreacutenaline + Dobu
ndash lactates = 410 ( 89)
ndash ECG ischeacutemie (Troponine = 176 ( 66))
ndash Eacutecho FES = 25 (proBNP=152 ( 1500))
bull J2 OHB
bull J3 sevrage des amines
bull J5 Echo fonction VG Nl
bull J11 sevrage de la VM
bull J12 eacutetat neurologique correct
bull J15 sortie de reacuteanimation
bull Prise en charge
ndash IOT + VM (FiO2=100)
ndash Transfert OHB
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
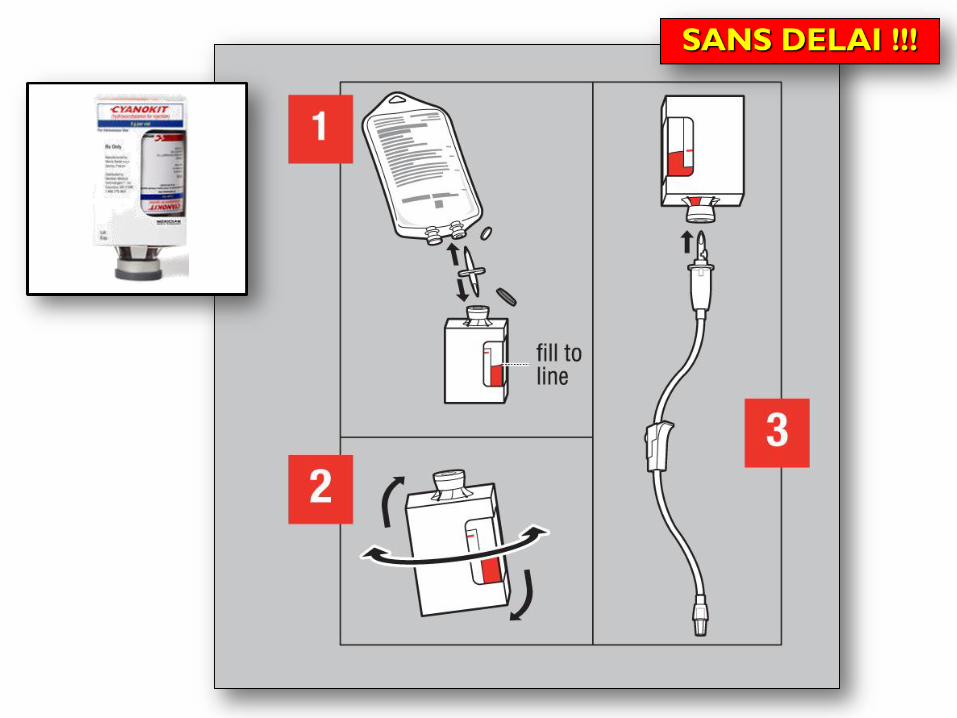
PROMPT SECOURS
bull Feu drsquohabitation
bull Homme 56 ans OH inconscient suies+++
bull Prise en charge
ndash 5 g hydroxocobalamine IV
ndash Transfert SAU pour OHB
bull Bilan
ndash G = 14 Fc = 139 TA = 1611
ndash SpO2=93 sous 10 Lmin O2
ndash SpCO=40 (CO expireacute = 106 ppm)
ndash ECG
SMUR
JL Fortincopy
SAU
bull Bilan
ndash G = 14 Fc = 96 TA=1710
ndash HbCO = 23
ndash Lactate = 942 mmolL
ndash ECG
bull Prise en charge amp Evolution
ndash 5 g hydroxocobalamine IV
ndash OHB gtgt ONB 12 h
ndash HbCO = 3
ndash Lactate = 28 mmolL
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr
DECHOCAGENonSpCO gt 5
(gt10 si fumeur)
Oui
Oui
Oui CYANOKIT sans deacutelai si fumeacutee
(lactate gt 8 mmolL)
Discuter lrsquoOHB en fonction de lrsquoaccessibiliteacute au centre hyperbare
du nb de victimes et de la capaciteacute agrave administrer de lrsquoONB pendant 12 h
Non
Diagnostic
diffeacuterentiel
plusmn Oui
Non
ONB pendant 12 heures
(FiO2 = 100 12 agrave 15 Lmin)
OuiSigne + HbCO gt 5
(gt10 si fumeur)
bull Arrecirct cardiaque
bull Signes neuro ou cardiorespiratoires
OXYGENOTHERAPIE NORMOBARE (ONB)
(FIO2=100 12 agrave 15 Lmin ou ventilation controcircleacutee)
Dosage HbCO par SpCO non invasive(agrave deacutefaut preacutelegravevement sanguin avec analyse rapide)
OXYGENOTHERAPIE HYPERBARE
Avis speacutecialiseacute preacutecoce
bull HbCO gt 25
bull Femme enceinte
Non
EXPOSITION CO
bull Contexte
bull Deacutetecteur CO atmospheacuterique
INCENDIE ampSYNDROME drsquoINHALATION
bull Espace clos
bull Signe neurologique
bull Brucirclures faciales etou Suies endocavitaires
- HbCO
-Tropo + ECG
- BHCG
- Avis speacutecialiseacute
- Suivi post urgence
mathieucoulangeap-hmfr