hémorragie digestive haute: indications, techniques...
TRANSCRIPT

Hémorragie digestive haute: Hémorragie digestive haute: indications, techniques et résultats de indications, techniques et résultats de
l’embolisation artériellel’embolisation artérielle
R Loffroy, P Rao, S Ota, M De Lin, BK Kwak,R Loffroy, P Rao, S Ota, M De Lin, BK Kwak,R Loffroy, P Rao, S Ota, M De Lin, BK Kwak,R Loffroy, P Rao, S Ota, M De Lin, BK Kwak,JF GeschwindJF Geschwind
The Russell H. Morgan Department of Radiology andThe Russell H. Morgan Department of Radiology andRadiological Science, Radiological Science,
Division of Vascular and Interventional Radiology, Division of Vascular and Interventional Radiology, The Johns Hopkins Hospital, The Johns Hopkins Hospital,
Baltimore, Maryland, USABaltimore, Maryland, USA
TT

Acute upper GI bleedingAcute upper GI bleeding
•• Endoscopic hemostasis: 85Endoscopic hemostasis: 85--90%90%
•• Unmanageable: 10Unmanageable: 10--15%15%•• Unmanageable: 10Unmanageable: 10--15%15%
-- Surgical rescueSurgical rescue
-- Endovascular rescueEndovascular rescue
No change over the past 2 decadesNo change over the past 2 decades
Evidence based medicineEvidence based medicine
•• Integration of:Integration of:
-- Individual clinical expertiseIndividual clinical expertise
-- Patients values and expectationsPatients values and expectations
-- Best available external evidenceBest available external evidence
Sackett DL et al. BMJ 1996;312:71Sackett DL et al. BMJ 1996;312:71--22
Literature reviewLiterature review
•• From 1990 to 2009From 1990 to 2009•• Pubmed queriesPubmed queries•• Keyword search:Keyword search:
-- «« upper gastrointestinalupper gastrointestinal » or «» or « gastroduodenal ulcergastroduodenal ulcer »»-- «« upper gastrointestinalupper gastrointestinal » or «» or « gastroduodenal ulcergastroduodenal ulcer »»-- and «and « bleedingbleeding » or «» or « hemorrhagehemorrhage »»-- and «and « embolizationembolization » or «» or « embolotherapyembolotherapy »»
•• English literatureEnglish literature•• Exclude portal hypertension, mixed series, case Exclude portal hypertension, mixed series, case
reports and series < 15 patientsreports and series < 15 patients
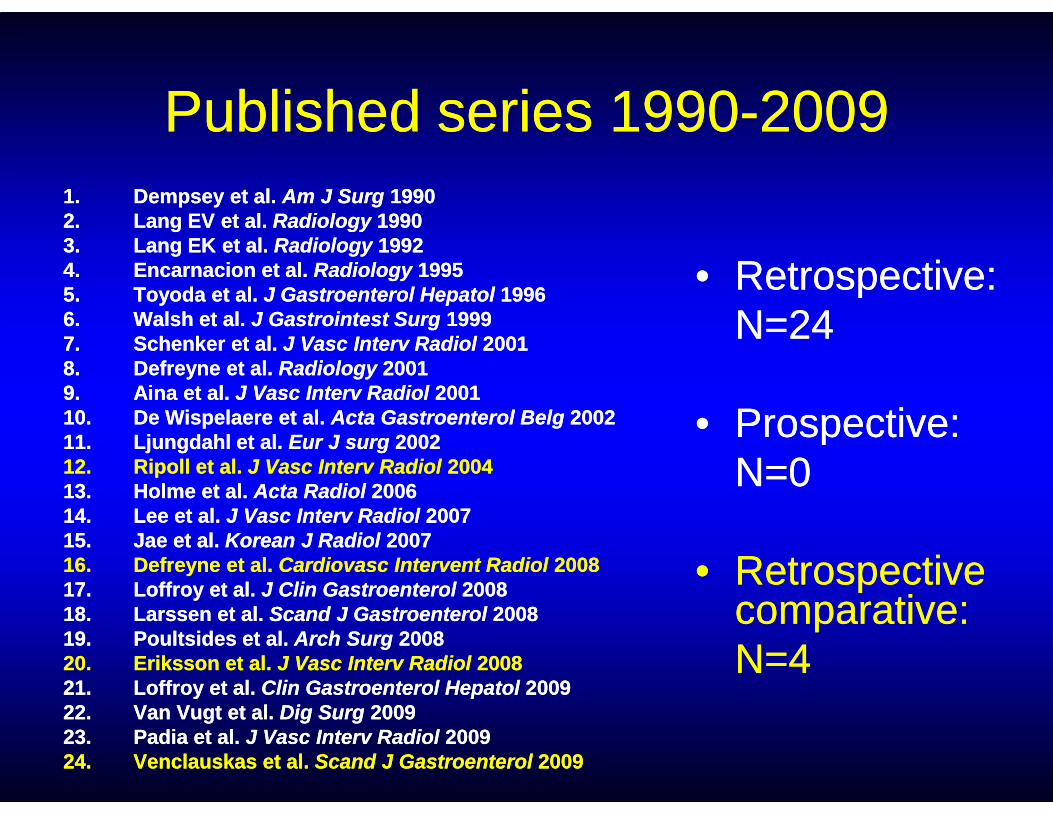
Published series 1990Published series 1990--200920091.1. Dempsey et al. Dempsey et al. Am J SurgAm J Surg 199019902.2. Lang EV et al. Lang EV et al. Radiology Radiology 199019903.3. Lang EK et al. Lang EK et al. Radiology Radiology 199219924.4. Encarnacion et al. Encarnacion et al. RadiologyRadiology 199519955.5. Toyoda et al. Toyoda et al. J Gastroenterol HepatolJ Gastroenterol Hepatol 199619966.6. Walsh et al. Walsh et al. J Gastrointest SurgJ Gastrointest Surg 199919997.7. Schenker et al. Schenker et al. J Vasc Interv RadiolJ Vasc Interv Radiol 200120018.8. Defreyne et al. Defreyne et al. Radiology Radiology 200120019.9. Aina et al. Aina et al. J Vasc Interv RadiolJ Vasc Interv Radiol 2001200110.10. De Wispelaere et al. De Wispelaere et al. Acta Gastroenterol BelgActa Gastroenterol Belg 20022002
•• Retrospective: Retrospective: N=24N=24
•• Prospective: Prospective: 10.10. De Wispelaere et al. De Wispelaere et al. Acta Gastroenterol BelgActa Gastroenterol Belg 2002200211.11. Ljungdahl et al. Ljungdahl et al. Eur J surgEur J surg 2002200212.12. Ripoll et al. Ripoll et al. J Vasc Interv RadiolJ Vasc Interv Radiol 2004200413.13. Holme et al. Holme et al. Acta RadiolActa Radiol 2006200614.14. Lee et al. Lee et al. J Vasc Interv RadiolJ Vasc Interv Radiol 2007200715.15. Jae et al. Jae et al. Korean J RadiolKorean J Radiol 2007200716.16. Defreyne et al. Defreyne et al. Cardiovasc Intervent RadiolCardiovasc Intervent Radiol 2008200817.17. Loffroy et al. Loffroy et al. J Clin GastroenterolJ Clin Gastroenterol 2008200818.18. Larssen et al. Larssen et al. Scand J GastroenterolScand J Gastroenterol 2008200819.19. Poultsides et al. Poultsides et al. Arch SurgArch Surg 2008200820.20. Eriksson et al. Eriksson et al. J Vasc Interv RadiolJ Vasc Interv Radiol 2008200821.21. Loffroy et al. Loffroy et al. Clin Gastroenterol HepatolClin Gastroenterol Hepatol 2009200922.22. Van Vugt et al. Van Vugt et al. Dig SurgDig Surg 2009200923.23. Padia et al. Padia et al. J Vasc Interv RadiolJ Vasc Interv Radiol 2009200924.24. Venclauskas et al. Venclauskas et al. Scand J GastroenterolScand J Gastroenterol 20092009
•• Prospective: Prospective: N=0N=0
•• Retrospective Retrospective comparative: comparative: N=4N=4
Outcome endpointsOutcome endpoints
•• Technical successTechnical success
•• Primary and secondary clinical success Primary and secondary clinical success within within 30 30 daysdayswithin within 30 30 daysdays
•• PeriPeri--procedural complicationsprocedural complications
•• 3030--day or inday or in--hospital mortalityhospital mortality
•• LongLong--term followterm follow--up up

Indications
• Peptic gastroduodenal ulcers: 50%• Other: 50%- Mallory-Weiss tears- Vascular ectasias- Dieulafoy’s lesions- Neoplasms- Iatrogenic: AI, AC, surgery, biopsy
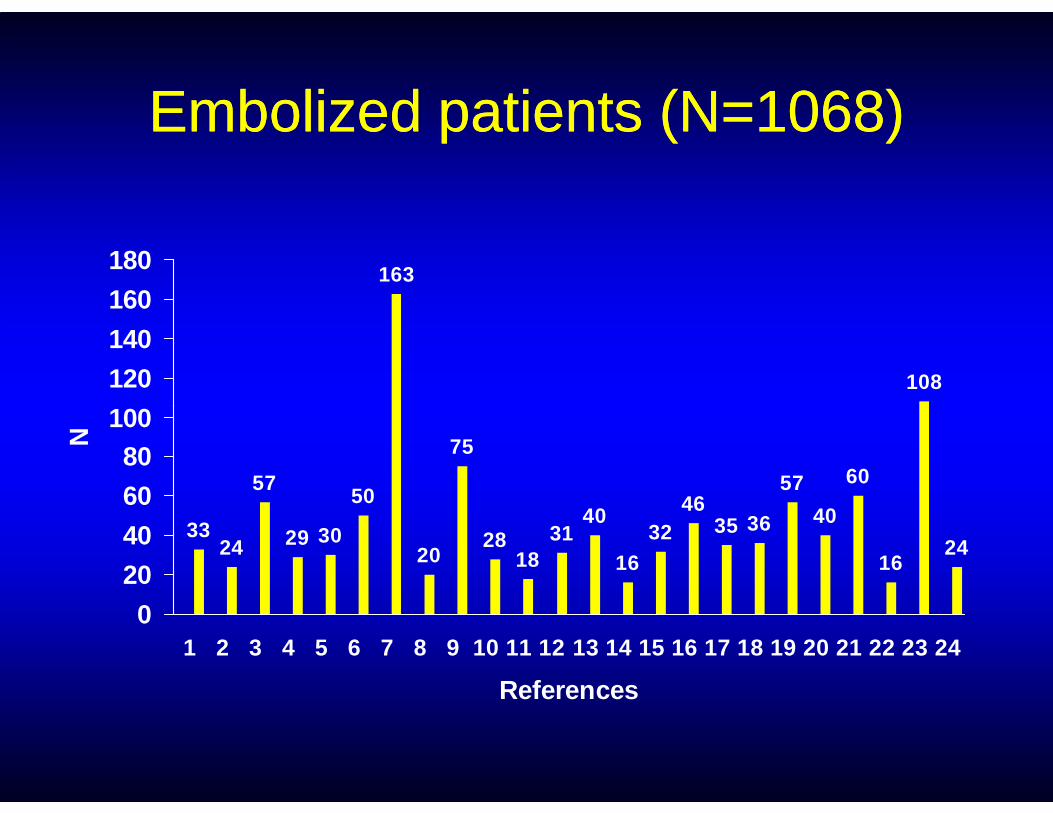
Embolized patients (N=Embolized patients (N=10681068))
163
108
100
120
140
160
180
3324
57
29 30
50
20
75
2818
3140
1632
4635 36
57
40
60
1624
0
20
40
60
80100
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
References
N
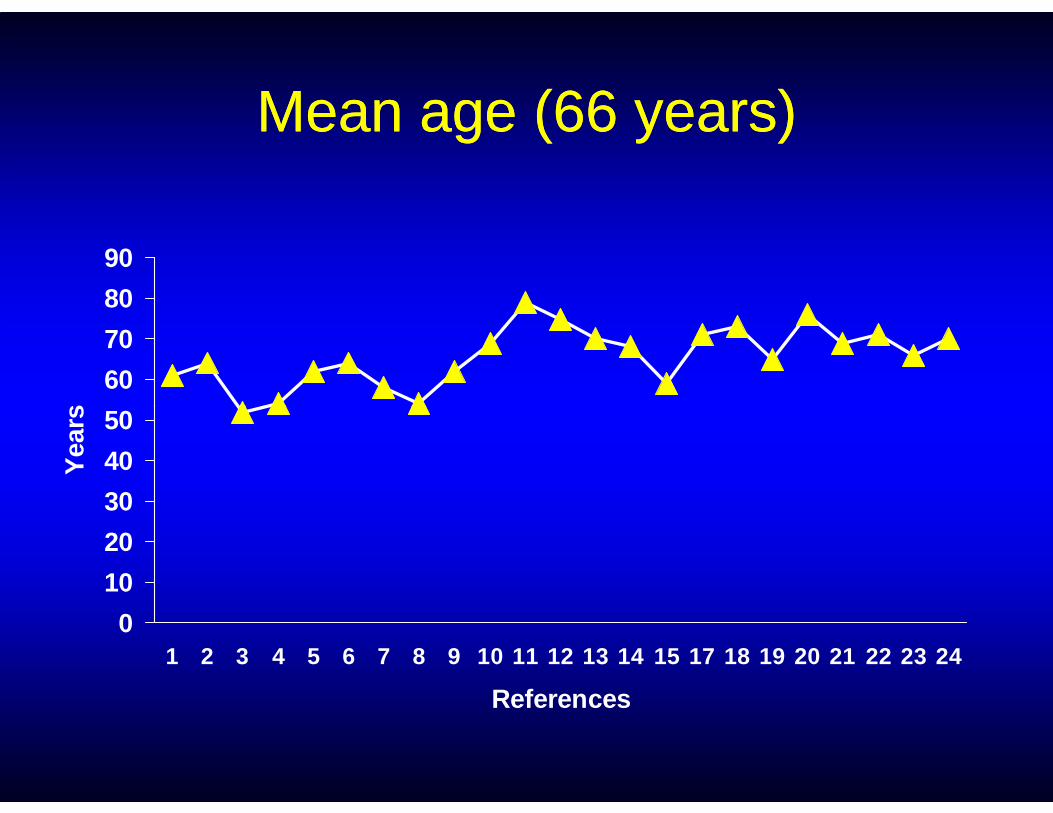
Mean age (66 years)Mean age (66 years)
50
60
70
80
90
rs
0
10
20
30
40
50
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 17 18 19 20 21 22 23 24
References
Yea
rs

Technical success (94%)Technical success (94%)
60
80
100
%
0
20
40
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 24
References
%
Success Failure
Causes for technique failureCauses for technique failure
•• Vascular anatomyVascular anatomy•• VasospasmVasospasm•• Arterial dissectionArterial dissection•• Arterial dissectionArterial dissection•• False negatively read angiogramFalse negatively read angiogram•• Multiple bleedings (coagulopathy)Multiple bleedings (coagulopathy)•• Tumorous bleedingTumorous bleeding
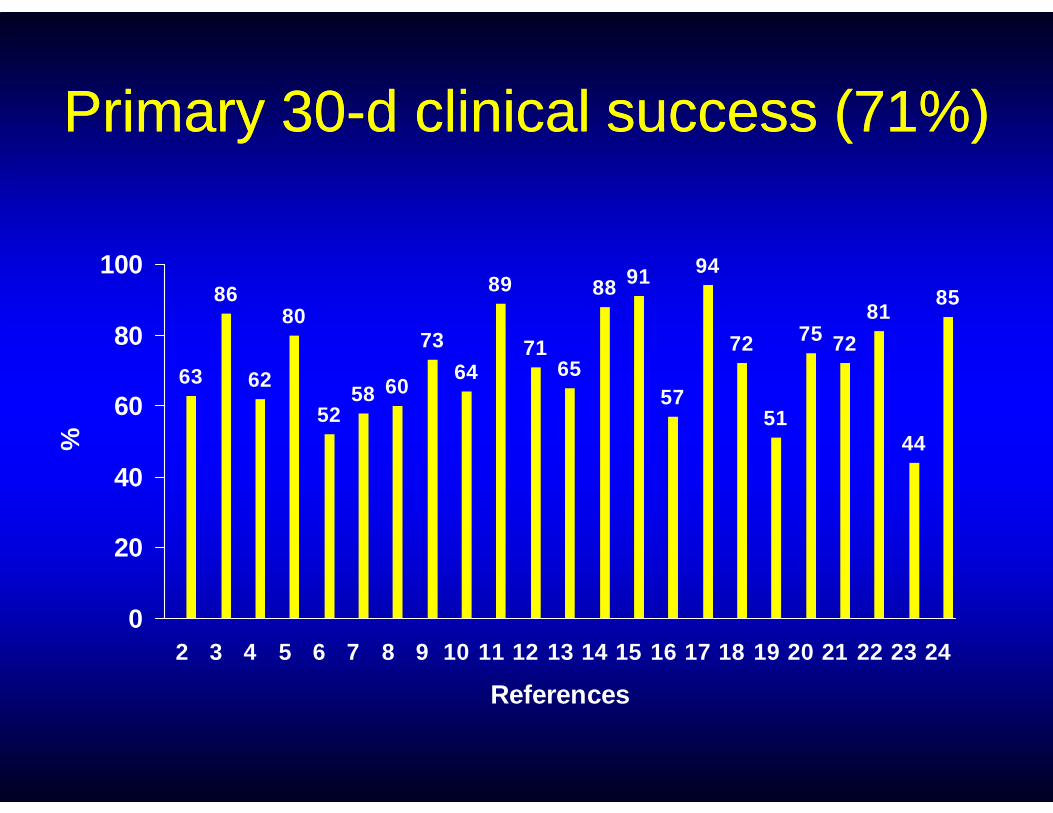
Primary 30Primary 30--d clinical success (71%)d clinical success (71%)
63
86
62
80
5258 60
73
64
89
7165
88 91
57
94
72
51
75 72
8185
60
80
100
5257
5144
0
20
40
60
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
References
%
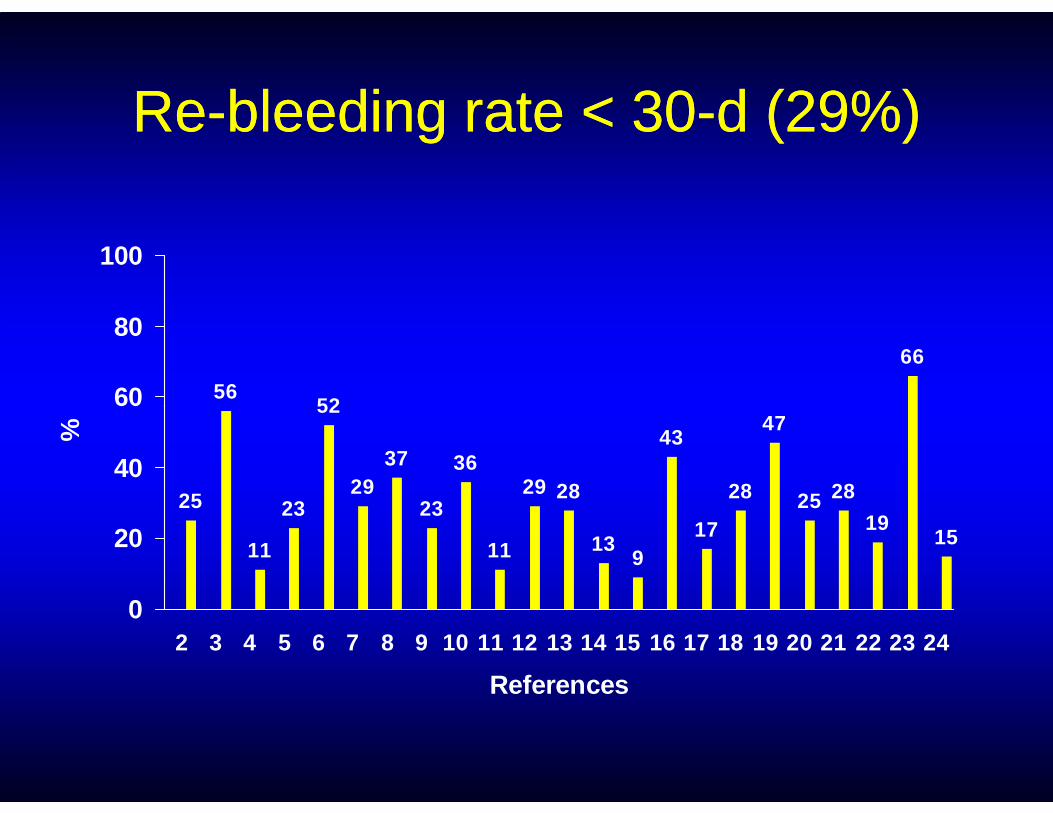
ReRe--bleeding rate < 30bleeding rate < 30--d (29%)d (29%)
5652
66
60
80
100
25
11
23
52
2937
23
36
11
29 28
139
43
17
28
47
25 28
1915
0
20
40
60
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
References
%

Secondary 30Secondary 30--d clinical success (92%)d clinical success (92%)
60
80
100
%
0
20
40
3 5 6 8 9 10 11 12 13 14 15 17 19 20 21 22 23 24
References
%
Success Failure
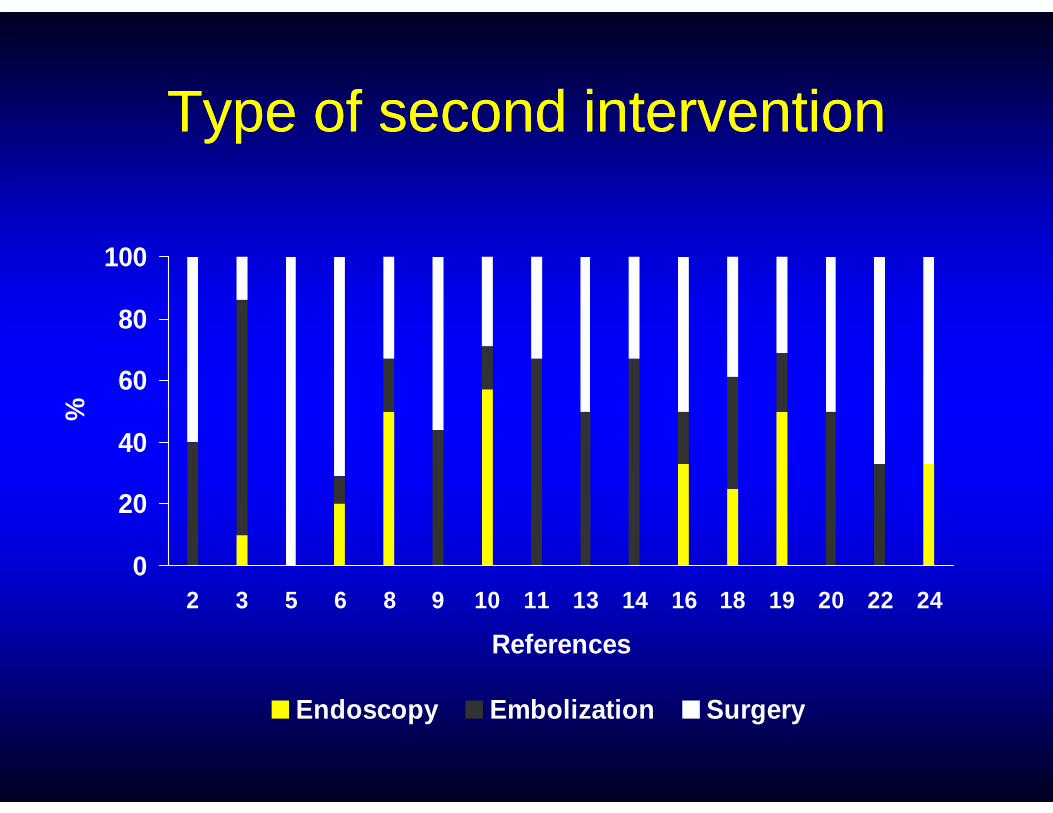
Type of second interventionType of second intervention
60
80
100
%
0
20
40
2 3 5 6 8 9 10 11 13 14 16 18 19 20 22 24
References
%
Endoscopy Embolization Surgery
Attempted hemostatic reAttempted hemostatic re--interventionintervention
•• For reFor re--bleeding patients or continuing bleeding patients or continuing bleeding patients:bleeding patients:
-- Endoscopic treatment Endoscopic treatment 1717%%-- Endoscopic treatment Endoscopic treatment ≈ ≈ 1717%%
-- ReRe--embolization embolization ≈ ≈ 3434%%
-- Surgery Surgery ≈ ≈ 4949%%
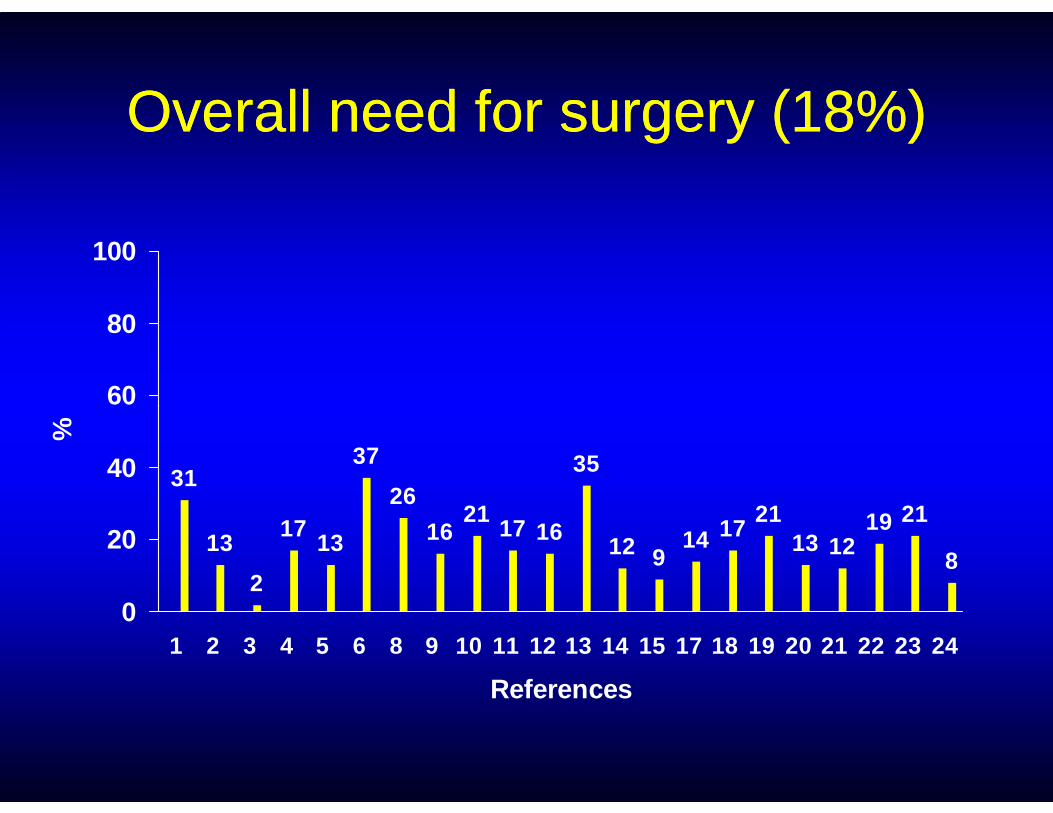
Overall need for surgery (Overall need for surgery (1818%)%)
60
80
100
31
13
2
1713
37
26
1621
17 16
35
12 914 17
2113 12
19 21
8
0
20
40
60
1 2 3 4 5 6 8 9 10 11 12 13 14 15 17 18 19 20 21 22 23 24
References
%
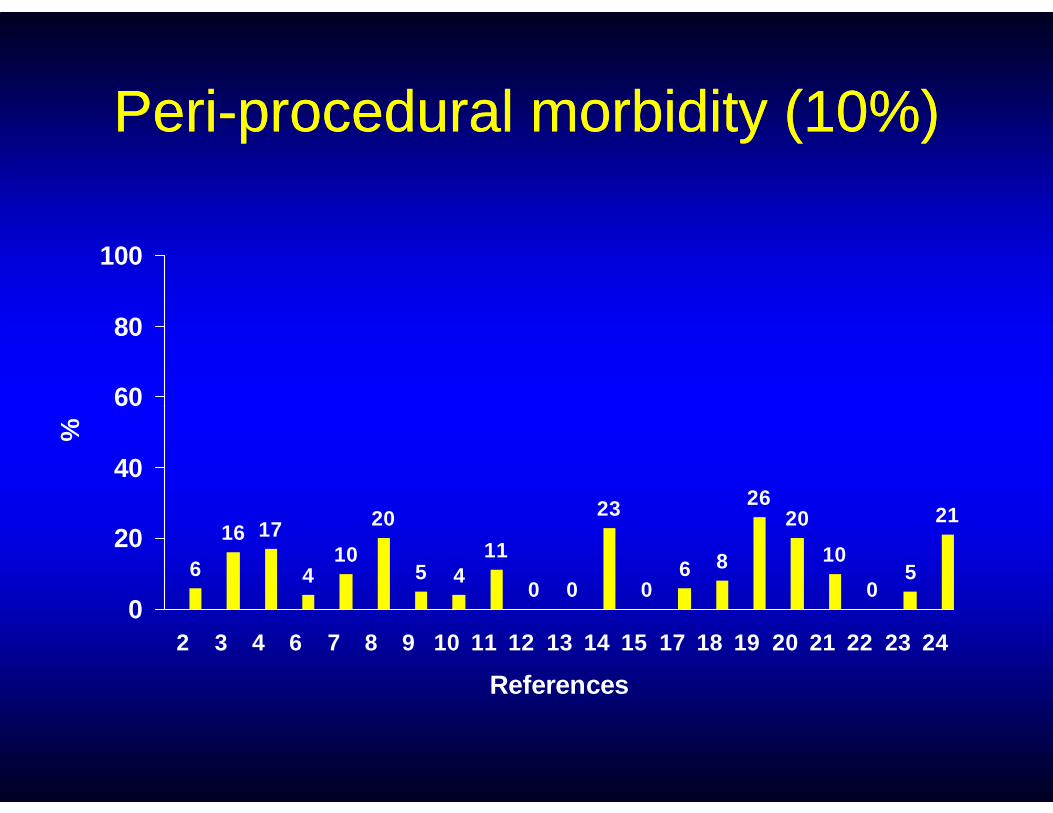
PeriPeri--procedural morbidity (10%)procedural morbidity (10%)
60
80
100
6
16 17
410
20
5 411
0 0
23
06 8
2620
10
05
21
0
20
40
60
2 3 4 6 7 8 9 10 11 12 13 14 15 17 18 19 20 21 22 23 24
References
%
Types of complicationsTypes of complications
•• Related to underlying conditions: +++Related to underlying conditions: +++
-- Advanced age and coAdvanced age and co--morbiditiesmorbidities
•• Related to the procedure:Related to the procedure:
-- Technical complications without clinicalTechnical complications without clinicalconsequencesconsequences
-- Risk of acute ischemic complications < 5%Risk of acute ischemic complications < 5%
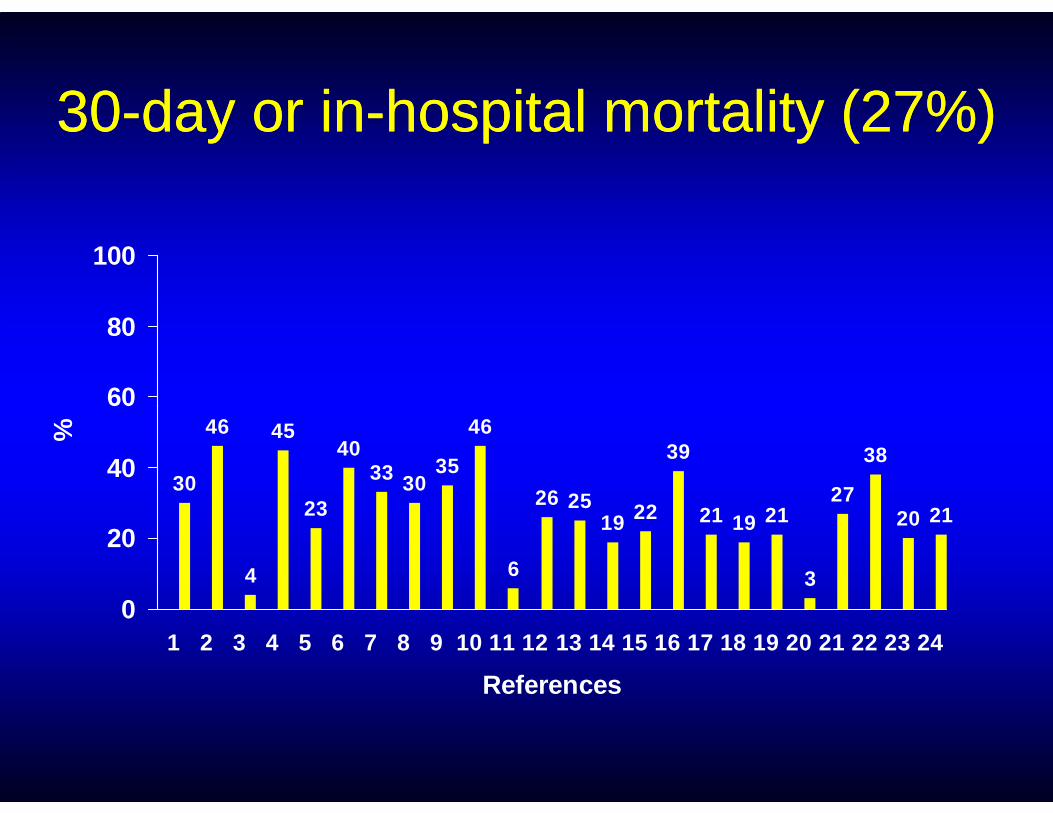
3030--day or inday or in--hospital mortality (27%)hospital mortality (27%)
60
80
100
30
46
4
45
23
4033 30
35
46
6
26 2519 22
39
21 19 21
3
27
38
20 21
0
20
40
60
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
References
%
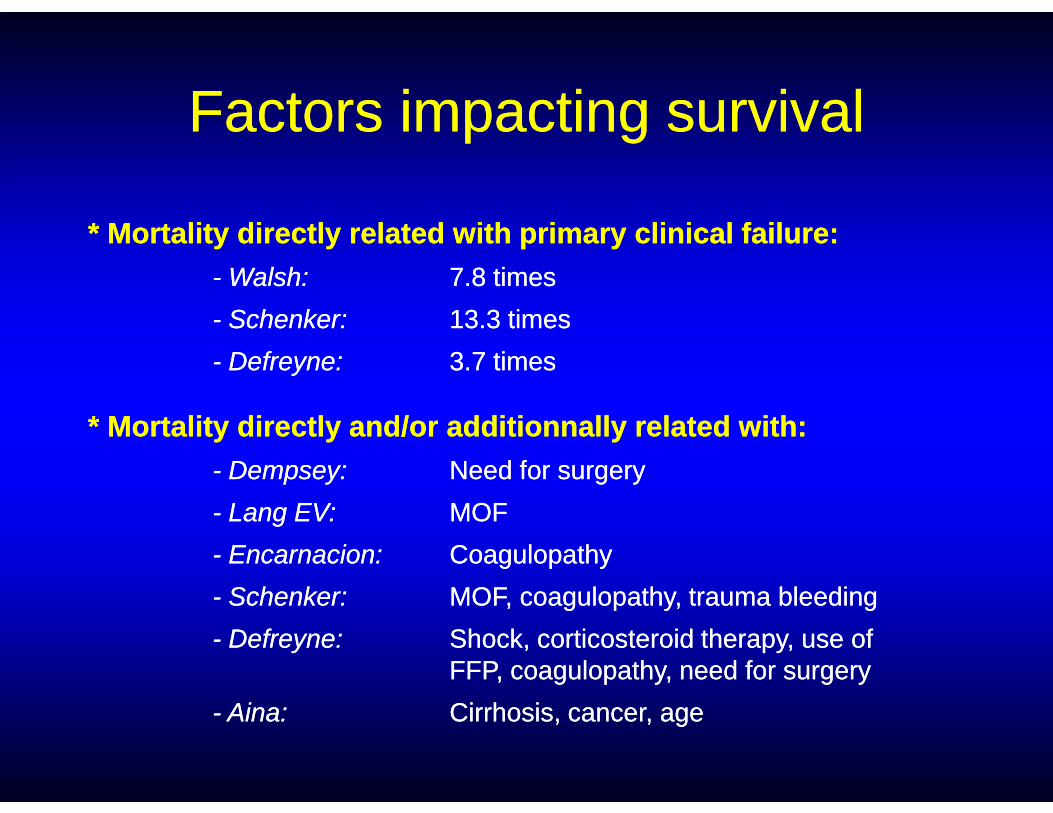
FactorsFactors impactingimpacting survivalsurvival
* Mortality directly related with primary clinical failure:* Mortality directly related with primary clinical failure:-- Walsh:Walsh: 7.8 times7.8 times
-- Schenker:Schenker: 13.3 times13.3 times
-- Defreyne:Defreyne: 3.7 times3.7 times
* Mortality directly and/or additionnally related with:* Mortality directly and/or additionnally related with:-- Dempsey:Dempsey: Need for surgeryNeed for surgery
-- Lang EV:Lang EV: MOFMOF
-- Encarnacion:Encarnacion: CoagulopathyCoagulopathy
-- Schenker:Schenker: MOF, coagulopathy, trauma bleedingMOF, coagulopathy, trauma bleeding
-- Defreyne:Defreyne: Shock, corticosteroid therapy, use of Shock, corticosteroid therapy, use of FFP, coagulopathy, need for surgery FFP, coagulopathy, need for surgery
-- Aina:Aina: Cirrhosis, cancer, ageCirrhosis, cancer, age
LongLong--termterm followfollow--upup
•• One study:One study:
-- Lang EK. RadiologyLang EK. Radiology19921992;;182182::703703--77
-- Late reLate re--bleeding rate: bleeding rate: 5656%%
•• Need for:Need for:
-- Systematic endoscopicSystematic endoscopiccontrolcontrol
-- Aggressive longAggressive long--termterm-- Late reLate re--bleeding rate: bleeding rate: 5656%%((33mm--77y)y)
-- Duodenal stenosis: Duodenal stenosis: 2525%%-- GDA embolizationGDA embolization-- Glue +++Glue +++
-- Aggressive longAggressive long--termtermrisk factor modificationrisk factor modification
-- Treatment for theTreatment for theunderlying peptic ulcerunderlying peptic ulcerdiseasedisease

OverallOverall
•• EvenEven if if externalexternal evidenceevidence sufferssuffers fromfrominconsistentinconsistent resultsresults ((heterogeneityheterogeneity++++):):
-- EmbolizationEmbolization isis safesafe and and efficacyefficacy for thefor thetreatmenttreatment of acute of acute upperupper GI GI bleedingbleedingtreatmenttreatment of acute of acute upperupper GI GI bleedingbleeding
-- ShouldShould bebe consideredconsidered the gold standard the gold standard for for endoscopyendoscopy--refractoryrefractory patientspatients
-- WeWe cancan maximizemaximize resultsresults and and minimizeminimizerecurrentrecurrent bleedingbleeding
(Loffroy et al. (Loffroy et al. CardiovascCardiovasc InterventIntervent RadiolRadiol 2010; In 2010; In PressPress))
How maximize results and How maximize results and minimize recurrent bleeding ?minimize recurrent bleeding ?
1. Post1. Post--endoscopy decision making: reendoscopy decision making: re--endoscopy, embolization or surgery ?endoscopy, embolization or surgery ?
2. Take into account the known factors2. Take into account the known factorsaffecting clinical success ?affecting clinical success ?
3. Other Tips ?3. Other Tips ?
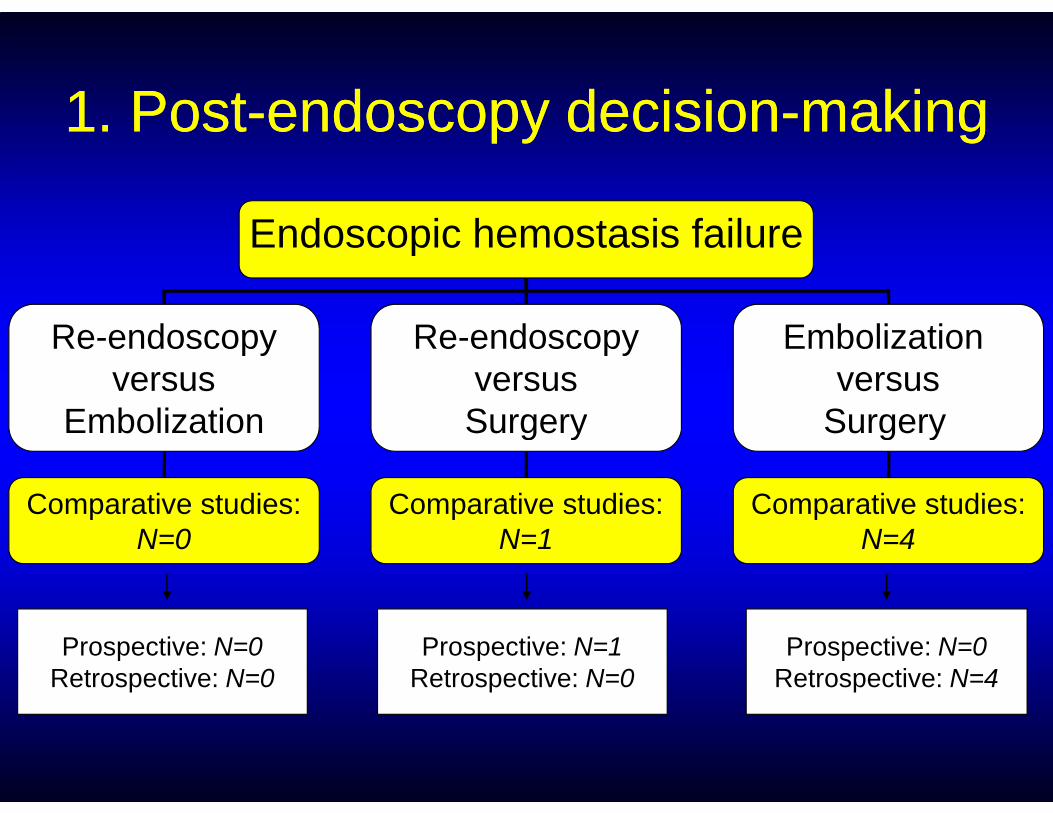
1. Post1. Post--endoscopy decisionendoscopy decision--makingmaking
Endoscopic hemostasis failure
Re-endoscopyversus
Embolization
Re-endoscopyversusSurgery
Embolization versus
SurgeryEmbolization Surgery Surgery
Comparative studies:N=0
Comparative studies:N=1
Comparative studies:N=4
Prospective: N=0Retrospective: N=0
Prospective: N=1Retrospective: N=0
Prospective: N=0Retrospective: N=4

ReRe--endoscopy versus surgeryendoscopy versus surgery
Conclusion:Conclusion:
In patients with peptic ulcers and recurrent bleeding afterIn patients with peptic ulcers and recurrent bleeding afterinitial endoscopic control of bleeding, endoscopic initial endoscopic control of bleeding, endoscopic retreatment reduces the need for surgery without retreatment reduces the need for surgery without
increasing the risk of death and is associated with fewerincreasing the risk of death and is associated with fewercomplications than surgery complications than surgery
((N Engl J Med 1999;340:751N Engl J Med 1999;340:751--66))
Embolization versus surgeryEmbolization versus surgery
•• No prospective randomized studyNo prospective randomized study
•• 4 retrospective comparative studies:4 retrospective comparative studies:
-- Ripoll et al. Ripoll et al. J Vasc Interv RadiolJ Vasc Interv Radiol 2004 2004 (31 vs. 39)(31 vs. 39)
-- Defreyne et al. Defreyne et al. Cardiovasc Intervent RadiolCardiovasc Intervent Radiol 2008 2008 (46 vs. 51)(46 vs. 51)
-- Eriksson et al. Eriksson et al. J Vasc Interv RadiolJ Vasc Interv Radiol 2008 2008 (40 vs. 51)(40 vs. 51)
-- Venclauskas et al. Venclauskas et al. Scand J GastroenterolScand J Gastroenterol 2009 2009 (24 vs. 50)(24 vs. 50)

PrePre--treatment patient characteristicstreatment patient characteristicsEmbolizationEmbolization SurgerySurgery PP--valuevalue
Mean ageMean age(years)(years)
RipollRipoll 75.275.2 63.363.3
P P < 0.05< 0.05P P > 0.05> 0.05
DefreyneDefreyne ?? ??
ErikssonEriksson 7676 7171
VenclauskasVenclauskas 69.669.6 61.961.9
ComorbidityComorbidity RipollRipoll 90.390.3 79.579.5(%)(%) P P < 0.05< 0.05
P P > 0.05> 0.05
DefreyneDefreyne 17.417.4 15.715.7
ErikssonEriksson 5858 4747
VenclauskasVenclauskas 7575 4040
CoagulopathyCoagulopathy(%)(%)
RipollRipoll 25.825.8 5.15.1
PP < 0.05< 0.05P P > 0.05> 0.05
DefreyneDefreyne 21.721.7 12.212.2
ErikssonEriksson ?? ??
VenclauskasVenclauskas 52.452.4 39.539.5
Bias: TAE for highBias: TAE for high--surgicalsurgical--risk patients risk patients (older, greater incidence of comorbidities, more often anticoagulated)(older, greater incidence of comorbidities, more often anticoagulated)
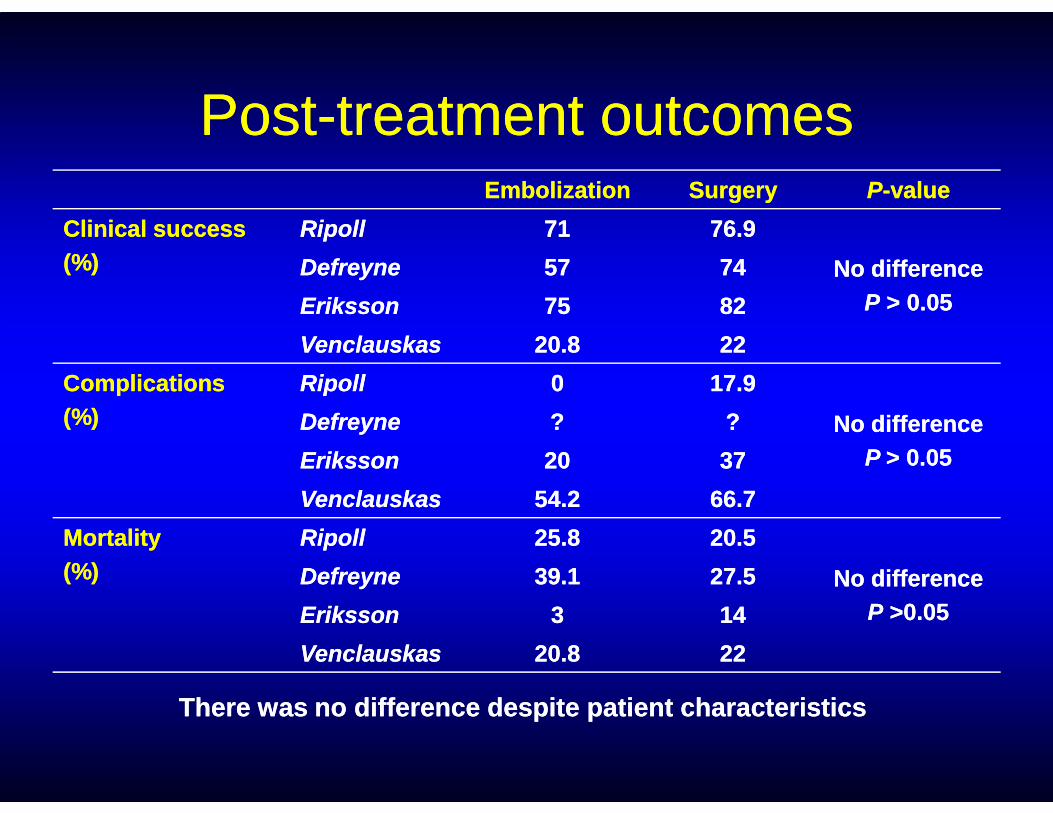
PostPost--treatment outcomestreatment outcomesEmbolizationEmbolization SurgerySurgery PP--valuevalue
Clinical successClinical success(%)(%)
RipollRipoll 7171 76.976.9
No differenceNo differencePP > 0.05> 0.05
DefreyneDefreyne 5757 7474
ErikssonEriksson 7575 8282
VenclauskasVenclauskas 20.820.8 2222
ComplicationsComplications(%)(%)
RipollRipoll 00 17.917.9(%)(%) No differenceNo difference
P P > 0.05> 0.05
DefreyneDefreyne ?? ??
ErikssonEriksson 2020 3737
VenclauskasVenclauskas 54.254.2 66.766.7
MortalityMortality(%)(%)
RipollRipoll 25.825.8 20.520.5
No differenceNo differencePP >0.05>0.05
DefreyneDefreyne 39.139.1 27.527.5
ErikssonEriksson 33 1414
VenclauskasVenclauskas 20.820.8 2222
There was no difference despite patient characteristicsThere was no difference despite patient characteristics

FinallyFinally
•• Is there a still a role for surgery ?Is there a still a role for surgery ?
-- as a last resort for most patientsas a last resort for most patients
-- may be preferable for healthier and youngermay be preferable for healthier and younger-- may be preferable for healthier and youngermay be preferable for healthier and youngerpatients with a peptic ulcer at endoscopy ?patients with a peptic ulcer at endoscopy ?
•• Is there a need for a prospective randomized Is there a need for a prospective randomized controlled study ?controlled study ?
-- but difficult to set up in the emergency but difficult to set up in the emergency
settingsetting
2. 2. FactorsFactors affectingaffecting clinicalclinical successsuccess
•• Clinical predictors of reClinical predictors of re--bleeding ?bleeding ?
•• Technical predictors of reTechnical predictors of re--bleeding ?bleeding ?
-- Blind embolizationBlind embolization
-- Endoscopic marking with a metallic clipEndoscopic marking with a metallic clip
-- Choice of approach/embolic agentChoice of approach/embolic agent
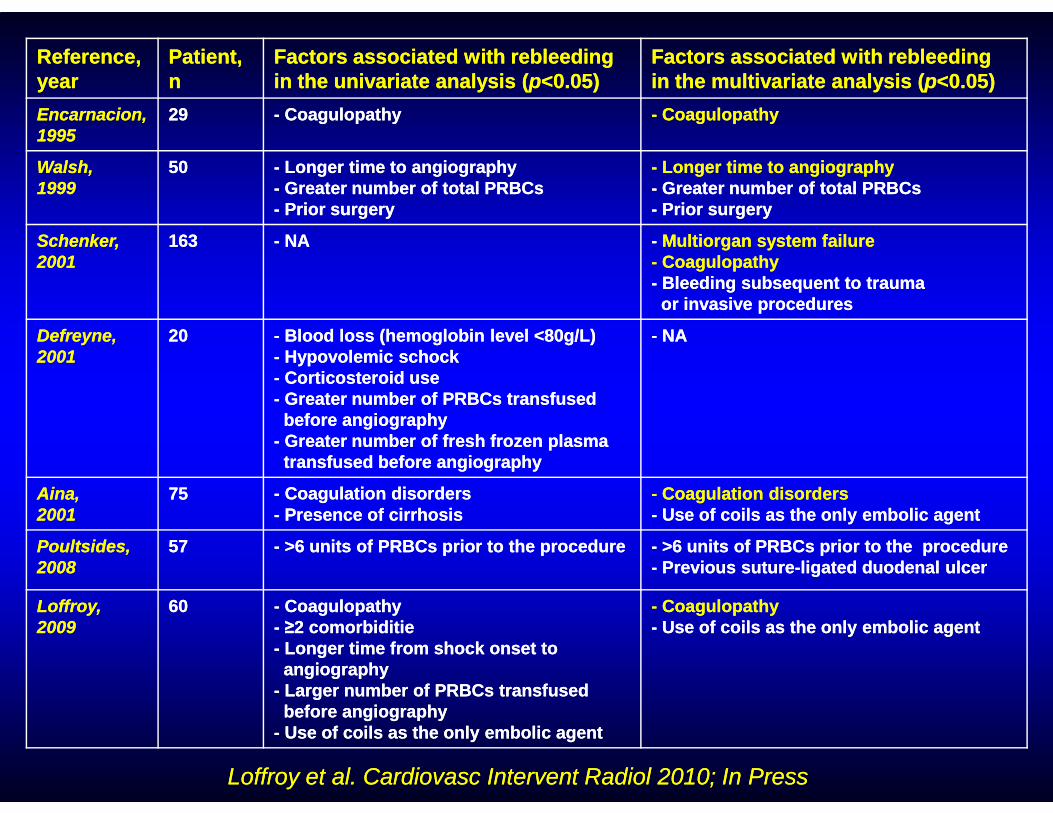
Reference,Reference,yearyear
Patient,Patient,nn
Factors associated with rebleedingFactors associated with rebleedingin the univariate analysis (in the univariate analysis (pp<0.05)<0.05)
Factors associated with rebleedingFactors associated with rebleedingin the multivariate analysis (in the multivariate analysis (pp<0.05)<0.05)
Encarnacion,Encarnacion,19951995
2929 -- Coagulopathy Coagulopathy -- Coagulopathy Coagulopathy
Walsh, Walsh, 19991999
5050 -- Longer time to angiographyLonger time to angiography-- Greater number of total PRBCsGreater number of total PRBCs-- Prior surgeryPrior surgery
-- Longer time to angiographyLonger time to angiography-- Greater number of total PRBCsGreater number of total PRBCs-- Prior surgeryPrior surgery
Schenker,Schenker,20012001
163163 -- NANA -- Multiorgan system failureMultiorgan system failure-- CoagulopathyCoagulopathy-- Bleeding subsequent to traumaBleeding subsequent to traumaor invasive proceduresor invasive procedures
Defreyne,Defreyne,20012001
2020 -- Blood loss (hemoglobin level <80g/L)Blood loss (hemoglobin level <80g/L)-- Hypovolemic schockHypovolemic schock-- Corticosteroid useCorticosteroid use-- Greater number of PRBCs transfusedGreater number of PRBCs transfused
-- NANA
-- Greater number of PRBCs transfusedGreater number of PRBCs transfusedbefore angiography before angiography
-- Greater number of fresh frozenGreater number of fresh frozen plasmaplasmatransfused before angiographytransfused before angiography
Aina,Aina,20012001
7575 -- Coagulation disordersCoagulation disorders -- Presence of cirrhosisPresence of cirrhosis
-- Coagulation disordersCoagulation disorders-- Use of coils as the onlyUse of coils as the only embolic agentembolic agent
Poultsides,Poultsides,20082008
5757 -- >6 units of PRBCs prior to>6 units of PRBCs prior to the procedurethe procedure -- >6 units of PRBCs prior to the>6 units of PRBCs prior to the procedureprocedure-- Previous suturePrevious suture--ligatedligated duodenal ulcerduodenal ulcer
Loffroy,Loffroy,20092009
6060 -- Coagulopathy Coagulopathy -- ≥2 comorbiditie≥2 comorbiditie-- Longer time from shockLonger time from shock onset toonset toangiographyangiography
-- Larger number of PRBCsLarger number of PRBCs transfusedtransfusedbefore angiographybefore angiography
-- Use of coils as the onlyUse of coils as the only embolic agentembolic agent
-- Coagulopathy Coagulopathy -- Use of coils as the onlyUse of coils as the only embolic agentembolic agent
Loffroy et al. Cardiovasc Intervent Radiol 2010; In PressLoffroy et al. Cardiovasc Intervent Radiol 2010; In Press

What can we act on ?What can we act on ?
•• Every effort should be made: Every effort should be made:
-- to perform embolization early after theto perform embolization early after the
onset of bleeding, before it results in MOFonset of bleeding, before it results in MOFonset of bleeding, before it results in MOFonset of bleeding, before it results in MOF
-- to correct coagulation disorders before,to correct coagulation disorders before,during, and after interventionduring, and after intervention

Blind embolizationBlind embolization
•• Empiric or prophylactic embolizationEmpiric or prophylactic embolization
•• Negative angiography and positive endoscopyNegative angiography and positive endoscopy
•• No statistically significant difference in outcome No statistically significant difference in outcome between blind and target embolization in seven between blind and target embolization in seven
•• No statistically significant difference in outcome No statistically significant difference in outcome between blind and target embolization in seven between blind and target embolization in seven retrospective studies:retrospective studies:
-- Univariate analysis: Univariate analysis: -- Multivariate analysisMultivariate analysis: :
+ Walsh et al. 1999 + Schenker et al. 2001+ Walsh et al. 1999 + Schenker et al. 2001+ Defreyne et al. 2001 + Aina et al. 2001+ Defreyne et al. 2001 + Aina et al. 2001+ Loffroy et al. 2009 + Poultsides et al. 2008+ Loffroy et al. 2009 + Poultsides et al. 2008+ Padia et al. 2009+ Padia et al. 2009
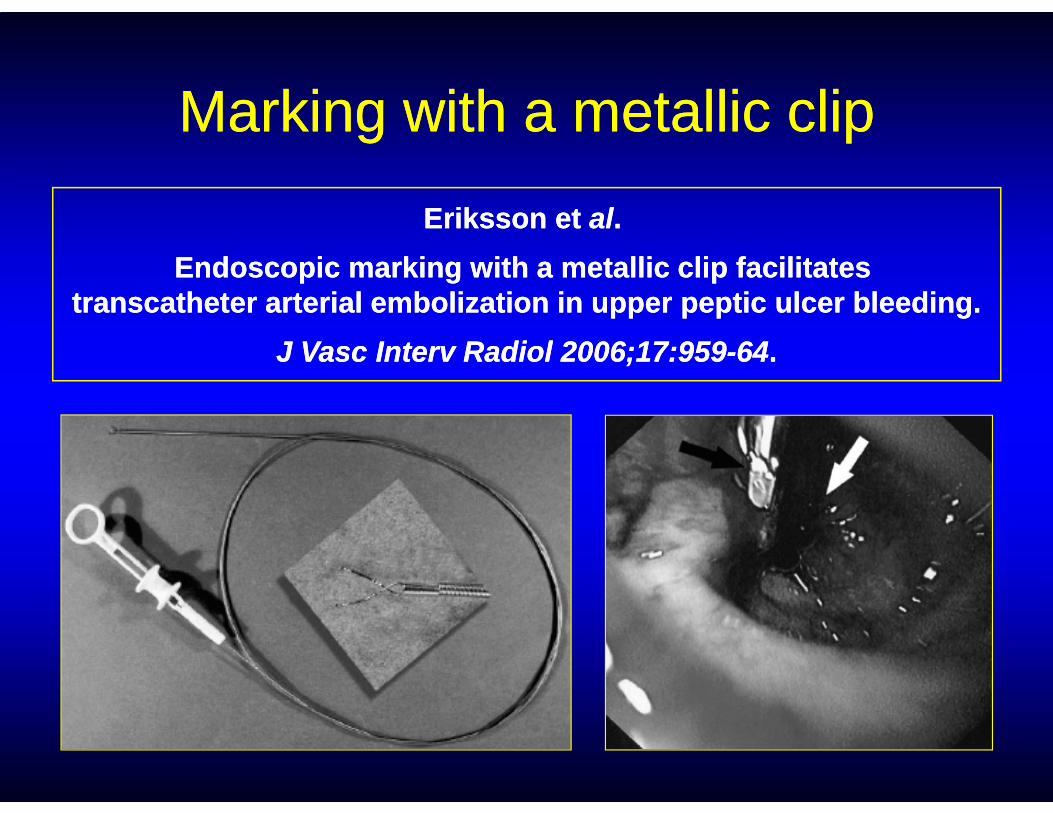
MarkingMarking withwith a a metallicmetallic clipclip
Eriksson et Eriksson et alal. .
Endoscopic marking with a metallic clip facilitates Endoscopic marking with a metallic clip facilitates transcatheter arterial embolization in upper peptic ulcer bleeding.transcatheter arterial embolization in upper peptic ulcer bleeding.
J Vasc Interv Radiol 2006;17:959J Vasc Interv Radiol 2006;17:959--6464..

Choice of embolic agentChoice of embolic agent
•• No consensusNo consensus•• Many embolic options available used alone or in Many embolic options available used alone or in
combinationcombination•• However, when used as the only embolic agent:However, when used as the only embolic agent:
-- Gelatin sponge: Gelatin sponge: low clinical success (<65%) low clinical success (<65%) -- Gelatin sponge: Gelatin sponge: low clinical success (<65%) low clinical success (<65%) + Encarnacion et al. 1992+ Encarnacion et al. 1992
+ Lang EK. 1992+ Lang EK. 1992
-- Coils: Coils: statistically correlated with restatistically correlated with re--bleeding bleeding + Aina et al. 2001 (OR=7.7)+ Aina et al. 2001 (OR=7.7)
+ Loffroy et al. 2009+ Loffroy et al. 2009 (OR=6.2) (OR=6.2)
-- Glue: Glue: high clinical success (>90%) high clinical success (>90%) + Lee et al. 2007+ Lee et al. 2007
+ Jae et al. 2007+ Jae et al. 2007

Any recommendations ?
•• Maybe coils and gelatin sponge should not be used alone Maybe coils and gelatin sponge should not be used alone but in combination, especially when using the sandwichbut in combination, especially when using the sandwichtechnique (GDA ++)technique (GDA ++)
•• Don’t hesitate to use glue, especially in patients withDon’t hesitate to use glue, especially in patients withcoagulopathy (better and faster hemostasis ++)coagulopathy (better and faster hemostasis ++)
•• However: it is preferable to choose the agent based on However: it is preferable to choose the agent based on operator’s experience and clinical situationoperator’s experience and clinical situation

Active bleeding gastric Dieulafoy lesion Active bleeding gastric Dieulafoy lesion at endoscopy in a 87at endoscopy in a 87--yearyear--old man old man
with coagulopathywith coagulopathy
Choice: Choice: Superselective glue embolizationSuperselective glue embolization(Loffroy et al. Clin Gastroenterol Hepatol 2009)(Loffroy et al. Clin Gastroenterol Hepatol 2009)
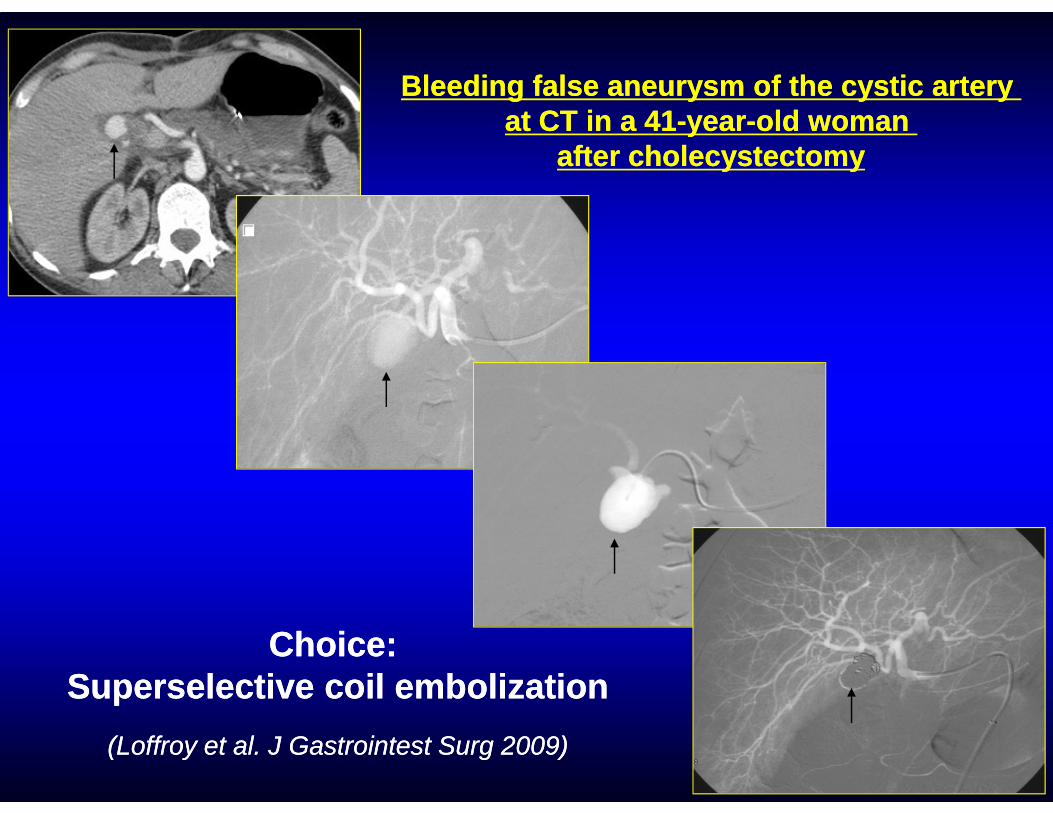
Bleeding false aneurysm of the cystic artery Bleeding false aneurysm of the cystic artery at CT in a 41at CT in a 41--yearyear--old woman old woman
after cholecystectomyafter cholecystectomy
Choice: Choice: Superselective coil embolizationSuperselective coil embolization
(Loffroy et al. J Gastrointest Surg 2009)(Loffroy et al. J Gastrointest Surg 2009)
3. Other Tips3. Other Tips
…some noteworthy technical points to …some noteworthy technical points to increase the chance of getting better increase the chance of getting better results:results:
-- Tip #1: get a good angiographyTip #1: get a good angiography
-- Tip #2: use a microcatheterTip #2: use a microcatheter
-- Tip #3: repeat angiographyTip #3: repeat angiography
-- Tip #4: check the back doorTip #4: check the back door

Tip #1Tip #1
•• Get a good angiography to characterize the Get a good angiography to characterize the lesion, the presence of anatomic variations and lesion, the presence of anatomic variations and the importance of vessel networkthe importance of vessel network

Tip #2Tip #2
•• Use a microcatheter to make the procedure Use a microcatheter to make the procedure much easier much easier
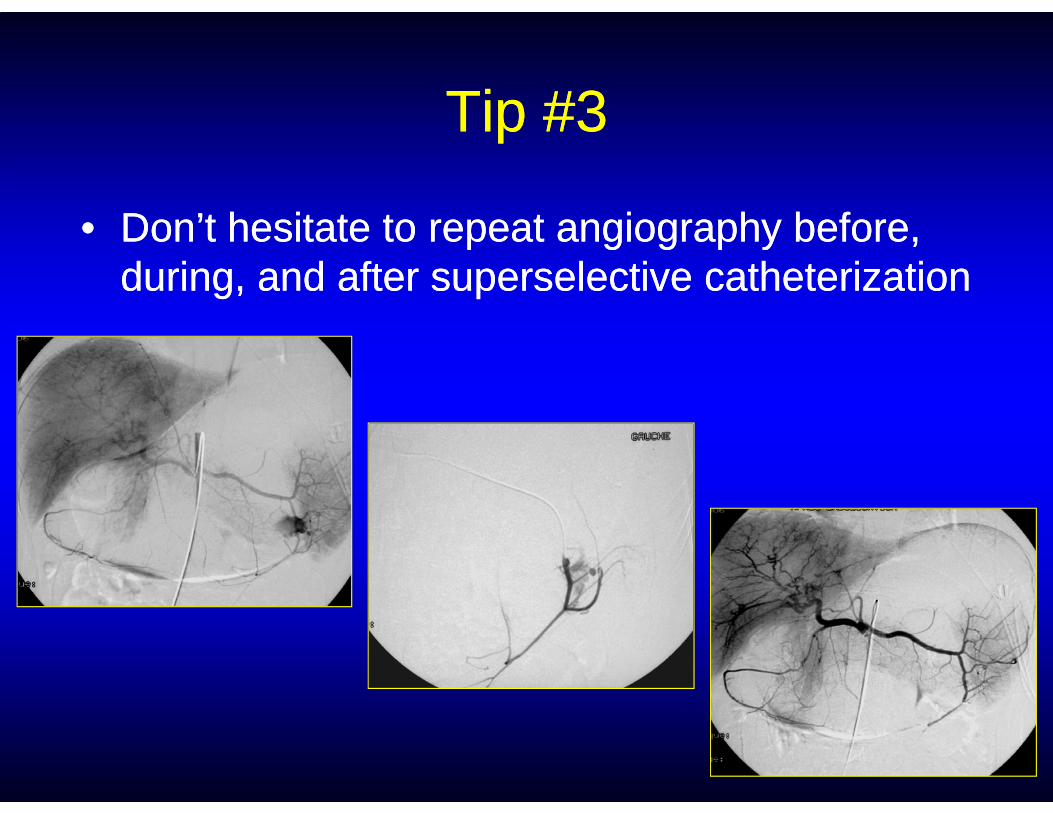
Tip #3Tip #3
•• Don’t hesitate to repeat angiography before, Don’t hesitate to repeat angiography before, during, and after superselective catheterizationduring, and after superselective catheterization
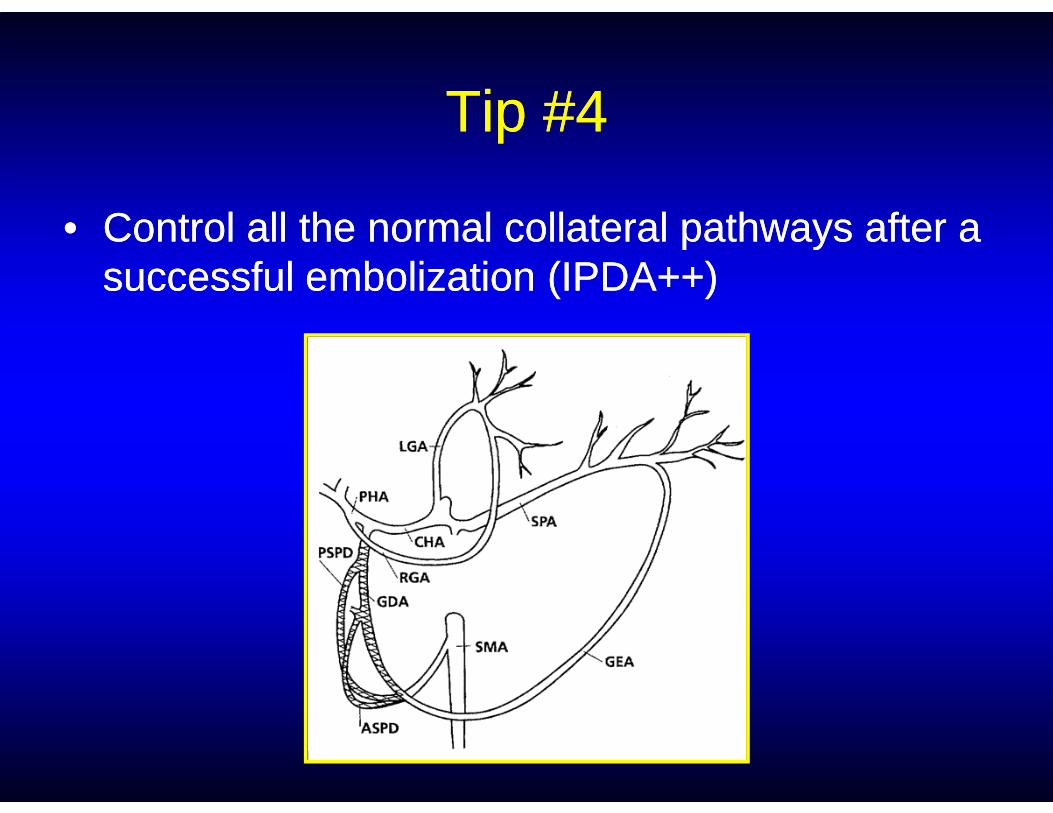
Tip #4Tip #4
•• Control all the normal collateral pathways after a Control all the normal collateral pathways after a successful embolization (IPDA++)successful embolization (IPDA++)

Conclusion: take home pointsConclusion: take home points
•• Embolization should be the second choiceEmbolization should be the second choice
•• Don’t forget to correct coagulation disorders Don’t forget to correct coagulation disorders
•• Cooperation is always welcomed: use endoscopic markingCooperation is always welcomed: use endoscopic marking
•• Usefulness of CTUsefulness of CT•• Usefulness of CTUsefulness of CT
•• Critical to know the anatomy and variantsCritical to know the anatomy and variants
•• Consider empiric embolizationConsider empiric embolization
•• Remember «Remember « back door bleedingback door bleeding »»
•• Don’t hesitate to use NBCADon’t hesitate to use NBCA
•• Be aggressive and fast: this procedure saves lives !Be aggressive and fast: this procedure saves lives !