sfav journée d’automne
TRANSCRIPT
SFAVSFAVJournJournéée de d’’automneautomne
J PengloanDécembre 2008
nn DOPPSDOPPSnn USRDSUSRDSnn ASNASNnn SNSN--SFDSFDnn Article Article
DOPPS
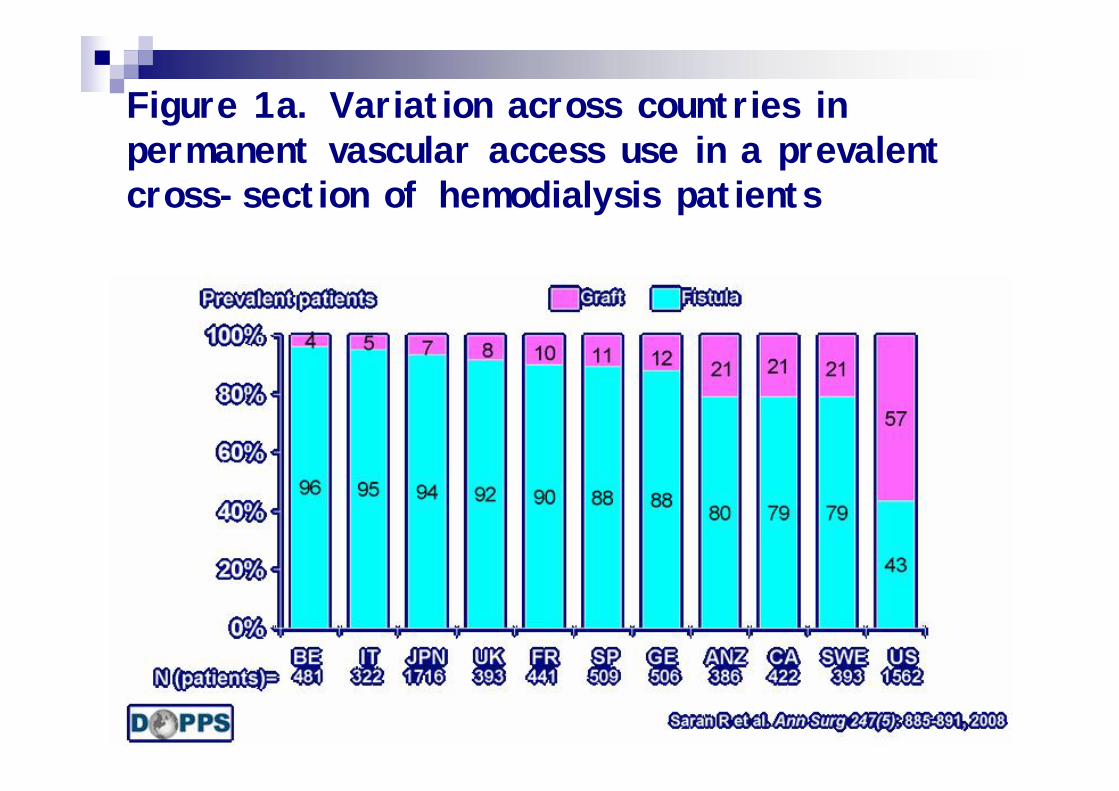
Figure 1a. Variation across countries in permanent vascular access use in a prevalent cross-section of hemodialysis patients
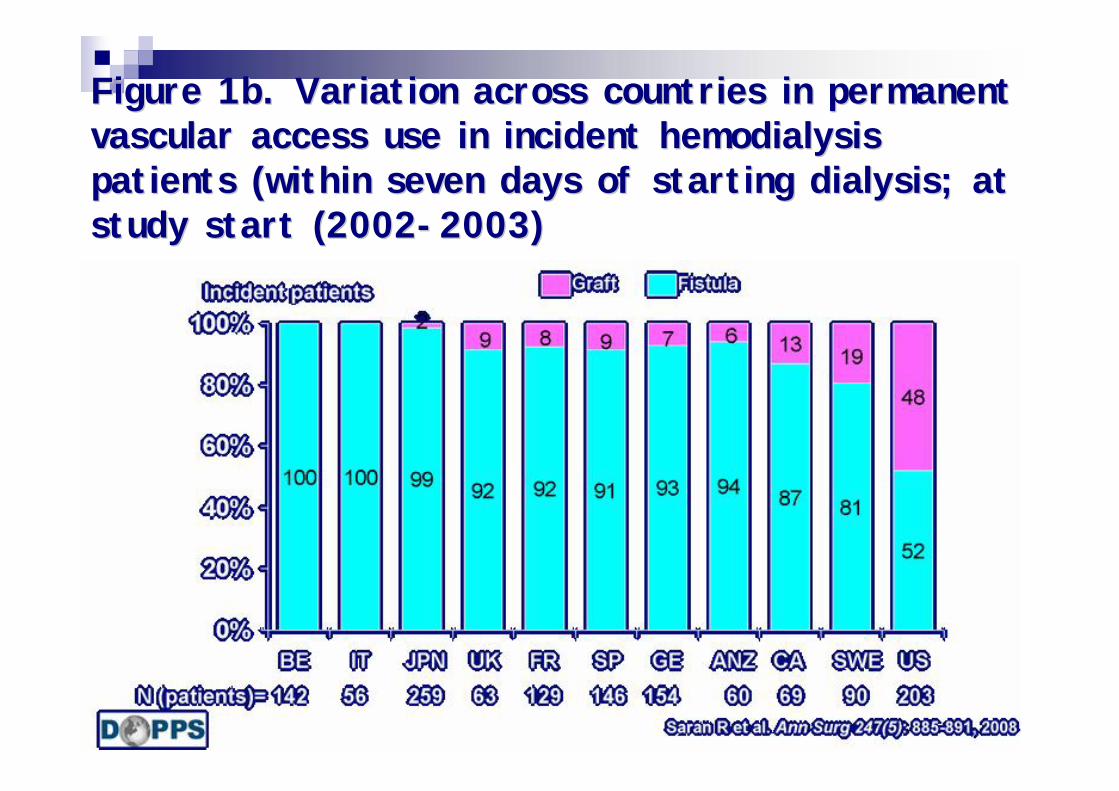
Figure 1b. Variation across countries in permanent Figure 1b. Variation across countries in permanent vascular access use in incident hemodialysis vascular access use in incident hemodialysis patients (within seven days of starting dialysis; at patients (within seven days of starting dialysis; at study start (2002study start (2002--2003)2003)
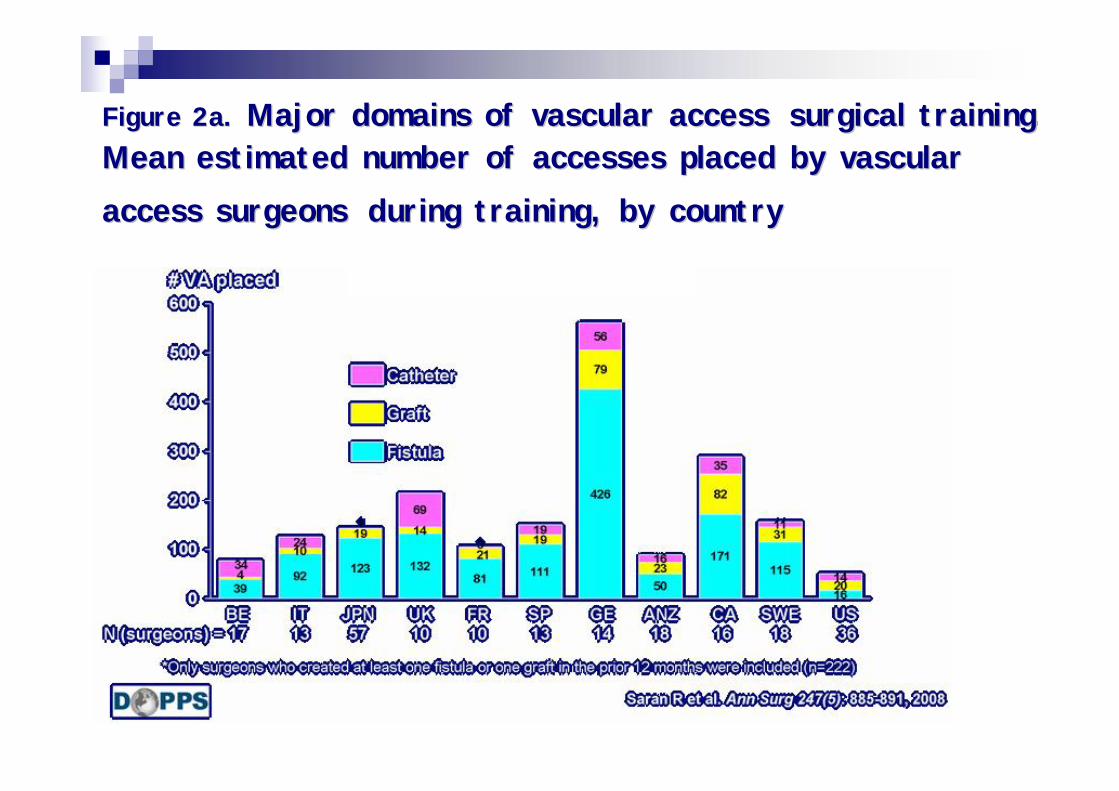
Figure 2a. Figure 2a. Major domains of vascular accessMajor domains of vascular access surgical training. surgical training. Mean estimated number of accesses placed by vascular Mean estimated number of accesses placed by vascular access surgeonsaccess surgeons during training, by countryduring training, by country
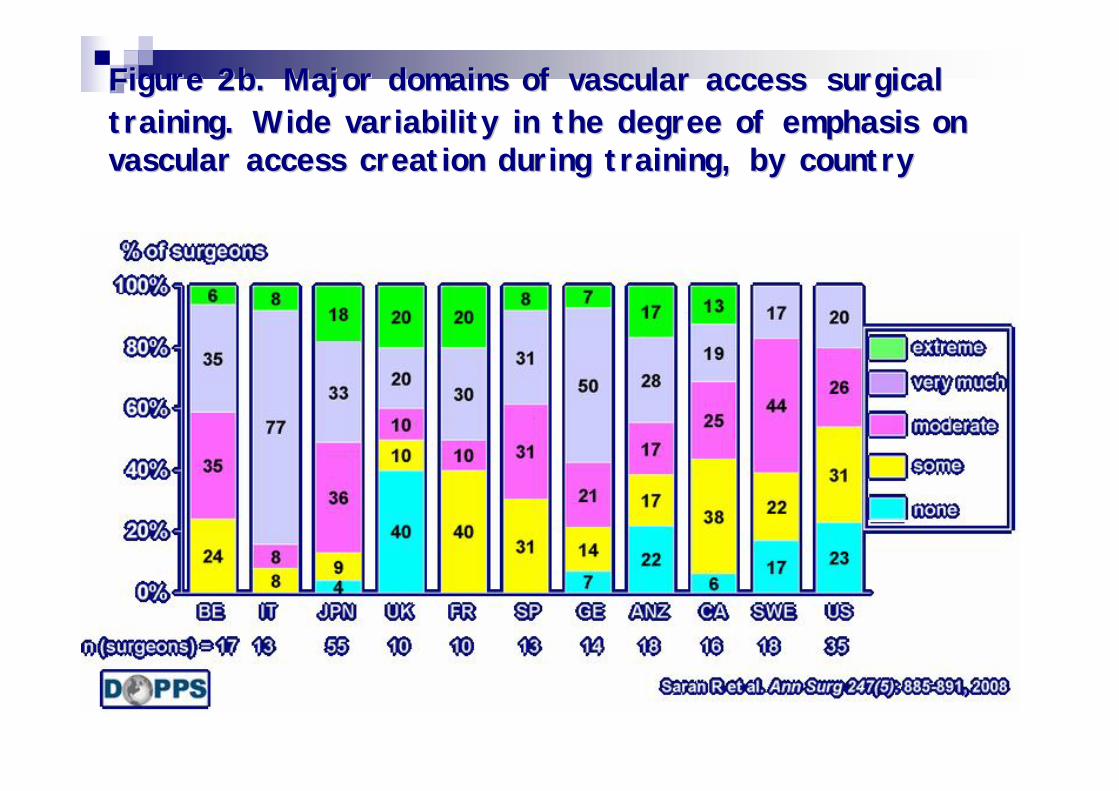
Figure 2b. Major domains of vascular accessFigure 2b. Major domains of vascular access surgical surgical training. Wide variability in the degree of emphasis on training. Wide variability in the degree of emphasis on vascular access creation during training, by countryvascular access creation during training, by country
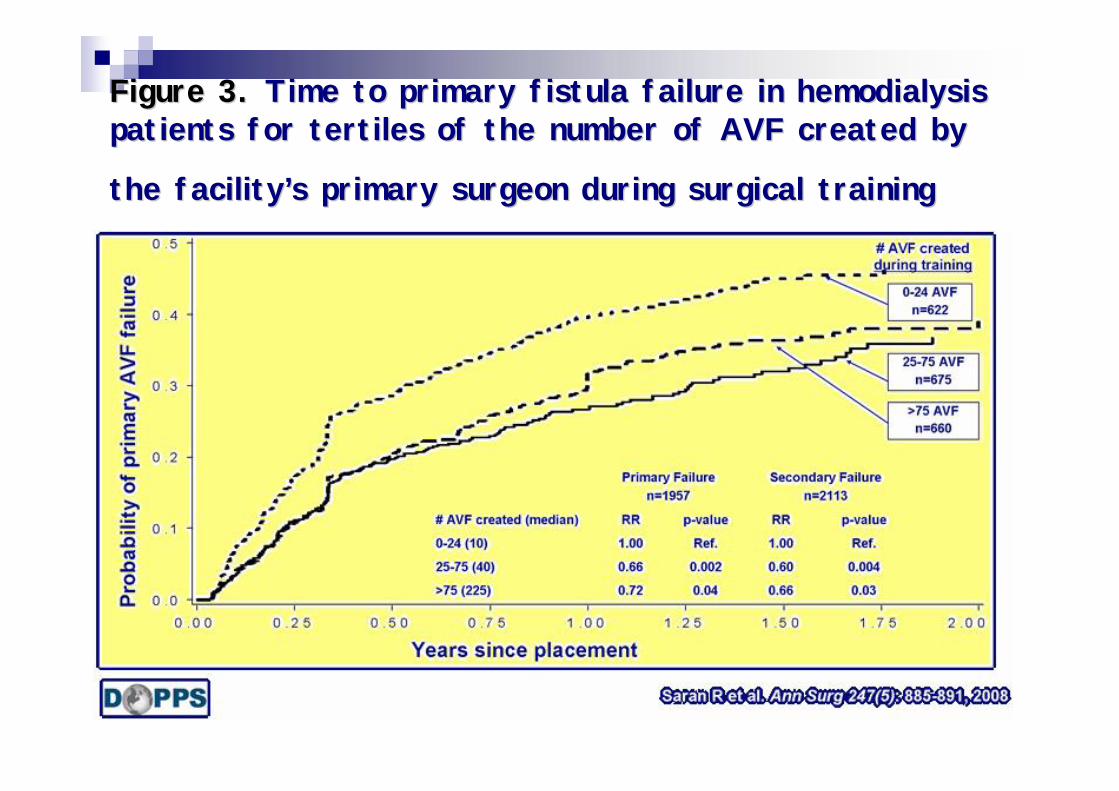
Figure 3. Figure 3. Time to primary fistula failure in hemodialysis Time to primary fistula failure in hemodialysis patients for tertiles of the number of AVF created by patients for tertiles of the number of AVF created by
the facilitythe facility’’s primary surgeon during surgical trainings primary surgeon during surgical training
ConclusionsConclusions
Consistent Aspirin Use Associated with Consistent Aspirin Use Associated with Improved Arteriovenous Fistula Survival Improved Arteriovenous Fistula Survival among Incident Hemodialysisamong Incident HemodialysisPatients in the Dialysis Outcomes and Patients in the Dialysis Outcomes and Practice Patterns StudyPractice Patterns Study
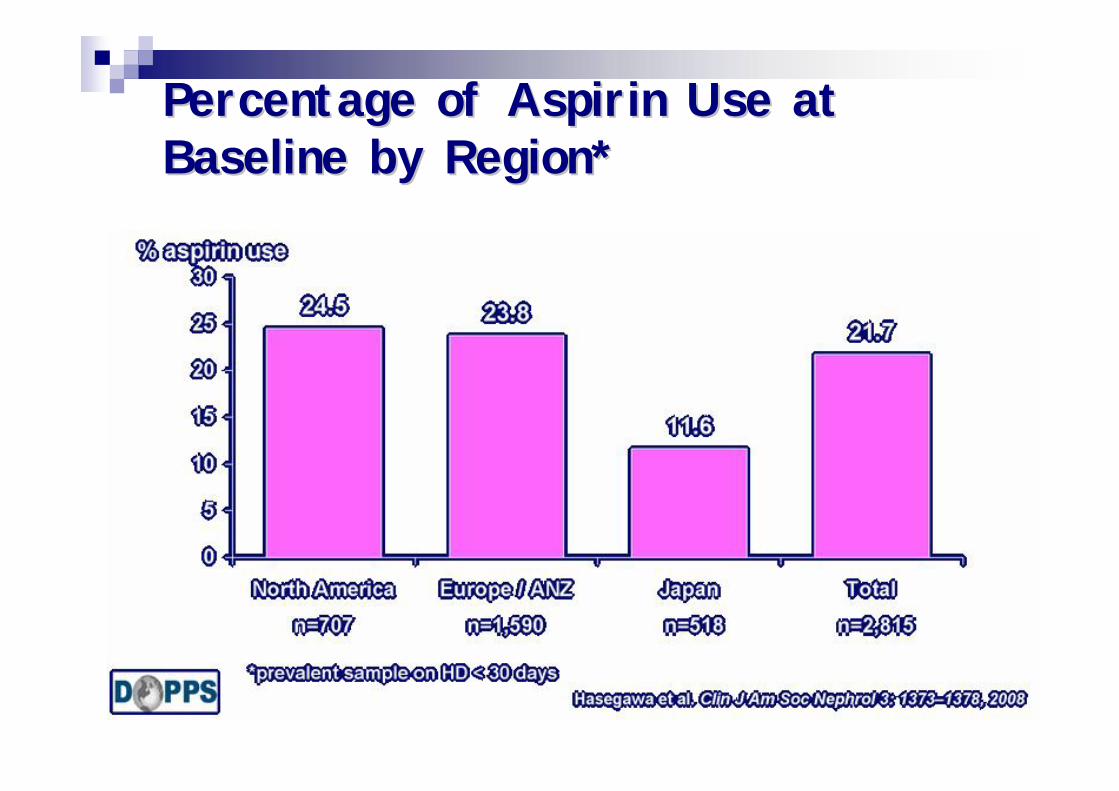
Percentage of Aspirin Use at Percentage of Aspirin Use at Baseline by Region*Baseline by Region*
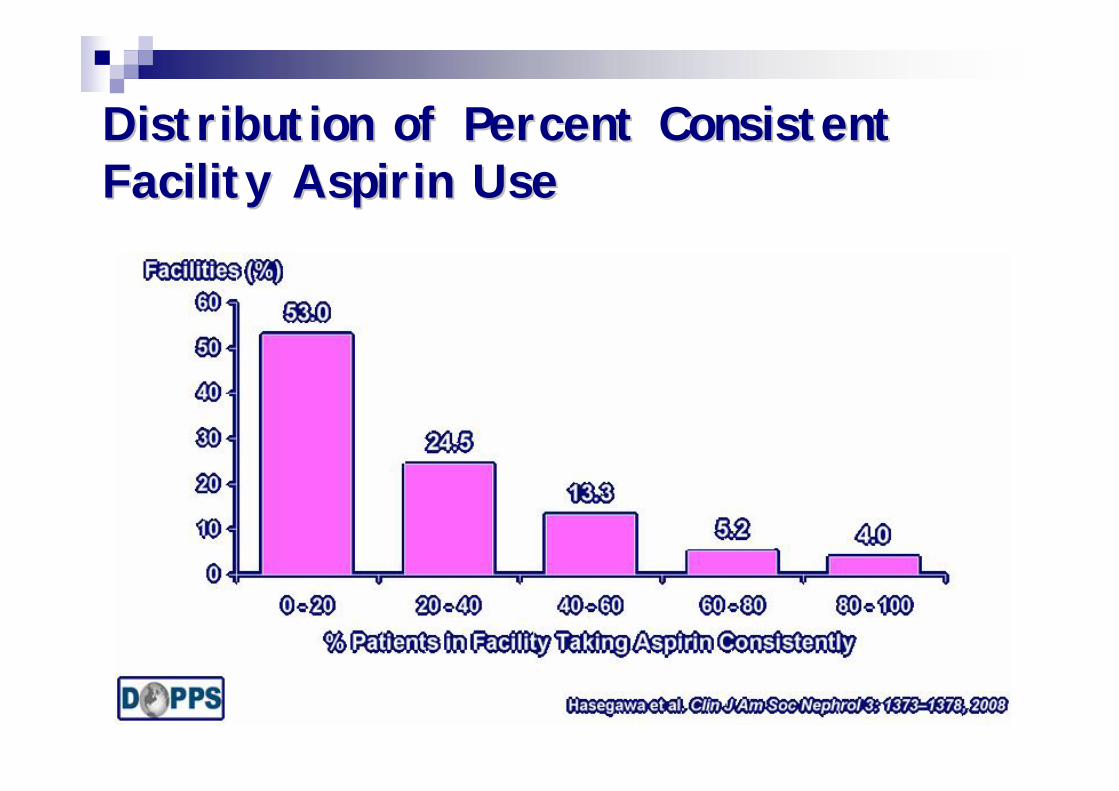
Distribution of Percent Consistent Distribution of Percent Consistent Facility Aspirin UseFacility Aspirin Use
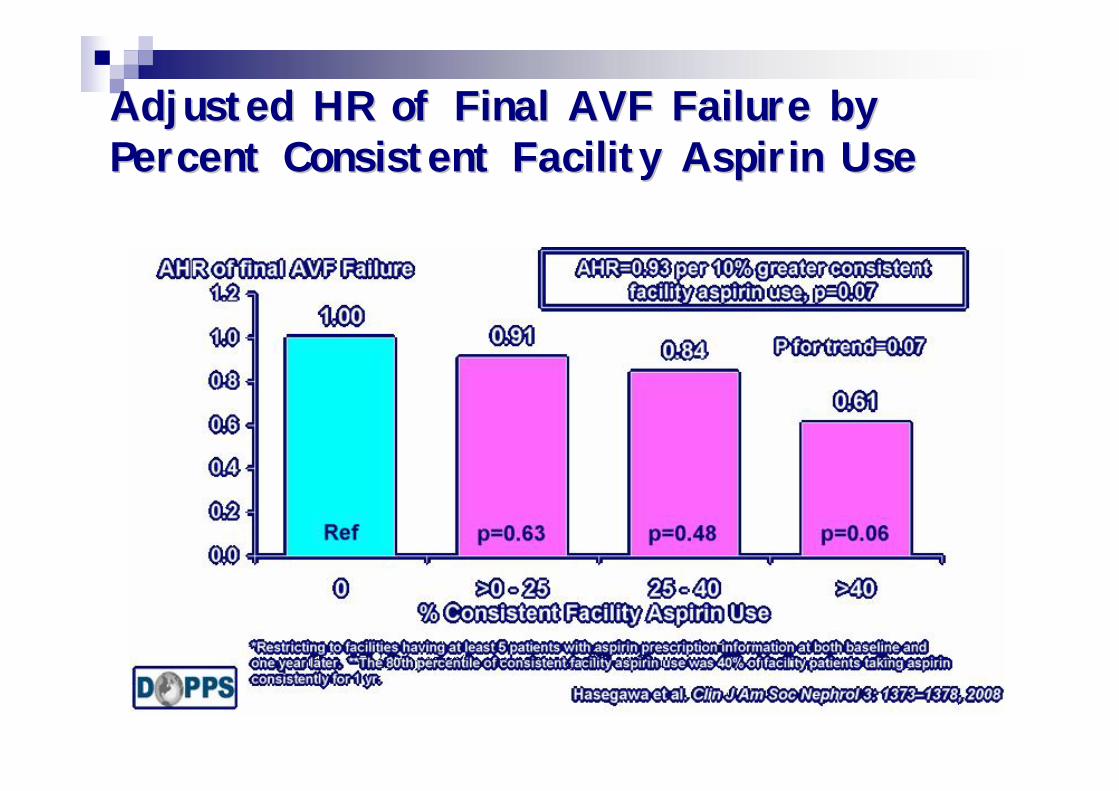
Adjusted HR of Final AVF Failure by Adjusted HR of Final AVF Failure by Percent Consistent Facility Aspirin UsePercent Consistent Facility Aspirin Use
ConclusionConclusion
USRDS 2008 Annual Data ReportInternational comparisonsInternational comparisons
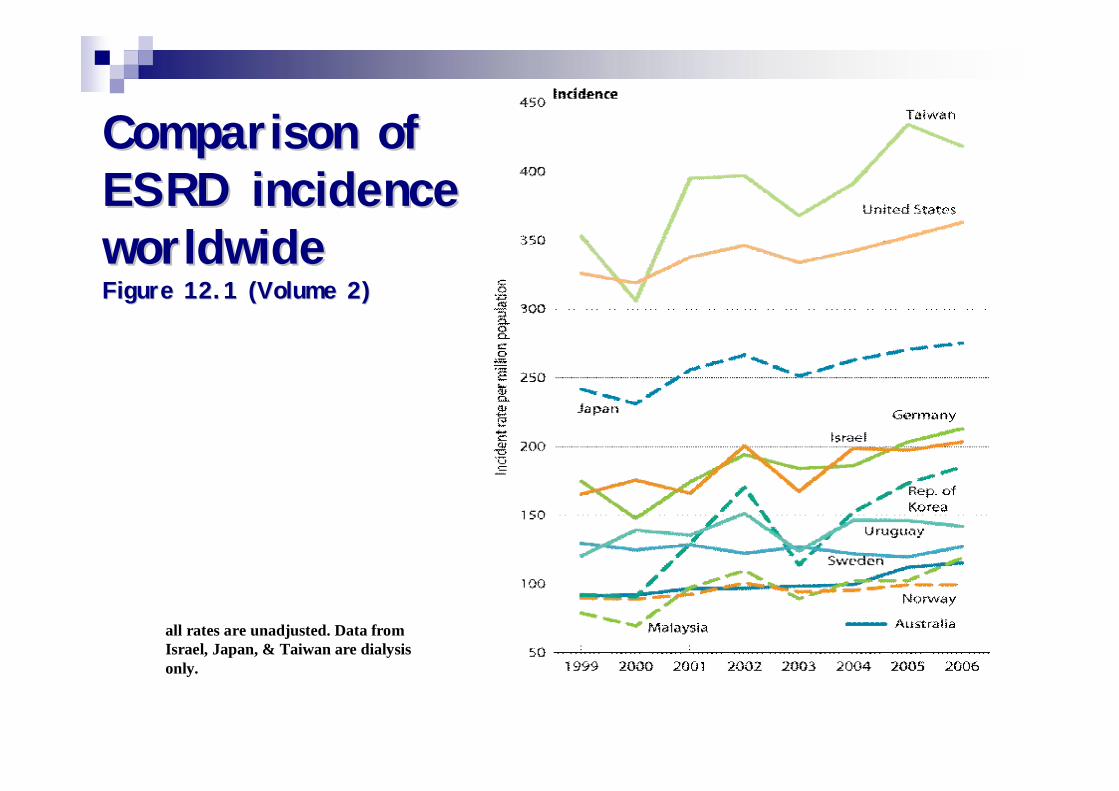
Comparison of Comparison of ESRD incidence ESRD incidence worldwideworldwideFigure 12.1 (Volume 2)Figure 12.1 (Volume 2)
all rates are unadjusted. Data from Israel, Japan, & Taiwan are dialysis only.
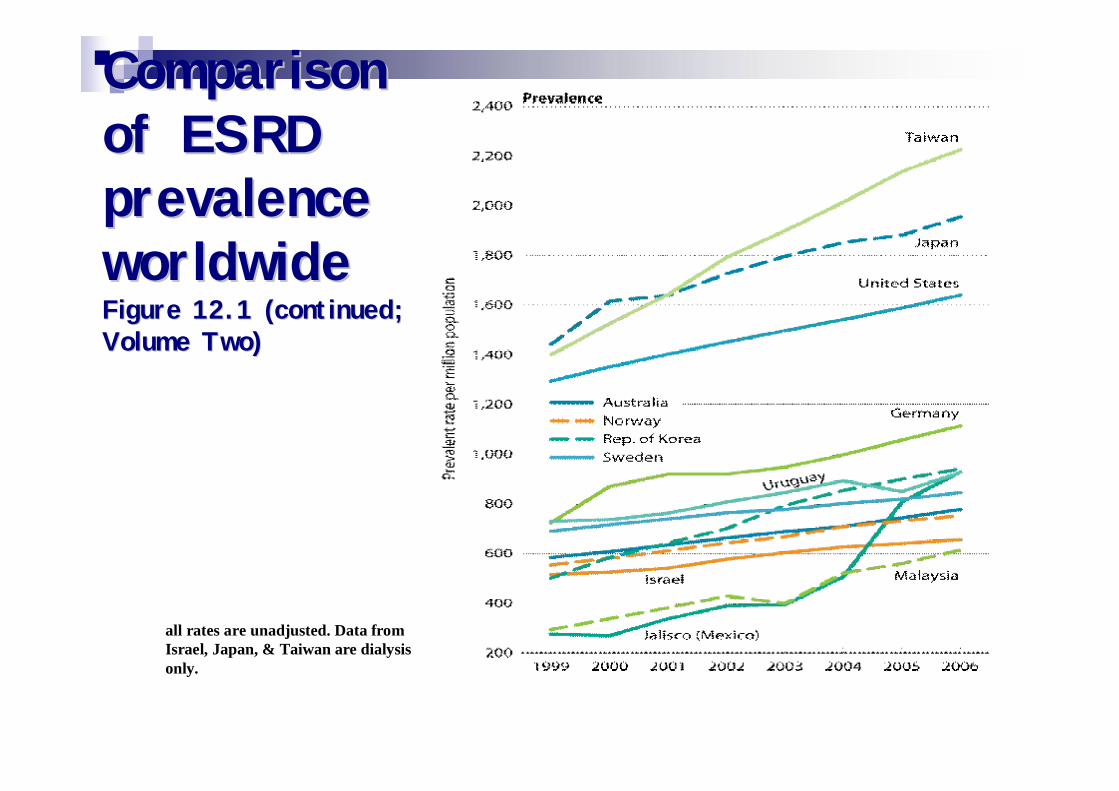
Comparison Comparison of ESRD of ESRD prevalence prevalence worldwideworldwideFigure 12.1 (continued; Figure 12.1 (continued; Volume Two)Volume Two)
all rates are unadjusted. Data from Israel, Japan, & Taiwan are dialysis only.
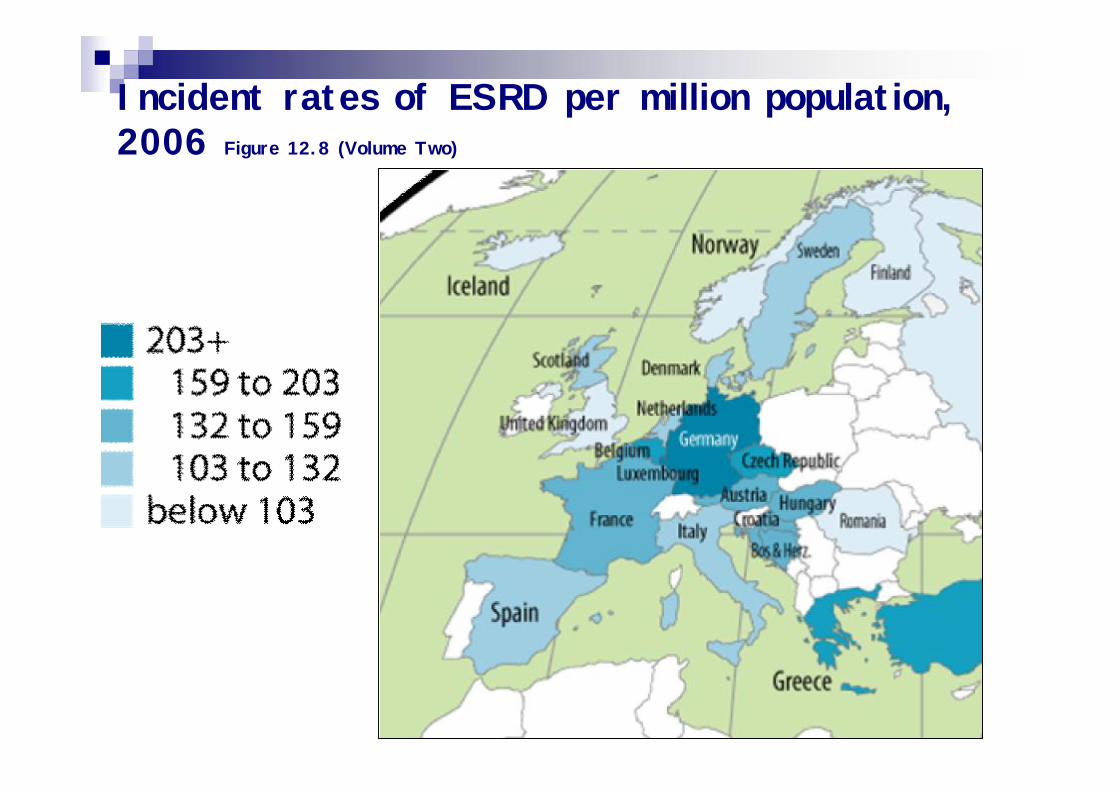
Incident rates of ESRD per million population, 2006 Figure 12.8 (Volume Two)
USRDS 2008 Annual Data Report
Costs of ESRDCosts of ESRD
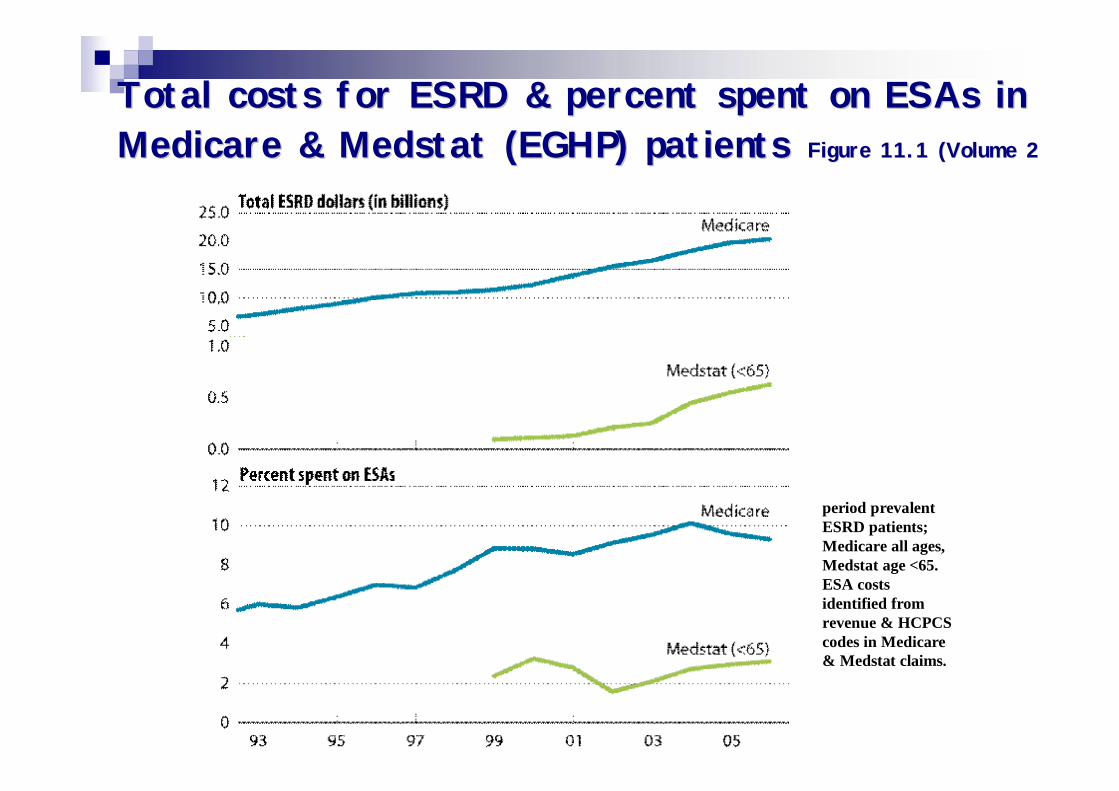
Total costs for ESRD & percent spent on ESAs in Total costs for ESRD & percent spent on ESAs in Medicare & Medstat (EGHP) patientsMedicare & Medstat (EGHP) patients Figure 11.1 (Volume 2)Figure 11.1 (Volume 2)
period prevalent ESRD patients; Medicare all ages, Medstat age <65. ESA costs identified from revenue & HCPCS codes in Medicare & Medstat claims.
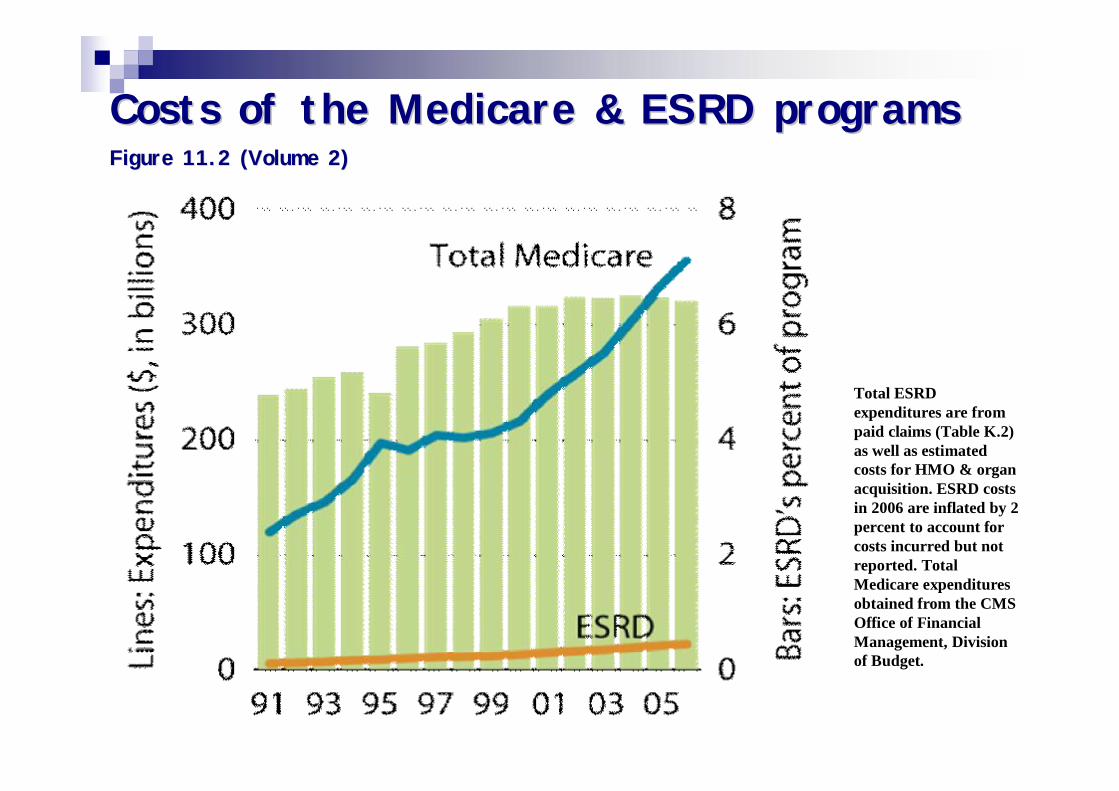
Costs of the Medicare & ESRD programs Costs of the Medicare & ESRD programs Figure 11.2 (Volume 2)Figure 11.2 (Volume 2)
Total ESRD expenditures are from paid claims (Table K.2) as well as estimated costs for HMO & organ acquisition. ESRD costs in 2006 are inflated by 2 percent to account for costs incurred but not reported. Total Medicare expenditures obtained from the CMS Office of Financial Management, Division of Budget.
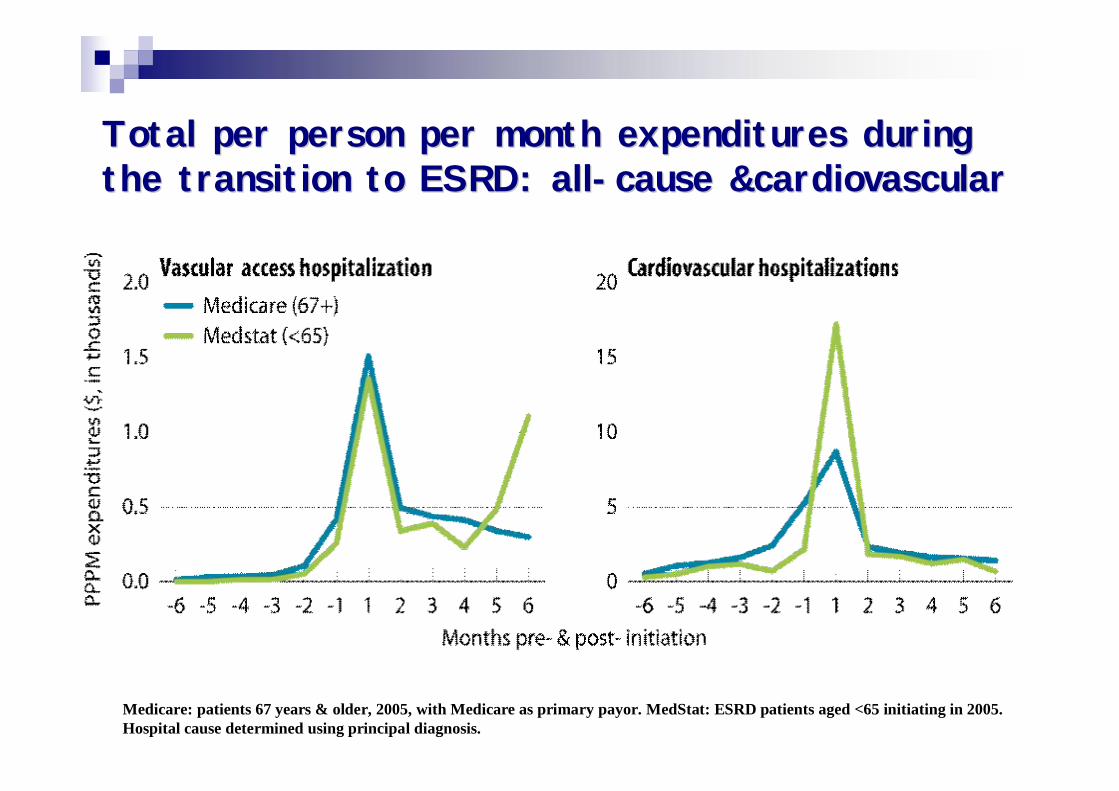
Total per person per month expenditures during Total per person per month expenditures during the transition to ESRD: allthe transition to ESRD: all--cause &cardiovascularcause &cardiovascular
Medicare: patients 67 years & older, 2005, with Medicare as primary payor. MedStat: ESRD patients aged <65 initiating in 2005. Hospital cause determined using principal diagnosis.
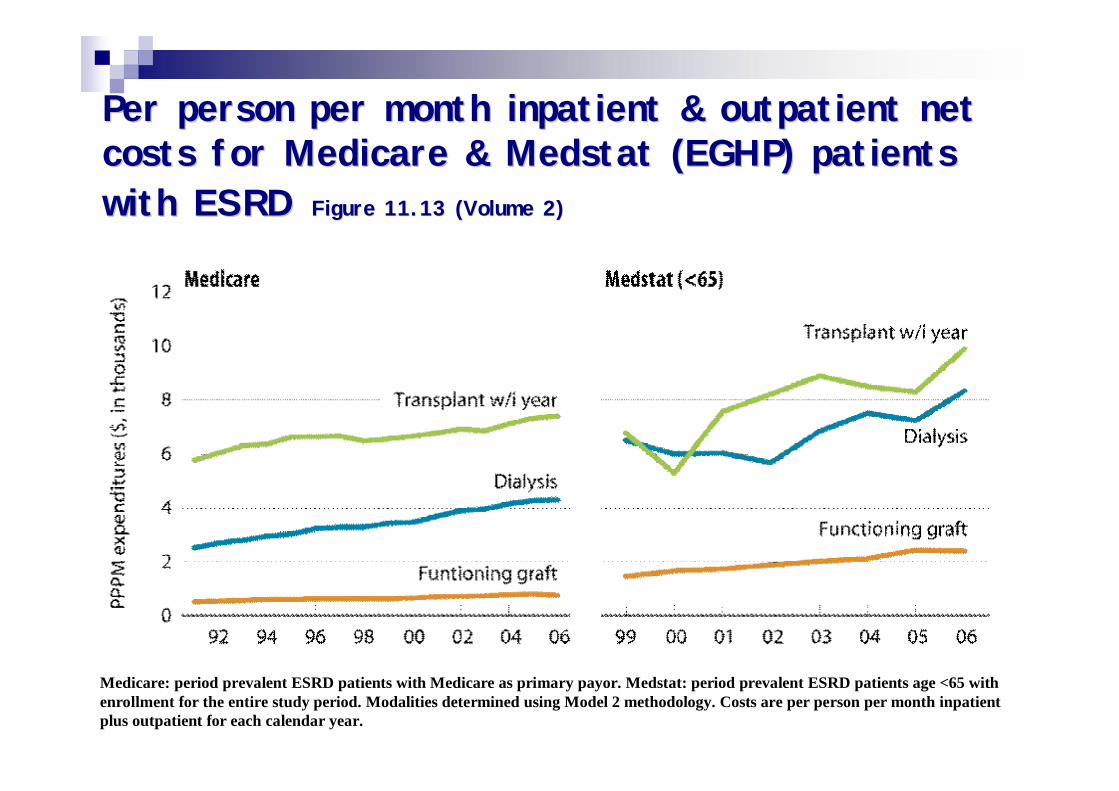
Per person per month inpatient & outpatient net Per person per month inpatient & outpatient net costs for Medicare & Medstat (EGHP) patients costs for Medicare & Medstat (EGHP) patients with ESRDwith ESRD Figure 11.13 (Volume 2)Figure 11.13 (Volume 2)
Medicare: period prevalent ESRD patients with Medicare as primary payor. Medstat: period prevalent ESRD patients age <65 with enrollment for the entire study period. Modalities determined using Model 2 methodology. Costs are per person per month inpatient plus outpatient for each calendar year.
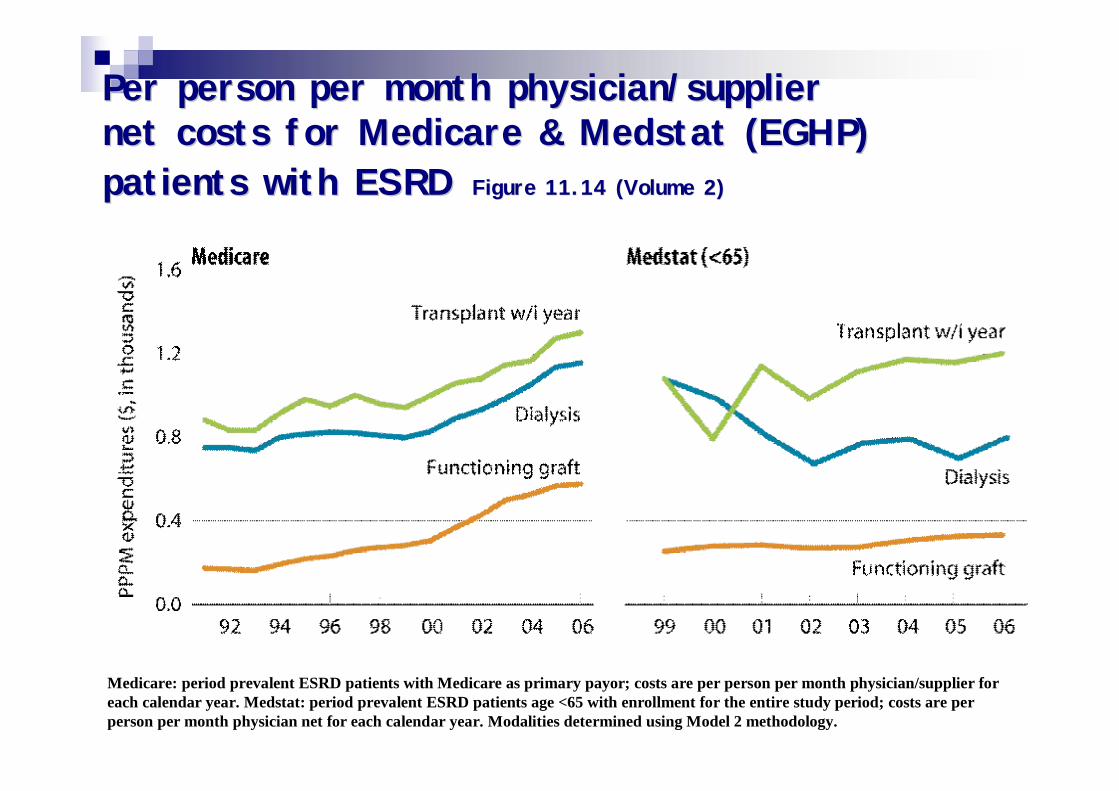
Per person per month physician/supplier Per person per month physician/supplier net costs for Medicare & Medstat (EGHP) net costs for Medicare & Medstat (EGHP) patients with ESRDpatients with ESRD Figure 11.14 (Volume 2)Figure 11.14 (Volume 2)
Medicare: period prevalent ESRD patients with Medicare as primary payor; costs are per person per month physician/supplier for each calendar year. Medstat: period prevalent ESRD patients age <65 with enrollment for the entire study period; costs are per person per month physician net for each calendar year. Modalities determined using Model 2 methodology.
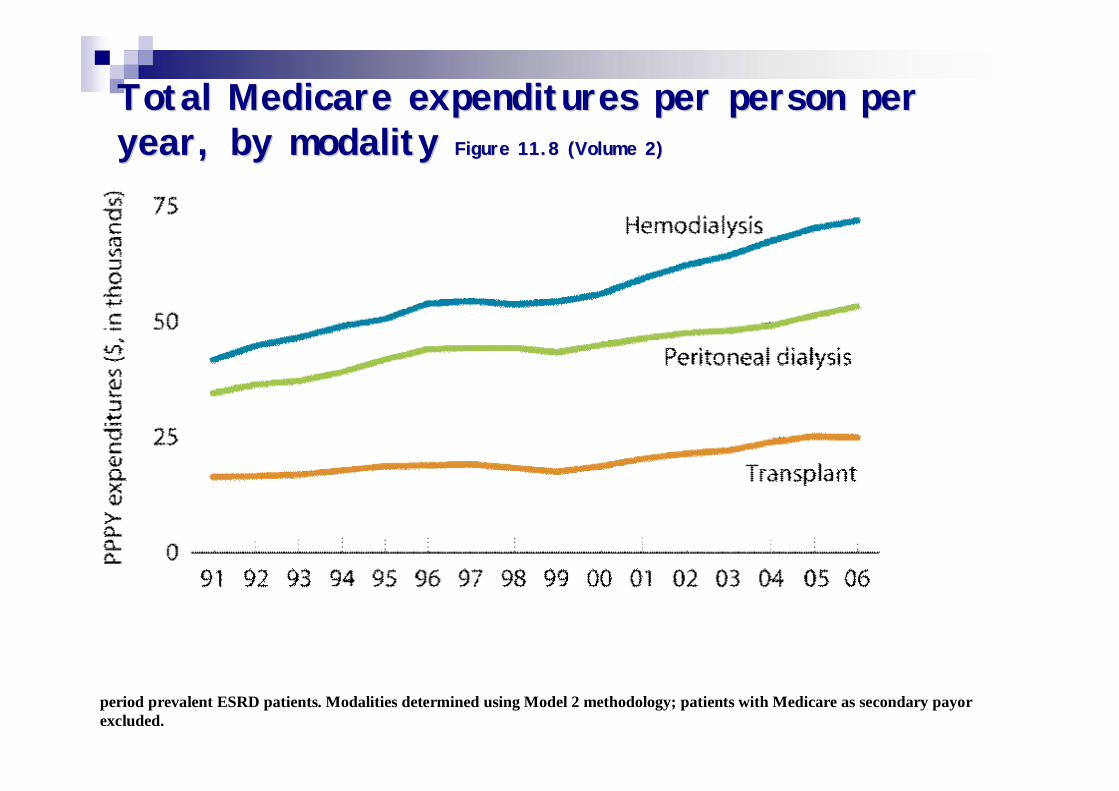
Total Medicare expenditures per person per Total Medicare expenditures per person per year, by modality year, by modality Figure 11.8 (Volume 2)Figure 11.8 (Volume 2)
period prevalent ESRD patients. Modalities determined using Model 2 methodology; patients with Medicare as secondary payor excluded.
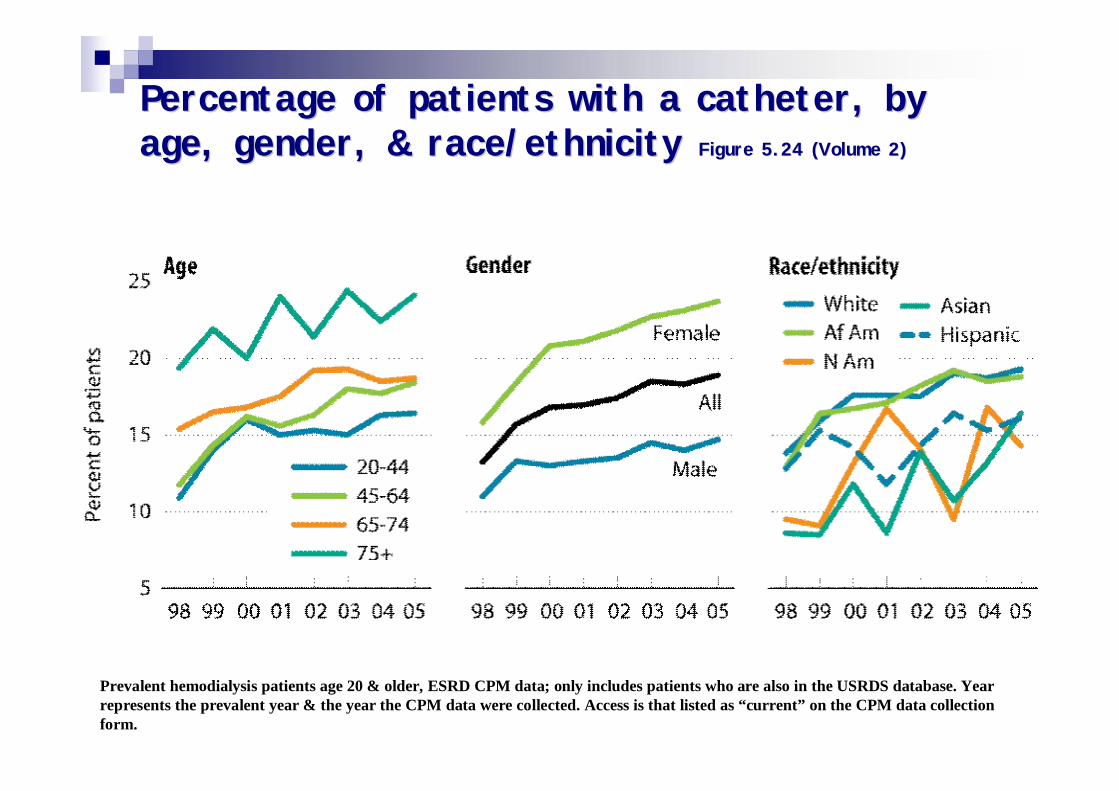
Percentage of patients with a catheter, by Percentage of patients with a catheter, by age, gender, & race/ethnicity age, gender, & race/ethnicity Figure 5.24 (Volume 2)Figure 5.24 (Volume 2)
Prevalent hemodialysis patients age 20 & older, ESRD CPM data; only includes patients who are also in the USRDS database. Year represents the prevalent year & the year the CPM data were collected. Access is that listed as “current” on the CPM data collection form.
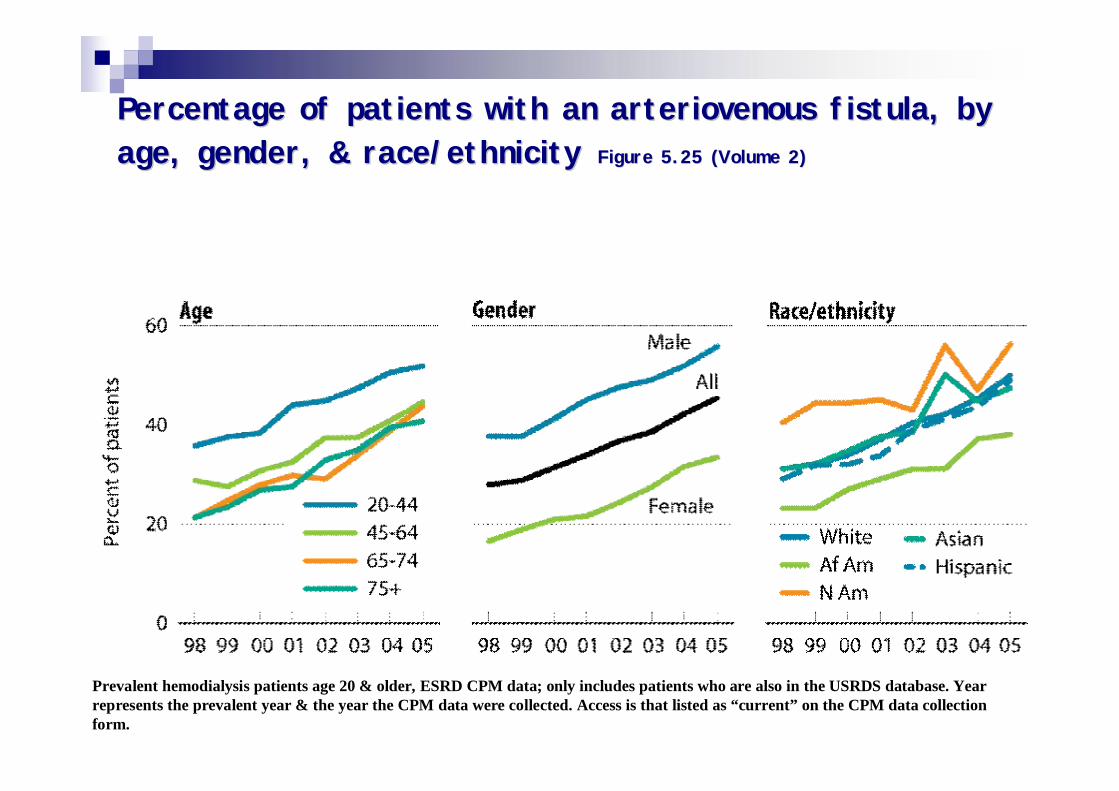
Percentage of patients with an arteriovenous fistula, by Percentage of patients with an arteriovenous fistula, by age, gender, & race/ethnicityage, gender, & race/ethnicity Figure 5.25 (Volume 2)Figure 5.25 (Volume 2)
Prevalent hemodialysis patients age 20 & older, ESRD CPM data; only includes patients who are also in the USRDS database. Year represents the prevalent year & the year the CPM data were collected. Access is that listed as “current” on the CPM data collection form.
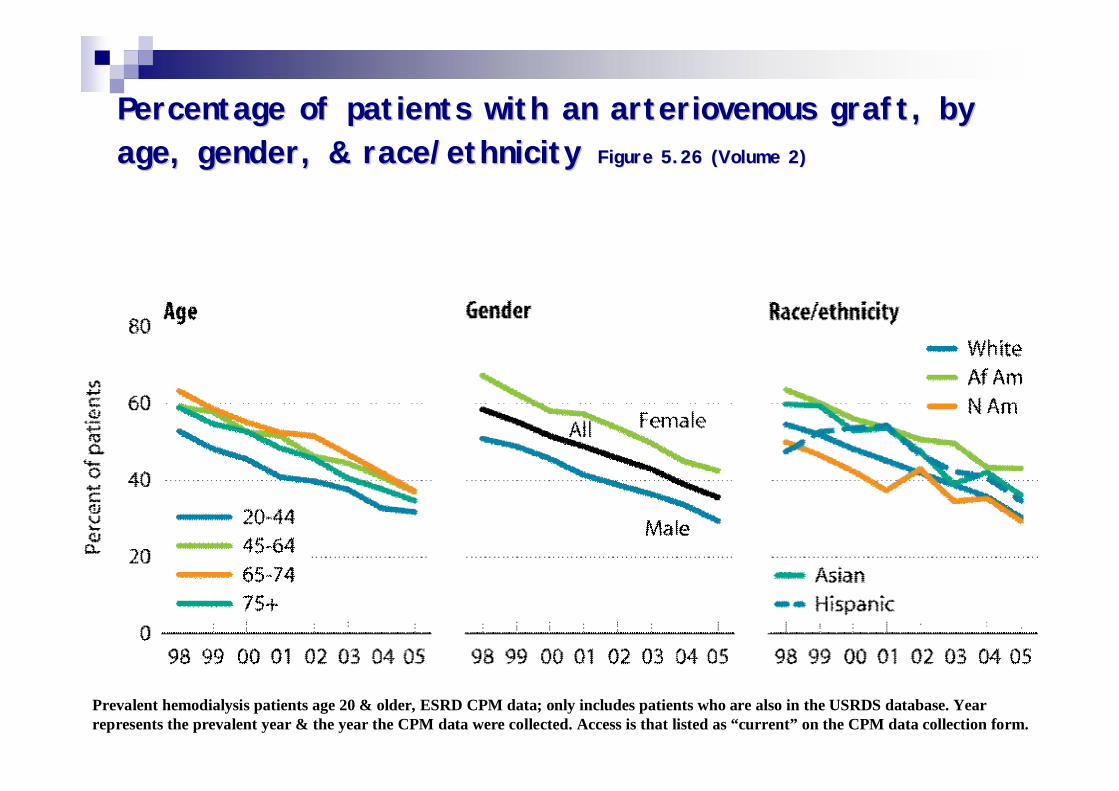
Percentage of patients with an arteriovenous graft, by Percentage of patients with an arteriovenous graft, by age, gender, & race/ethnicityage, gender, & race/ethnicity Figure 5.26 (Volume 2)Figure 5.26 (Volume 2)
Prevalent hemodialysis patients age 20 & older, ESRD CPM data; only includes patients who are also in the USRDS database. Year represents the prevalent year & the year the CPM data were collected. Access is that listed as “current” on the CPM data collection form.
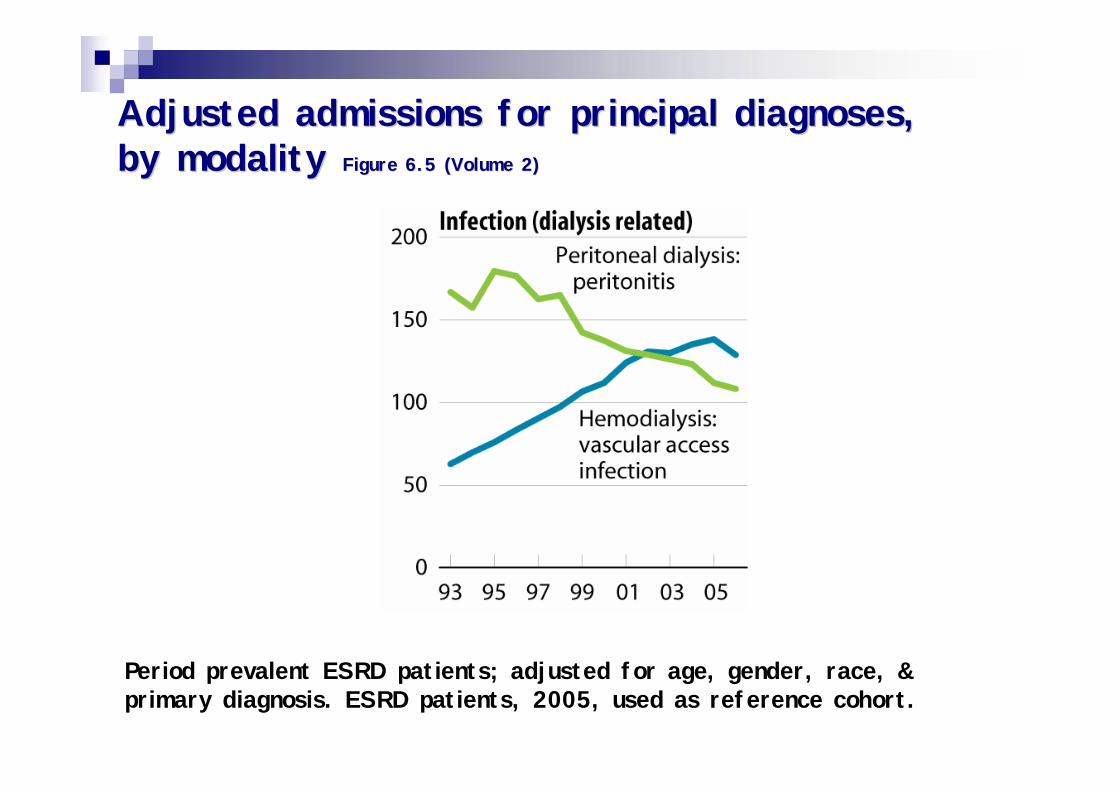
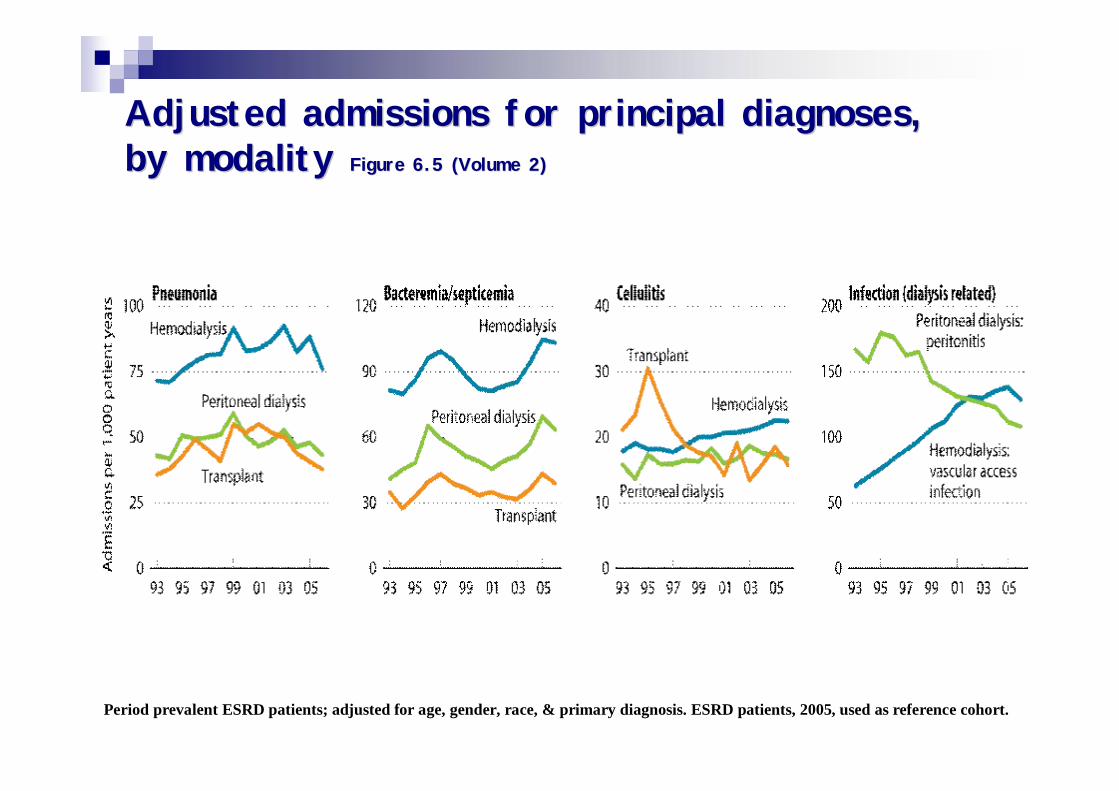
Adjusted admissions for principal diagnoses, Adjusted admissions for principal diagnoses, by modality by modality Figure 6.5 (Volume 2)Figure 6.5 (Volume 2)
Period prevalent ESRD patients; adjusted for age, gender, race, & primary diagnosis. ESRD patients, 2005, used as reference cohort.
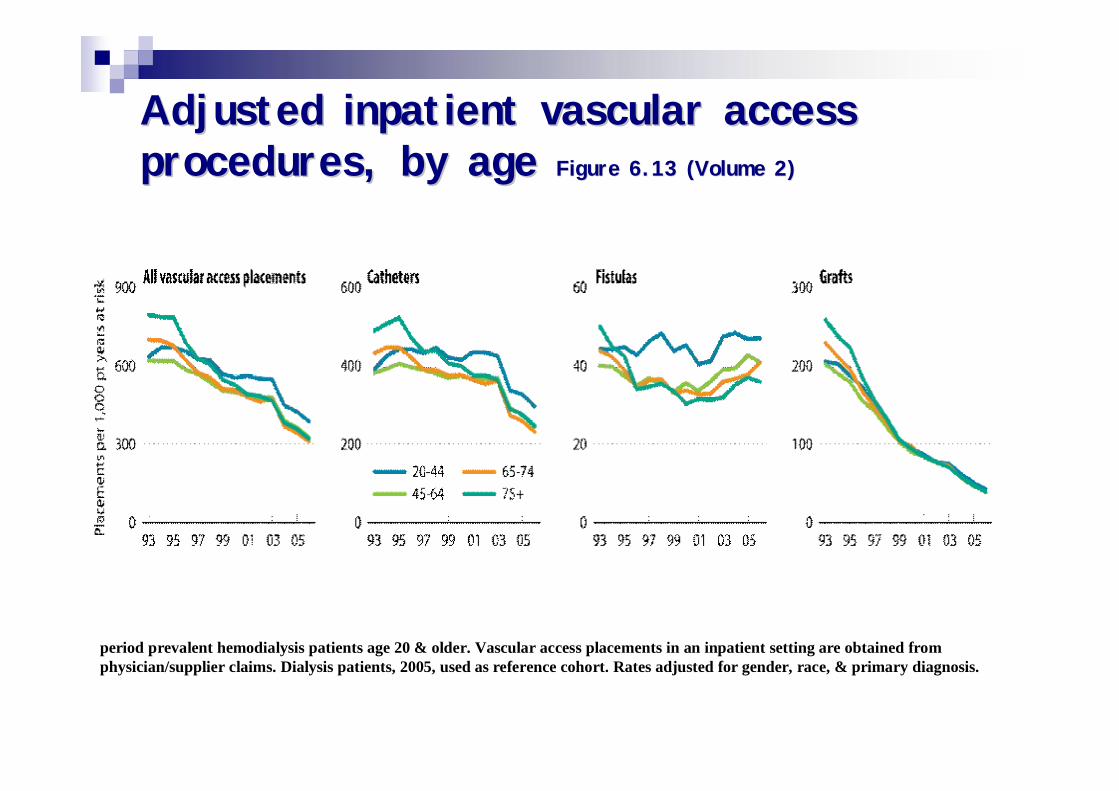
Adjusted inpatient vascular access Adjusted inpatient vascular access procedures, by age procedures, by age Figure 6.13 (Volume 2)Figure 6.13 (Volume 2)
period prevalent hemodialysis patients age 20 & older. Vascular access placements in an inpatient setting are obtained from physician/supplier claims. Dialysis patients, 2005, used as reference cohort. Rates adjusted for gender, race, & primary diagnosis.
ASN
Controversies in Vascular Access
n Moderators:Gerald A. Beathard, MD, PhD, FASNAnatole Besarab, MD
n Arteriovenous Grafts: New Insights Ivan D. Maya, MD
n Does Physical Examination Help in Access Evaluation? Arif Asif, MD
n Do Endovascular Stents Help? Alexander S. Yevzlin, MD
n What is Required to Obtain a Functional Fistula? Aris Q. Urbanes, MD
ASN
Genes impliquésn Heme oxygenase-1 (HO-1)
¨ Chromosome 22q12 ¨ Libère CO et Fer- Action antiproloférative et
antiinflammatoire CMLn NO synthetase eNOS
¨ Dim NO production et augm proliferation des CML¨ Polymorphisme associé avec resténose coronaire
n MTHFR (methylenetetrahydrofolate réductase)¨ Homocysteine¨ Génotype TT X par 3 le risque d’échec de FAV
n Polymorphisme de l’ACE¨ Associé avec thrombose de grafts
Etude en coursEtude en cours
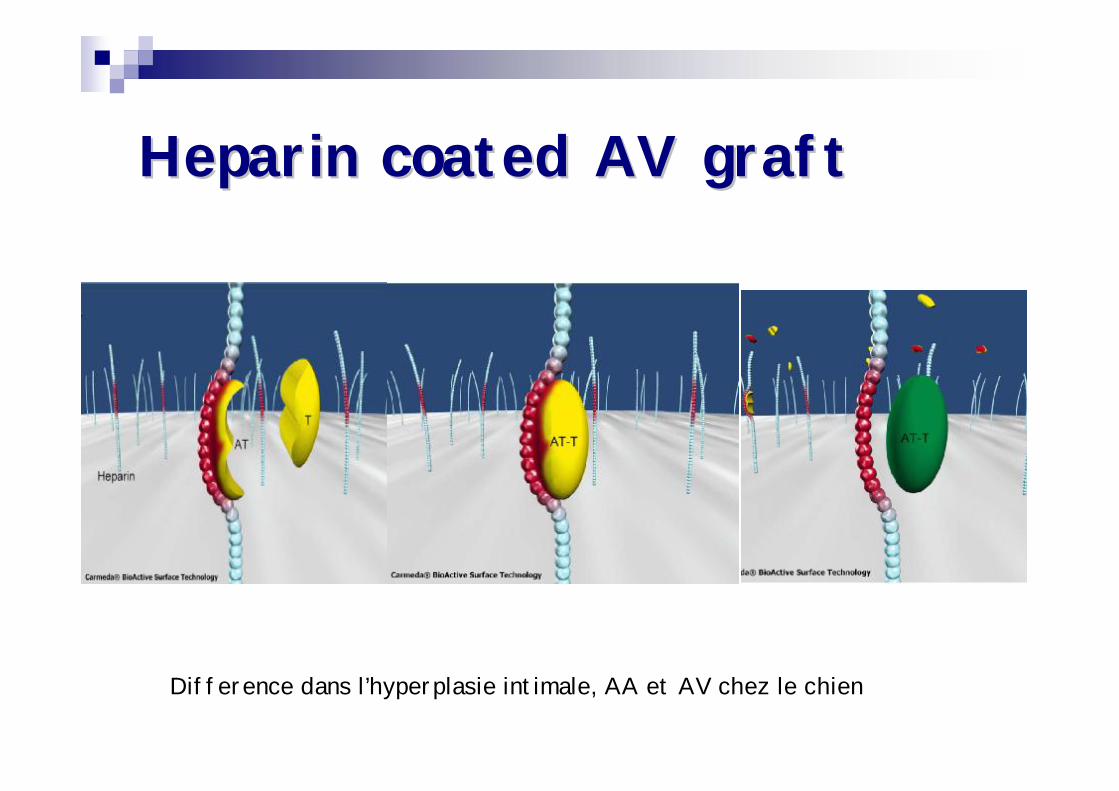
Heparin coated AV graftHeparin coated AV graft
Difference dans l’hyperplasie intimale, AA et AV chez le chien
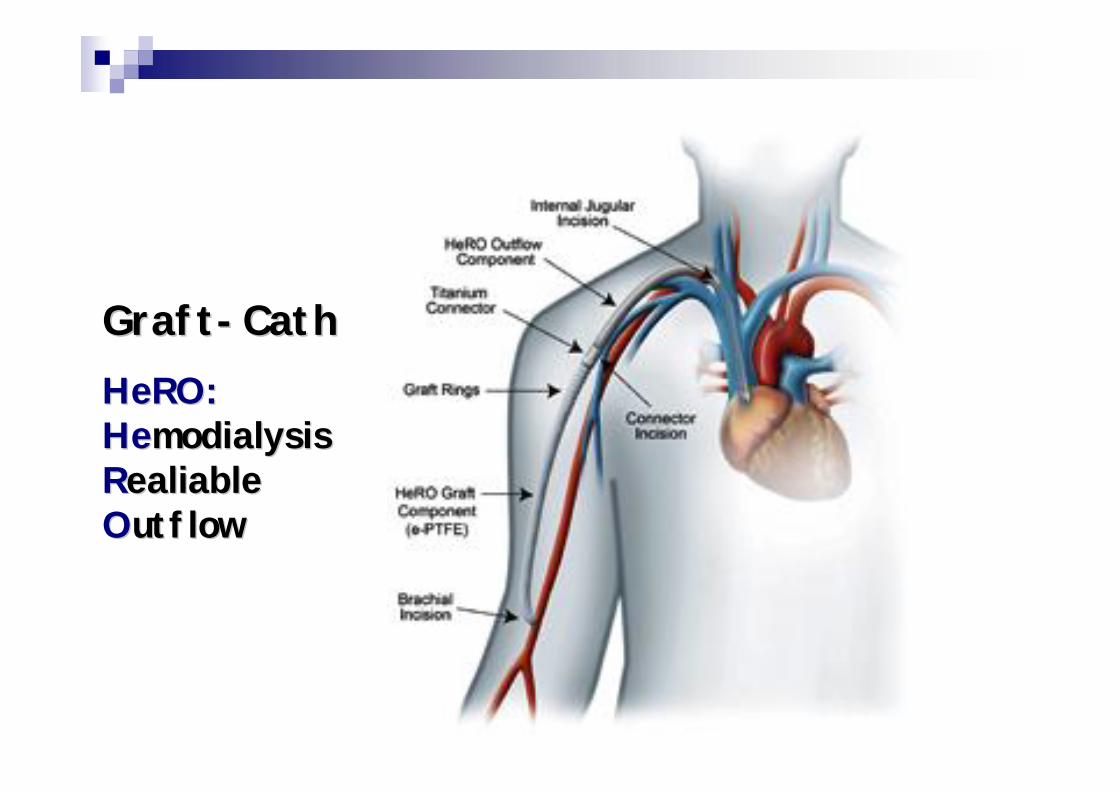
GraftGraft--CathCathHeRO:HeRO:HeHemodialysis modialysis RRealiable ealiable OOutflowutflow

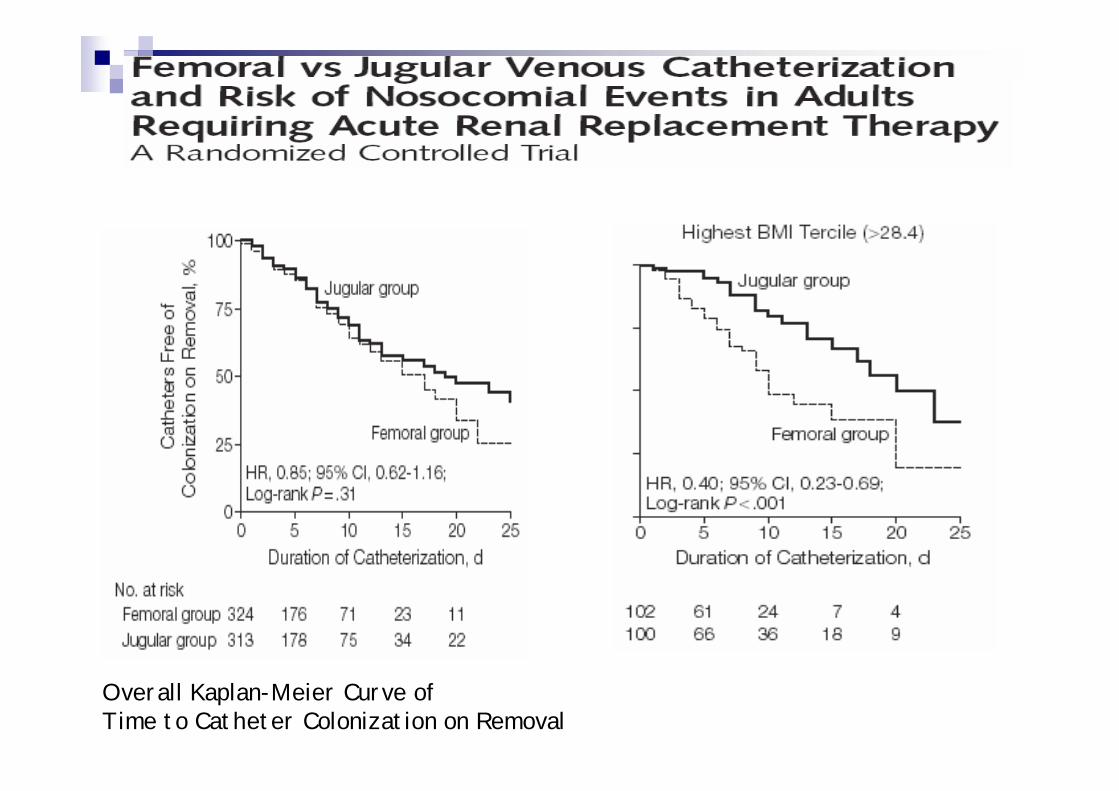
Overall Kaplan-Meier Curve ofTime to Catheter Colonization on Removal
Adjusted admissions for principal diagnoses, Adjusted admissions for principal diagnoses, by modality by modality Figure 6.5 (Volume 2)Figure 6.5 (Volume 2)
Period prevalent ESRD patients; adjusted for age, gender, race, & primary diagnosis. ESRD patients, 2005, used as reference cohort.