insuffisance cardiaque aiguë post-opératoire -...
TRANSCRIPT
Insuffisance cardiaque aiguë post-opératoire
Alexandre Mebazaa Hôpital Lariboisière,
University Paris 7, U942 Inserm; Paris, France
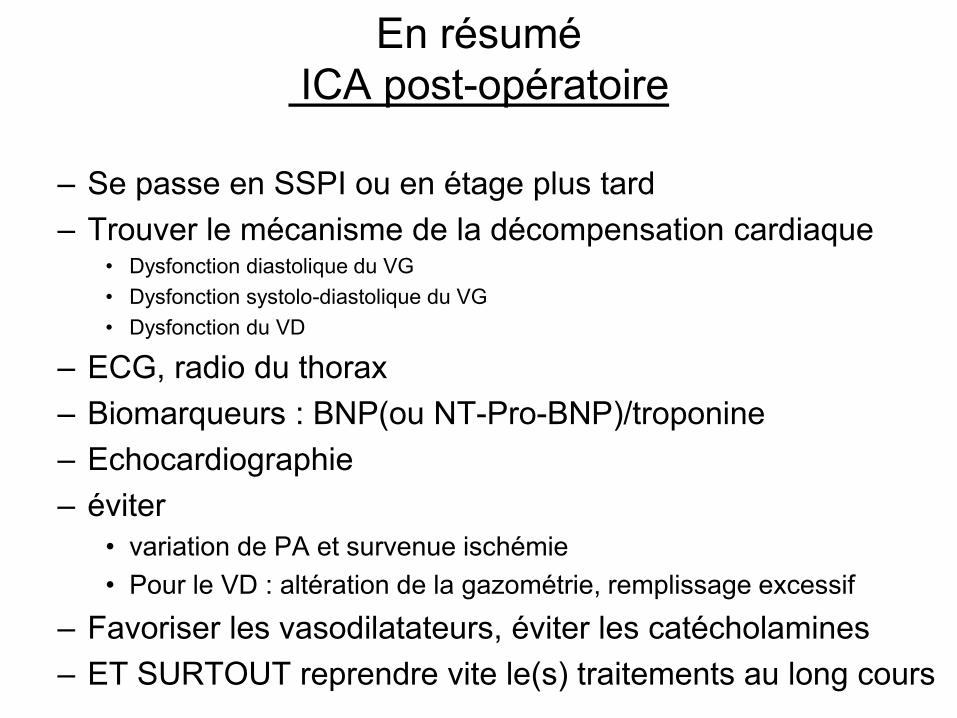
En résumé ICA post-opératoire
– Se passe en SSPI ou en étage plus tard – Trouver le mécanisme de la décompensation cardiaque
• Dysfonction diastolique du VG • Dysfonction systolo-diastolique du VG • Dysfonction du VD
– ECG, radio du thorax – Biomarqueurs : BNP(ou NT-Pro-BNP)/troponine – Echocardiographie – éviter
• variation de PA et survenue ischémie • Pour le VD : altération de la gazométrie, remplissage excessif
– Favoriser les vasodilatateurs, éviter les catécholamines – ET SURTOUT reprendre vite le(s) traitements au long cours

Il existe 3 types d’IC chronique :
IC chronique avec dysfonction VG systolique et diastolique : bas débit circulatoire
IC chronique avec dysfonction diastolique isolée : OAP
IC droite avec ou sans HTAP

Oedème pulmonaire aiguë
ProblèmeVasculaire Aiguë + Dysfonction Diastolique VG
TOUJOURS
Dyspnée + PAS > 140 mmHg
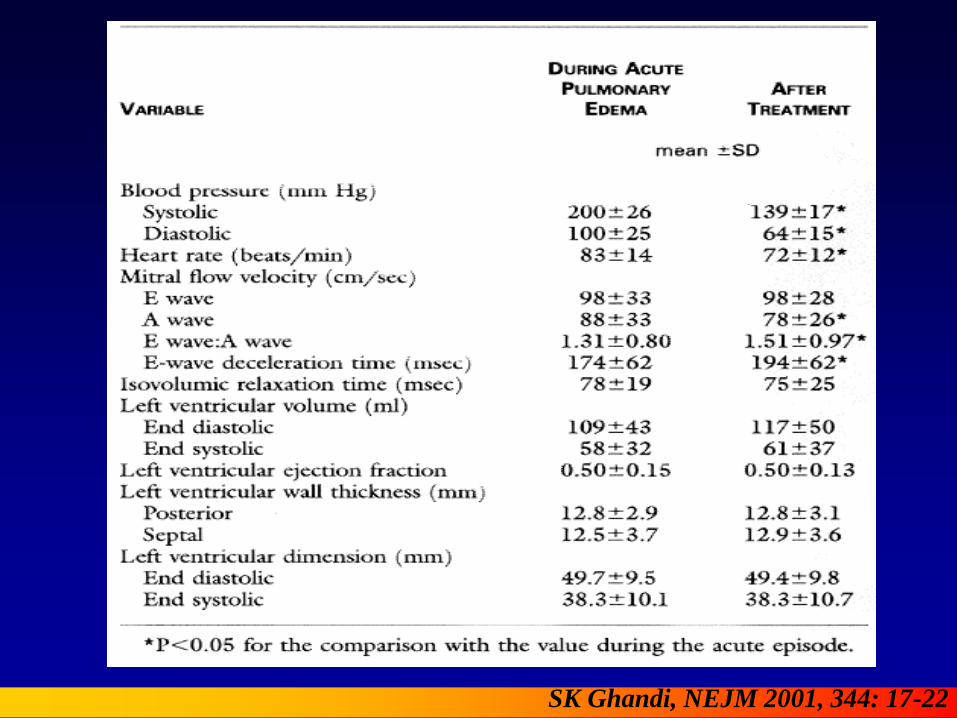
SK Ghandi, NEJM 2001, 344: 17-22
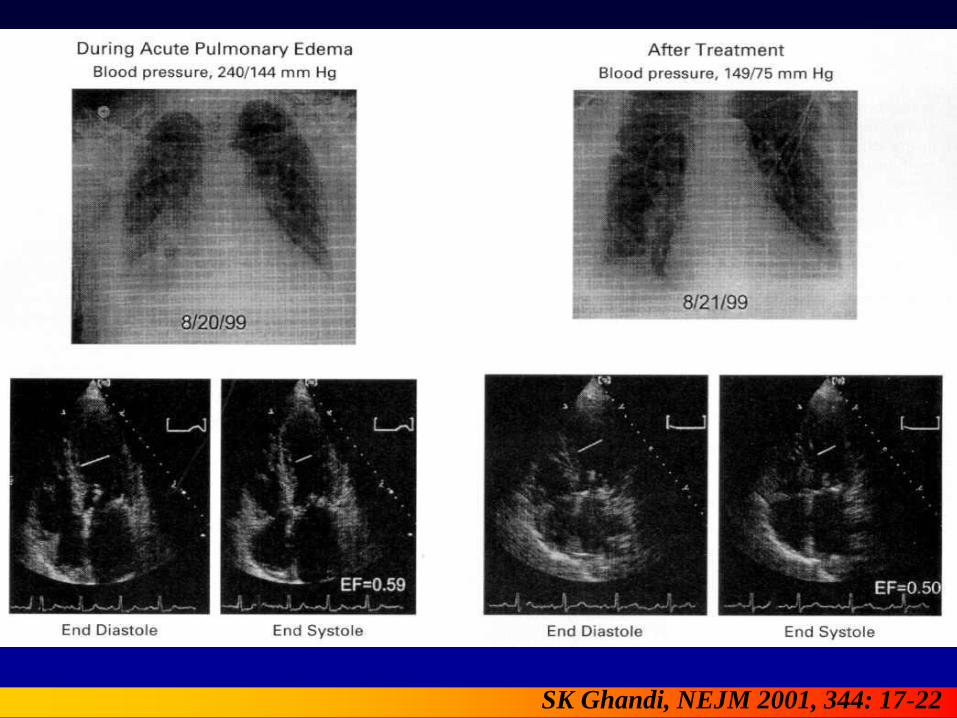
SK Ghandi, NEJM 2001, 344: 17-22

Pathogénie de l’OAP
• Est un signe de congestion pulmonaire = élévation de la PAPo = POG = PTDVG
• Est un signe de dysfonction diastolique et non systolique SK Ghandi, NEJM 2001, 344: 17-22
Pirracchio et al. Br. J. Anaesth.2007; 98: 707-721
L’oedème aiguë du poumon :
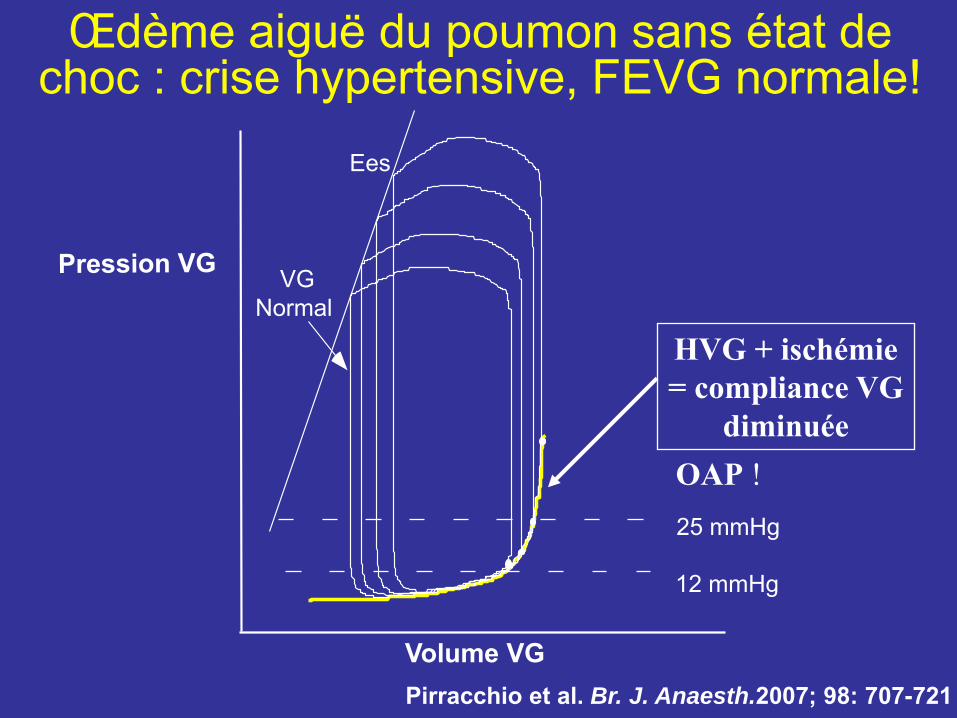
Œdème aiguë du poumon sans état de choc : crise hypertensive, FEVG normale!
VG Normal
12 mmHg
25 mmHg
Volume VG
Ees
HVG + ischémie = compliance VG
diminuée OAP !
Pirracchio et al. Br. J. Anaesth.2007; 98: 707-721
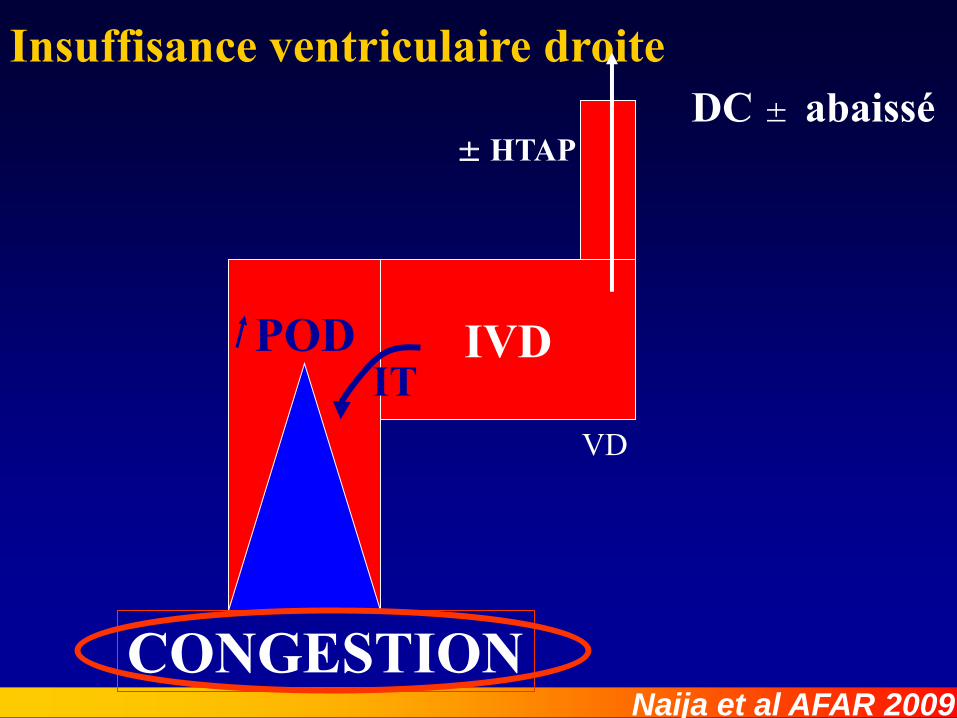
DC ± abaissé Insuffisance ventriculaire droite
IVD
± HTAP
VD
CONGESTION
IT POD
Naija et al AFAR 2009
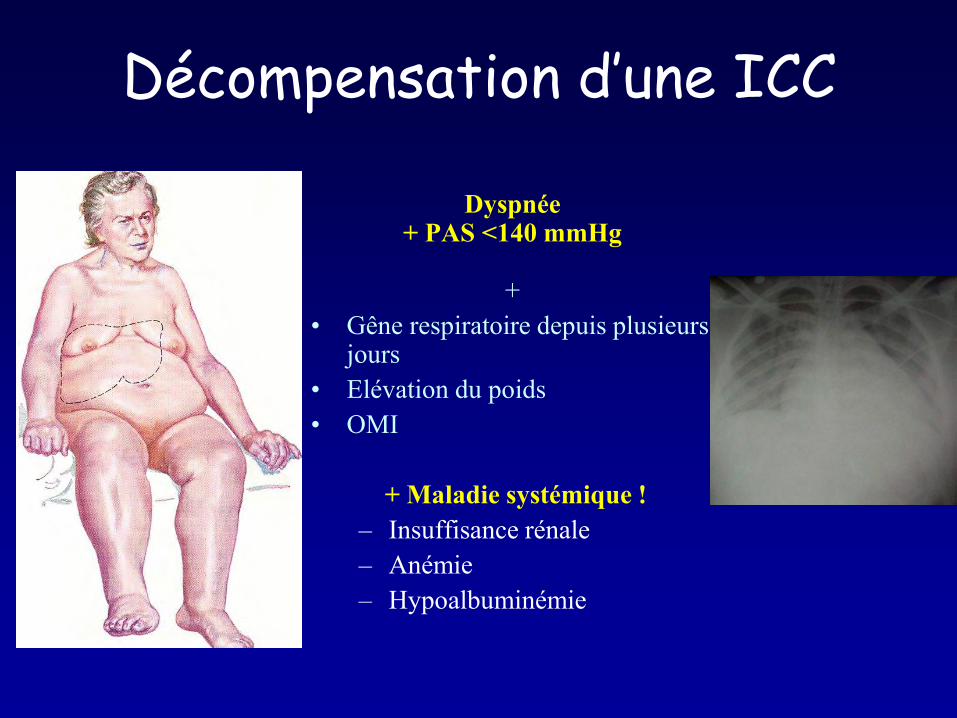
Décompensation d’une ICC
Dyspnée + PAS <140 mmHg
+
• Gêne respiratoire depuis plusieurs jours
• Elévation du poids • OMI
+ Maladie systémique !
– Insuffisance rénale – Anémie – Hypoalbuminémie

Chaudhry E al. Circulation 2007; 116: 1549-15
ADHF
no ADHF
Daily weight change SAU
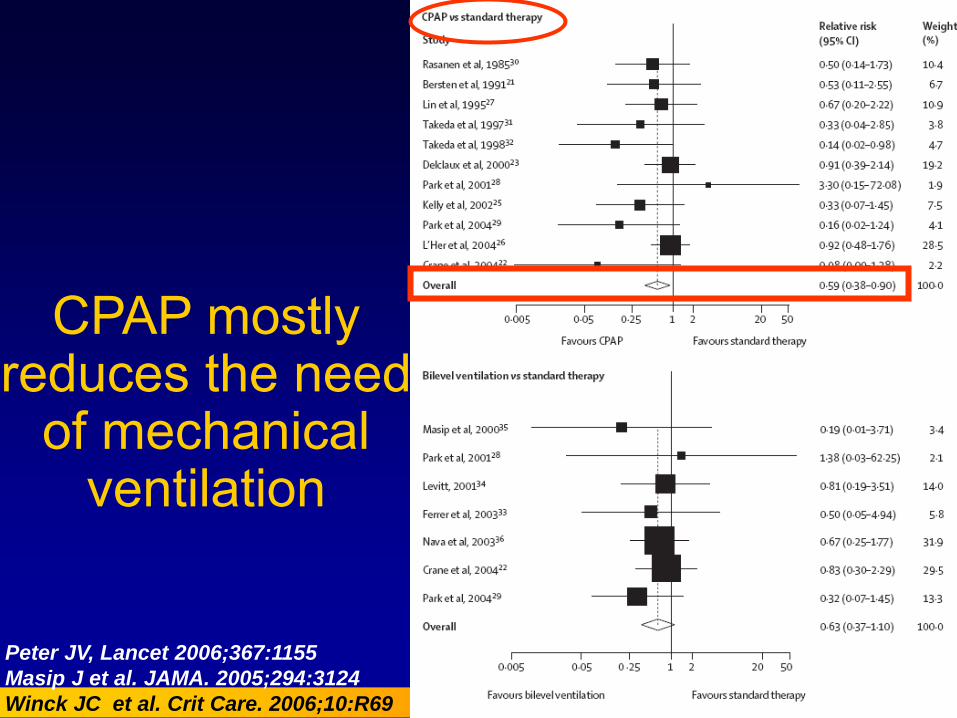
CPAP mostly reduces the need
of mechanical ventilation
Peter JV, Lancet 2006;367:1155
Masip J et al. JAMA. 2005;294:3124
Winck JC et al. Crit Care. 2006;10:R69
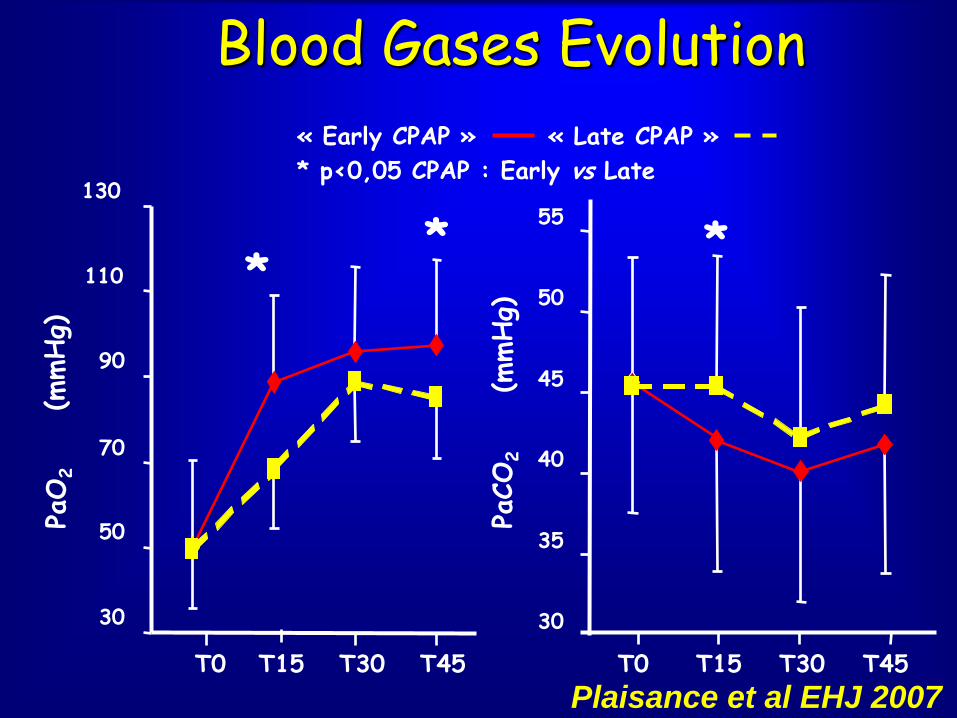
Blood Gases Evolution
30
50
70
90
110
130
T0 T15 T30 T45
PaO
2
(mmHg)
* *
30
35
40
45
50
55
T0 T15 T30 T45
*
PaCO
2
(mmHg)
« Early CPAP » « Late CPAP »
* p<0,05 CPAP : Early vs Late
Plaisance et al EHJ 2007
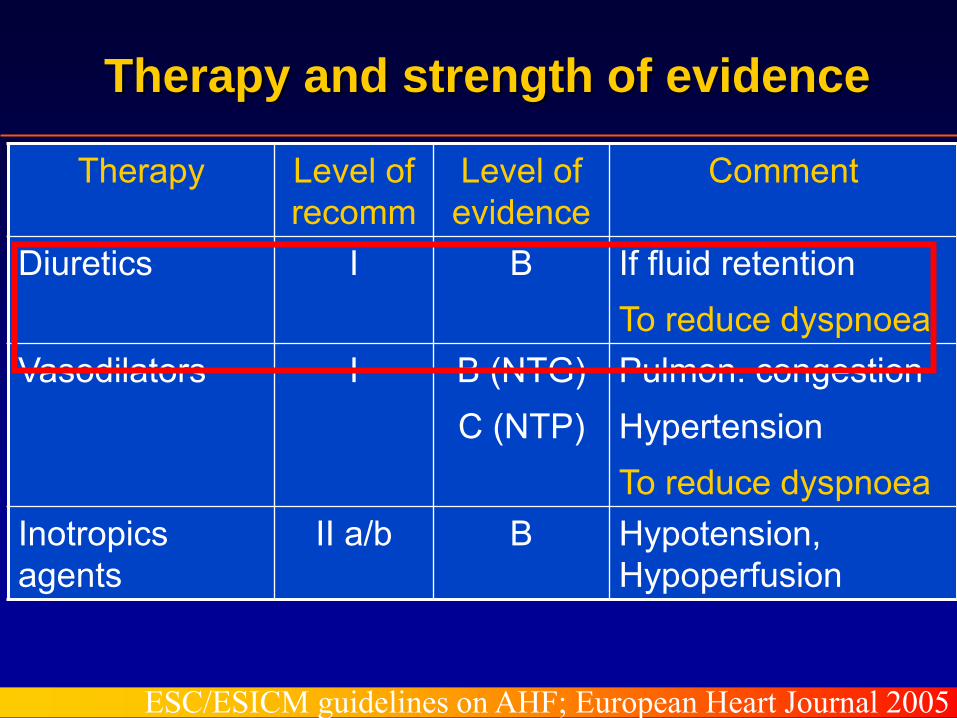
Therapy Level of recomm
Level of evidence
Comment
Diuretics I B If fluid retention To reduce dyspnoea
Vasodilators I B (NTG) C (NTP)
Pulmon. congestion Hypertension To reduce dyspnoea
Inotropics agents
II a/b B Hypotension, Hypoperfusion
Therapy and strength of evidence
ESC/ESICM guidelines on AHF; European Heart Journal 2005
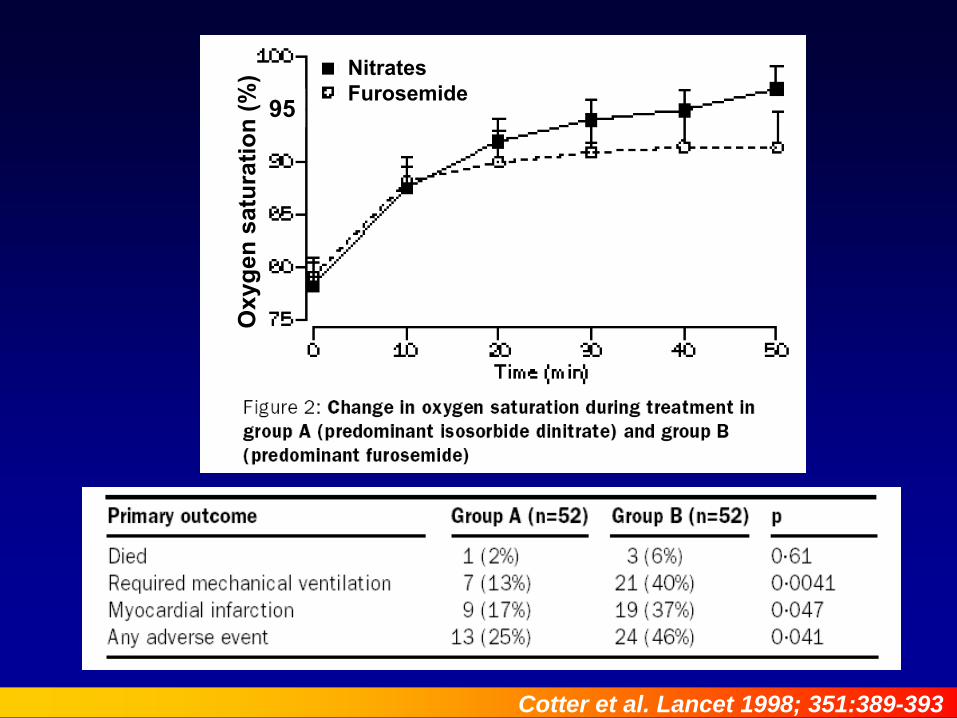
Cotter et al. Lancet 1998; 351:389-393
95
Oxy
gen
satu
ratio
n (%
) Nitrates Furosemide
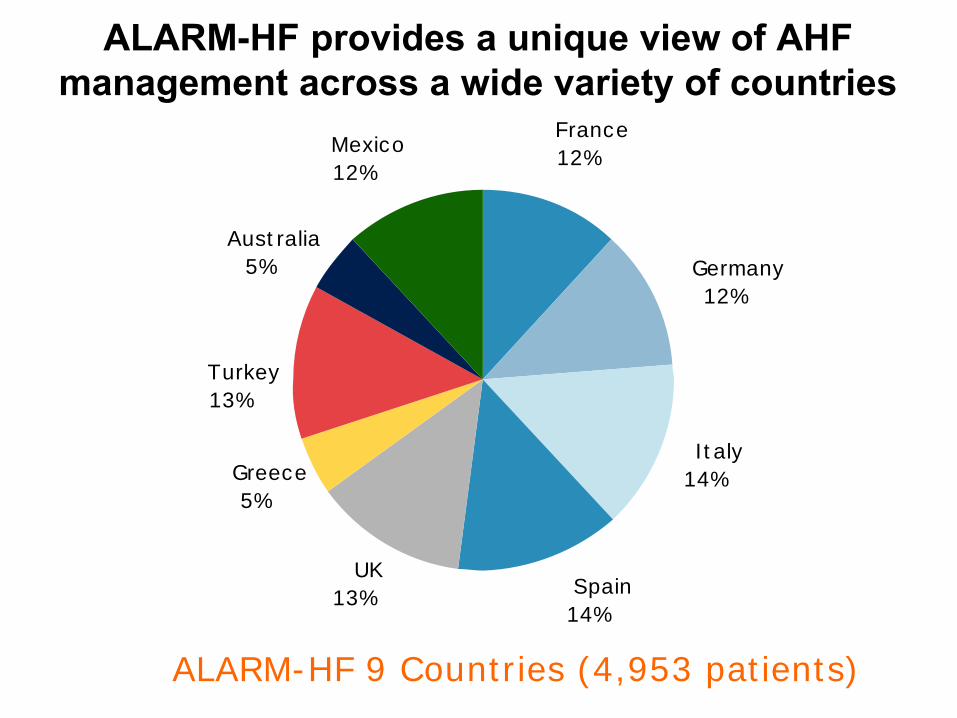
Italy
14%
Spain
14%
UK
13%
Greece
5%
France
12%
Turkey
13%
Germany
12%
Mexico
12%
Australia
5%
ALARM-HF provides a unique view of AHF management across a wide variety of countries
ALARM-HF 9 Countries (4,953 patients)
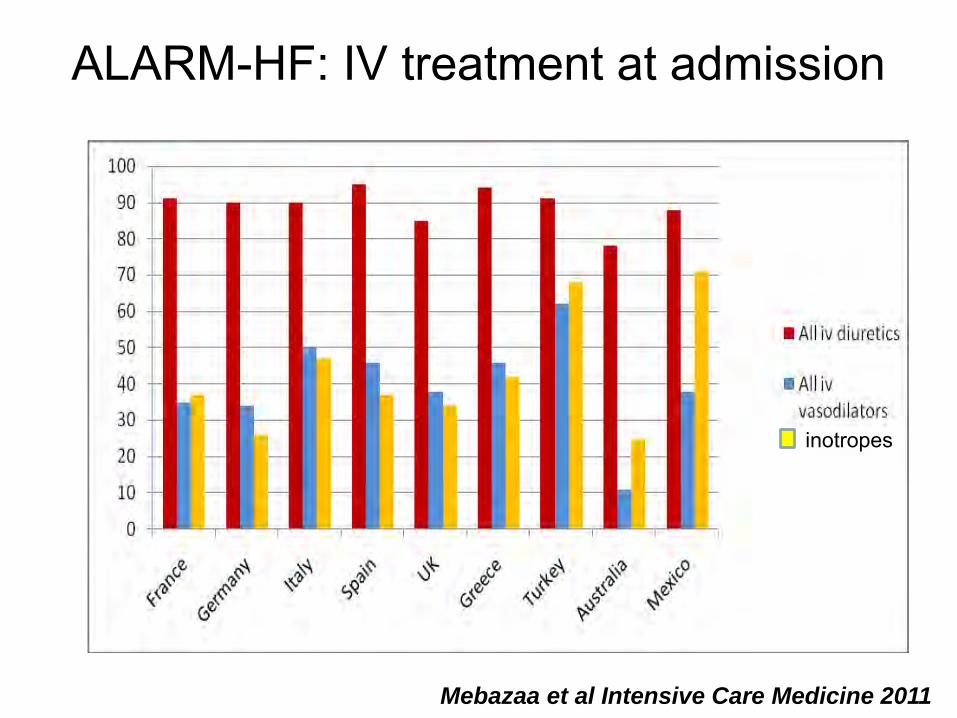
Mebazaa et al Intensive Care Medicine 2011
inotropes
ALARM-HF: IV treatment at admission
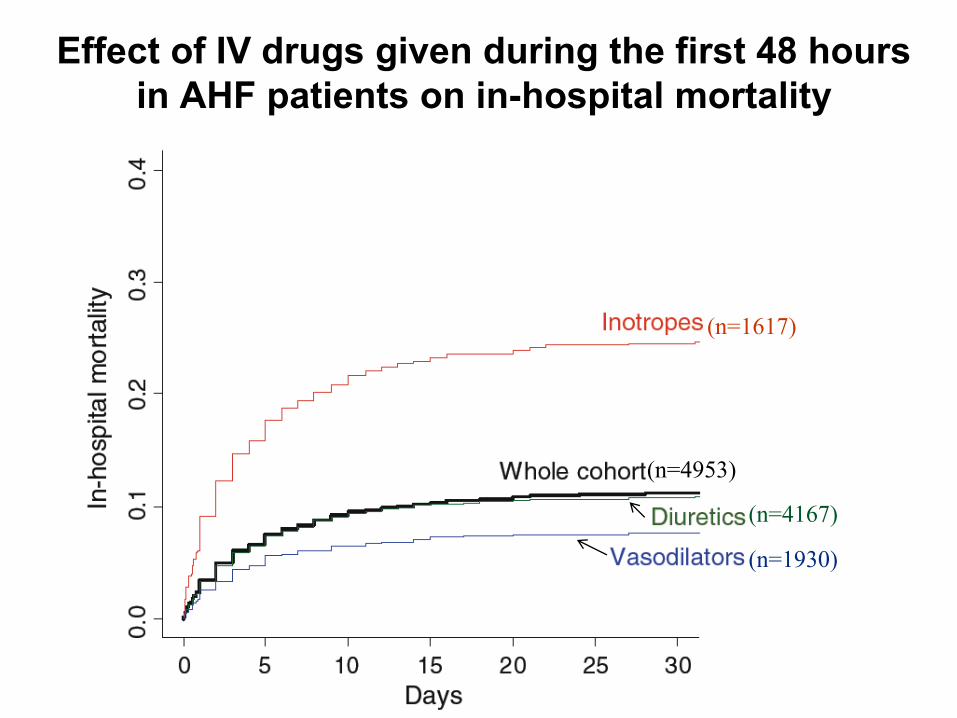
(n=4953)
(n=4167)
(n=1930)
(n=1617)
Effect of IV drugs given during the first 48 hours in AHF patients on in-hospital mortality
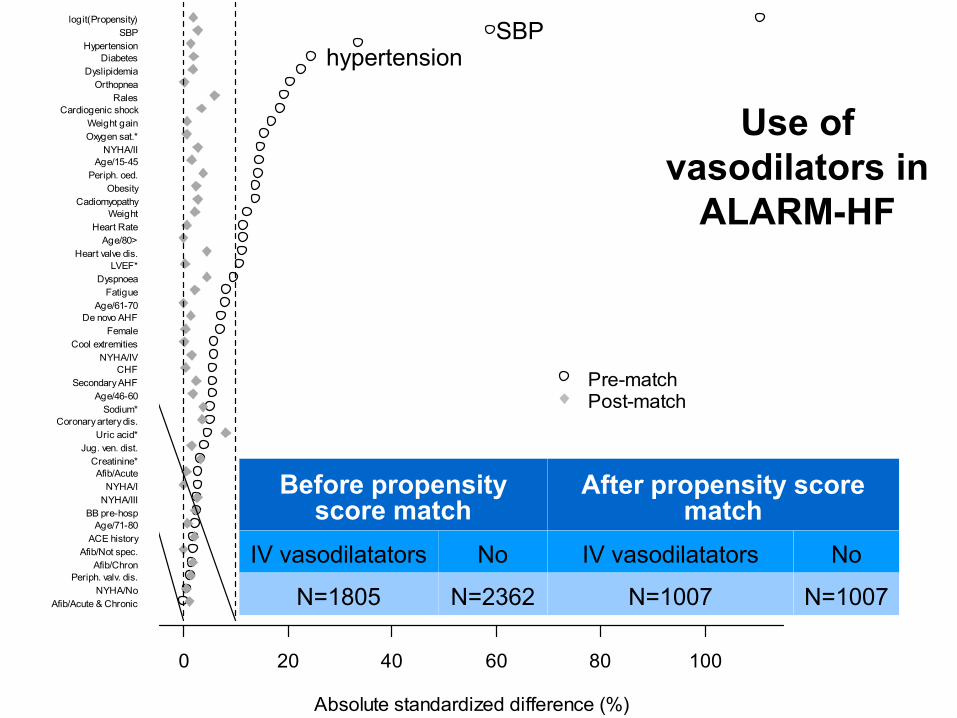
Absolute standardized difference (%)
0 20 40 60 80 100
Afib/Acute & ChronicNYHA/No
Periph. valv. dis.Afib/Chron
Afib/Not spec.ACE history
Age/71-80BB pre-hosp
NYHA/IIINYHA/I
Afib/AcuteCreatinine*
Jug. ven. dist.Uric acid*
Coronary artery dis.Sodium*
Age/46-60Secondary AHF
CHFNYHA/IV
Cool extremitiesFemale
De novo AHFAge/61-70
FatigueDyspnoea
LVEF*Heart valve dis.
Age/80>Heart Rate
WeightCadiomyopathy
ObesityPeriph. oed.
Age/15-45NYHA/II
Oxygen sat.*Weight gain
Cardiogenic shockRales
OrthopneaDyslipidemia
DiabetesHypertension
SBPlogit(Propensity)
Pre-matchPost-match
SBP hypertension
Before propensity score match
After propensity score match
IV vasodilatators No IV vasodilatators No
N=1805 N=2362 N=1007 N=1007
Use of vasodilators in
ALARM-HF
Results • IV diuretics and IV vasodilators were started at a median
of 0.5 [0.0 – 1.0] hour and 0.5 [0.0 – 2] hour respectively after admission.
• IV vasodilators were quasi-exclusively nitrates: nitroglycerine in 76 % and isosorbite dinitrate 19 %
• In-hospital mortality: - Before matching 7.6 vs 14.2 % with and without vasoD - After matching 7.8 versus 11 % with and without vasoD
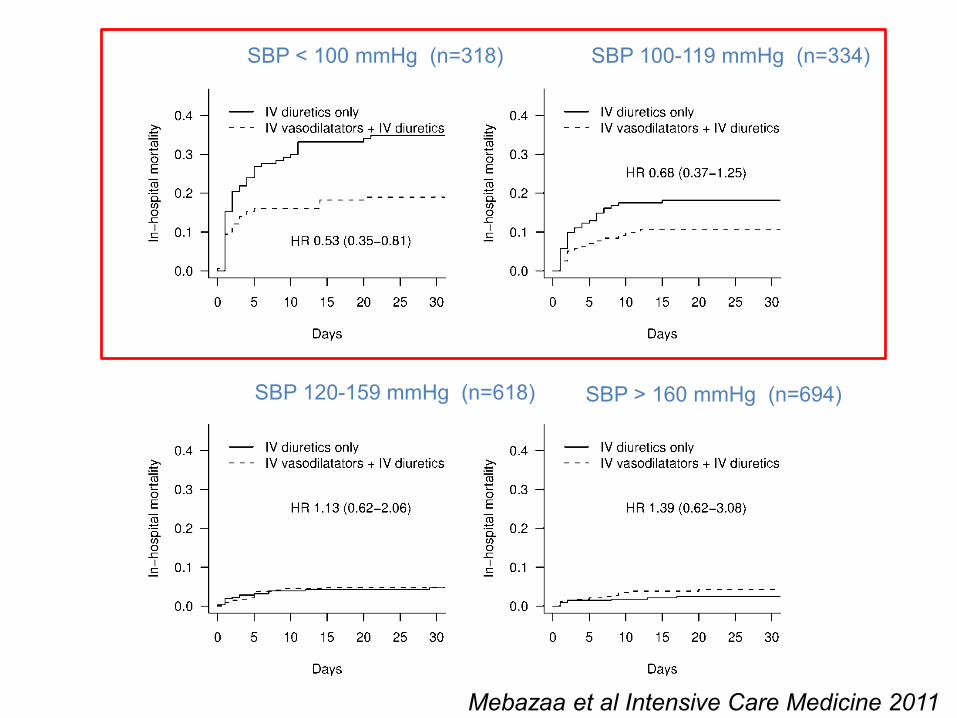
SBP < 100 mmHg (n=318) SBP 100-119 mmHg (n=334)
SBP 120-159 mmHg (n=618) SBP > 160 mmHg (n=694)
Mebazaa et al Intensive Care Medicine 2011

Co-Primary outcome: 30-day all-cause mortality or HF rehospitalization (n=6836)
10.1
4.0
6.1
Hazard Ratio 0.93 (95% CI: 0.8,1.08)
9.4
3.6
6.0
Placebo Nesiritide
HF Rehospitalization
30-day Death/HF Rehospitalization
30-day Death
0
2
4
6
8
10
12
Risk Diff (95 % CI) -0.7 (-2.1; 0.7) -0.4 (-1.3; 0.5) -0.1 (-1.2; 1.0)
%
P=0.31
Hernandez AHA 2010
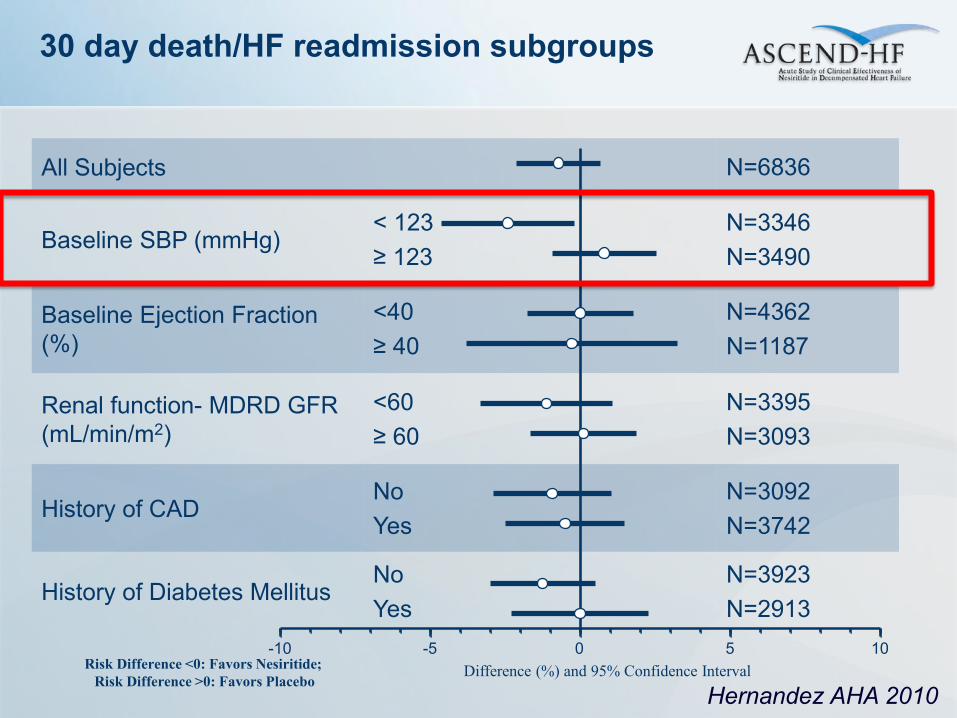
All Subjects N=6836
Baseline SBP (mmHg) < 123 ≥ 123
N=3346 N=3490
Baseline Ejection Fraction (%)
<40 ≥ 40
N=4362 N=1187
Renal function- MDRD GFR (mL/min/m2)
<60 ≥ 60
N=3395 N=3093
History of CAD No Yes
N=3092 N=3742
History of Diabetes Mellitus No Yes
N=3923 N=2913
-10 -5 0 5 10
30 day death/HF readmission subgroups
Difference (%) and 95% Confidence Interval Risk Difference <0: Favors Nesiritide;
Risk Difference >0: Favors Placebo
Hernandez AHA 2010
30/08/09 26
Absolute standardized difference (%)
0 20 40 60 80 100 120
ObesityAfib/AcuteAfib/Chron
DyslipidemiaCoronary artery dis.
Afib/Not spec.OrthopneaAge/61-70
Afib/Acute & ChronicCHF
DyspnoeaPeriph. valv. dis.Heart valve dis.
NYHA/IUric acid*
RalesFatigue
DiabetesCreatinine*
FemaleHypertension
Sodium*De novo AHF
CadiomyopathyAge/71-80
Jug. ven. dist.BB pre-hospPeriph. oed.
WeightAge/15-45Heart Rate
NYHA/IINYHA/IV
Age/46-60Weight gain
NYHA/NoOxygen sat.*
Age/80>Secondary AHF
ACE historyNYHA/III
LVEF*Cool extremities
Cardiogenic shockSBP
logit(Propensity)
Pre-matchPost-match
After propens
Before propensity score match
After propensity score match
IV inotrope/ vasopressor
No IV inotrope/ vasopressor
No
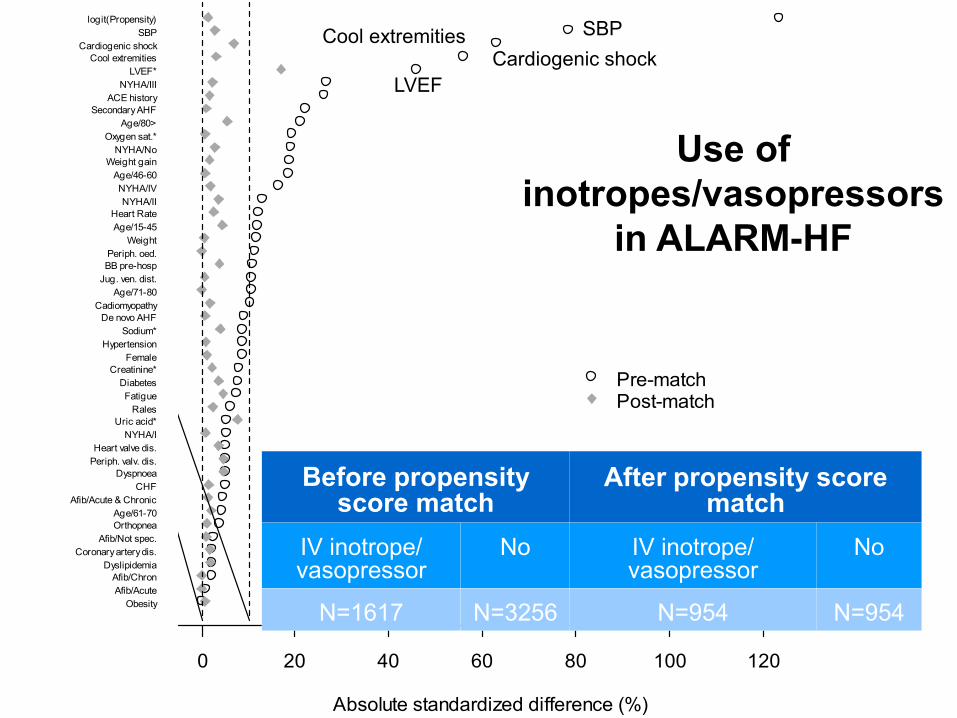
N=1617 N=3256 N=954 N=954
Use of inotropes/vasopressors
in ALARM-HF
SBP Cardiogenic shock
LVEF
Cool extremities

0 5 10 15 20 25 30
0.0
0.1
0.2
0.3
0.4
0.5
0.6
Days
In-h
ospi
tal m
orta
lity
Whole cohort
Dopamine Dobutamine
Epinephrine
Norepinephrine
Levosimendan
Diuretics
Vasodilatators
Post-discharge treatement after discharge from Acute Heart Failure
0,4
0,5
0,6
0,7
0,8
0,9
1,0
0 30 60 90 120 150 180
Days Since Start of Study Drug Infusion
Prob
abili
ty o
f Sur
vivi
ng LevosimendanDobutamine
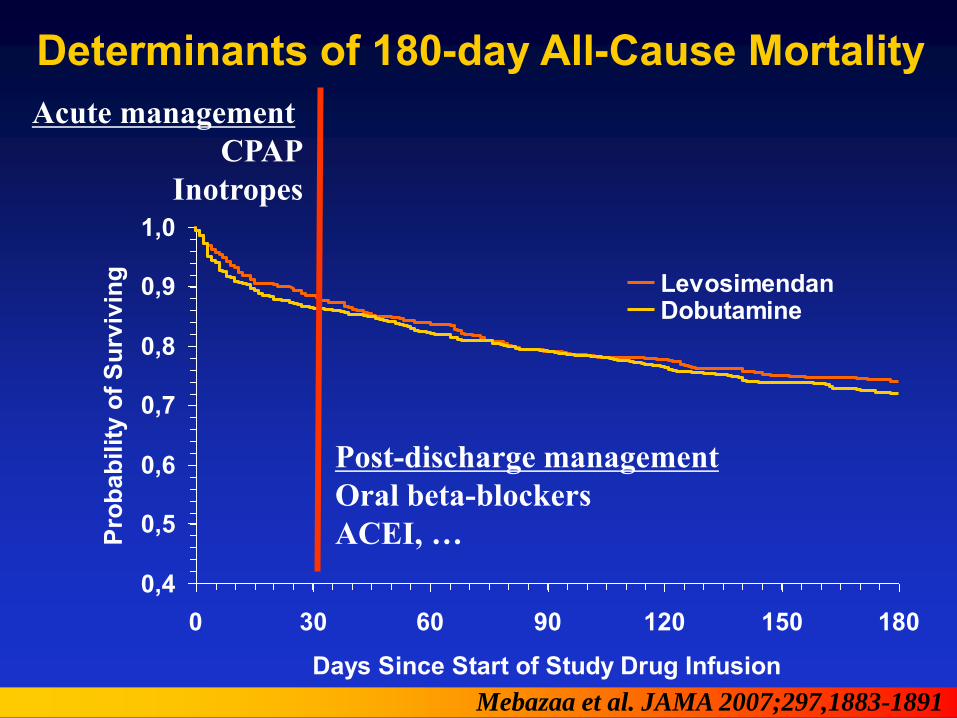
Determinants of 180-day All-Cause Mortality
Mebazaa et al. JAMA 2007;297,1883-1891
Acute management CPAP
Inotropes
Post-discharge management Oral beta-blockers ACEI, …
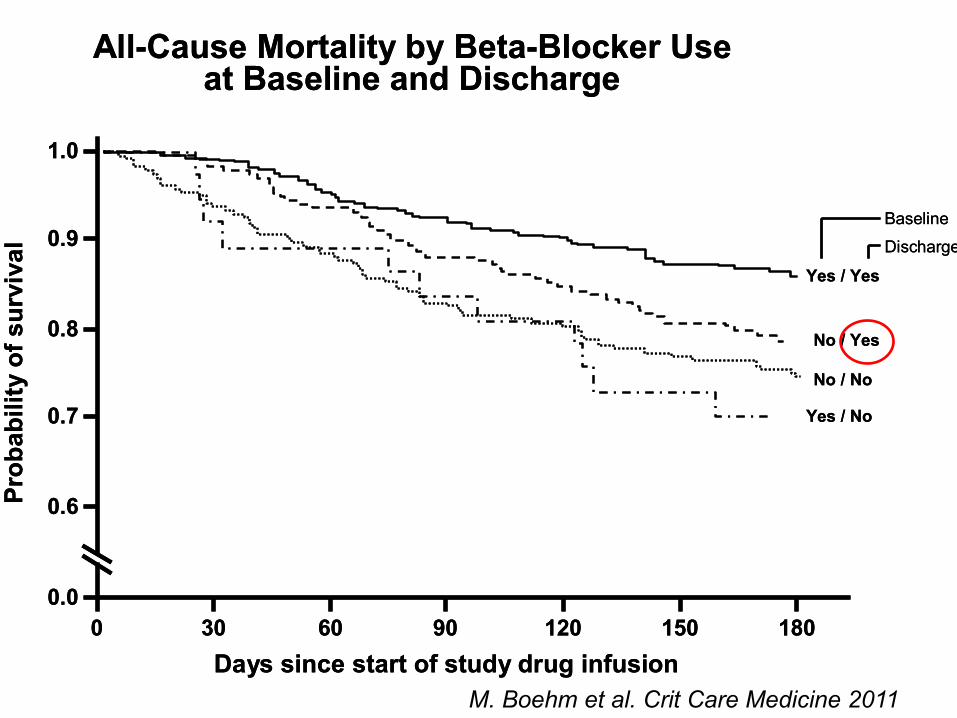
Fig. 2
All-Cause Mortality by Beta-Blocker Useat Baseline and Discharge
0.0
0.6Prob
abili
tyof
sur
viva
l
0 30Days since start of study drug infusion
0.7
0.8
0.9
1.0
60 90 120 150 180
No / No
No / Yes
Yes / Yes
Yes / No
Baseline
Discharge
Fig. 2
All-Cause Mortality by Beta-Blocker Useat Baseline and Discharge
0.0
0.6Prob
abili
tyof
sur
viva
l
0 30Days since start of study drug infusion
0.7
0.8
0.9
1.0
60 90 120 150 180
No / No
No / Yes
Yes / Yes
Yes / No
Baseline
Discharge
M. Boehm et al. Crit Care Medicine 2011
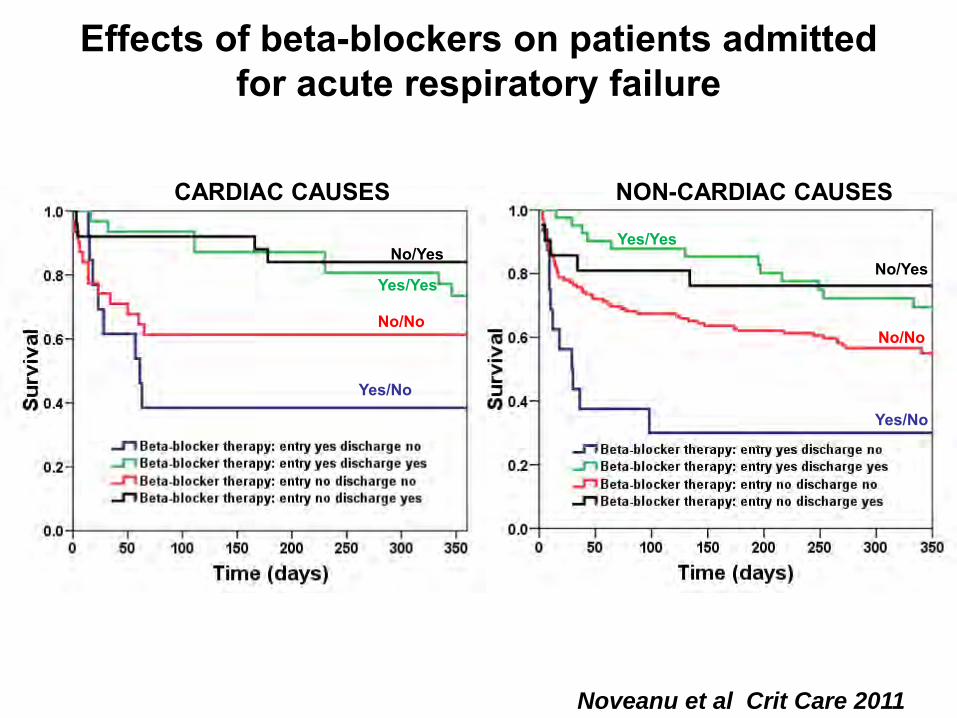
Effects of beta-blockers on patients admitted for acute respiratory failure
Yes/No
No/No
No/Yes
Yes/Yes
Yes/Yes
No/Yes
No/No
Yes/No
CARDIAC CAUSES NON-CARDIAC CAUSES
Noveanu et al Crit Care 2011
Mebazaa et al. Critical Care Medicine, 2008, Suppl 36:129-139
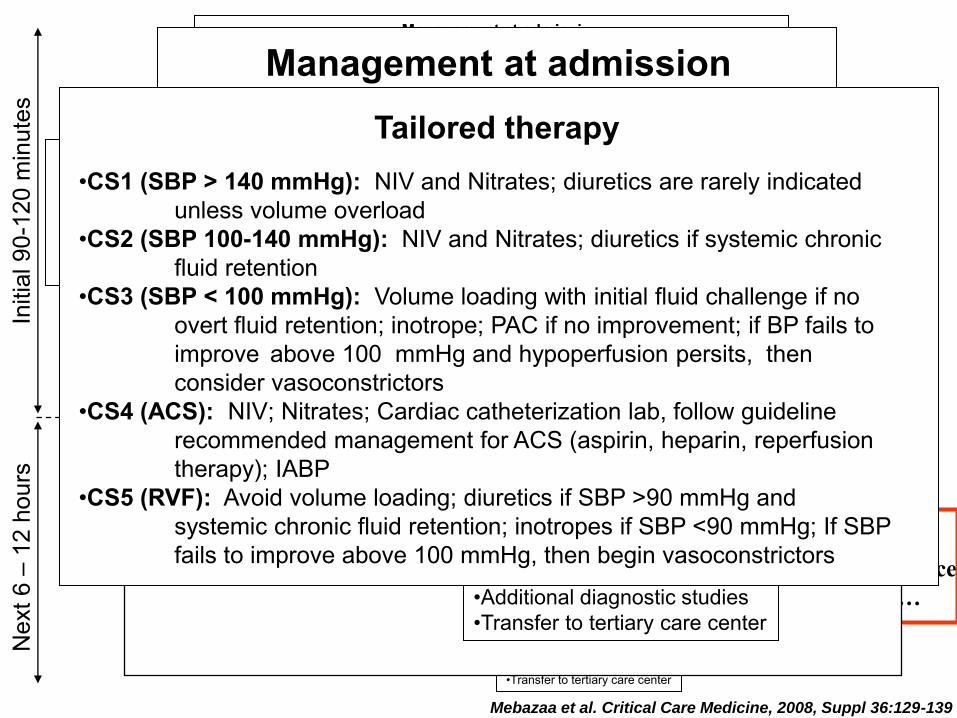
•Non-invasive monitoring (SaO2, BP, temperature) •O2 •Non-invasive ventilation (NIV) as indicated •Physical exam
Management at admission •Lab tests •BNP or NT-pro BNP when diagnosis is uncertain •ECG •Chest X-Ray
Tailored therapy •CS1 (SBP > 140 mmHg): NIV and Nitrates; diuretics are rarely indicated unless volume overload •CS2 (SBP 100-140 mmHg): NIV and Nitrates; diuretics if systemic chronic fluid retention •CS3 (SBP < 100 mmHg): Volume loading with initial fluid challenge if no overt fluid retention; inotrope; PAC if no improvement; if BP fails to improve above 100 mmHg and hypoperfusion persits, then consider vasoconstrictors •CS4 (ACS): NIV; Nitrates; Cardiac catheterization lab, follow guideline recommended management for ACS (aspirin, heparin, reperfusion therapy); IABP •CS5 (RVF): Avoid volume loading; diuretics if SBP >90 mmHg and systemic chronic fluid retention; inotropes if SBP <90 mmHg; If SBP fails to improve above 100 mmHg, then begin vasoconstrictors
Initi
al 9
0-12
0 m
inut
es
•CCU/ICU admission •ECHO if not recently done •Central or arterial line •Additional diagnostic studies •Transfer to tertiary care center
Nex
t 6 –
12
hour
s
Mebazaa et al. Critical Care Medicine, 2008, Suppl 36:129-139
At discharge: Please keep or introduce oral b-blockers etc…
•Non-invasive monitoring • (SaO2, BP, temperature) •O2 •NIV as indicated •Physical exam
Management at admission •Lab tests •BNP or NT-pro BNP •ECG •Chest X-Ray
Treatment Objectives •Decrease dyspnea •Improve well being •Decrease heart rate
•Urine output >0.5 ml/kg/h •Maintain/improve SBP •Restore adequate perfusion
•If dyspnea persists • if SBP <100 mmHg • Organ hypoperfusion • Right ventricular Failure •SaO2 <90% despite O2
•Stay in the ER/Ward
Reassess frequently Clinical and Physical Exam
Treatment Objectives •Decrease dyspnea •Improve well being •Decrease heart rate
•Urine output >0.5 ml/kg/h •Maintain/improve SBP •Restore adequate perfusion •If dyspnea persists • if SBP <100 mmHg
• Organ hypoperfusion • Right ventricular Failure •SaO2 <90% despite O2
•Stay in the ER/Ward
•CCU/ICU admission •ECHO if not recently done •Central or arterial line •Additional diagnostic studies •Transfer to tertiary care center
Reassess frequently Clinical and Physical Exam
Tailored therapy •CS1 (SBP > 140 mmHg): NIV and Nitrates; diuretics are rarely indicated unless volume overload •CS2 (SBP 100-140 mmHg): NIV and Nitrates; diuretics if systemic chronic fluid retention •CS3 (SBP < 100 mmHg): Volume loading with initial fluid challenge if no overt fluid retention; inotrope; PAC if no improvement; if BP fails to improve above 100 mmHg and hypoperfusion persits, then consider vasoconstrictors •CS4 (ACS): NIV; Nitrates; Cardiac catheterization lab, follow guideline recommended management for ACS (aspirin, heparin, reperfusion therapy); IABP •CS5 (RVF): Avoid volume loading; diuretics if SBP >90 mmHg and systemic chronic fluid retention; inotropes if SBP <90 mmHg; If SBP fails to improve above 100 mmHg, then begin vasoconstrictors
Autres nouveautés ?
-Biomarqueurs du diagnostic de l’ICA -Mortalité de l’ICA
Sen
sitiv
ity
BNP (ELISA) QSOX-1 (MS)
0 1
0
1 BNP (ELISA) QSOX-1 (MS)
Sen
sitiv
ity
0 1
0
1
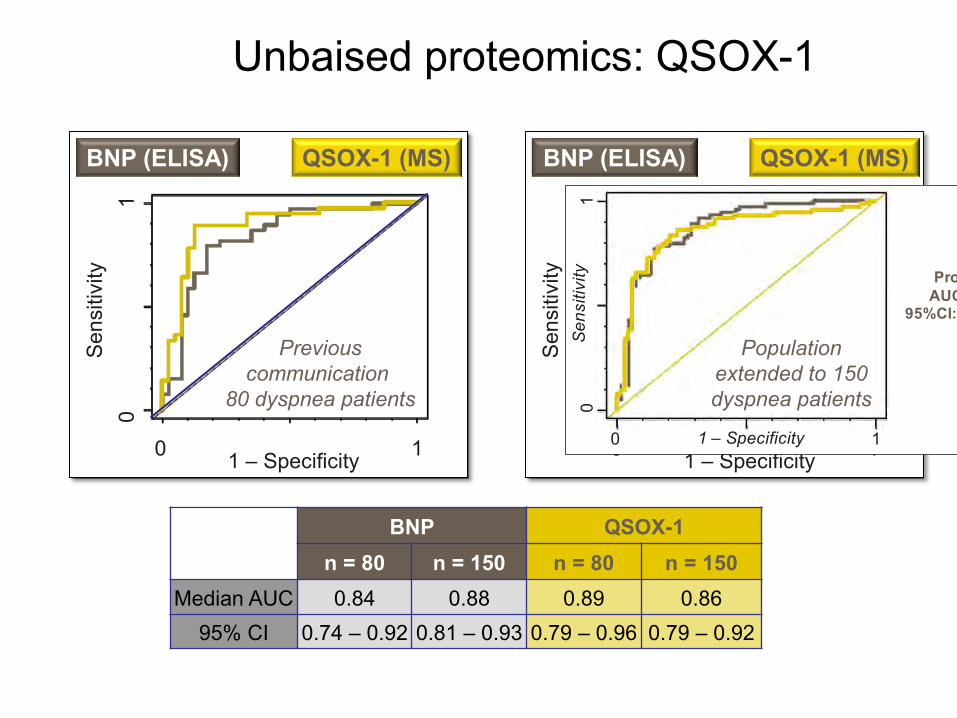
BNP QSOX-1 n = 80 n = 150 n = 80 n = 150
Median AUC 0.84 0.88 0.89 0.86 95% CI 0.74 – 0.92 0.81 – 0.93 0.79 – 0.96 0.79 – 0.92
1 – Specificity 1 – Specificity
Unbaised proteomics: QSOX-1
BNPAUC: 0.88
95%CI: 0.81-0.93
0
1
Sen
sitiv
ity
0 11 – Specificity
Pro-M22AUC: 0.86
95%CI: 0.79-0.92
Previous communication
80 dyspnea patients
Population extended to 150 dyspnea patients
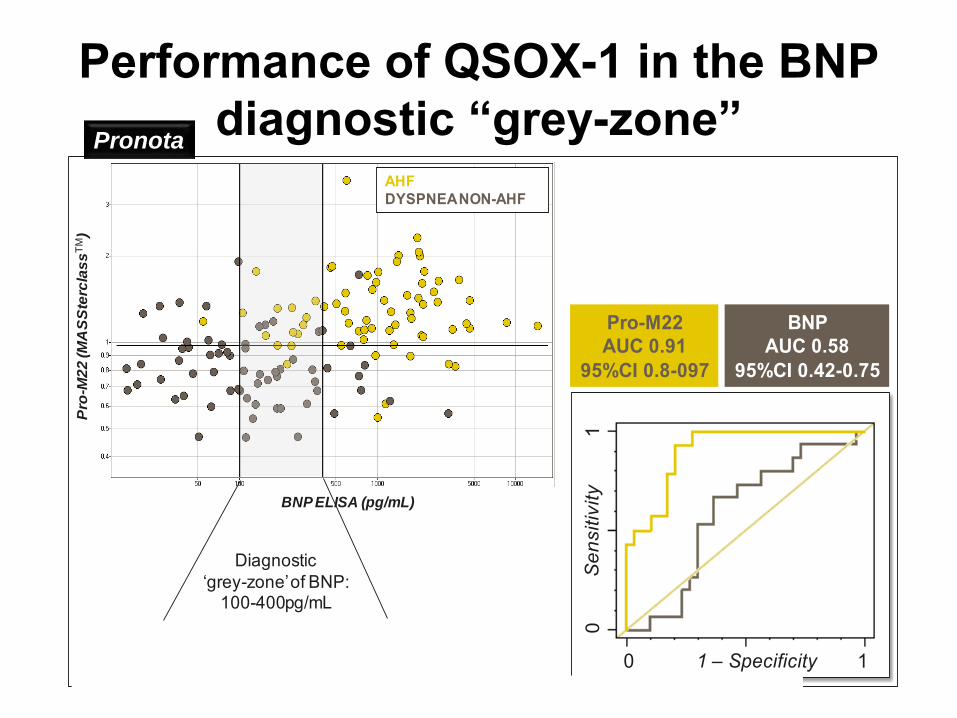
Performance of QSOX-1 in the BNP diagnostic “grey-zone”
0 1
0
1
Pro-M22AUC 0.91
95%CI 0.8-097
BNPAUC 0.58
95%CI 0.42-0.75
BNP ELISA (pg/mL)
Pro
-M2
2 (M
AS
Ste
rcla
ss
TM)
AHFDYSPNEA NON-AHF
Sen
sitiv
ity
1 – Specificity
Diagnostic ‘grey-zone’ of BNP:
100-400pg/mL
Pronota
QSOX-1

0
20
40
60
80
100
1201
98
7
19
88
19
89
19
90
19
91
19
92
19
93
19
94
19
95
19
96
19
97
19
98
19
99
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
Total F rance
Total G reece
Total F inland
Total S weden
Total S pain
Standardized death rates per 100 000 hab
S Laribi et al.

En résumé ICA post-opératoire
Se passe en SSPI ou en étage plus tard Trouver le mécanisme de la décompensation cardiaque
Dysfonction diastolique du VG Dysfonction systolo-diastolique du VG Dysfonction du VD
ECG, radio du thorax Biomarqueurs : BNP(ou NT-Pro-BNP)/troponine Echocardiographie éviter
variation de PA et survenue ischémie Pour le VD : altération de la gazométrie, remplissage excessif
Favoriser les vasodilatateurs, éviter les catécholamines ET SURTOUT reprendre vite le(s) traitements au long cours