consiglio nazionale delle ricerche - emedea.it · preliminary meg studies on healthy volunteers....
TRANSCRIPT
Consiglio Nazionale delle RicercheIstituto per l’Energetica e le Interfasi – Lecco
Nuove tecnologie per ortesiSimone Pittaccio, Ph.D.
HIGH-TECH IN NEURORIABILITAZIONE INFANTILE: TRAGUARDI E SFIDEIRCCS E. Medea-Associazione La Nostra Famiglia, 24-25 Settembre 2015

Indice
2
① Breve introduzione alle leghe a memoria di forma
② Applicazione 1: Terapie di riposizionamento
③ Applicazione 2: Movimentazione della caviglia
④ Conclusioni
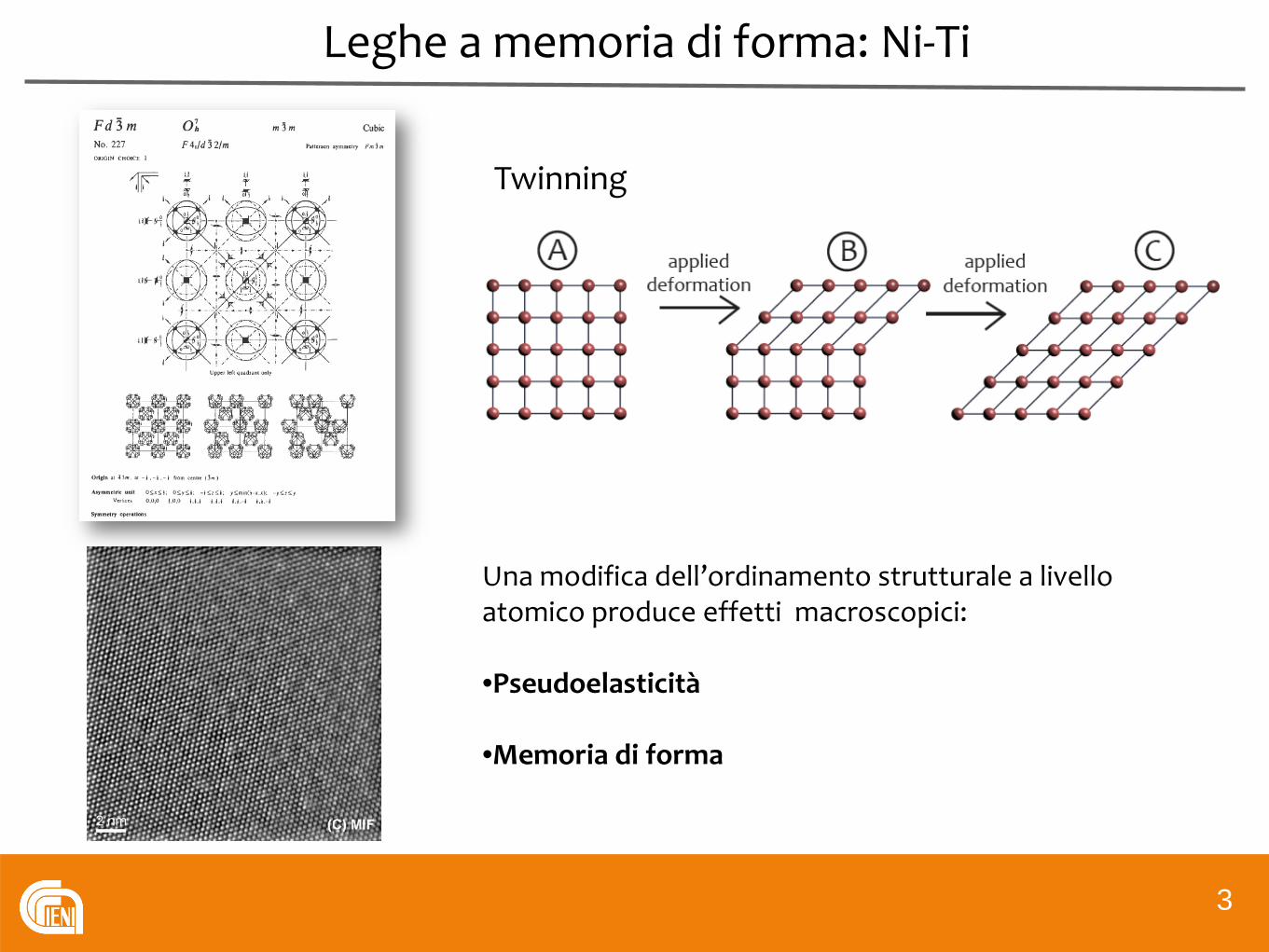
Leghe a memoria di forma: Ni-Ti
3
Una modifica dell’ordinamento strutturale a livello atomico produce effetti macroscopici:
•Pseudoelasticità
•Memoria di forma
Twinning
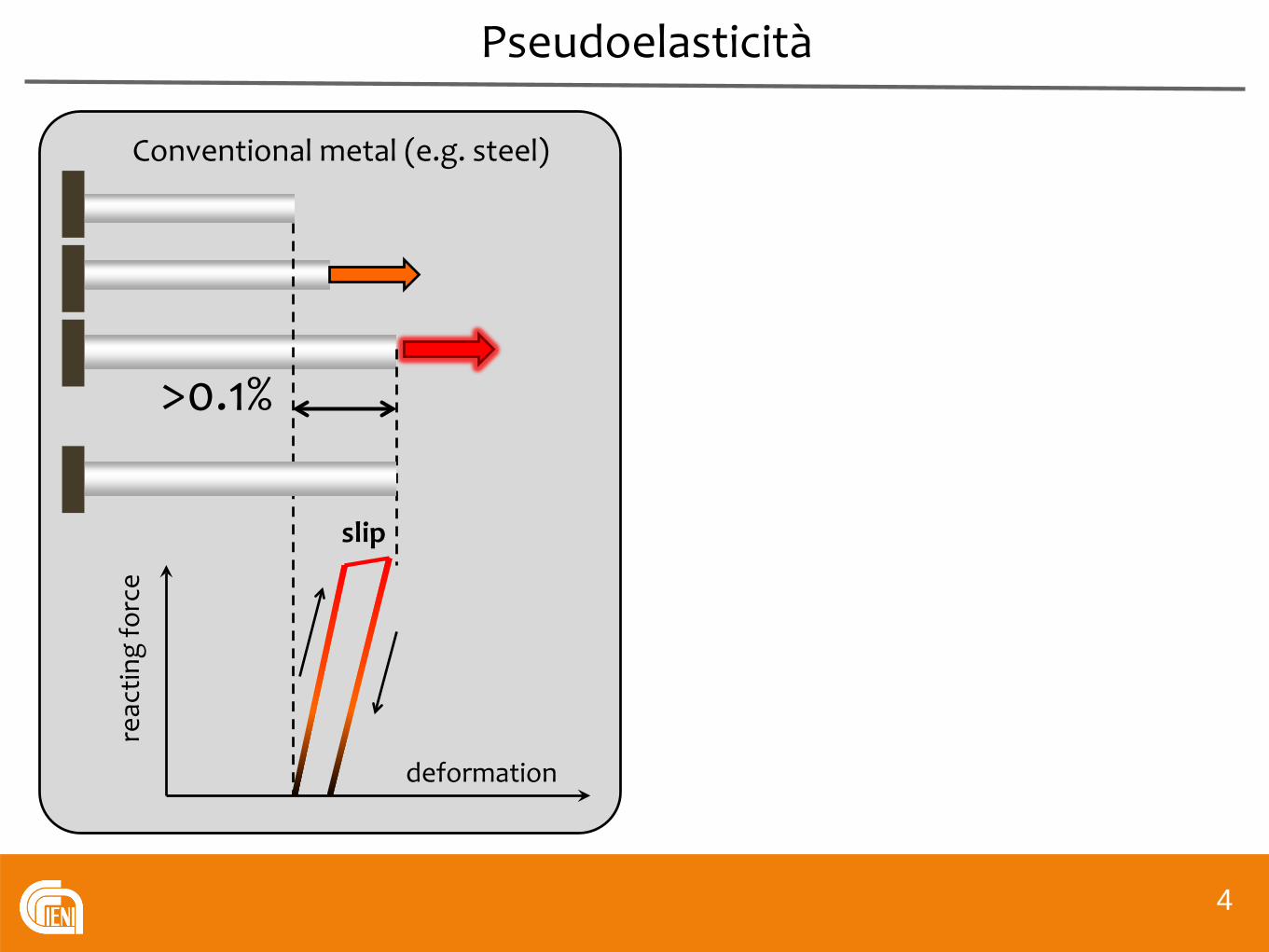
Pseudoelasticità
4
Conventional metal (e.g. steel)
>0.1%
deformation
reac
ting
forc
e
slip
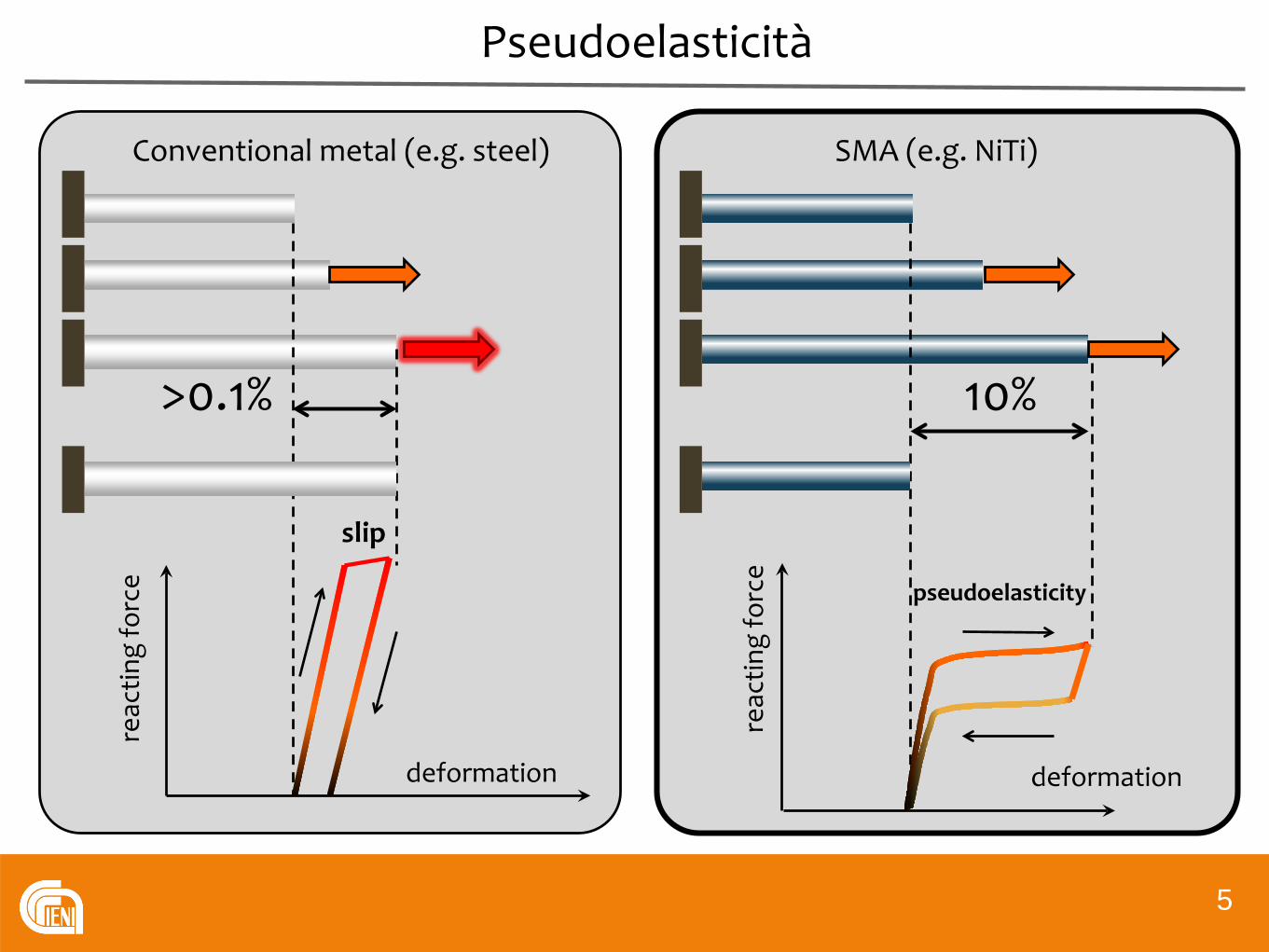
Pseudoelasticità
5
Conventional metal (e.g. steel) SMA (e.g. NiTi)
>0.1% 10%
deformation deformation
reac
ting
forc
e
reac
ting
forc
e
pseudoelasticity
slip

Memoria di forma
6
pseudoplastic deformationand constrained shape recovery
pseudoplastic deformationand free shape recovery
heating heating
reco
very
forc
e
Applications in Upper Motorneuron syndromes
7
Molle di richiamo
Ortesi dinamiche con proprietà nonlineari
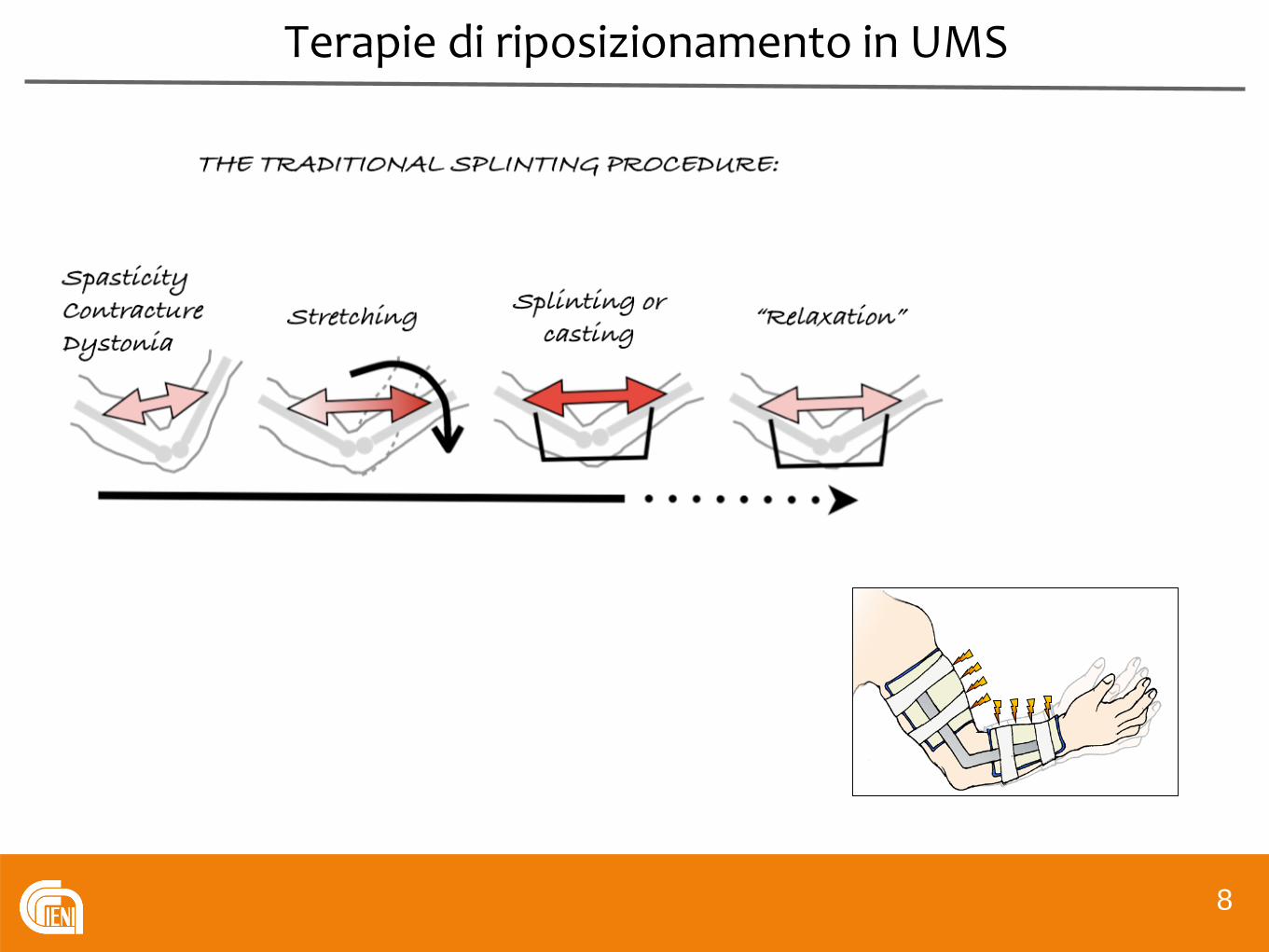
Terapie di riposizionamento in UMS
8

Applications in Upper Motorneuron syndromes
9
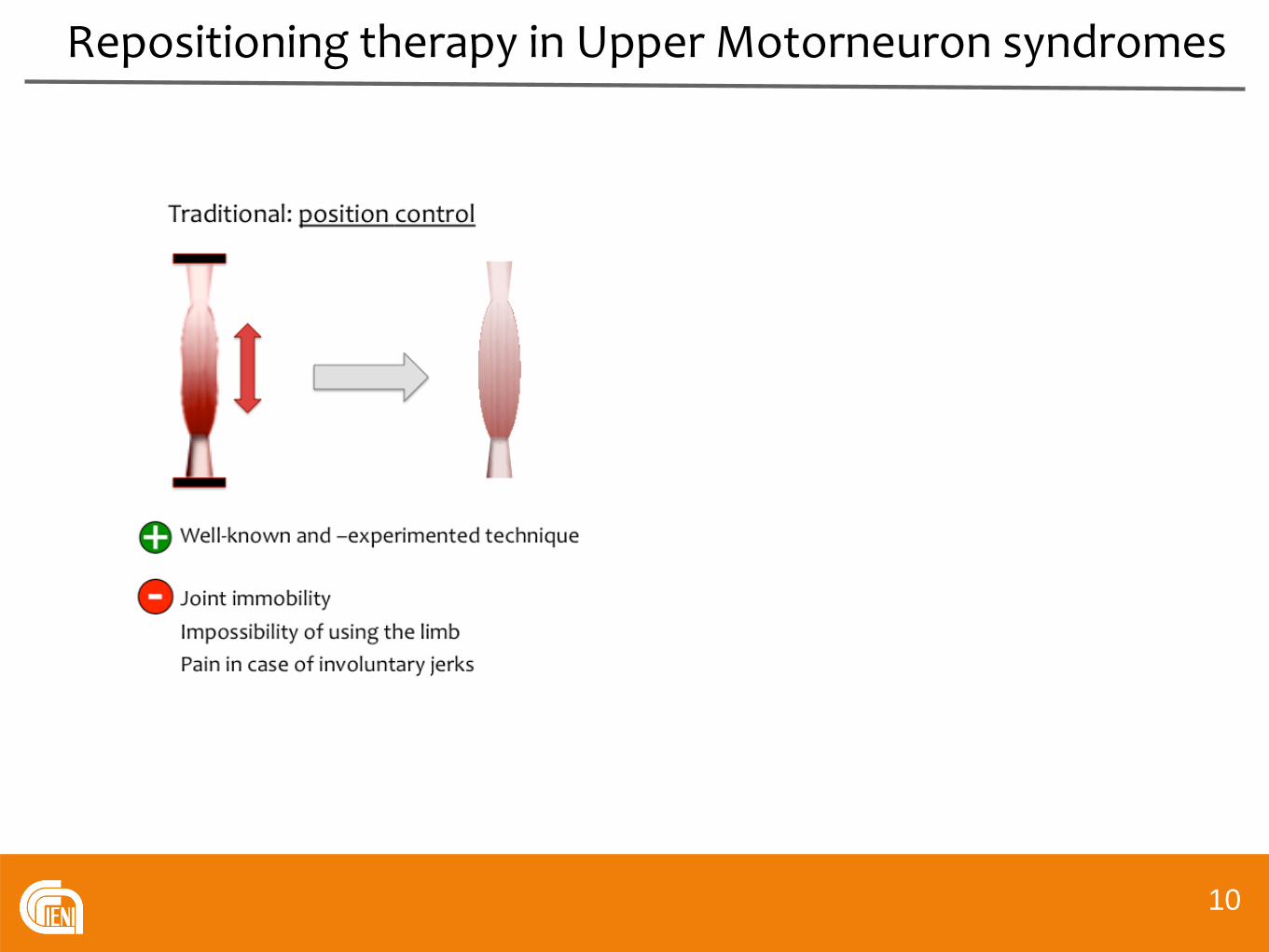
Repositioning therapy in Upper Motorneuron syndromes
10
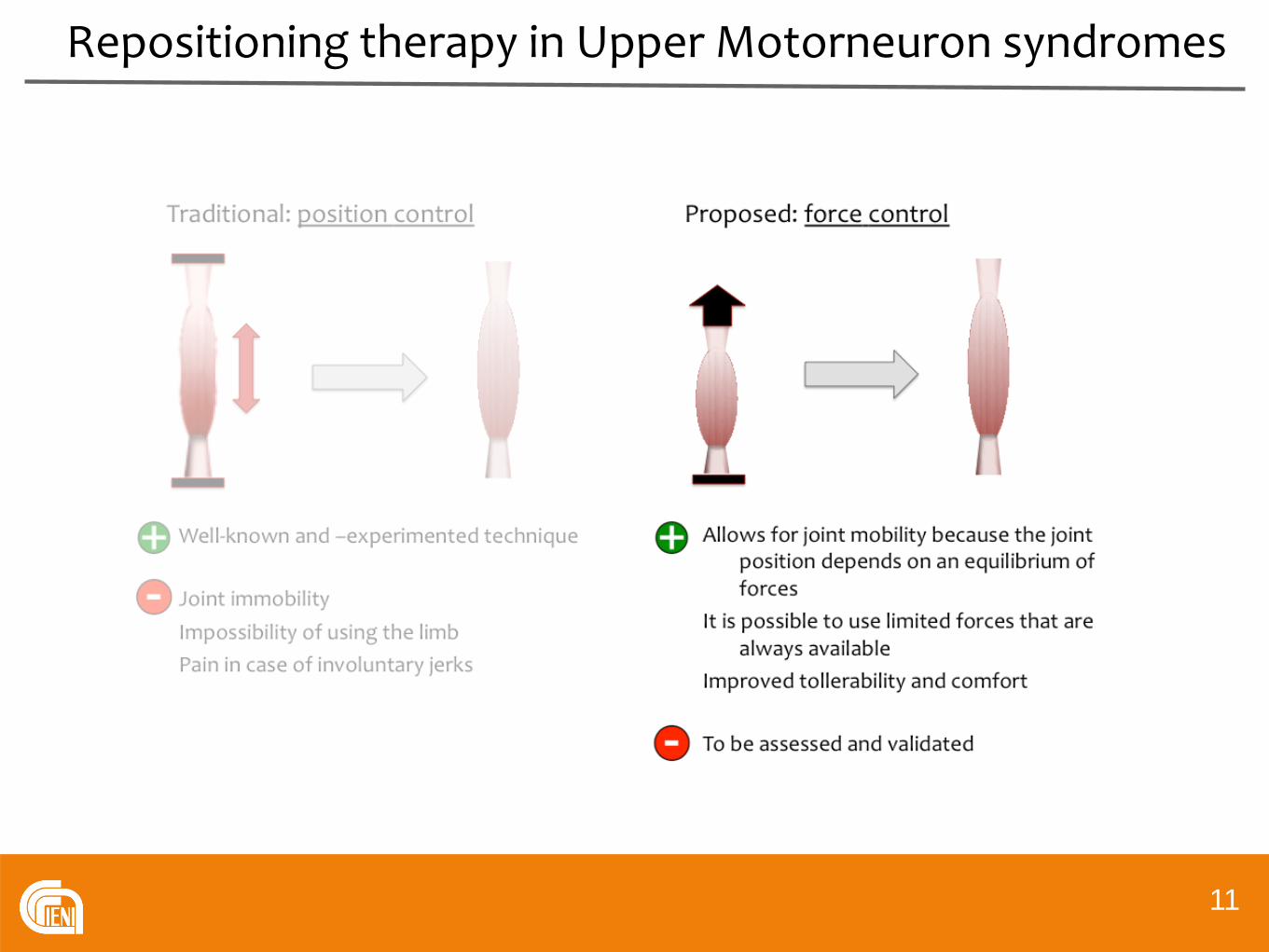
Repositioning therapy in Upper Motorneuron syndromes
11
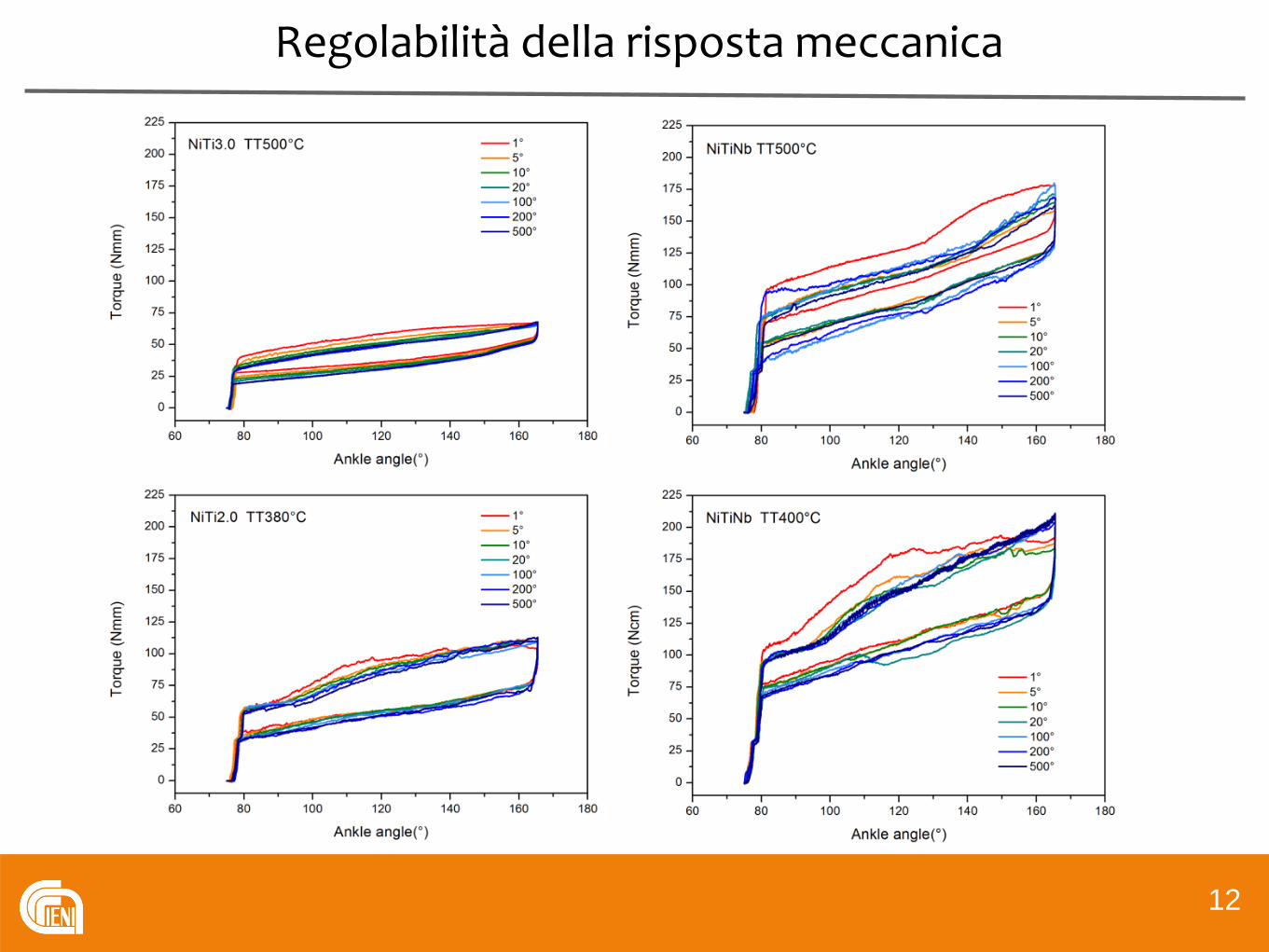
Regolabilità della risposta meccanica
1212
13
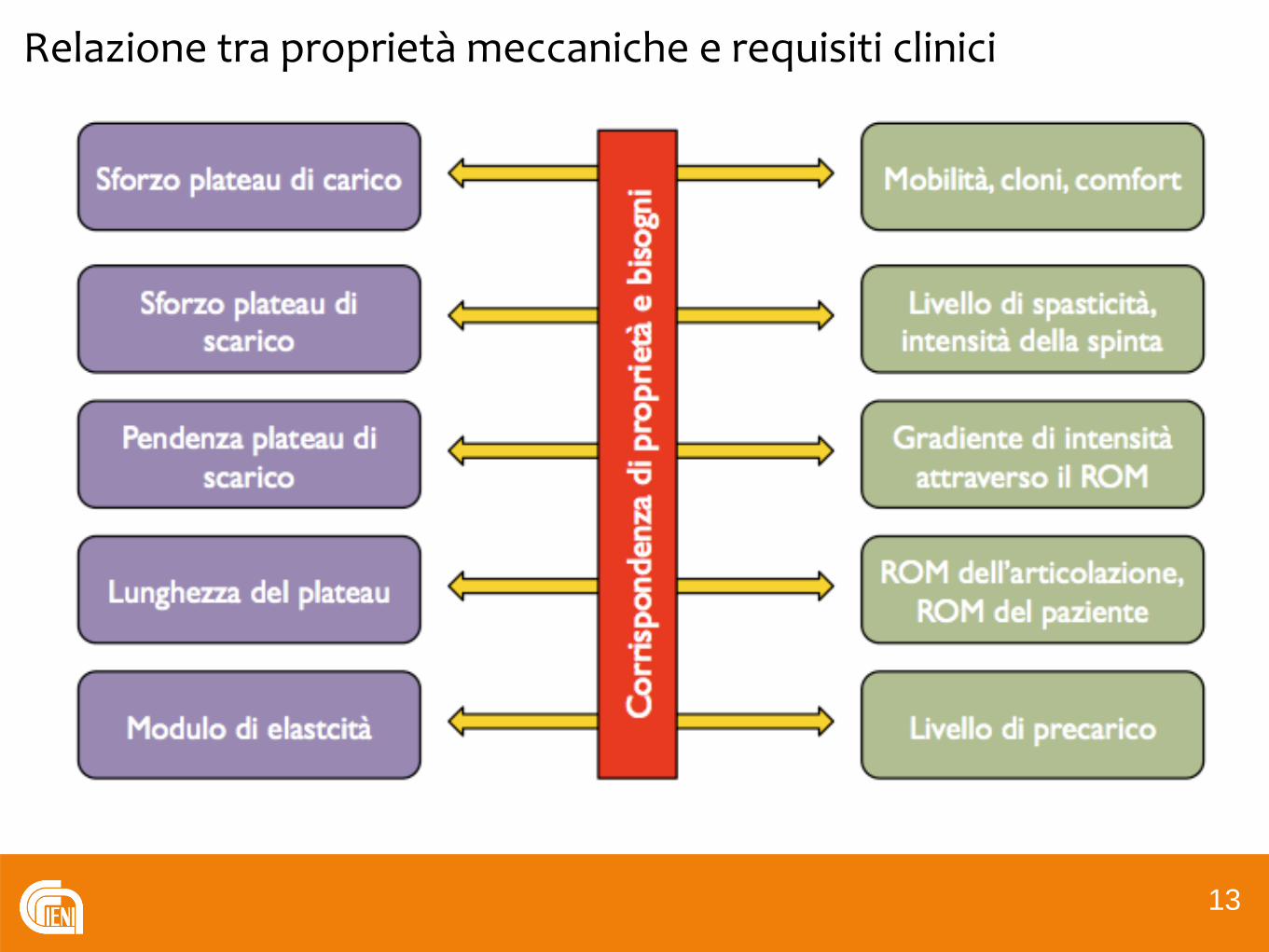
Relazione tra proprietà meccaniche e requisiti clinici
13

Ortesi pseudoelastiche per il riposizionamento
1414
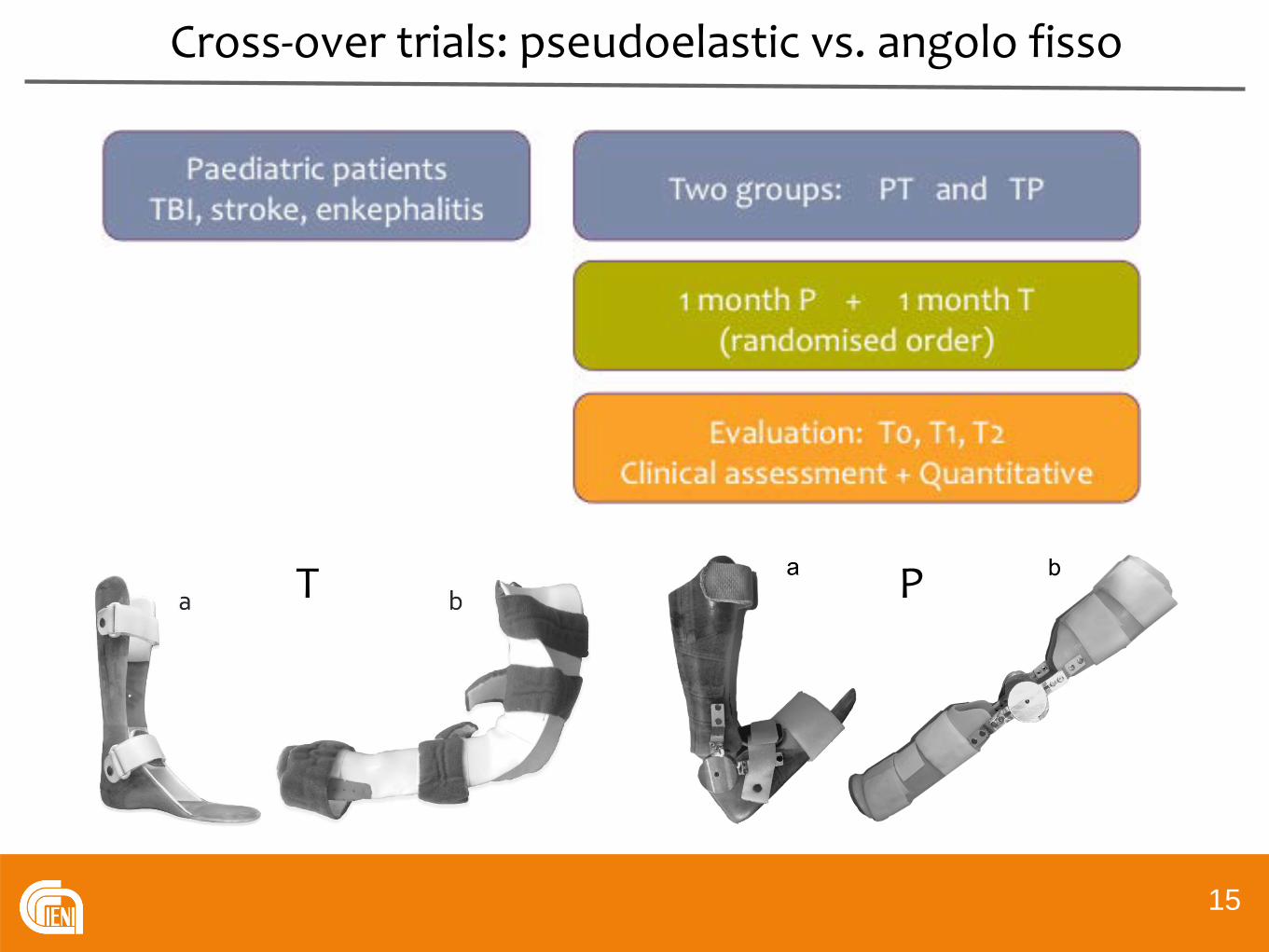
Cross-over trials: pseudoelastic vs. angolo fisso
15
T P

Paziente selezionato: evoluzione della rigidezza articolare
16

Risultati statistici
17
Le ortesi pseudoelastiche salvaguardiano le proprietà iscoelasticheriducendo la rigidità articolare.

Aspects of rehabilitation
Rehabilitation
Segmental/joint rehabilitation
Functional/occupationalrecovery
Quality of life
18
Rehabilitation
Segmental/joint rehabilitation
Functional/occupationalrecovery
Quality of life
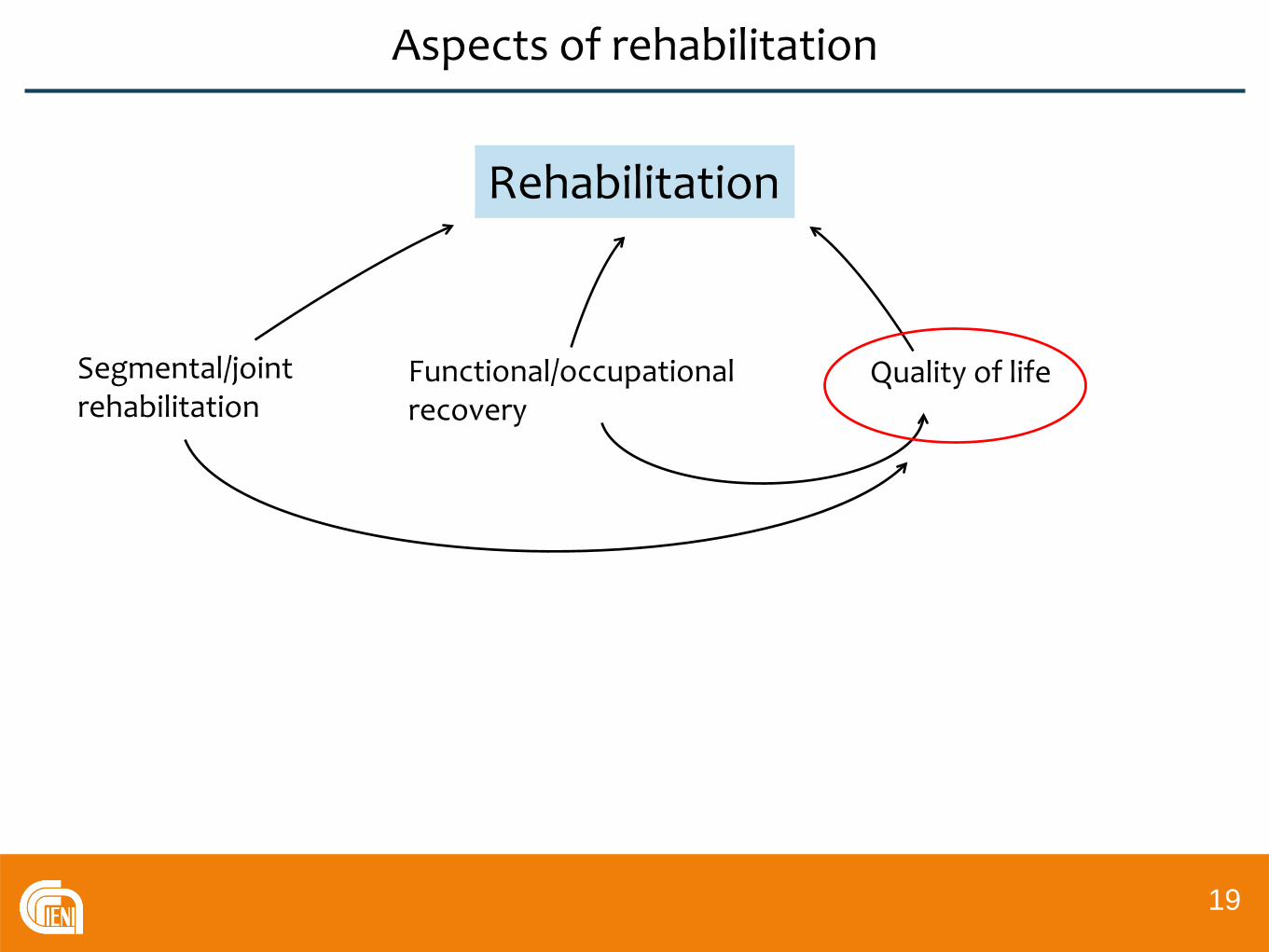
Aspects of rehabilitation
19

Rehabilitation
Segmental/joint rehabilitation
Functional/occupationalrecovery
Quality of life
Pain
Quality of sleep
Comfort of posture
Aspects of rehabilitation
20
Aspects of rehabilitation
Rehabilitation
Segmental/joint rehabilitation
Functional/occupationalrecovery
Quality of life
Dynamic orthotic rehabilitation
????
21

Sensorizzazione dell’ortesi
22
ADC
Bluetooth
Accelerometro triassiale
Elettrogoniometro Snodo pseudoelastico
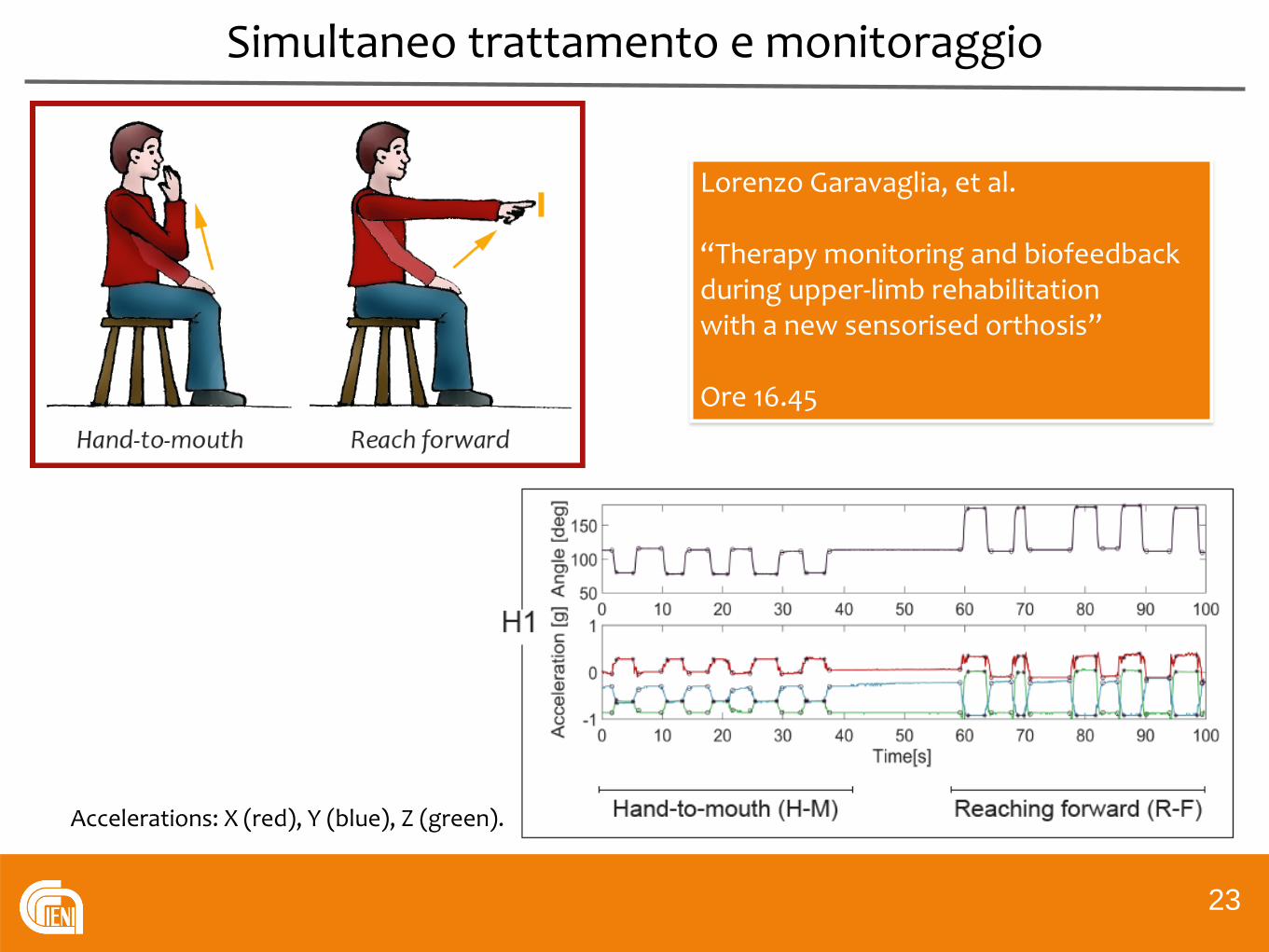
Simultaneo trattamento e monitoraggio
23
Accelerations: X (red), Y (blue), Z (green).
Lorenzo Garavaglia, et al.
“Therapy monitoring and biofeedback during upper-limb rehabilitation with a new sensorised orthosis”
Ore 16.45
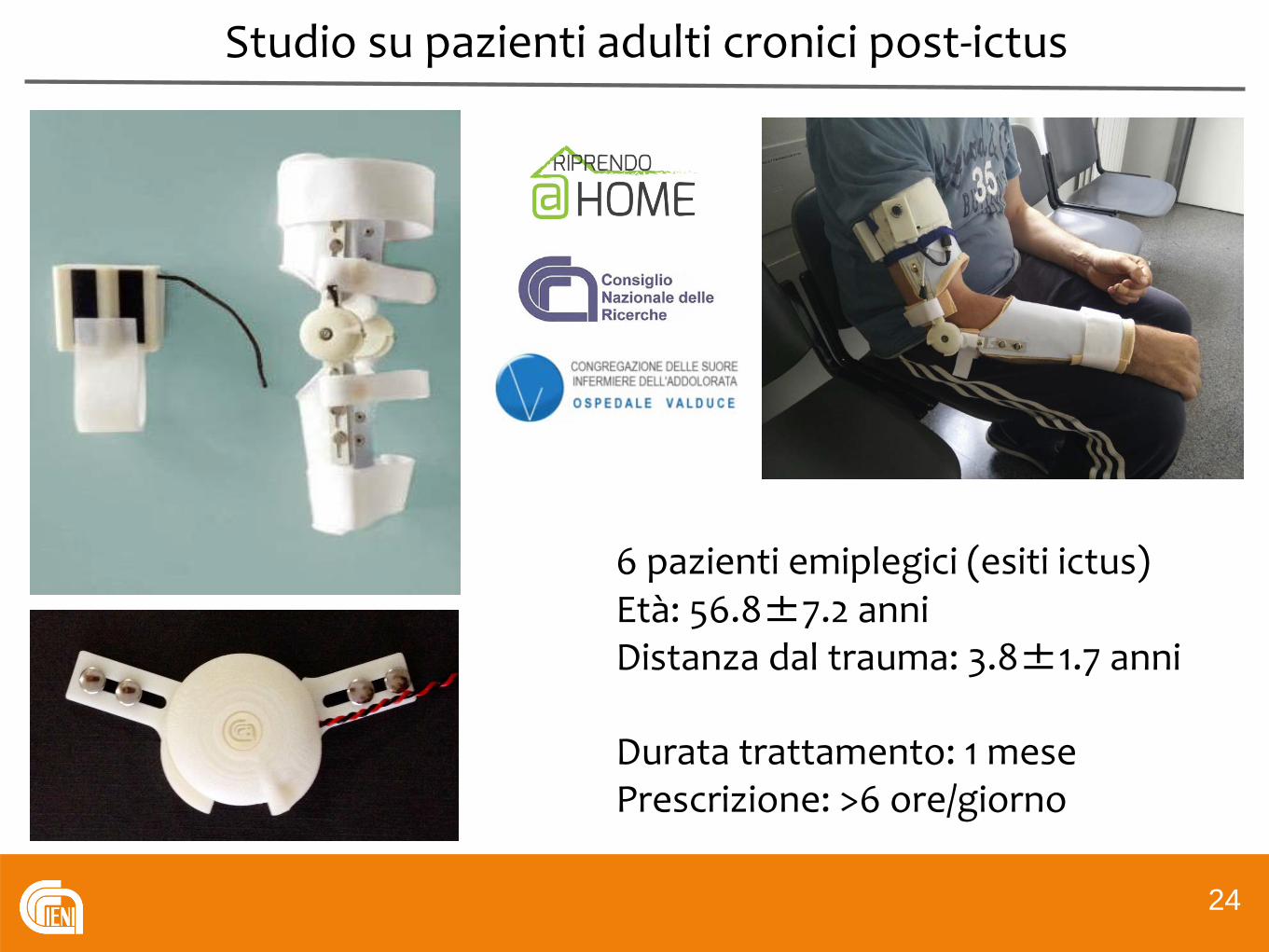
Studio su pazienti adulti cronici post-ictus
24
6 pazienti emiplegici (esiti ictus)Età: 56.8±7.2 anniDistanza dal trauma: 3.8±1.7 anni
Durata trattamento: 1 mese Prescrizione: >6 ore/giorno
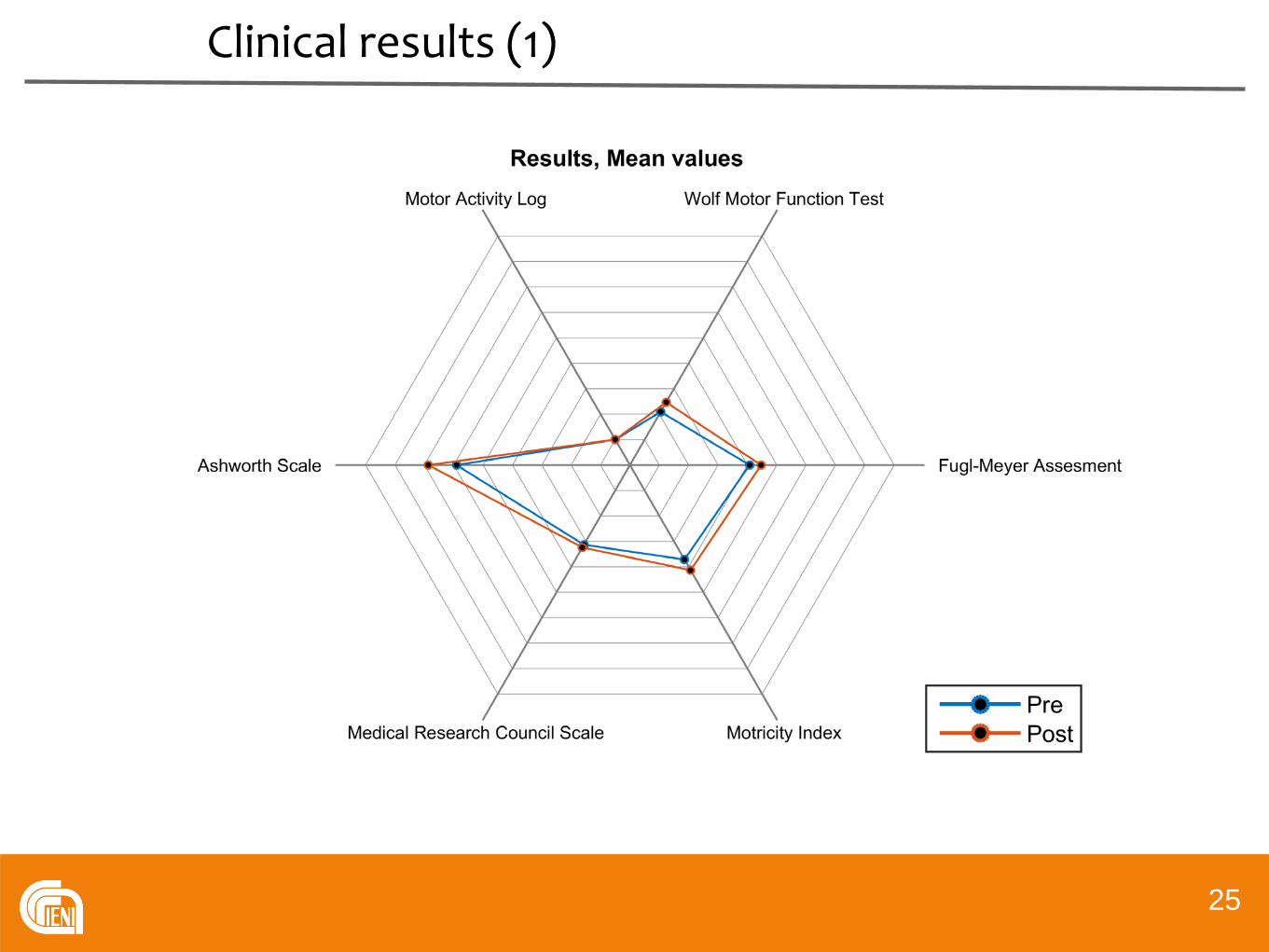
Clinical results (1)
25

Clinical results (2)
26

Applicazioni nel trattamento di UML
27
Attuatori a memoria di forma
Mobilizzatore per la caviglia

Push-pull cartridge actuator
28
Inextensible thread
Coilings of SMA wire
Electric connections
Aluminium frame
Linear guide and carriage
Plastic double-groove pulleys
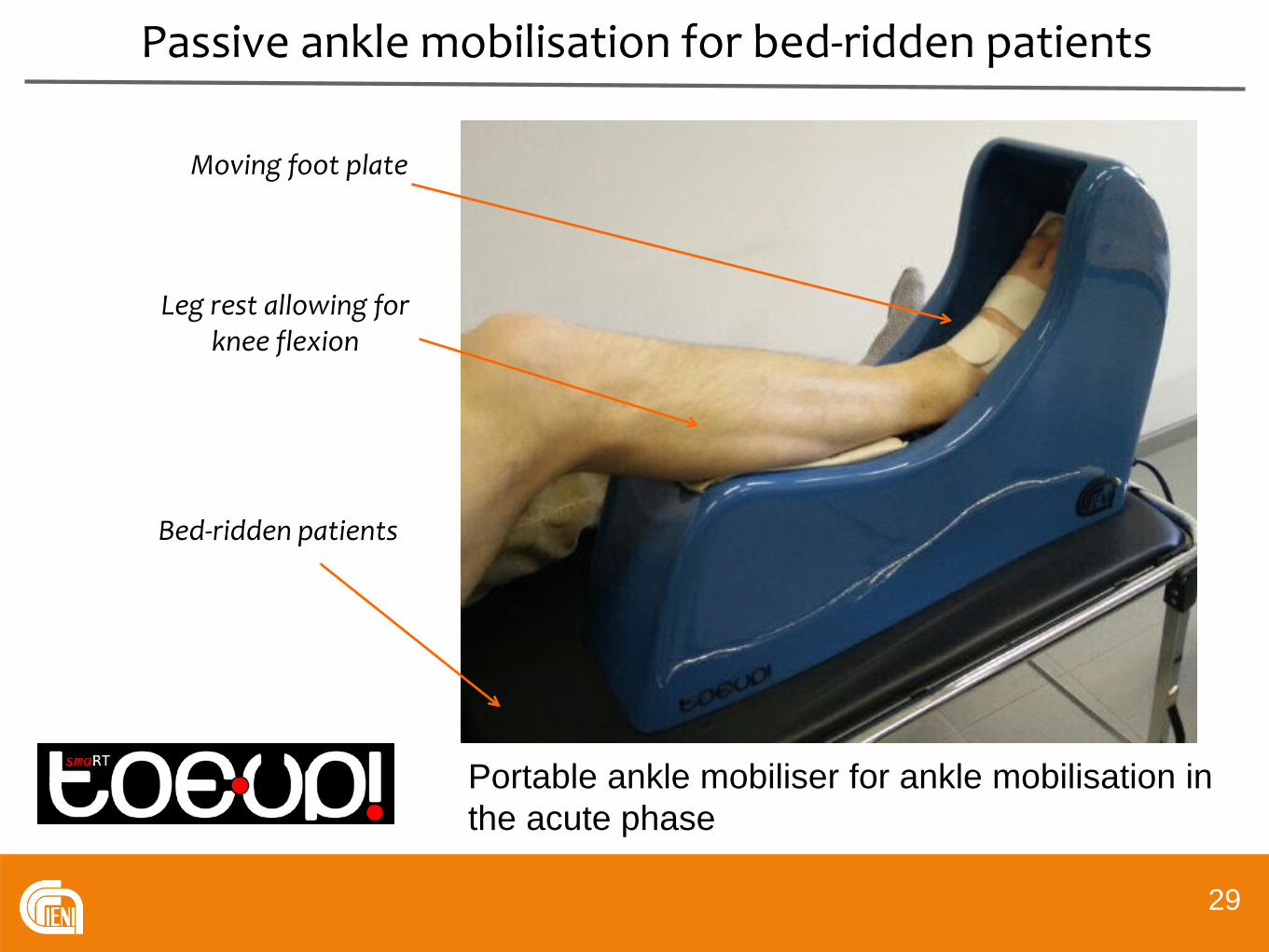
Passive ankle mobilisation for bed-ridden patients
29
Portable ankle mobiliser for ankle mobilisation in the acute phase
Moving foot plate
Bed-ridden patients
Leg rest allowing for knee flexion

Preliminary MEG studies on healthy volunteers
30
in collaboration with
11 normal volunteers (5 males, aged 24 ± 4 years)
MEG165 channels
S Pittaccio, et al. Primary sensory and motor cortex activities during voluntary and passive ankle mobilisation by the SHADE orthosis, Human Brain Mapping, 2011, 32:60–70
S Pittaccio, et al. Passive ankle dorsiflexion by an automated device and the reactivity of the motor cortical network., Proceedings 35th IEEE-EMBC, 2013, Osaka, pp. 6353-6356
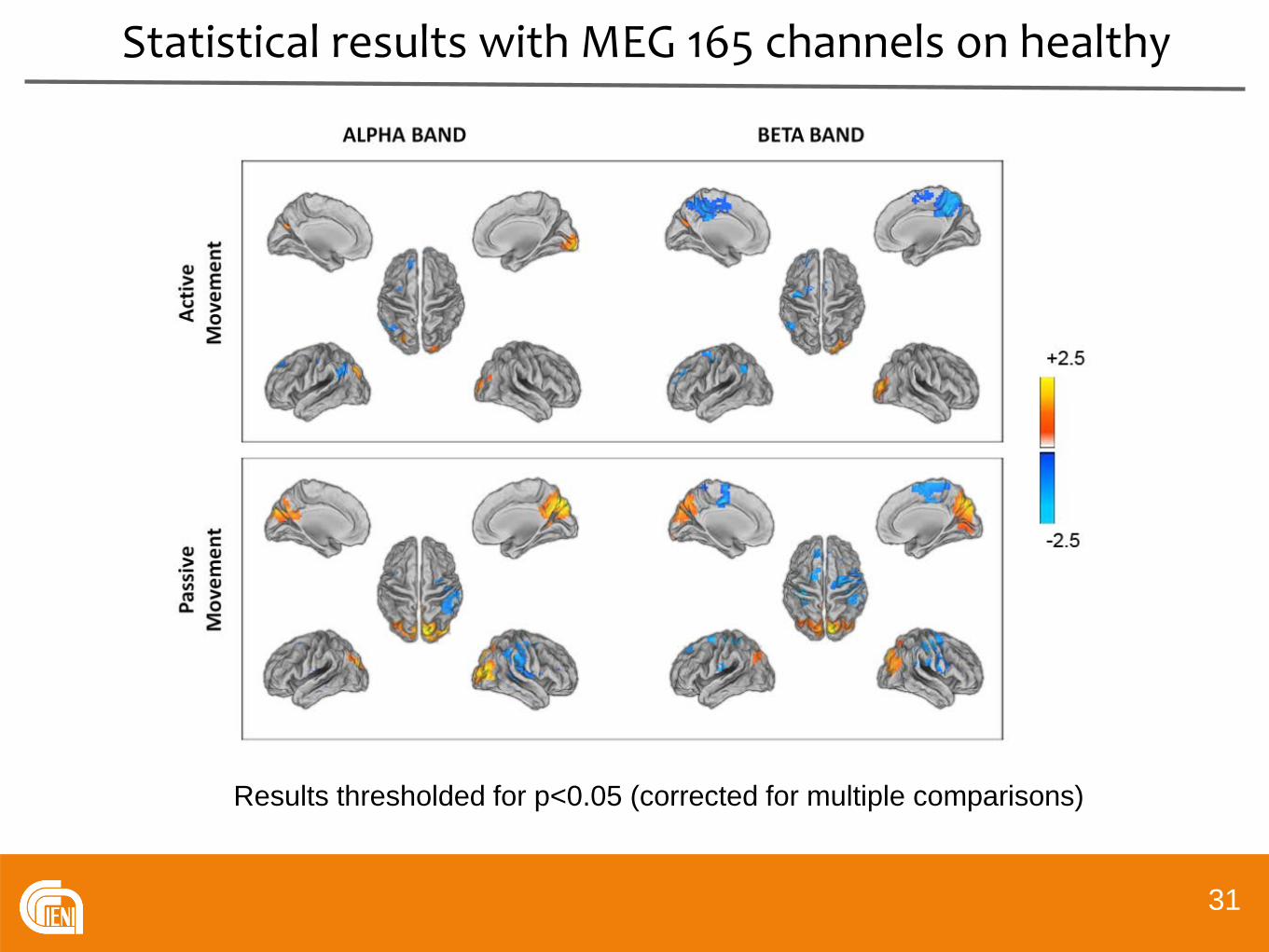
Statistical results with MEG 165 channels on healthy
31
Results thresholded for p<0.05 (corrected for multiple comparisons)

Statistical results with MEG 165 channels on healthy
32
BET
A B
AND
ALPH
A B
AND
Event Related Desynchronization (ERD) was evaluated in alpha (8-13 Hz) and beta (15-25 Hz) bands in the period following the onset of PM and AIC.
Similar patterns of band power modulation in alpha and beta band were found for VM and O-PM in the contralateral primary sensory and motor areas.
A greater ERD in beta band was found during VM compared to O-PM in supplementary motor area and bilateral premotor areas.
PM ERD in alpha band was greater in bilateral secondary somatosensory areas than for VM, probably resulting from an increased sensory integration during PM.
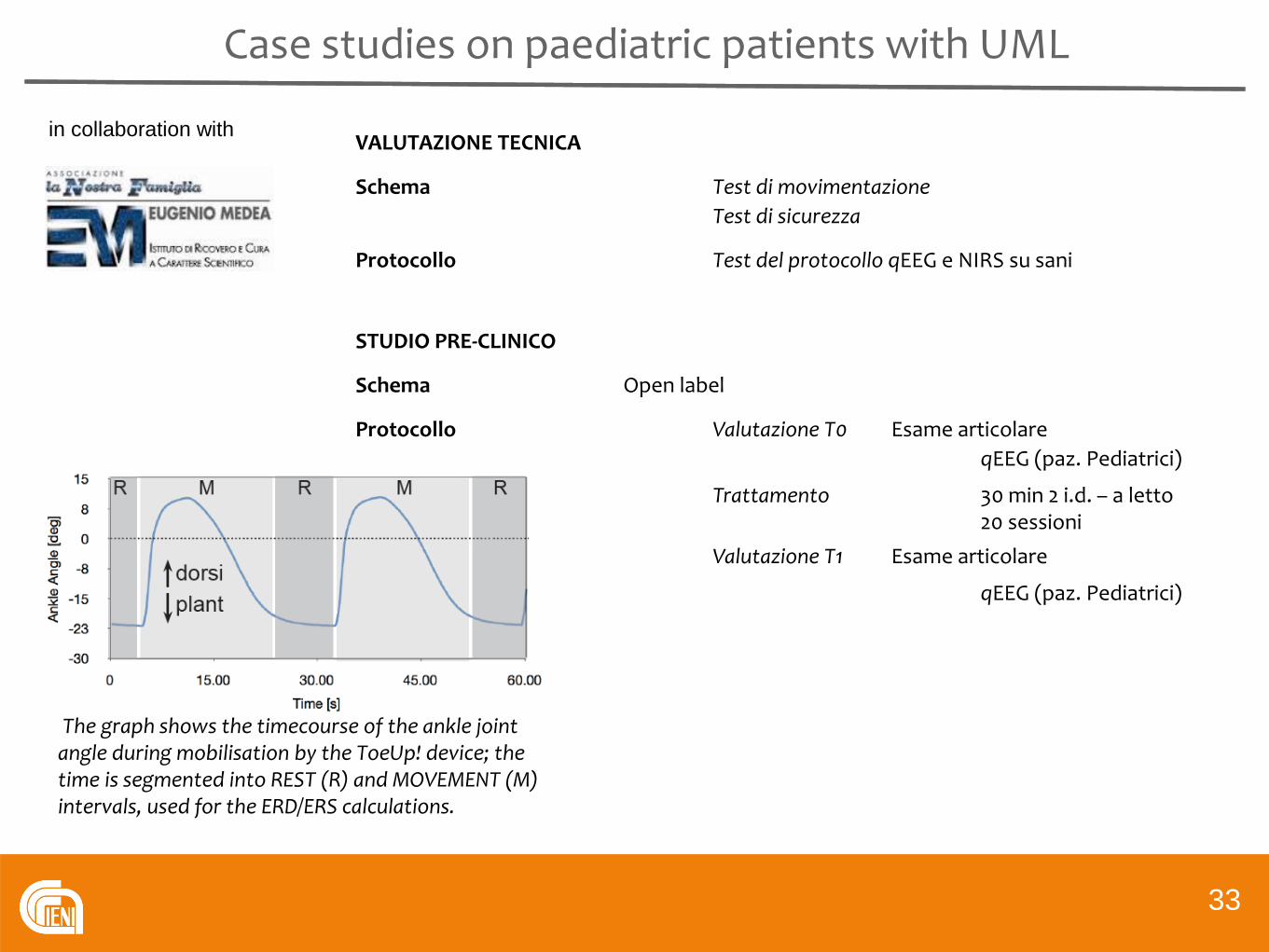
Case studies on paediatric patients with UML
33
in collaboration with VALUTAZIONE TECNICA
Schema Test di movimentazioneTest di sicurezza
Protocollo Test del protocollo qEEG e NIRS su sani
STUDIO PRE-CLINICO
Schema Open label
Protocollo Valutazione T0 Esame articolareqEEG (paz. Pediatrici)
Trattamento 30 min 2 i.d. – a letto20 sessioni
Valutazione T1 Esame articolare
qEEG (paz. Pediatrici)
The graph shows the timecourse of the ankle joint angle during mobilisation by the ToeUp! device; the time is segmented into REST (R) and MOVEMENT (M) intervals, used for the ERD/ERS calculations.
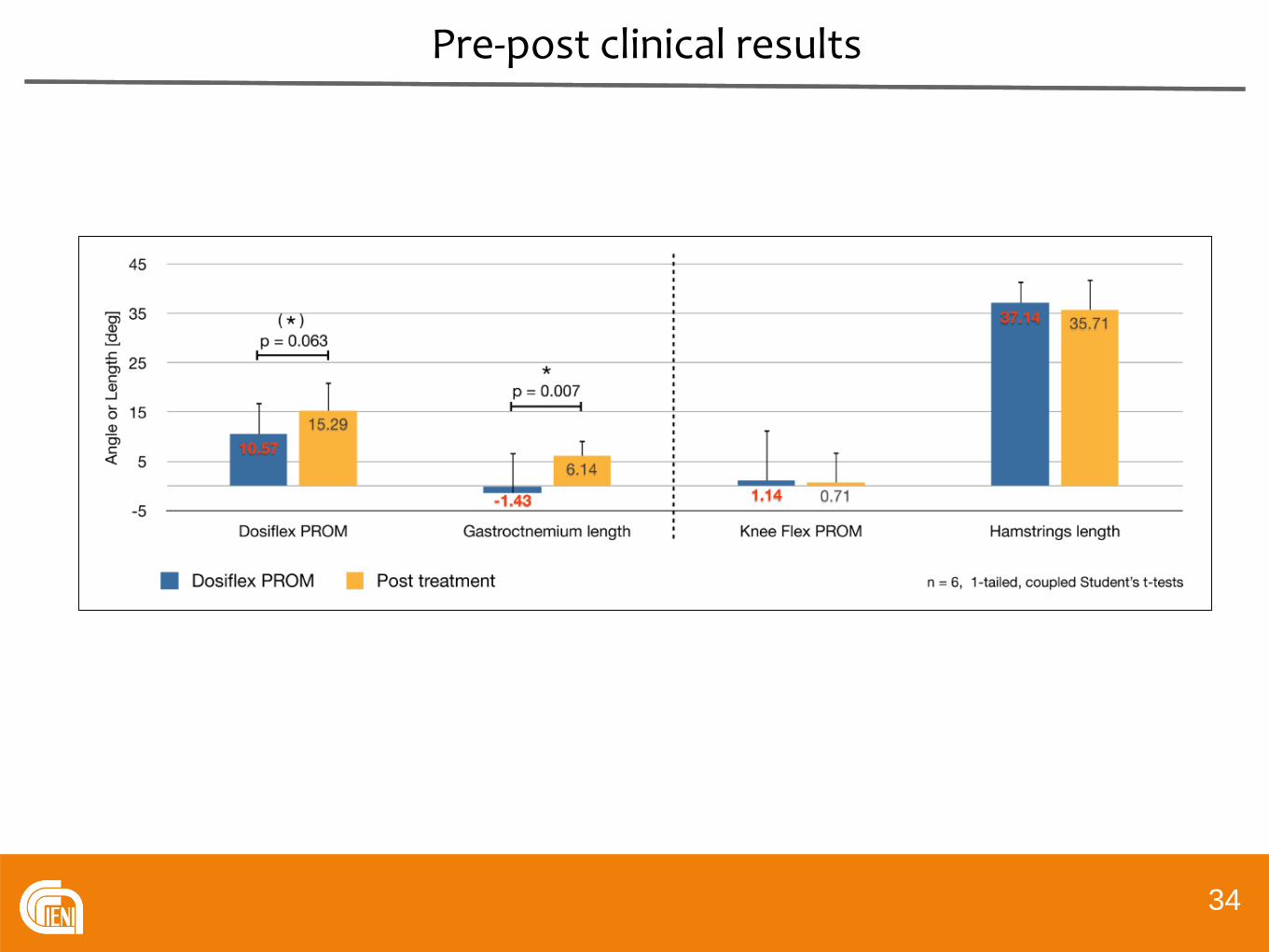
Pre-post clinical results
34

Pre-post clinical results
35
Pediatrici post-traumatici (dettaglio questionario)
DOMANDA 1: Con quanta DIFFICOLTA’ suo figlio ha eseguito le sedute riabilitative con ToeUp?
Mio figlio non ha potuto utilizzare il dispositivo, ed il trattamento è stato interrotto perché non idoneo alla condizione di mio figlio.Estrema difficoltà, che ha ripetutamente impedito l’utilizzo del dispositivo durante le sedute riabilitative.Molta difficoltà, che talvolta ha complicato, o occasionalmente impedito il corretto utilizzo del dispositivoQualche difficoltà, che tuttavia non ha impedito il corretto utilizzo del dispositivo durante tutto il trattamento.Nessuna difficoltà. Mio figlio ha potuto eseguire correttamente tutte le sedute riabilitative programmate,
in quanto il dispositivo riabilitativo era del tutto idoneo alla condizione di mio figlio.
DOMANDA 2: Le difficoltà incontrate durante l’utilizzo del dispositivo si sono verificate principalmente:
Durante tutte le sedute(Soprattutto) nella parte iniziale del trattamento(Soprattutto) nella parte finale del trattamentoUnicamente nelle primissime sedute di trattamentoNon si sono verificate difficoltà
DOMANDA 3: Dopo aver osservato suo figlio mentre eseguiva riabilitazione con Toe-Up!, come giudica il COMFORT, cioè il grado di comodità del dispositivo?
Il dispositivo è inutilizzabile perché troppo scomodoIl dispositivo è molto poco confortevoleIl dispositivo è poco confortevoleIl dispositivo è confortevole e ben tolleratoIl dispositivo è talmente confortevole da costituire un incentivo alla riabilitazione per mio figlio.
1 preferenza4 preferenze
4 preferenze
1 preferenza
3 preferenze2 preferenze

Risultati EEG preliminari
36
The graphs show the PSD spectra of channelCPz for the same patient of the ERD/ERSmaps (left). After the treatment powerincreases overall and particularly in the αband.
L. Garavaglia, et al. Pilot Study of the Cortical Correlates and Clinical Effects of Passive Ankle Mobilisation in Children with Upper Motorneuron Lesions, Proceedings 37th IEEE-EMBC, 2015, Milan

Conclusions
37
Shape memory alloys, thanks to their nonlinear and adjustablemechanical and functional characteristics are a resource in designing devices for a number of applications in neuromuscularrehabilitation.
These range from passive mobilisation devicesto repositioning orthoses,and wearable devices for movementstabilisation and conditioning.

The Institute for Energetics and Interphases at Lecco
38Thanks! [email protected]
Thanks to
Lorenzo GaravagliaFabio Lazzari



Amagnetic actuators
41
International patentWO/2011/141183
S Viscuso, S Pittaccio, Design and implementation of a portable amagnetic shape memory rotary actuator, 2012, Journal of Intelligent Materials Systems and Structures, 24:454-72
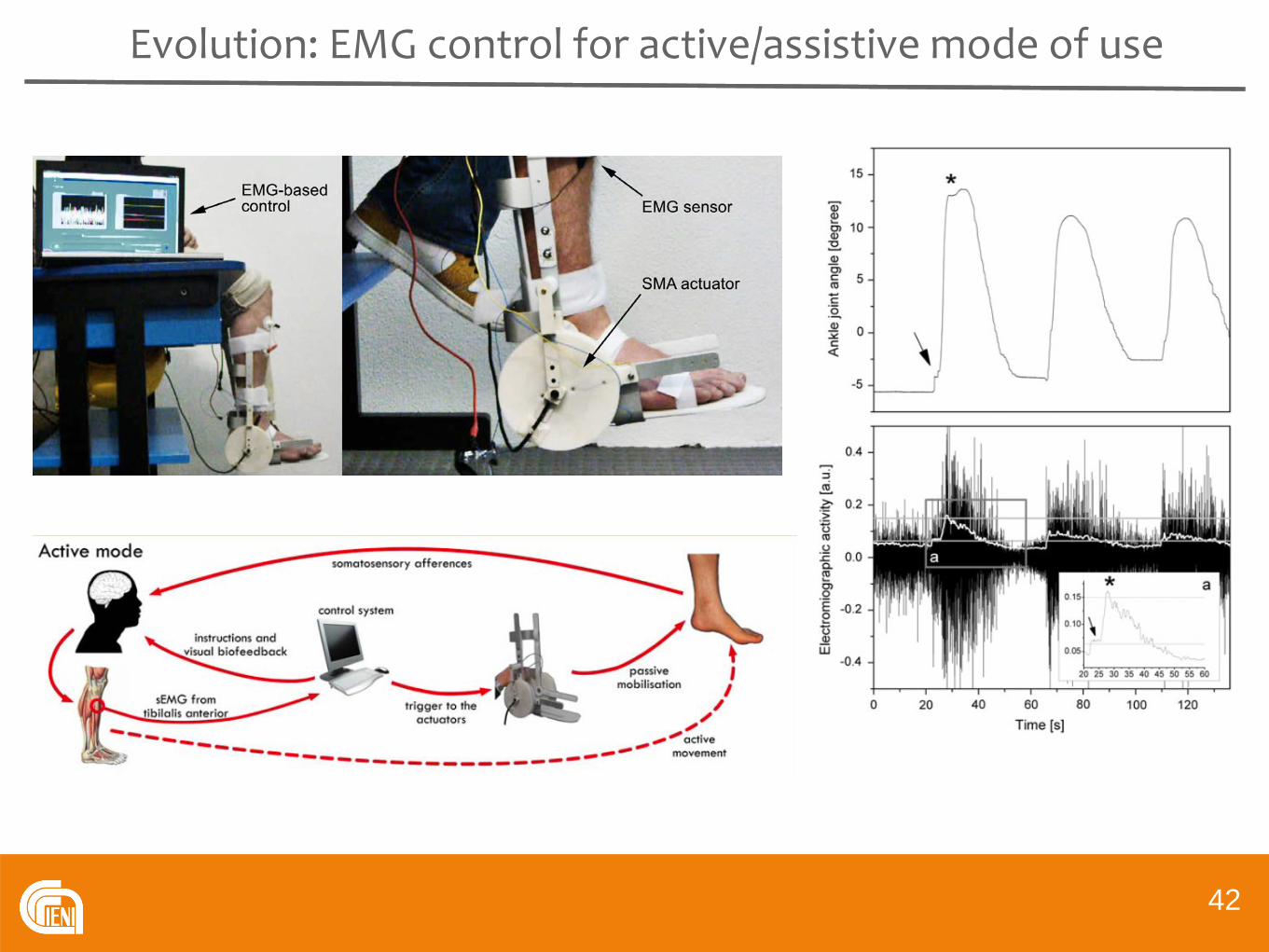
Evolution: EMG control for active/assistive mode of use
42
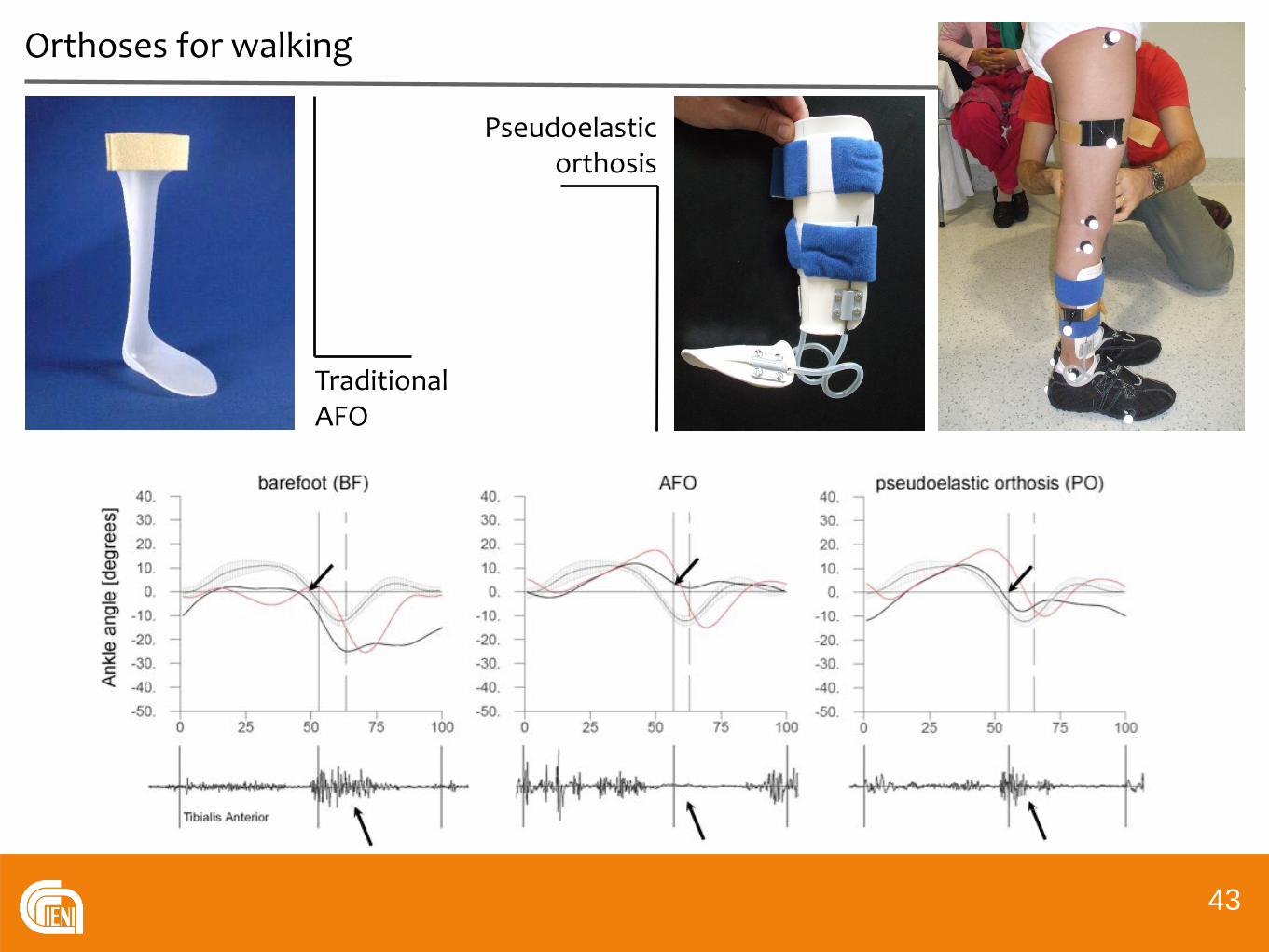
TraditionalAFO
Pseudoelastic orthosis
Orthoses for walking
43
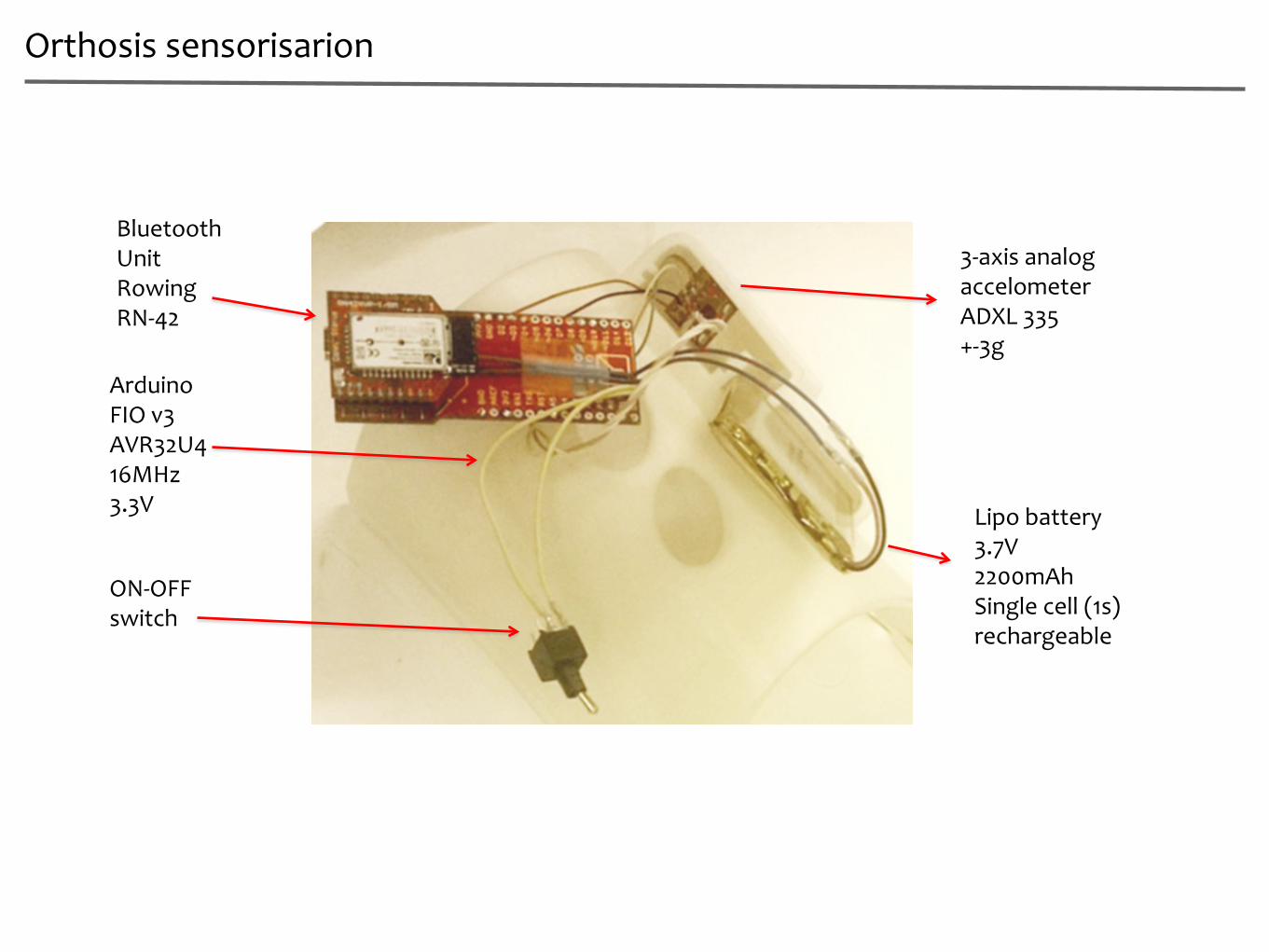
Orthosis sensorisarion
3-axis analogaccelometerADXL 335+-3g
ArduinoFIO v3AVR32U416MHz3.3V
BluetoothUnitRowingRN-42
Lipo battery3.7V2200mAhSingle cell (1s)rechargeable
ON-OFFswitch

3D printed orthoses
45
Morphing from anatomical data
Imagesegmentation
Acquisition of anatomicaldataset
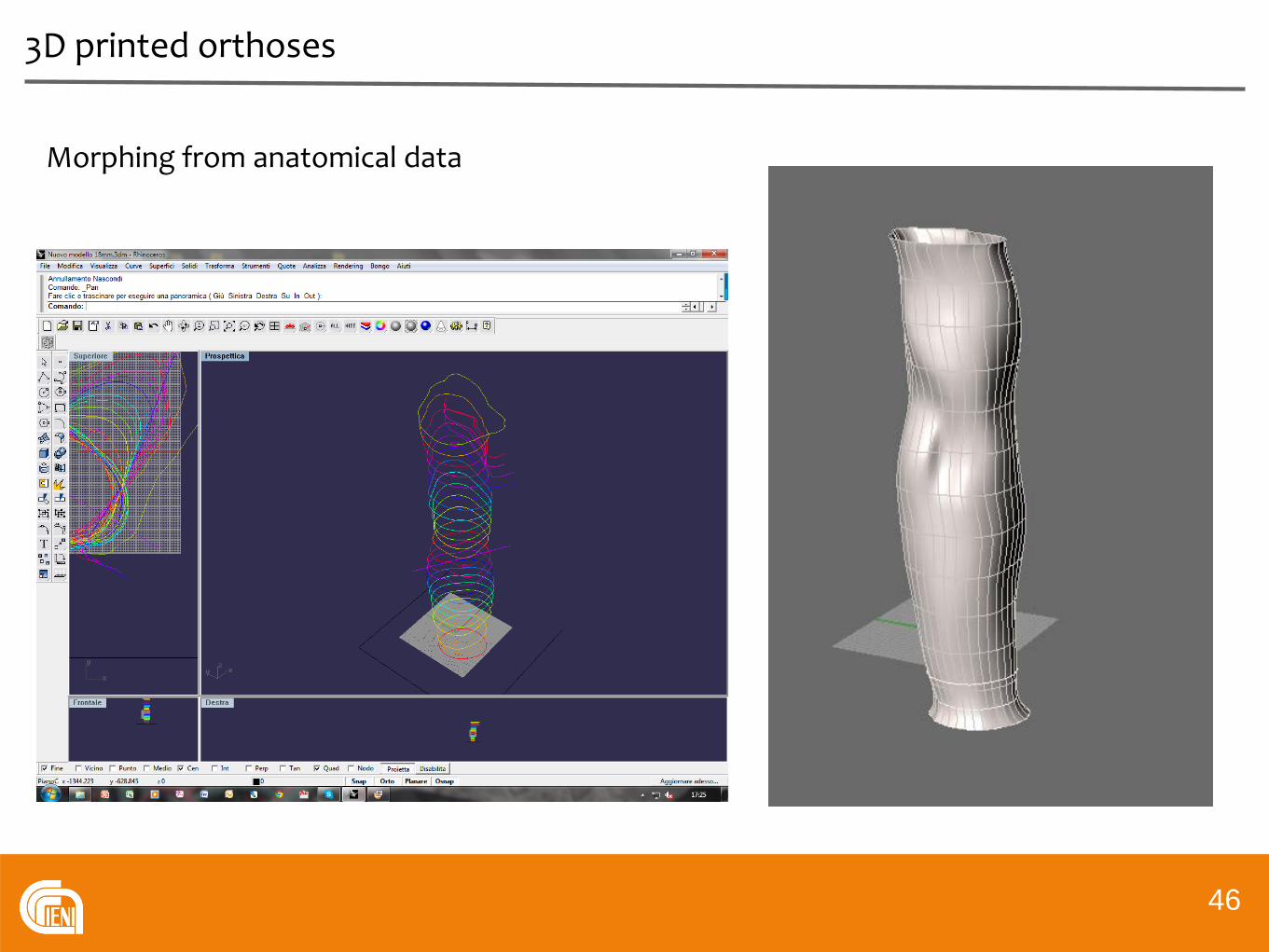
3D printed orthoses
46
Morphing from anatomical data
3D printed orthoses
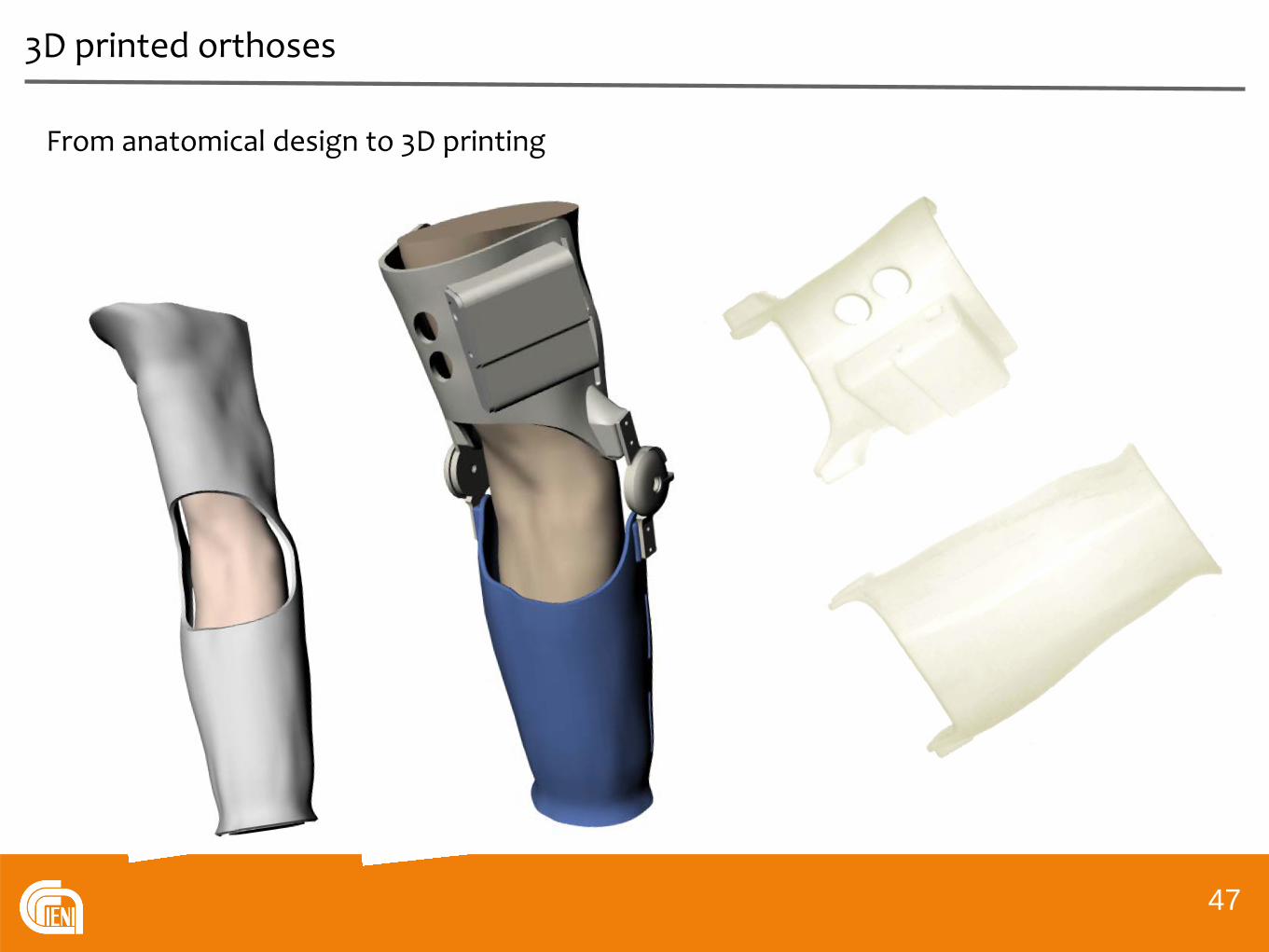
47
From anatomical design to 3D printing

3D printed orthoses
Advantages of morphing and 3D printing
• Perfect matching of skin interface minimised contact pressures
• Perfect localisation of anatomical elbow axis best allignment of hinges
minimised sliding and friction
• Perfect parallel allignment of hinges optimal mechanical function
• Integration of electronic system minimised volume
improved comfort