official response - who · international tree nut council (inc) - 3 - june 15, 2002 1. introduction...
TRANSCRIPT

International Tree Nut Council (INC)Consejo Internacional de los Frutos Secos
OOffffiicciiaall RReessppoonnsseettoo
WWoorrlldd HHeeaalltthh OOrrggaanniizzaattiioonn ((WWHHOO))FFoooodd aanndd AAggrriiccuullttuurree OOrrggaanniizzaattiioonn ((FFAAOO))
EExxppeerrtt CCoonnssuullttaattiioonn oonn DDiieett,, NNuuttrriittiioonn aanndd tthheePPrreevveennttiioonn ooff CChhrroonniicc DDiisseeaasseess
Geneva, June 15, 2002

International Tree Nut Council (INC) - 2 - June 15, 2002
Official Response to Draft Report of Joint World HealthOrganization (WHO) Food and Agriculture Organization (FAO)
Expert Consultation on Diet, Nutrition and the Prevention ofChronic Diseases
Table of Contents
1. Introduction to INC ...........................................................................................................................3
A. Background on OrganizationB. Global Tree Nut ProductionC. Worldwide Tree Nut ConsumptionD. Implications and Directions for Increased Trade and Consumption
2. Summary of Tree Nut Research ........................................................................................................8
A. Health Outcome Studies - USAB. Health Outcome Studies - EuropeC. Human Clinical Trials ! Cardiovascular Disease - Mixed Nut Studies ! Cardiovascular Disease - Single Nut Studies ! Obesity/Weight Reduction ! Diabetes ! Cancer
3. Tree Nut Composition.....................................................................................................................16
4. Specific Feedback on WHO/FAO Draft Report..............................................................................19
5. Conclusions and INC Recommendations........................................................................................21
6. References .......................................................................................................................................24
7. Contributors/Reviewers....................................................................................................................30

International Tree Nut Council (INC) - 3 - June 15, 2002
1. Introduction to INC
A. Background on Organization
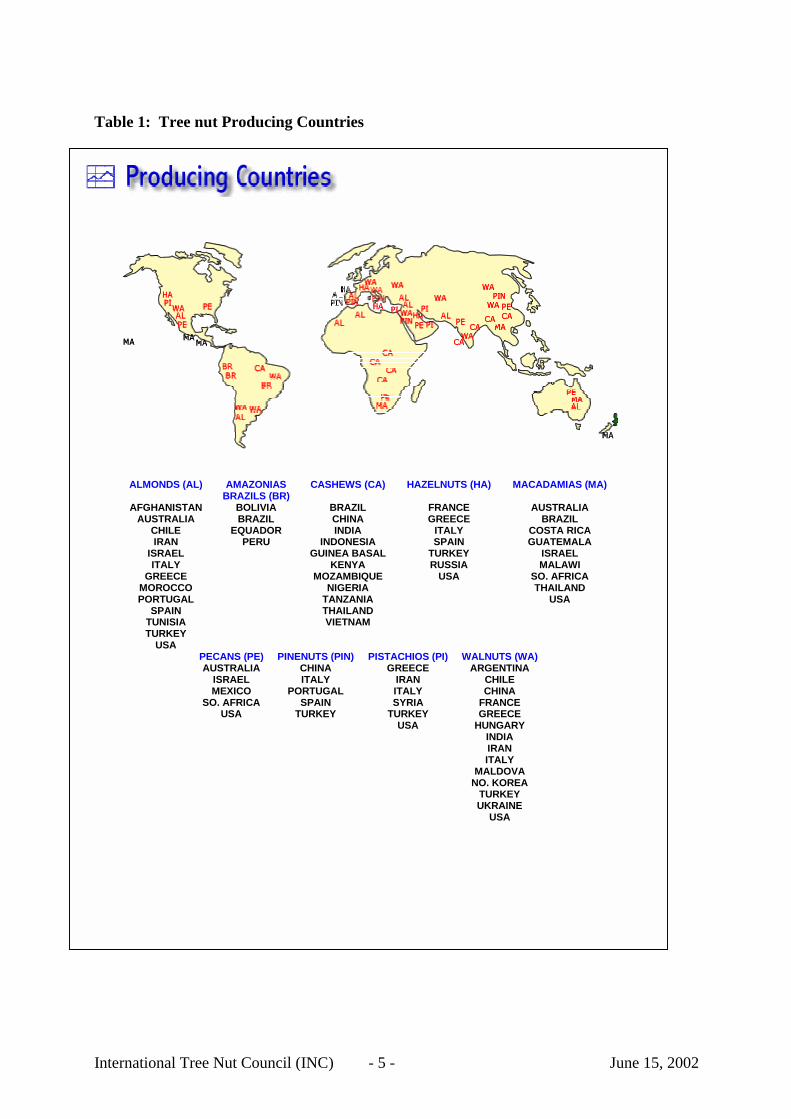
The tree nut industry consists of almonds, brazil nuts, cashews, hazelnuts, macadamias,pecans, pinenuts, pistachios and walnuts. Tree nuts are produced in more than 40 developedand less-developed countries (see Table 1) and consumed worldwide. Millions of hectares ofland are devoted to tree nuts, providing economic livelihood for hundreds of thousands ofproducers and small families.
The International Tree Nut Council (INC) is an international, non-profit, non-governmentalorganization that supports market research and promotional efforts throughout the world.Members include those associations and organizations that represent the nine tree nuts(almonds, brazils, cashews, hazelnuts, macadamias, pecans, pinenuts, pistachios and walnuts)in a number of producing countries. The INC's mission is to expand global consumption ofall tree nuts. Among the key objectives:
• To increase understanding about nutritional benefits, growing, processing, marketing,distribution and consumption trends in the tree nut industry.
• To collect and distribute a single source of annual statistical information fromproducing and consuming countries of the nine tree nuts.
• To assure that global quality standards and trading terms are within the framework ofexisting national and international bodies and do not inhibit trade within the industry.
• To promote research and new product development.
• To facilitate international cooperation by interacting with various public, private,national and international organizations which share common goals.
• To increase goodwill and mutual understanding of the tree nut industry by promotinginternational scientific meetings in producing and consuming countries.
In 1994, INC began to support and participate in educational forums devoted to the scientificissues regarding the positive role that tree nuts play in prevention of heart disease and otherchronic diseases (Oldways Monograph 1995). At this international symposium, it wasconcluded that tree nuts, as one of the integral plant foods in the traditional Mediterraneandiet, had been overlooked by the nutrition research community. In 1997, the World CancerResearch Fund (WCRF) acknowledged that nuts and seeds, which have been common inhuman diets since pre-agricultural peoples, are nutrient dense and a good source ofunsaturated fats, protein, dietary fiber and micronutrients. The WCRF referred to brazil nuts,macadamias and cashews as seeds.
However, the WCRF pointed out, nuts needed to be identified separately in human studies tobetter evaluate their protective effects on human health. Since the mid 1990’s, INC hassupported research globally and has held research forums in Europe and North America.

International Tree Nut Council (INC) - 4 - June 15, 2002
For further information on this report, please contact Don Soetaert, INC President.
U.S. Contact Information:International Tree Nut Council2413 Anza AvenueDavis, CA 95616Ph.: (+1-530) 297-5895Fax: (+1-530) [email protected]
INC Headquarters:Consejo Internacional de los Frutos SecosCalle Boule 2,43201 Reus, SpainPh.: (+34-977) 331416Fax: (+34-977) [email protected]
International Tree Nut Council (INC) - 5 - June 15, 2002
Table 1: Tree nut Producing Countries
ALMONDS (AL)
AFGHANISTANAUSTRALIA
CHILEIRAN
ISRAELITALY
GREECEMOROCCOPORTUGAL
SPAINTUNISIATURKEY
USA
AMAZONIASBRAZILS (BR)
BOLIVIABRAZIL
EQUADORPERU
CASHEWS (CA)
BRAZILCHINAINDIA
INDONESIAGUINEA BASAL
KENYAMOZAMBIQUE
NIGERIATANZANIATHAILANDVIETNAM
HAZELNUTS (HA)
FRANCEGREECE
ITALYSPAIN
TURKEYRUSSIA
USA
MACADAMIAS (MA)
AUSTRALIABRAZIL
COSTA RICAGUATEMALA
ISRAELMALAWI
SO. AFRICATHAILAND
USA
PECANS (PE)AUSTRALIA
ISRAELMEXICO
SO. AFRICAUSA
PINENUTS (PIN)CHINAITALY
PORTUGALSPAIN
TURKEY
PISTACHIOS (PI)GREECE
IRANITALYSYRIA
TURKEYUSA
WALNUTS (WA)ARGENTINA
CHILECHINA
FRANCEGREECE
HUNGARYINDIAIRANITALY
MALDOVANO. KOREA
TURKEYUKRAINE
USA

International Tree Nut Council (INC) - 6 - June 15, 2002
B. Global Tree Nut Production
Following is a summary of global tree nut production. Data is based on information gatheredfrom producing country government statistics and industry sources (brazil and cashew datafrom FAO production database).
TREE NUT 2001 PRODUCTION (Metric Tons)Shelled Inshell
Almonds 469,000Brazil Nuts 67,700Cashews 1,100,000Hazelnuts 850,000Macadamias 21,600Pecans 190,000Pinenuts 5,000Pistachios 224,000Walnuts 528,000
International Tree Nut Council, 2002
C. Worldwide Tree Nut Consumption
Tree nuts are widely consumed in both raw and processed forms. Unlike groundnuts, whichare predominantly used for oil and feeding stuff, tree nuts are primarily consumed as wholefoods, as ingredients in foods, or in medicinal preparations. For example, in several Asiancultures, almonds play a significant role in Auyervedic preparations, a philosophy which forthousands of years has promoted the interrelationship of nutrition/diet with healing,prevention and longevity.
Per Capita ConsumptionLocation Kg/Year Range
Africa 1.0 0.0 - 7.3N. and C. America 2.3 0.0 - 3.3South America 0.5 0.0 - 6.4Asia (inc. Middle East) 1.0 0.2 - 13.6Europe 2.8 0.6 - 9.9Oceania 2.6 0.1 - 3.4World 1.3 0.0 - 13.6FAO 1999 Food Balance Sheets
Based on data contained in the 1999 FAO Food Balance Sheets, it is apparent that tree nutconsumption varies both among and within the regions where there is tree nut production. Forinstance, the European region is shown as having consumption of 2.8 kg/person per year.However, when looking more closely at individual country consumption within that region,Spain and Greece (tree nut producers) have consumption levels of 7.3 and 9.9 kg/person,respectively. The variations in consumption between North and South Europe are even moreapparent in the food availability (as kg/cap/year) calculations done by Nanos and

International Tree Nut Council (INC) - 7 - June 15, 2002
Gerasopoulos (2001) with EU (4.0), Spain (6.7) and Greece (10.0). They also cite that treenuts are five times more available to Greeks than U.S. consumers. Consumption levels inAsia, with vast population levels, are even more skewed.
An obsession to lower fat took its toll on the consumption of tree nuts in North America in the1980-1990s. As more recent research emerged on unsaturated fats and health, dietaryrecommendations have moved toward moderate rather than low fat with specific focus on theneed for unsaturated fatty acids in the diet. Tree nuts are poised to lead the way to bring focusto and examine what is going on in scientific research as well as changes in dietary guidance,food and healthy eating patterns, media coverage and consumer nutrition and health trendsthat have implications for tree nuts. As the science on nuts unfolds in key nutrition researchareas of health promotion and disease prevention, nuts are gaining more prominence as awhole food choice that can help promote good health. The strength of the scientific body ofevidence is convincing that nuts, which contain predominantly unsaturated fat, are linked tolowering blood cholesterol and heart disease risk. Along with reduction in heart disease risk,there is new, emerging science in weight management, type II diabetes, hypertension andcancer all of which have further implications for nuts or the components of nuts in healthfuleating.
D. Implications and Directions for Increased Trade and Consumption
Exports of tree nuts have seen double digit increases from 1990 to 20001. In particular,increases have occurred in a number of developing countries in Africa, which dominatescashew production, and China, which is now a significant supplier of walnuts to the worldmarket. With increased tree nut production, there is an opportunity for expandedconsumption of tree nuts in a number of markets, particularly those in need of food-basednutritional supplements. Nutrition research, conducted in North America, Europe and Asia,has demonstrated that tree nuts provide important macro- and micronutrients includingprotein, unsaturated fats, vitamins and minerals. In addition, tree nuts are a source ofimportant phytochemicals and antioxidants, which have been shown to have beneficial effectson overall health. Tree nuts also provide a valuable source of vegetable protein and calcium.
In many countries, a public health priority is basic nutrition and insufficient food supply.Tree nuts are perceived to be comparatively expensive to other plant foods such as legumes orbeans. However, this constraint is being overcome by increased production, which islowering cost and increasing availability. In addition, on-going bilateral and multilateralnegotiations are resulting in agreements which reduce tariffs and duties, in addition toharmonizing phytosanitary requirements that are potential barriers to trade.
WHO (1990) recommended that a minimum of 30g/day of a combination of nuts, seeds andpulses be included within its recommendation of a minimum intake of 400g/day of vegetablesand fruits. This recommendation was focused on some types of cancer, as well as coronaryheart disease. In the current report of the Expert Consultation, nuts are only specificallymentioned in terms of CVD. It is important to note that nutrition research has demonstratedthat as little as 30 grams of nutrient dense nuts per day can have a positive effect on
1 FAO Statistical Database, 1990-2000; exports of almonds, brazils, cashews, hazelnuts,pistachios and walnuts. No data was available for pinenuts, pecans, and macadamias.

International Tree Nut Council (INC) - 8 - June 15, 2002
health. Moreover, tree nuts are a nutrient-dense, shelf-stable, non-perishable, whole foodsource of valuable micro- and macronutrients, which are crucial considerations in countrieswith limited controlled storage or processing facilities.
2. Summary of Tree Nut Research
A. Health Outcome Studies – USA
Nuts and Cardiovascular DiseaseHu and Stampfer (1999) summarized the relationship between nut consumption and risk ofcoronary heart disease (CHD) as, “So far, five large prospective cohort studies (the AdventistHealth Study, the Iowa Women’s Health Study, the Nurses’ Health Study, the Physicians’Health Study and the CARE Study) have examined the relation between nut consumption andthe risk of CHD, and all have found an inverse association. In addition, several clinicalstudies have observed beneficial effects of diets high in nuts (including walnuts, peanuts,almonds and other tree nuts) on blood lipids. The beneficial effects of nut consumptionobserved in clinical and epidemiological studies underscores the importance of distinguishingdifferent types of fat.” Ellsworth et al. (2001) further examined the specific relationshipbetween the frequency of nut intake and risk of death in the 34,111 postmenopausal women inthe 12-year Iowa Health Study and concluded frequent nut consumption may offer thesewomen modest protection against the risk of death from all causes and CHD. Theyrecommended that future studies should consider using a more precise way to measure nutintake.
Based on the data from the Nurses’ Health Study, the researchers estimated that substitutingone ounce (~28 grams) of nuts for the equivalent energy from carbohydrate in an average diet,was associated with a 30% reduction in CHD risk. The substitution of nut fat for saturated fatwas associated with a 45% reduction in risk. Hu and Stampfer (1999) concluded regular nutconsumption can be recommended in the context of a healthy and balanced diet.
Fraser et al. (1992) reported on the cohort investigation of 31,208 non-Hispanic, white,California Seventh-Day Adventists with detailed information on how the nut-eating cohortswere healthier and less obese. For six years annual questionnaires were mailed to allparticipants as a screening mechanism for CHD and any hospitalization. Much to theirsurprise, upon study completion and analysis, subjects who consumed nuts frequently(>4x/week) had less CHD, despite all covariant adjustments. The apparent protective effectof nuts was independent of established coronary risk factors such as age, sex, smoking habits,history of hypertension, relative weight and physical exercise. They also found thatconsumers of nuts were less obese. Numerous components in nutrient dense tree nuts arereported to contribute to their protective effect in reducing the risk of heart disease:unsaturated fatty acids, vitamin E, magnesium, copper and arginine (Cooke et al. 1993,Durlach 1998, Klevay 1993, and Kris-Etherton et al., 1999). Kris-Etherton reviewed 18feeding trials that used diets containing nuts and found that there was a 25% greatercholesterol lowering response than predicted from equations for blood cholesterol, in responseto changes in dietary fatty acids. They concluded that these results suggest that there are non-fatty acid constituents in nuts that have additional cholesterol-lowering effects (Kris-Ethertonet al., 1999).

International Tree Nut Council (INC) - 9 - June 15, 2002
Nuts and Obesity/VegetarianismSabaté and Blix (2001) summarized the frequency of nut consumption in relation to all-causemortality in several California Seventh-Day Adventist sub-populations and found reducedhazard ratios for nut consumers, regardless of age, sex, race or fitness status. In three dietarysubgroups, the prevalence of obesity at baseline between vegetarian and non-vegetariangroups was also strikingly different (Sabaté and Blix, 2001). For both men and women, BMIincreased as the frequency of meat consumption increased. Vegetarian men and women had atwo point lower BMI value than non-vegetarians. Although these results were for middleaged (45-60 years) subjects, similar results were observed for other ages.
Summarized BMI data from the four large published studies of adult vegetarians, (Key et al.,1998), allow a comparison with non-vegetarian counterparts of the same cohort. Vegetariansin each study on average had 1 to 2 points lower BMI values than meat eaters within the samegroup. This difference is similarly observed in men and women. There is a substantialvariation in BMI values, with USA having greater BMI than European cohorts. This can beattributed to methodological differences in data collection, geographic location, seculartrends, and ethnic or genetic differences. Overall, these epidemiological data clearly suggestthat meatless diets are associated with lower overall BMI scores and low prevalence ofobesity in adults.
Hu et al. (1998) concluded from the Nurses’ Health Study that persons who consumed morenuts tended to weigh less, indicating that in practice, the energy contained in nuts can readilybe balanced by reductions in other sources of energy or increased physical activity.Finally, it is well known that vegetarians consume more nuts than non-vegetarians (3.7servings/wk vs. 2.1 for non-vegetarians) (Rajaram and Wien, 2001).
B. Health Outcome Studies – Europe
In respect to prevention of degenerative diseases such as cardiovascular disease (CVD) andcancer, the importance of antioxidant supply with daily nutrition is increasingly recognized(Langseth 1995). Ginter (1998) reports that the CVD epidemic in Central and Eastern Europeseems to be only partially associated with a high prevalence of traditional risk factors(hypercholesterolemia, hypertension, smoking). Hence, the effect of traditional risk factorsmay be intensified by additional unidentified factors, such as environmental and psychosocialproblems, and specific nutritional antioxidant deficiencies (antioxidant vitamins, flavonoids,folic acid). The intake of antioxidants from fruits, vegetables, nuts and vegetable oils wasreported to be substantially lower in most Eastern European countries than in the West (Ginter1998). Thus, in Eastern Europe factors increasing free radical production may not besufficiently counterbalanced by protective nutritional antioxidants, and oxidative stress playsa crucial role in CVD pathogenesis.
In contrast, Mediterranean diets are known for a high tocopherol (vitamin E) content, aparticularly important antioxidant (Trichopoulou and Vasilipoulou 2000; Kafatos, 1999;Colquhoun, 2000). It’s been shown that apparent benefits of the Mediterranean diet seem tobe transferable to population groups from different origins and dietary habits (Kouris-Blazoset al., 1993; Noah and Truswell, 2001), Trichopoulou and Vasilopoulou (2000) concluded,that a diet that adheres to the principles of the traditional Mediterranean one is associated withlonger survival. The Mediterranean diet as secondary prevention measure is also inexpensive

International Tree Nut Council (INC) - 10 - June 15, 2002
compared to other diets or drug treatments (see Table 9 in Colquhoun, 2000). As a primarilyplant food-based diet, the Mediterranean diet is characterized by a large variety of foods highin beta-carotene, vitamin C, vitamin E, minerals and phytochemicals. This traditional dietalso has a moderate to high fat content (e.g., Italy 30%, Greece 40% of daily energy intake)(Trichopoulou and Lagiou, 1997), compared to widely promoted lower fat diets. However, theMediterranean dietary fat is typically rich in beneficial unsaturated, primarilymonounsaturated, fatty acids (MUFA), and is low in saturated fatty acids (SFA).
Tree nuts provide a similar fatty acid profile and also contain protein, fiber, importantvitamins and minerals, and phytochemicals. For example, almonds and hazelnuts areexcellent sources of natural alpha-tocopherol (AT). One ounce (28.35 g, 1 handful) provides7.3 mg AT (USDA, 2001). Walnuts are a rich, plant-based source of omega-3 fatty acids andcontain a favorable ratio of omega-6 to omega-3 fatty acids. One brazil nut provides all of theselenium needed per day (N.A.S., 2000). Dr. de Longeril, the principal investigator from theLyon Heart Study, makes a compelling argument that scientists and physicians should have ashigh priority to study natural foods such as nuts to better understand the nature of theircardioprotective properties since they do better than aspirin or prevastatin for primaryprevention of CHD (de Longeril et al., 2001).
Many European epidemiological studies have assessed nut intake. However, assessmentand/or analysis was often done without differentiation, and different dietary assessmentmethodologies were used (i.e., diet history, Food Frequency Questionnaire, 24-hour dietaryrecall or dietary records/diary). For example, (a) tree nuts and groundnuts (peanut, a legume)are assessed together as 'nuts' or 'snacks' (e.g. Slimani et al., 2000; DIfE, 1995; Thiebaut et al.,2001; Verschuren et al., 1993); (b) nuts are assessed or listed in the food group 'fruits', maybecombined with seeds as a specific food sub-group (e.g. Slimani et al., 2000; Döring et al.,1998; Panico et al., 1992). Hence additional analyses of existing databases should bewarranted to get a better picture of specific tree nut intake and their contribution to energy andnutrient supply in conjunction with chronic disease prevention. In development of futuredietary instruments for health surveillance tree nuts should be separately considered as keyfoods.
Serra Majem et al. (2000) observed in their Canary Island cross-sectional dietary survey, afairly low nut consumption of 2 g/day for the 6-75 year old representative population sample.Also the Spanish enKid Study, a population-based, cross-sectional nutrition survey in childrenand youth aged 2-24 years, showed for both gender a low mean daily consumption of 5 g/dayof 'dry fruits and nuts' (Serra-Majem et al. 2001), and moreover, low consumption of fish,fruits and vegetables. All typical elements of the Mediterranean diet. The authors stressed thechanges in feeding habits that have occurred in Spain, especially in the youth, where thecharacteristics of the Mediterranean diet are unraveling. Data from the Dietary and NutritionalSurvey of British Adults showed that only 12% of the adult population ate any unsalted nuts,with an average intake of only 8 g/week (Gregory et al., 1990). Results from the GermanNutrition Survey 1998 (Mensink et al., 2000) show low mean intakes for the combined foodgroup of 'nuts, seeds and oil fruits', ranging from as low as 1 g/day in women aged 65-79years to 6 g/day in men in the age strata 35-44 and 45-54 years.

International Tree Nut Council (INC) - 11 - June 15, 2002
C. Human Clinical Trials
Cardiovascular Disease, Mixed Nut StudiesThere have been six published clinical trials involving mixed nuts (Bruce et al., 2000; Jenkinset al., 1997; Bruce et al., 1997; Abbey et al., 1994; Singh et al., 1992; Berry et al., 1991). Inall of the studies, the “nut diets” significantly reduced total cholesterol (TC) from 7-25% andlow-density lipoprotein (LDL) cholesterol by 10-33%. No studies found any significanteffect on HDL, and two found a significant decrease in triglycerides (TG) (Jenkins et al.,1997; Bruce et al., 1997; Abbey et al., 1994; Singh et al., 1992).
The most recent study involved 12 hyperlipidemic women in a crossover design that lasted fortwo 4-week periods. Subjects first consumed a refined-food diet and then switched to aphytochemical-rich diet primarily consisting of whole grains, legumes, fruits, vegetables,seeds and two tablespoons of almonds, hazelnuts or pecans per day. Compared to the refined-food diet, the phytochemical-rich diet lowered TC by 13% and LDL by 16% with nosignificant changes in HDL or TG (Bruce et al., 2000).
A second study involved 10 adults in a randomized crossover design that lasted for two 2-week periods. The control diet was the subjects’ habitual diet. The study diet consisted ofmainly vegetables, fruit, avocados and nuts (limited to 60-120g/day, average consumptionwas 100g/day). Compared to the control diet, TC was reduced by approximately 25%, LDLby 33% and TG by 20%, with no significant change in HDL (Jenkins et al., 1997).
Another intervention study, conducted in Australia, involved 15 adults who ate a plant-baseddiet that included whole grains, sun-dried raisins and mixed nuts (almonds, hazelnuts andwalnuts) and nut butters (almond and sesame). After four weeks, TC decreased by 8%, LDLdecreased by 15% and HDL was not significantly effected (Bruce et al., 1997).
The fourth study involved 16 normolipidemic men in a consecutive, supplemental field studythat lasted for three 3-week dietary periods. During the first three weeks, subjects consumed areference diet that included a background diet supplemented with 50g/day of peanuts, 40g/dayof coconut, and 50g/day of a coconut confectionary bar. During the second three weeks,subjects consumed the background diet supplemented with almonds (84g/day) and duringweeks 7-9, subjects consumed the background diet supplemented with walnuts (68g/day).Compared to the reference diet, the almond diet lowered TC by 7% and LDL by 10%, whilethe walnut diet lowered TC by 5% and LDL by 9%. Neither diet had a significant effect onHDL or TG (Abbey et al., 1994).
A fifth study, conducted in India, involved 406 patients who were recruited 24 to 48 hoursafter having an acute myocardial infarction (MI). The randomized, single-blind interventionstudy lasted 6 weeks. Subjects were divided into two groups. One group consumed Diet A inwhich meat and eggs were replaced by fish, vegetarian meat substitutes and nuts (almondsand walnuts). Those following Diet B ate a low-calorie, typical hospital diet, followed by adiet prescribed by their doctors. Those consuming Diet A had a 9% decrease in TC, 10%decrease in LDL and 9% decrease in TG compared with the initial levels and the changes indiet group B. Those following Diet A also had a 36% decrease in cardiovascular eventscompared to those consuming Diet B (Singh et al., 1992).

International Tree Nut Council (INC) - 12 - June 15, 2002
Finally, the Jerusalem Nutrition Study was a randomized, controlled crossover studyinvolving 18 young men that examined the effects of a high mono-unsaturated fat (MUFA)diet (including almonds, olive oil and avocado) versus a high polyunsaturated fat (PUFA) diet(including walnuts, safflower and soy oils) during two 12-week dietary periods. The MUFAdiet lowered TC by approximately 10% and LDL by 14% compared to baseline values, whilethe PUFA diet lowered TC by 16% and LDL by 21%. There were no significant effects onHDL or TG (Berry et al., 1991).
Cardiovascular Disease, Single Nut Studies (alphabetical order)
AlmondsAn almond meta-analysis was just reported for seven studies (Fulgoni et al., 2002). Therehave been four published clinical trials involving almonds and all found that the almond dietssignificantly reduced TC (range 8-12%) and LDL (range 9-15%). There were no significantchanges in HDL or TG (Hyson et al., 2002; Spiller et al.,1998; Berry et al., 1992; Spiller etal., 1992.) The Mediterranean-diet-type study involved 45 hypercholesterolemic adults in arandomized, controlled, parallel study that lasted four weeks (following one week on abaseline diet). The control group consumed a diet of whole and unrefined foods plus 85g/dayof cheddar cheese, 28g/day of butter, and 21g/day of rye crackers. The olive oil groupconsumed a base diet of whole and unrefined foods plus 48g/day of olive oil, 113g/day ofcottage cheese and 21g/day of rye crackers. The almond group consumed the same base dietof whole and unrefined foods plus 100g/day of raw, unblanched almonds (both whole andground). The almond diet lowered TC by 12% and LDL by 15% compared to baselinevalues, while the olive oil diet had no significant effects (Spiller et al., 1998). A recentclinical trial on almonds compared whole almonds and almond oil and found they had similarcholesterol-lowering effects, which were greater than accounted for by the MUFA contentalone, indicating that other fat soluble components (alpha-tocopherol vitamin E, phytosterols)contribute to the beneficial effects on plasma lipids (Hyson et al., 2002). The first doseresponse study, a randomized, crossover study of 27 hyperlipidemic men and women with full(73g) or half almond dosage, has been accepted to a medical journal (Kendall et al., 2002a,b).The almonds had favorable effects on serum blood lipids and lipoprotein profile for those atrisk for CHD. A dose-response relationship was evident and almonds reduced oxidation ofLDL cholesterol. The authors concluded that the significant reduction in CHD risk factorswas in part related to the non-fat components of the almond (Kendall et al., 2002a,b).
HazelnutsThirty healthy medical students added 1 gram of hazelnuts per kilogram of body weight perday to their normal daily diet for 30 days. TC was lowered by 6%, LDL by 19%, while HDLincreased 7% and TG 25% compared to baseline values. Plasma antioxidant potential (AOP)also increased by 20% (Durak et al., 1999). Alphan et al. (1997) gave 19 patients with non-insulin dependent diabetes a diet supplemented with hazelnuts to provide 40% of energy fromcarbohydrates and 45% from fat. Compared to the baseline diet (60% carbohydrates, 25%fat), triglycerides were not significantly altered after consumption of the hazelnut diet. Totalcholesterol and LDL were significantly lowered, HDL was not significantly changed.
MacadamiasTwo randomized, crossover studies have examined the effects of macadamias on cholesterollevels. Both studies reported a reduction in TC (range 5-8%), LDL (range 5-11%) and TG

International Tree Nut Council (INC) - 13 - June 15, 2002
(range 10-21%). Only one of the studies found a significant effect on HDL (5% decrease)(Curb et al., 2000; Colquhoun et al.,1996). The more recent study involved 30 subjects whoconsumed three different diets each for 30 days. The first diet was a typical American diet(AM), high in saturated fat, the second diet was the American Heart Association (AHA) Step1 diet, and the third diet was a macadamia-based diet (MAC) high in monounsaturated fattyacids. Compared to the AM diet, the MAC diet lowered TC, LDL and HDL each by 5% andTG by 10%. The AHA diet had similar results except for an 8% increase in TG (Curb et al.,2000).
PecansA randomized, controlled, parallel study involved 19 healthy adults who followed either acontrol diet (no nuts) or a pecan diet which included 68 grams of pecans per day (with noadditional nuts). After eight weeks, those following the pecan diet had a 6% decrease in LDLcompared to the baseline value. Effects on TC, HDL and TG were not significant (Morganand Clayshulte, 2000).
PistachiosTwo studies have looked at the effects of pistachios on blood lipid levels. In one study, 10patients with moderate hypercholesterolemia were enrolled in a controlled, randomized,crossover study for two 3-week periods. A reference diet of 37% total fat was compared to apistachio diet of 39% total fat (66g/day of pistachios) in which 20% of the daily caloric intakewas substituted with pistachios. Compared to initial values, the pistachio diet decreased totalcholesterol by 2% and increased HDL by 12%, while there was no significant effect on LDLor TG (Edwards et al., 1999).
Most recently, researchers observed that daily inclusion of pistachios in the diet can decreasetotal cholesterol and LDL in subjects with moderate hypercholesterolemia (fasting serumcholesterol > 250 mg/dl). Ten subjects were randomized to the pistachio group (20% of dailycaloric intake from pistachios) and 10 to the regular snack group and crossed-over at fourweeks. Both diets were maintained isocaloric, with pistachios substituted for the usual snacksthe subjects consumed during the day. On the pistachio diet, significant reductions were seenin total cholesterol (247+5 vs. 234+6, p=0.02), LDL (165+6 vs. 147+8, p=0.006) and APOB(133+4 vs. 117+4, p=0.002). Significant increase was observed in APOA (139+7 vs. 151+7,p=0.006). In subjects on the regular snack food diet, no lipid values were significantlydifferent from baseline. (Erario et al., 2001).
WalnutsA recent scientific review of all walnut-specific clinical research concluded that the body ofresearch is strong that eating walnuts reduces the risk for heart disease due to theirpreventative properties. Key findings suggest that: (1) consuming walnuts did not cause a netgain in body weight ; (2) walnuts decreased serum cholesterol and reduced heart disease risk;(3) walnuts are unique among nuts due to their polyunsaturated fat (omega-3 and omega-6)fatty acid content. The author, and four independent experts, evaluated the content andquality of scientific evidence for a potential beneficial health relationship between the intakeof walnuts and the reduction and prevention of coronary heart disease. Five controlled, peer-reviewed, human clinical walnut intervention trials involving approximately 200 subjectsconsidered representative of the adult population in the United States at risk of coronary heartdisease were reviewed. Daily intake of 48-84 grams of walnuts lowered low-density

International Tree Nut Council (INC) - 14 - June 15, 2002
lipoprotein cholesterol with little effect on high-density lipoprotein cholesterol and had otherbeneficial effects on blood lipids, all of which have been shown in numerous other studies toreduce the risk of coronary heart disease, according to the lead author. (Feldman, 2002).
In four published clinical trials involving walnuts, all found that the walnut diets reduced TC(range 4-12%) and LDL (range 8-16%) (Zambon et al., 2000; Chisolm et al., 1998; Sabaté etal., 1993). HDL decreased by 5% in one study (Sabaté et al., 1993), increased by 14% inanother (Chisolm et al., 1998), and remained unchanged in the other two (Zambon et al.,2000; Iwamoto et al., in press 2002). No significant changes were reported in TG levels inthree of the studies (Iwamoto et al., 2002; Chisolm et al., 1998; Sabaté et al., 1993), while onefound an 8% decrease (Zambon et al., 2000). Apo A-1 levels were measured in only onestudy, which showed a 5% decrease (Zambon et al., 2000). Three studies measured APOBlevels and observed a decrease of 7-13%. Only one study recorded lipoprotein(a) levels (9%decrease) and VLDL levels (12% decrease) (Zambon et al., 2000).
The most recent walnut study was a randomized, crossover feeding study in which 49 adultswith hypercholesterolemia consumed a Mediterranean diet (MD) emphasizing vegetableproducts, fish and olive oil (no nuts), and a walnut diet (WD) which partially replaced oliveoil and other fatty foods of the MD with 41-56 grams of walnuts per day. Compared tobaseline values, the WD and MD lowered TC by 9% and 5%, and LDL by 11% and 6%,respectively, but had no significant effect on HDL. Only the WD lowered TG by 8%(Zambon et al., 2000).
Obesity/Weight ReductionCiting results from various almond, macadamia, and walnut clinical studies, Fraser (1999)stated: “Several investigators have noted that in certain human nut feeding studies, thatincluded only limited dietary advice, weight gain was not a problem despite supplements ofseveral hundred calories of nuts and/or nut fat each day. Suggested explanations for such apossible result include a satiety effect of nuts compensating for the additional nut calories bydecrease intake of other foods; limited absorption of the fat due to the nut fiber or poormastication; or an unexplained metabolic effect whereby nut fats are ‘burned’ rather thanstored, perhaps associated with a higher metabolic rate.” Fraser et al. (2002) found thatincorporating 320 kcal of almonds into the daily diet of 81 free-living subjects for six monthsdid not lead, on average, to statistically or biologically significant changes in body weight.Long term daily almond consumption improved the fatty acid and micronutrient profiles andeating patterns of free-living individuals.
In a recent randomized, parallel study, 101 overweight adults were followed for 18 months.Subjects were divided into two groups and consumed one of two study diets, both of whichwere calorie controlled (1200 kcal/day for women; 1500 kcal/day for men). The low-fat diet(LF) had a total of 20% calories from fat, while the high-unsaturated fat diet (UNSAT)consisted of 35% total fat and included tree nuts, peanuts, canola and olive oils.
After six months the average weight loss was comparable in both groups. However, there wasa significant difference at the end of the 18 months in participation rates. In the LF group,only 20% were still actively participating in the study compared to 54% of the UNSAT group.One factor which may contribute to the greater participation rate is that a moderate fat diet

International Tree Nut Council (INC) - 15 - June 15, 2002
may induce the feelings of satiety after a snack or meal. In addition, the participants in theunsaturated group reported that they did not feel like they were “dieting” and therefore, didnot feel deprived (McManus et al., 2001).
DiabetesA number of studies have linked the rate of carbohydrate digestion with risk of chronicdisease. The standardized method of measuring the rate of carbohydrate digestion in vivo is byuse of the glycemic index. The glycemic index (Jenkins et al., 1981; Brand Miller, 1994;Wolever et al., 1991) allows ranking of foods from those which give rise to the highest bloodglucose and insulin response (high glycemic food) to those associated with the lowest bloodglucose and insulin response (low glycemic index foods). Epidemiological studies haveshown that a low glycemic index diet is linked to reduced risk for type II diabetes (Salmeronet al., 1997; Salmeron, Ascherio et al., 1997), cardiovascular diseases (Liu et al., 2000) andcancer (Corpet et al., 1998). In experimental studies in type II diabetic subjects, a lowglycemic index diet is seen to improve important risk factors, such as glycated hemoglobins(Jenkins et al., 1988; Brand et al., 1991; Järvi et al., 1999), clotting factors (Järvi et al., 1999)and HDL levels (Luscombe et al., 1999).
Nuts are good sources of unsaturated fatty acids, vegetable protein, fiber and associatedantioxidant flavonoids, which in a limited number of studies, have independently been shownto have a number of effects including blunting the postprandial glucose rise, improvingcarbohydrate tolerance and reducing risk factors for diabetic complications (Garg, 1998;Sarkkinen et al., 1996; Chandalia et al. 2000; Kaneto et al., 1999; Paolisso et al., 1993). Nutsare also associated with protection from the development of type II diabetes in large cohortstudies (Salmeron et al., 1997a,b).
INC is currently funding research at the University of Toronto to look at the glycemic effectof tree nuts in both non-insulin dependent and non-diabetics. Preliminary findings show thatnuts are a very low glycemic food. The researchers plan to conduct a large, multi-center,multi-national study to further investigate the effects of nuts on diabetes. In collaborationwith this study, other research is ongoing to evaluate the relationship between the structure ofnuts, digestibility, and bioavailability of nutrients (Ren et al., 2001).
CancerIn a report by the World Cancer Research Fund (WCRF) and the American Institute forCancer Research (AICR) the authors concluded, “While there are theoretical reasons tobelieve that diets high in nuts and seeds might protect against some cancers, the evidence iscurrently lacking.” (AICR, 1997).
A year later, a study was published on prostate cancer, the most prevalent cancer among men,representing a large and growing health problem in the U.S. and other Western countries. Inthis large, 59-country study, researchers tried to identify predictive measures for prostatecancer mortality. They concluded, “The specific food-related results from this study areconsistent with previous information and support the current dietary guidelines andhypothesis that grains, cereals and nuts are protective against prostate cancer.” (Hebert et al.,1998).
International Tree Nut Council (INC) - 16 - June 15, 2002
Currently, a clinical trial study is underway in China to evaluate the effect of fortified almondmilk on the antioxidant status and immune systems of cancer patients while undergoingtreatment.
3. Tree Nut Composition
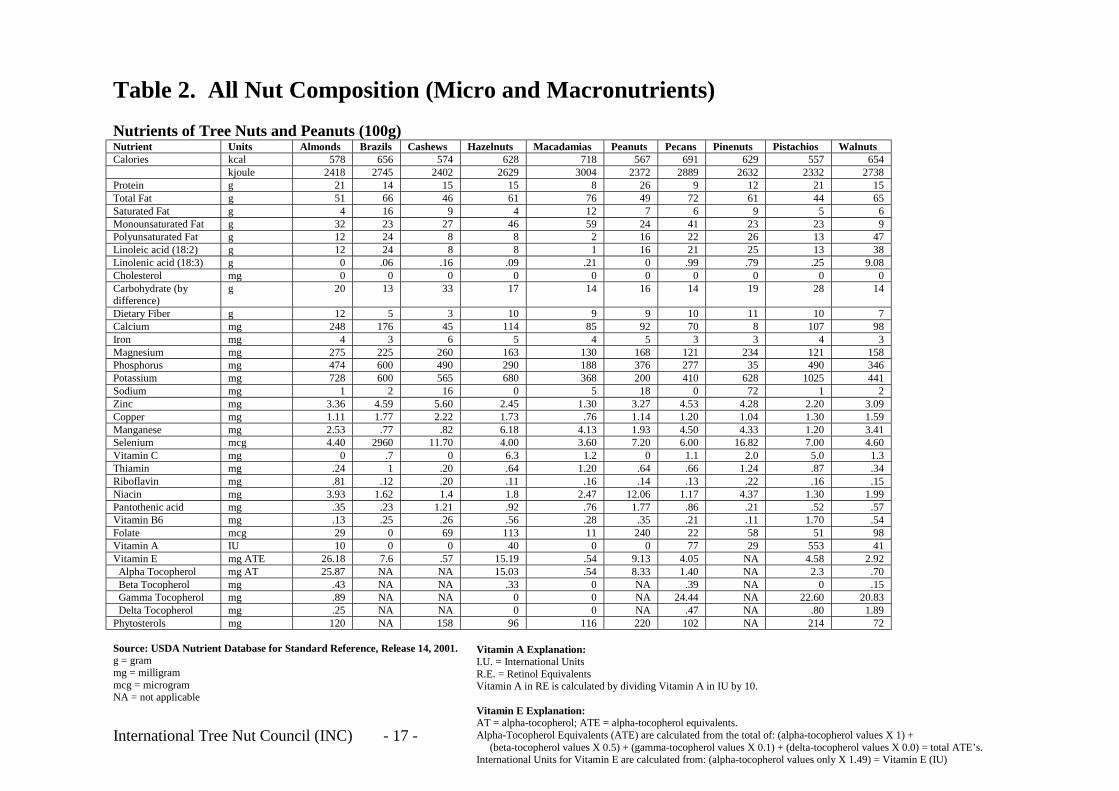
In 1999, INC worked closely with U.S. Department of Agriculture (USDA) to reanalyze all ofthe tree nuts for their nutritional content. This information was then added to the USDAnutrient database (see Table 2).
In addition to the macro- and micronutrients, a variety of phytochemicals (i.e., ellagic acid,phenolic compounds, luteolin and tocotrienols) are also present in tree nuts (Borchers, 2001).Research has shown that these plant chemicals may help reduce the risk of heart disease,certain cancers and other chronic diseases. INC is currently working with USDA again, toanalyze the flavonoid content of tree nuts, as part of a large program to establish a flavonoiddatabase. This is an area of great interest for plant based foods overall, as flavonoids areantioxidants, and a number of in vitro and in vivo studies are showing protective effects(Hollman et al, 2000). For almonds two recent studies have identified and quantified the rangeof flavonoids in almonds skins for the first time (Frison-Norris and Sporns, 2002; Sang et al.,2002).Research to assess the benefical effects for humans are ongoing. Preliminary datashould be available by Fall 2002. The final data will appear in the USDA nutritional databaseand the findings will be published in 2003.
International Tree Nut Council (INC) - 17 - Jun
Table 2. All Nut Composition (Micro and Macronutrients)
Nutrients of Tree Nuts and Peanuts (100g)Nutrient Units Almonds Brazils Cashews Hazelnuts Macadamias Peanuts WalnutsCalories kcal 578 656 574 628 718 567 654
kjoule 2418 2745 2402 2629 3004 2372 2738Protein g 21 14 15 15 8 26 15Total Fat g 51 66 46 61 76 49 65Saturated Fat g 4 16 9 4 12 7 6Monounsaturated Fat g 32 23 27 46 59 24 9Polyunsaturated Fat g 12 24 8 8 2 16 47Linoleic acid (18:2) g 12 24 8 8 1 16 38Linolenic acid (18:3) g 0 .06 .16 .09 .21 0 9.08Cholesterol mg 0 0 0 0 0 0 0Carbohydrate (bydifference)
g 20 13 33 17 14 16 14
Dietary Fiber g 12 5 3 10 9 9 7Calcium mg 248 176 45 114 85 92 98Iron mg 4 3 6 5 4 5 3Magnesium mg 275 225 260 163 130 168 158Phosphorus mg 474 600 490 290 188 376 346Potassium mg 728 600 565 680 368 200 441Sodium mg 1 2 16 0 5 18 2Zinc mg 3.36 4.59 5.60 2.45 1.30 3.27 3.09Copper mg 1.11 1.77 2.22 1.73 .76 1.14 1.59Manganese mg 2.53 .77 .82 6.18 4.13 1.93 3.41Selenium mcg 4.40 2960 11.70 4.00 3.60 7.20 4.60Vitamin C mg 0 .7 0 6.3 1.2 0 1.3Thiamin mg .24 1 .20 .64 1.20 .64 .34Riboflavin mg .81 .12 .20 .11 .16 .14 .15Niacin mg 3.93 1.62 1.4 1.8 2.47 12.06 1.99Pantothenic acid mg .35 .23 1.21 .92 .76 1.77 .57Vitamin B6 mg .13 .25 .26 .56 .28 .35 .54Folate mcg 29 0 69 113 11 240 98Vitamin A IU 10 0 0 40 0 0 41Vitamin E mg ATE 26.18 7.6 .57 15.19 .54 9.13 2.92 Alpha Tocopherol mg AT 25.87 NA NA 15.03 .54 8.33 .70 Beta Tocopherol mg .43 NA NA .33 0 NA .15 Gamma Tocopherol mg .89 NA NA 0 0 NA 20.83 Delta Tocopherol mg .25 NA NA 0 0 NA 1.89Phytosterols mg 120 NA 158 96 116 220 72
Source: USDA Nutrient Database for Standard Reference, Release 14, 2001.g = grammg = milligrammcg = microgramNA = not applicable
Vitamin A Explanation:I.U. = International UnitsR.E. = Retinol EquivalentsVitamin A in RE is calculated by dividin
Vitamin E Explanation:AT = alpha-tocopherol; ATE = alpha-tocAlpha-Tocopherol Equivalents (ATE) are (beta-tocopherol values X 0.5) + (gamInternational Units for Vitamin E are calc
Pecans Pinenuts Pistachios691 629 557
2889 2632 23329 12 21
72 61 446 9 5
41 23 2322 26 1321 25 13.99 .79 .25
0 0 014 19 28
10 11 1070 8 107
3 3 4121 234 121277 35 490410 628 1025
0 72 14.53 4.28 2.201.20 1.04 1.304.50 4.33 1.206.00 16.82 7.00
1.1 2.0 5.0.66 1.24 .87.13 .22 .16
1.17 4.37 1.30.86 .21 .52.21 .11 1.7022 58 5177 29 553
4.05 NA 4.581.40 NA 2.3
.39 NA 024.44 NA 22.60
.47 NA .80102 NA 214
e 15, 2002
g Vitamin A in IU by 10.
opherol equivalents. calculated from the total of: (alpha-tocopherol values X 1) +ma-tocopherol values X 0.1) + (delta-tocopherol values X 0.0) = total ATE’s.ulated from: (alpha-tocopherol values only X 1.49) = Vitamin E (IU)


International Tree Nut Council (INC) - 19 - June 15, 2002
4. Specific Feedback on WHO/FAO Draft Report
The Expert Consultation raises many important considerations in advancing the crucial role ofdiet and nutrition in the prevention of chronic diseases. In particular, noting the changes inthe world food economy from the standpoint of dietary patterns and lifestyle is a key elementto moving a nutrition dialog forward. However, equally important is to recognize there is no“worldwide” dietary strategy - rather than trying to encourage categorization of “good foods”versus “bad foods,” the nutrition discussion must elevate the strategy to one which promotesbalance in food and nutrition choices and respects regional, ethnic, and cultural differences.
Unlike earlier reports, the current report often associates energy-density with high fat, withoutalways acknowledging the beneficial effects of the type of fat in a diet - e.g. foods which areenergy-dense in mono- and polyunsaturated fats versus saturated fats can play a vital role inan overall healthy diet. Krawczyk (2001) has clearly shown when reviewing the dietaryguidelines for fat around the world that guidance on dietary fat is influenced by level ofprosperity or poverty within a country (which may encompass the two extremes), local cultureand tradition, and domestic food production. He concludes that although some countriesrecommend limiting total fat, more focus is placed on reducing saturated fat in the diet, withan increasing number of countries starting to give advice on levels of polyunsaturated and/ormonounsaturated fatty acids in the diet. Among the authorities which have moved in thedirection of types of fat recommended is the American Heart Association (Krauss et al.,2001). Scientific research is refining our understanding of nutritional benefits, allowinggreater flexibility in food choices which provide diversity and alternative sources of valuablemicro-/macronutrients. The report therefore must provide a framework for incorporatingfoods into dietary strategies as research clarifies and demonstrates their contribution to anoverall healthy diet.
The role of the food industry should not be undervalued in this discussion. From the producerthrough the processor, it is often the food industry which is working in partnership withgovernments, NGOs, consumer organizations, and health influencers to support nutritionresearch and the dissemination of dietary information. In addition, it is these producer-industry groups which must balance the commercial, practical aspects of the sustainability ofproduction in light of growing environmental concerns. In the case of tree nuts, production islargely traditional, low-intensity farming which is concentrated in developing countries.
The report is correct to notice the importance of organizations such as Codex Alimentarius inany dialog which involves dietary recommendations and management of chronic disease.However, Codex Alimentarius has the dual responsibility of also ensuring fair internationaltrade. Food safety guidelines agreed at an international level must consider the abilities of themost developed and the least developed; it makes no sense to establish international standardswhich are based on analytical methods of detection as opposed to true consumer health risks.In those situations, developing countries are unable to compete internationally, causinggreater economic pressure and balance of trade inequities.
There is some concern regarding the report’s recommendation to “tax” those foods which areassociated with being energy-dense or nutrient-poor as well as to pressure schools and otherpublic facilities to not have vending machines. WHO/FAO’s role should focus on theprovision of guidance in terms of nutrition recommendations and dietary guidelines.

International Tree Nut Council (INC) - 20 - June 15, 2002
However, the actual public policy strategies determined to be appropriate - whether it is tolimit vending machines in schools, fiscal pricing policies or limited advertising to children - isa discussion which must be left to national authorities, based on their individual internalpolicies and priorities.

International Tree Nut Council (INC) - 21 - June 15, 2002
5. Conclusions and INC Recommendations
Evolving Dietary Recommendations Highlight the Potential Role of Tree Nuts inHealthy Eating for Disease Prevention and Health Promotion
The emphasis on low-fat diets is now under scrutiny in the United States as a more moderateapproach has currently been taken for making dietary recommendations for fat intake. Whilelowering saturated fat to lower heart disease risk is well accepted, examining the amount andtype of fat associated with healthy eating has become the focal point. A “moderate” dietaryrecommendation approach to total fat, emphasizing unsaturated fat and whole food choices isincluded in the USDA Dietary Guidelines for Americans 2000. The 2000 American HeartAssociation (AHA) Dietary Guidelines recommendation to “limit foods high in saturated fatand cholesterol; and substitute unsaturated fat from vegetables, fish, legumes, and nuts”includes nuts in a more predominant role than the past (Krauss et al. 2000). In May 2001, theNational Institutes of Health’s National Cholesterol Education Program Report formalized itsrecommendation to keep total fat in the diet between 25-35% of calories (N.I.H. 2001). Therecommendation for polyunsaturated fat in the diet is up to 10 % of calories. It alsorecommended the consumption of monounsaturated fat up to 20% of calories. This is the firsttime monounsaturated fat has been officially “increased” as part of a recommended healthyeating plan. This has a major implication for all tree nuts, which contain significant amountsof unsaturated fatty acids.
In recent years, nutrition experts and Oldways Preservation and Exchange Trust have begunto recommend a Mediterranean-like diet characterized by abundant plant foods (fruit,vegetables, breads, other forms of cereals, beans, nuts and seeds), fresh fruit, olive oil, dairyproducts (principally cheese and yogurt), fish and poultry consumed in low to moderateamounts, zero to four eggs consumed weekly, red meat consumed in low amounts, and wineconsumed in low to moderate amounts, normally with meals (Oldways, 1995). Dietary datafrom the Mediterranean region shows the lowest recorded rates of chronic diseases and thehighest adult life expectancy. And, it has been shown that apparent benefits of theMediterranean diet seem to be transferable to population groups from different origins anddietary habits (Kouris-Blazos et al., 1999). The Mediterranean diet as a secondary preventionmeasure is also much less expensive compared to other diet or drug treatments (Colquhoun,2000).
While the majority of unsaturated fat and tree nut research-to-date has focused on heartdisease prevention, researchers are beginning to investigate the potential impact ofunsaturated fat and tree nut consumption on prevention of other chronic diseases includingweight management, diabetes type II, hypertension and cancer. These research areas areemerging and deserve some attention although much more research is needed
Weight ManagementAddressing the increasing problem of obesity in America has become the major focal point ofdietary recommendations in the United States. This shift in thinking ideally suits therecommendation for individual or whole foods to help build healthy eating patterns.However, caloric intake then becomes of greater importance. Nuts continue to shouldercommon misperceptions of being too high in fat and calories, and a food to be avoided.Healthy weight management requires an emphasis on calories and exercise. Recent studies do

International Tree Nut Council (INC) - 22 - June 15, 2002
not implicate unsaturated fat or nuts in the diet as a contributor to weight gain (Fraser et al.,2002). For example, a report in the 2001 Journal of International Obesity showed that anenergy-restricted diet containing 35% calories from fat (the extra fat coming from unsaturatedfat foods such as peanuts, peanut butter, tree nuts and olive oil) produced similarimprovements in body weight to a low-fat diet. And, an extra serving of vegetables wereconsumed by the high-unsaturated fat diet. Participation rates were significantly higher overan 18-month period for the high-unsaturated fat diet (McManus et al., 2001).
Diabetes Type IIThe American Diabetes Association currently recommends an individualized approach tonutrition that is based on the nutritional assessment and desired outcome of each patient. Thisapproach takes into consideration patient preferences, control of high blood sugar and highblood lipids (ADA, 2002). To achieve these nutritional goals, either high-unsaturated-fat dietsor low-saturated fat, high-carbohydrate diets are currently advised. A meta-analysis of variousstudies comparing these two approaches to diet therapy in patients with type II diabetes,revealed that high-monounsaturated-fat diets improve lipoprotein profiles as well as glycemiccontrol (Garg, 1998). Furthermore, there is no evidence that high-monounsaturated-fat dietsinduce weight gain in patients with diabetes mellitus, provided that energy intake iscontrolled.
The DASH Diet and Blood Pressure ControlResearch has shown that diet can affect high blood pressure (hypertension). The clinicalstudy, called "DASH" (or “Dietary Approaches to Stop Hypertension) (Svetkey et al., 1999),found that elevated blood pressure can be reduced with an eating plan low in saturated fat,total fat and cholesterol, and rich in fruits, vegetables and low-fat dairy foods. The planincludes 50g of nuts, seeds, and dry beans 4-5 times per week. The DASH diet is rich inmagnesium, potassium and calcium, as well as protein and fiber. Pistachios, almonds,walnuts and other tree nuts, peanuts, sunflower seeds, kidney beans, lentils and peas providethese important nutrients.
Diet and CancerCurrent recommendations for cancer prevention from the American Institute for CancerResearch (AICR) include, "Choose a diet rich in a variety of plant-based foods." While the1997 AICR report, Food, Nutrition and the Prevention of Cancer: a Global Perspective reportsno data on nuts and cancer, an epidemiological study has been published linking nutconsumption with decreased incidence of prostate cancer. The data on phytochemicals andbioactive components in nuts and other foods like fruits and vegetables is just beginning.Nuts contain phytosterols (beta-sitosterol), polyphenols (flavonoids, ellagic acid),phytoestrogens (isoflavonoids), tocotrienols, antioxidants, and nutrients like vitamin E andselenium which have been implicated in cancer prevention, although the science is still in itsinfancy stages.
INC appreciates the opportunity to contribute its comments to this draft report and to provideWHO/FAO with a summary of the diversity of research on tree nuts. In terms of therecommendations of the report, research has demonstrated that tree nuts are consistent withthe profile of plant-based foods which should be incorporated in a nutritionally balanced diet.

International Tree Nut Council (INC) - 23 - June 15, 2002
Among our specific recommendations:
1. The report indicates that a probable level of evidence exists demonstrating a decreasedrisk of CVD from nuts. Additional compelling results of almond and walnut meta-analyses are in publication. Given the growing body of research which demonstrates thecontribution of nuts in the dietary management of other chronic diseases:
• Specify nuts under the fresh fruits/vegetable category to increase awareness of theircontribution as a nutrient- and energy-dense plant food.
• Include the recommendation of incorporating 30g of nuts, seeds and pulses within the400g fruits and vegetable category (as previously recommended in the 1990 report ofthe WHO study group).
2. Continue to encourage joint research which further explores the contribution diverse foodssuch as tree nuts can make to traditional diets (e.g. Mediterranean, vegetarian, etc.) whichare more focused on plant-based foods.
3. Encourage partnerships with NGOs and the food industry in moving forward a globalnutrition and dietary education agenda which encourages balanced food choices and fooddiversity.
4. Since food knowledge and nutrition is an evolving science, provide a structure toincorporate the growing body of research pointing to the role nutrient- and energy-densefoods such as tree nuts can provide in managing chronic diseases.
5. Promote dietary management policies from the context of an overall approach,recognizing that access to safe water and medical services are also paramount contributorsto food safety.
6. Given the fact that a number of plant-based crops are subject to naturally-occurringcontaminants/mycotoxins which vary depending upon production capabilities:
• Encourage establishment of international food safety standards based on science-basedrisk assessments rather than advances in analytical techniques.
• Ensure that valuable foods are not excluded from the overall diet solely due toimproved analytical detection methods rather than true health risks.

International Tree Nut Council (INC) - 24 - June 15, 2002
6. References
Abbey, M., M. Noakes, G.B. Belling, P.J. Nestel, 1994. Partial replacement of saturated fatty acids withalmonds or walnuts lowers total plasma cholesterol and low-density-lipoprotein cholesterol. Am J Clin Nutr.59: 995-9.
Almario, R.U., V. Vonghavaravat, R. Wong, S. Kasin-Karakas, 2001. Effects of walnut consumption on plasmafatty acids and lipoproteins in combined hyperlipidemia. Am J Clin Nutr. 74: 72-9.
Alphan, E., M. Pala, F. Ackurt, T. Yilmaz, 1997. Nutritional composition of hazelnuts and its effects on glucoseand lipid metabolism. In: Kosal AI, Oky Y, Gunes NT, eds. Proceedings of the fourth InternationalSymposium on Hazelnut, Acta Hort 445. 305-10.
American Diabetes Association (ADA). Nutrition recommendations and principles for people with diabetesmellitus (Position Statement). Diabetes Care 2000: 23 (Suppl. 1): S43–6.
American Institute for Cancer Research, 1997. World Cancer Research Fund. Food, nutrition and the preventionof cancer: a global perspective. Nuts and Seeds. 450-1.
Berry, E.M., S. Eisenberg, Y. Friedlander, D. Haratz, N.A. Kaufmann, Y. Norman, Y. Stein, 1992. Effects ofdiets rich in monounsaturated fatty acids on plasma lipoproteins – the Jerusalem Nutrition Study. IIMonounsaturated fatty acids vs. carbohydrates. Am J Clin Nutr. 56: 394-403.
Berry, E.M., S. Eisenberg, D. Haratz, Y. Friedlander, Y. Norman, N.A. Kaufmann, Y. Stein, 1991. Effects ofdiets rich in monounsaturated fatty acids on plasma lipoproteins – the Jerusalem Nutrition Study: highMUFAs vs. high PUFAs. Am J Clin Nutr. 53: 899-907.
Borchers, A., 2001. Review of the Scientific Literature on Phenolic Compounds and Phytosterols in Tree Nuts.(unpublished 28 page report for INC with 279 references).
Brand, J.C., S. Colagiuri, S. Crossman, A. Allen, D.C. Roberts, A.S. Truswell, 1991. Low-glycemic index foodsimprove long-term glycemic control in NIDDM. Diabetes Care. 14: 95-101.
Brand Miller, J., 1994. The importance of glycemic index in diabetes. Am J Clin Nutr. 59 (suppl): 747S-52S.
Bruce, B., G.A. Spiller, L.M. Klevay, S.K. Gallagher, 2000. A diet high in whole and unrefined foods favorablyalters lipids, antioxidant defenses, and colon function. J Am Coll Nutr. 19(1): 61-7.
Bruce, B., G.A. Spiller, J.W. Farquhar, 1997. Effects of a plant-based diet rich in whole grains, sun-dried raisinsand nuts on serum lipoproteins. Veg Nutr. 1/2: 58-63.
Chandalia, M., A. Garg, D. Lutjohann, K. von Bergmann, S.M. Grundy, L.J. Brinkley, 2000. Beneficial effectsof high dietary fiber intake in patients with type-2 diabetes mellitus. N Engl J Med. 342:1392-8.
Chisolm, A., J. Mann, M. Skeaff, C. Franpton, W. Sutherland, A. Duncan, and S. Tiszavari, 1998. A diet rich inwalnuts favorably influences plasma fatty acid profile in moderately hyperlipidemic subjects. Eur J ClinNutr. 52: 12-6.
Colquhoun, D.M., 2000. Food for prevention of coronary heart disease: Beyond the low fat, low cholesteroldiet. Asia Pacific J Clin Nutr. 9(Suppl): S86-90.
Colquhoun, D.M., et al., 1996. Effects of a macadamia nut enriched diet on serum lipids and lipoproteinscompared to a low fat diet. Food Australia. 48(5): 216-22.
Cooke, J.P., P. Tsao, A. Singer, B.Y. Wang, J. Kosck, H. Drexler, 1993. Anti-atherogenic effect of nuts: is theanswer NO? Arch Intern Med 153: 896, 899, 902.

International Tree Nut Council (INC) - 25 - June 15, 2002
Corpet, D.E., B. Peiffer, S. Tache, 1998. Glycemic index, nutrient density, and promotion of aberrant crypt fociin rat colon. Nutr Cancer. 32: 29-36.
Curb, J.D., G. Wergowske, J.C. Dobbs, R.D. Abbott, B. Huang, 2000. Serum lipid effects of a high-monounsaturated fat diet based on macadamia nuts. Arch Intern Med. 160(8): 1154-8.
de Longeril, M., P. Salen, F. Laporte, F. Boucher and J. De Leiri, 2001. Potential use of nuts for the preventionand treatment of coronary heart disease: From natural to functional foods. Nutr Metab Cardiovasc Dis.11:362-71.
DIfE (Deutsches Institut für Ernährungsforschung) Potsdam-Rehbrücke. GEK "Gesundheit Ernährung Krebs",Deutsche Teilstudie der Europäischen Studie zu Ernährung und Krebs (EPIC). Fragebogen zuErnährungsgewohnheiten (Questionnaire edition 1995).
Döring, A, K. Honig-Blum, G. Winkler, R. Kammerlohr, B. Fischer, U. Keil, 1998. MONICA Project RegionAugsburg. Data Book Dietary surveys 1984/85 and 1994/95 in middle-aged men from the city of Augsburg.Neuherberg: GSF-Forschungszentrum.
Durak, I., I. Koksal, M. Kacmaz, S. Buyukkocak, B.M. Cimen, H.S. Ozturk, 1999. Hazelnut supplementationenhances plasma antioxidant potential and lowers plasma cholesterol levels. [Letter to the Editor]. Clin ChimActa. 284(1): 113-5.
Durlach, J., Y. Rayssiquier, 1993. Fatty acid profile, fiber content and high magnesium density may protectagainst risk of coronary heart disease events. Magnes. Res. 6: 191-2.
Edwards, K., I. Kwaw, J. Matud, I. Kurtz, 1999. Effect of pistachio nuts on serum lipid levels in patients withmoderate hypercholesterolemia. J Am Coll Nutr. 18(3): 229-32.
Ellsworth, J.L., L.H. Kushi and A.R. Folsom, 2001. Frequent nut intake and risk of death from coronary heartdisease and all causes in postmenopausal women: The Iowa Women’s Health Study. Nutr Metab CardiovascDis. 11:372-7.
Erario, M, J. N. Cooper, M. J. Sheridan, 2001. Effect of daily pistachio nut consumption on serum lipid levels.FASEB J 15(4): 327 4A. Feldman, E.B., 2002. LSRO Report: The scientific evidence for a beneficial healthrelationship between walnuts and coronary heart disease. J. Nutr. 132: 1062S-101S.
Fraser, G.E., 1999. Nut consumption, lipids and risk of a coronary event. Clin Cardiol. 22 (Suppl. III): 11-5.
Fraser, G.E., J. Sabaté, W.L. Beeson, T.M. Strahan, 1992. A possible protective effect of nut consumption onrisk of coronary heart disease. Arch. Intern. Med. 152: 1416-24.
Fraser, G.E., H.W. Bennett, K.B. Jaceldo, J. Sabaté, 2002. Effect of body weight on a free 70 kilojoules (320calorie) daily supplement of almonds for 6 months. J Am Coll Nutr. 21 (3): 275-83.
Frison-Norrie, S.L., P. Sporns, 2002. Identification and quantification of flavonol glycosides in almondseedcoats using MALDI-TOF MS. J. Agri. Food Chem. 50: 2782-7.
Fulgoni, V.L., M. Abbey, P. Davis, D. Hyson, D. Jenkins, J. Lovejoy, M. Most, J. Sabate, G. Spiller, 2002.Almonds Lower Blood Cholesterol and LDL-Cholesterol But Not HDL-Cholesterol or Triglycerides inHuman Subjects: Results of a Meta-Analysis. FASEB J: 16(5): A961.
Garg A., 1998. High monounsaturated fat diets for patients with diabetes mellitus: a meta-analysis. Am J ClinNutr. 67(suppl):577s-82s..
Ginter, E., 1998. Cardiovascular disease prevention in Eastern Europe. Nutrition. 14(5): 452-7.
Gregory, J., K. Foster, H. Tyler, M. Wiseman, 1990. The dietary and nutritional survey of British adults.London: HMSO.

International Tree Nut Council (INC) - 26 - June 15, 2002
Hebert, J.R., T.G. Hurley, B.C. Olendzki, J. Teas, Y. Ma, J.S. Ha, 1998. Nutritional and socioeconomic factorsin relation to prostate cancer mortality: a cross-national study. J Natl Cancer Inst. 90:1637-47.
Hollman P.C.H., I.C. Arts, 2000. Flavonols, flavones and flavanols- nature, occurence and dietary burden. J. Sci.Food Agric. 80: 1081-93.
Hu, F.B., M.J. Stampfer, 1999. Nut consumption and risk of coronary heart disease: a review of epidemiologicevidence. Current Atherosclerosis Reports. (1): 205-10.
Hu, F.B., M.J. Stampfer, J.E. Manson, E.B. Rimm, G.A. Colditz, B.A. Rosner, F.E. Speizer, C.H. Hennekens,W.C. Willett, 1998. Frequent nut consumption and risk of coronary heart disease in women: prospectivecohort study. British Med J. 317: 1341-5.
Hyson, D., B.O. Schneeman, P.A. Davis, 2002. Almonds and almond oil have similar effects on plasmalipids and LDL oxidation in healthy men and women. J. Nutr. 132(4) 703-7.
Iwamoto, M., K. Imaizumi, M. Sato, Y. Hirooka, K. Sakai, A. Takeshita, M. Kono, 2002. Serum lipid profiles inJapanese women and men during consumption of walnuts. Eur J Clin Nutr. 56(7). (In Press)
Järvi, A.E., B.E. Karlstrom, Y.E. Granfeldt, I.E. Bjorck, N.G. Asp, B.O. Vessby, 1999. Improved glycemiccontrol and lipid profile and normalized fibrinolytic activity on a low-glycemic index diet in type 2 diabeticpatients. Diabetes Care. 22(1): 10-8.
Jenkins, D.J.A., D.G. Popovich, C.W.C. Kendall, E. Vidgen, N. Tariq, T.P.P. Ransom, T.M.S. Wolever, V.Vuksan, C.C. Mehling, D.L. Boctor, C. Bolognesi, J. Huang, and R. Patten, 1997. Effect of a diet high invegetables, fruit, and nuts on serum lipids. Metabolism. 46(5): 530-7.
Jenkins, D.J., T.M. Wolever, B. Buckley, et al., 1988. Low-glycemic-index starchy foods in the diabetic diet.Am J Clin Nutr. 48:248-54.
Jenkins, D.J.A., T.M.S. Wolever, R.H. Taylor, 1981. Glycemic index of foods: a physiological basis forcarbohydrate exchange. Am J Clin Nutr. 34: 362-6.
Kafatos, A.G., 1999. Diet, antioxidants, and health - Case study: the Cretan experience. In: Mediterranean Diets(World Review of Nutrition and Dietetics. Vol. 87). A.P. Simopoulos (ed.) CRC Press LLC. 119-29.
Kaneto, H., Y. Kajimoto, J. Miyagawa, T. Matsuoka, Y. Fujitani, Y. Umayahara, T. Hanafusa, Y. Matsuzawa, Y.Yamasaki, M. Hori, 1999. Beneficial effects of antioxidants in diabetes: possible protection of pancreaticbeta-cells against glucose toxicity. Diabetes. 48(12): 2398-406.
Kendall, C.W.C., D.J.A. Jenkins, A. Marchie, T. Parker, P. Connelly, 2002a. Dose response of almondson coronary heart disease risk factors -- blood lipids, oxidized LDL, Lp(a), homocysteine andpulmonary nitric oxide: a randomized controlled cross-over trial. Circulation. (In Press)
Kendall, C., D. Jenkins, A. Marchie, T. Parker, P. Conelly, 2002b. Dose response of almonds in hyperlipidemia:a randomized controlled cross-over trial. Am J Clin Nutr. 75 (2S): 384.
Key, T., G. Fraser, M. Thorogood, 1998. Mortality in vegetarians and non-vegetarians: a collaborative analysisof 8300 deaths among 76,000 men and women in five prospective studies. Pub Health Nutr. 1(1): 33-41.
Klevay, L.M., 1993. Copper in nuts may lower heart disease risk. Arch Intern Med. 153: 401-2.
Kouris-Blazos, A., C. Gnardellis, M.L. Wahlqvist, D. Trichopoulos, W. Lukito, A. Trichopoulous, 1999. Arethe advantages of the Mediterranean diet transferable to other populations? A cohort study in Melbourne,Australia. Br J Nutr. 82: 57-61.
Krauss R.M., R.H. Eckel, B. Howard, L.J. Appel, S.R. Daniels, R.J. Deckelbaum, J.W. Erdman, Jr, P. Kris-therton, I.J.Goldberg, T.A. Kotchen, A.H. Lichtenstein, W.E. Mitch, R. Mullis, K. Robinson, J. Wylie-Rosett,S. St Jeor, J. Suttie, D.L. Tribble, T.L. Bazzarre, 2000. AHA Dietary Guidelines: Revision 2000: A Statement

International Tree Nut Council (INC) - 27 - June 15, 2002
for Healthcare Professionals from the Nutrition Committee of the American Heart Association. Circulation102:2284-99.
Krauss, R.M., R.H. Eckel, B. Howard, L.J., et al., 2001. Revision 2000: a statement for healthcare professionalsfrom the Nutrition Committee of the American Heart Association. J Nutr. 131(1): 132-46.
Krawczyk, T., 2001. Fat in dietary guidelines around the world. Inform. 12: 126-40.
Kris-Etherton, P.M., S. Yu-Poth, J. Sabate, H.E. Ratcliffe, G. Zhao, T.D. Etherton, 1999. Nuts and theirbioactive constituents: effects on serum lipids and other factors that affect disease risk. Am. J. Clin. Nutr. 70(Suppl.): 504S-11S.
Langseth, L., 1995. Oxidants, antioxidants, and disease prevention. ILSI Europe Concise Monograph Series,Brussels, Belgium: ILSI Europe.
Lavedrine, F., D. Zmirou, A. Ravel, F. Balducci, J. Alary, 1999. Blood cholesterol and walnut consumption: across-sectional survey in France. Prev Med 28(4): 333-9.
Lin, B.H., E. Frazao, J. Allhouse, 2001. U.S. consumption patterns of tree nuts. Food Review 24 (2): 54-8.
Lino, M., K. Marcoe, J.M. Dinkins, H. Hiza, R. Anand, 2000. USDA Center for Nutrition Policy andPromotion. The role of nuts in a healthy diet. Insight 23, December.
Liu, S., W. Willett, M. Stampfer, et al., 2000. A prospective study of dietary glycemic load, carbohydrate intakeand risk of coronary heart disease in US women. Am J Clin Nutr. 71: 1455-61.
Luscombe, N., M. Noakes, P. Clifton, 1999. Diets high and low in glycemic index versus high monounsaturatedfat diets: effects on glucose and lipid metabolism in NIDDM. Eur J Clin Nutr. 53: 473-8.
Mann, J., 2000. Optimizing the plant-based diet. Asia Pacific J. Clin. Nutr. 9 (Suppl.) S60-4.
McManus, K., L. Antinoro, F. Sacks, 2001. A randomized controlled trial of a moderate fat, low energy dietcompared with a low fat, low energy diet for weight loss in overweight adults. Int J Obesity. 25: 1503-11.
Mensink, G., R. Beitz, M. Burger, S. Bisson, 2000. Lebensmittelkonsum in Deutschland. Ernährungs-Umschau47(9): 328-32.
Milbury, P., C.Y. Chen, C. Kim, J. Blumberg, 2002. Polyphenolics (PP) from almond skins with a-tocopherol(aT) synergistically increase the resistance of LDL to Oxidation. FASEB J. 16(5): A1106.
Morgan, W.A., B.J. Clayshulte. 2000. Pecans lower low-density lipoprotein cholesterol in people with normallipid levels. J Am Diet Assoc. 100(3): 312-8.
Munoz, S., M. Merlos, D. Zambon, C. Rodriguez, J. Sabate, E. Ros, J.C. Laguna, 2001. Walnut-enriched dietincreases the association of LDL from hypercholesterolemic men with human HepG2 cells. J Lipid Res.42(12): 2069-76.
Nanos, G.D., D.G. Gerasopoulos, 2001. Fruits, vegetables, legumes and grains. In: The Mediterranean diet:Constituents and health promotion. A.L. Matalas, A. Zampelas, V. Stavrinos, I. Wolinsky (eds) CRC Press,London. 97-125.
N.A.S., 2000. Dietary reference intakes for vitamin C, vitamin E, selenium, and carotenoids. Food andNutrition Board, Inst. of Med., National Academy Press, Washington, D.C.
N.I.H. Expert Panel on Detection, Evaluation and Treatment of High Cholesterol in Adults, 2001. Executivesummary of the third report of the National Cholesterol Education Program expert panel on detection,evaluation & treatment of high blood cholesterol in adults (adult treatment panel III). J Am Med Assn 285:2486-97.
Noah, A., A.S. Truswell, 2001. There are many Mediterranean diets. Asia Pacific J. Clin. Nutr. 10 (1): 2-9.

International Tree Nut Council (INC) - 28 - June 15, 2002
Oldways Preservation & Exchange Trust, Characteristics of the Mediterranean Diet http://www.oldwayspt.org.
Oldways, 1995. Tree nuts, health and the Mediterranean diet. A summary report. Boston, USA. 51 pages.
Panico, S., I.R. Dello, E. Celentano, R. Galasso, P. Muti, M. Salvatore, M.P. Mancini, 1992. ATENA, a studyon the etiology of major chronic diseases in women: design, rationale and objectives. Eur J Epidemiol. 8:601-8.
Paolisso, G., A. D'Amore, D. Giugliano, A. Ceriello, M. Varricchio, F. D'Onofrio, 1993. Pharmacologic dosesof vitamin E improve insulin action in healthy subjects and non-insulin-dependent diabetic patients. Am JClin Nutr. 57(5): 650-6.
Rajaram, S., K. Burke, B. Connell, T. Myint, J. Sabate, 2001. A monounsaturated fatty acid-rich pecan-enricheddiet favorably alters the serum lipid profile of healthy men and women. J Nutr. 131(9): 2275-9.
Rajaram, S., M. Wien, 2001. Vegetarian diets in the prevention of osteoporosis, diabetes, and neurologicaldisorders. In: Sabaté, J., (ed.) Vegetarian Nutrition, CRC Press, Boca Raton, 109-34.
Sabaté, J., G. Blix, 2001. Vegetarian diets and obesity prevention: In: Sabaté, J., (ed.), Vegetarian Nutrition.CRC Press, Boca Raton, 91-107.
Sabaté, J., G.E. Fraser, K. Burke, S.F. Knutsen, H. Bennett, K.D. Lindsted, 1993. Effects of walnuts on serumlipid levels and blood pressure in normal men. N Engl J Med. 328(9): 603-7.
Sabaté, J., E. Haddad, 2001. Almond-rich diets simultaneously improve plasma lipoproteins and alpha-tocopherol levels in men and women. Ann Nutr Metab. 45(1): 596.
Sabaté, J., S. Rajaram, P. Jambazian, J.S. Tanzman, E. Haddad, 2001. Dose response effects of almonds onserum lipid levels in healthy men and women: a randomized feeding trial. FASEB J. 15(5): A601.
Salmeron, J., A. Ascherio, E.B. Rimm, et al., 1997a. Dietary fiber, glycemic load, and risk of NIDDM in men.Diabetes Care. 20: 545-50.
Salmeron, J., J.E. Manson, M.J. Stampfer, G.S.A. Colditz, W.C. Willett, 1997b. Dietary fiber, glycemic load,and risk of NIDDM in women. JAMA. 277: 472-7.
Sang, S., K. Lapsley, W.-S. Jeong, P.A. Lachance, R.T. Rosen, C.-T. Ho, 2002. Antioxidative phenoliccompounds isolated from almond skin (Prunus amygdalus Batsch). J. Agric. Food Chem. 50: 2459-63.
Sarkkinen, E., U. Schwab, L. Niskanen, M. Hannuksela, M. Savolainen, K. Kervinen, A. Kesaniemi, M.I.Uusitupa, 1996. The effects of monounsaturated-fat enriched diet and polyunsaturated-fat enriched diet onlipid and glucose metabolism in subjects with impaired glucose tolerance. Eur J Clin Nutr. 50(9): 592-8.
Serra Majem, L., N. Armas, B.L. Ribas, 2000. Food consumption and food sources of energy and nutrients inCanary Islands (1997-1998) [in Spanish]. Arch Latinoam Nutr. 50(Suppl 1): 23-33.
Serra-Majem L, R. García-Closas, L. Ribas, C. Pérez-Rodrigo, J. Aranceta, 2001. Food patterns of Spanishschoolchildren and adolescents: The enKid Study. Public Health Nutrition. 4(6A): 1433-8.
Singh, R.B., S.S. Rastogi, R.Verma, L. Bolaki, and R. Singh, 1992. An Indian experiment with nutritionalmodulation in acute myocardial infarction. Am J Cardiol. 69: 879-85.
Slimani, N., P. Ferrari, M. Ocke, et al., 2000. Standardization of the 24-hour diet recall calibration method usedin the European prospective investigation into cancer and nutrition (EPIC): general concepts and preliminaryresults. Eur J Clin Nutr. 54(12): 900-17.
Spiller, G., 1992. Effect of a diet high in monounsaturated fat from almonds on plasma cholesterol andlipoproteins. J Am Coll Nutr. 11 (2): 126-30.

International Tree Nut Council (INC) - 29 - June 15, 2002
Spiller, G.A., D.A.J. Jenkins, O. Bosello, J.E. Gates, L.N. Cragen, B. Bruce, 1998. Nuts and plasma lipids: analmond-based diet lowers LDL-C while preserving HDL-C. J Am Coll Nutr. 17(3): 285-90.
Svetkey L.P., F.M. Sacks, E. Obarzanek, W.M. Vollmer, L.J. Appel, P.H. Lin, N.M. Karanja, D.W. Harsha, G.A.Bray, M. Aickin, M.A. Proschan, M.M. Windhauser, J.F. Swain, P.B. McCarron, D.G. Rhodes, R.L. Laws,1999. The DASH diet, sodium intake and blood pressure trial (DASH-sodium): rationale and design. DASH-Sodium Collaborative Research Group. J Am Diet Assoc (8 Suppl):S96-104.
Thiebaut, A.C., F. Clavel-Chapelon, 2001. Fat consumption and breast cancer: preliminary results from theE3N-Epic cohort [in French]. Bull Cancer. 88(10): 954-8.
Trichopoulou, A., E. Vasilopoulou, 2000. Mediterranean diet and longevity. Br J Nutr. 84(Suppl2): S205-9.
Trichopoulou, A., P. Lagiou, 1997. Healthy traditional Mediterranean diet: an expression of culture, history, andlifestyle. Nutrition Reviews 55(11): 383-9.
USDA Dietary Guidelines for Americans 2000, 5th Edition, Center for Nutrition Policy and Promotion.
USDA, 2001. Agricultural Research Service. USDA Nutrient Database for Standard References, Release No. 14.Nutrient Data Laboratory Home Page http://www.nal.usda.gov/fnic/foodcomp.
Verschuren, W.M.M., E.M. van Leer, A. Blockstra, J.C. Seidell, H.A. Smit, H.B. Bueno de Mesquita, G.L.Oberman-de Boer, D. Kromhout, 1993. Cardiovascular disease risk factors in The Netherlands. Neth JCardiol. 4: 205-10.
Wolever, T.M.S., D.J.A. Jenkins, A.L. Jenkins, R.G. Josse, 1991. The glycemic index: methodology and clinicalimplications. Am J Clin Nutr. 54: 846-54.
Zambón, D., J. Sabaté, S. Munoz, B. Campero, E. Casals, M. Merlos, J.C. Laguna, E. Ros, 2000. Substitutingwalnuts for monounsaturated fat improves the serum lipid profile of hypercholesterolemic men and women.A randomized crossover trial. Ann Intern Med. 4:132(7): 538-46.

International Tree Nut Council (INC) - 30 - June 15, 2002
7. Contributors/Reviewers
Julie G. Adams, Almond Board of California, Modesto, California, USA
Sigrid Beer-Borst, M.Sc., Projects in Nutritional Sciences, Koeniz, Switzerland
Dr. Andrea Borchers, Consultant, Berlin, Germany
Dr. Bernard Decarli, Clinical Evaluation, Nestle Research Center, Lausanne, Switzerland
Dr. Johannes F. Diehl, Karlsruhe, Germany
Dr. Peter R. Ellis, King’s College London, Div. of Life Sciences, London, UK
Guy Johnson, Ph.D., Kalamazoo, Michigan, USA
Dr. Khalil I. Ereifej, Dept. of Nutrition and Food Tech., Jordan Univ. of Science and Technology, Jordan
Karen Lapsley, D.Sc. Almond Board of California, Modesto, California, USA
Kathleen McMahon, Ph.D., RD, on behalf of California Pistachio Commission, Chicago, Illinois, USA
Peter Pribis, MD, Ph.D., Deutscher Verein für Gesundheitspflege, Ostfildern, Germany
Maureen Ternus, MS, RD, International Tree Nut Council, Davis, California, USA
Dr. Nicola Uccela, Mediterranean Food Research Centre, Calabria University, Arcavacata, Italy