nathan peiffer-smadja -porteur projet antibioclic-afrique
TRANSCRIPT
Nathan PEIFFER-SMADJA - Porteur projet Antibioclic-Afrique
SMIT CHU Bichat Paris, IAME Inserm, HPRU HCAI and AMR Imperial College London
25/06/2020
COVID-19 : Etat des lieux de la recherche sur les traitements
Plan général
• Recherche thérapeutique durant une pandémie liée à une maladie nouvelle
• Quelques résultats de RCT • Lopinavir/ritonavir +/- IFN ß-1• Hydroxychloroquine• Remdesivir• Corticothérapie
• Conclusion
Stratégie globale face à une maladie nouvelle
• Tester des traitements repositionnés, seuls ou en combinaison, à différents stades de la maladie
• Développer de nouvelles thérapies
• Créer un vaccin
Plan de l’OMS - 2017
Merci à Prof Florence Ader pour la diapositive
Choisir les candidats repositionnés
• Exemples de maladies comparables
• Données in vitro
• Modèles animaux
• Études cliniques initiales, à réaliser de façon très rigoureuse, afin d’avoir des pistes thérapeutiques à évaluer ensuite
• EN PARALLELE si possible de la mise en place d’essais cliniques randomisés qui sont les seuls à même d’apporter des réponses fiables
L’exemple des autres maladies virales aiguës
• SARS 1• Pas de traitement spécifique efficace
• Zika• Pas de traitement spécifique efficace
• Dengue• Pas de traitement spécifique efficace
• Chikungunya• Pas de traitement spécifique efficace
• Grippe sévère• Traitement efficace sur la durée de symptômes = oseltamivir
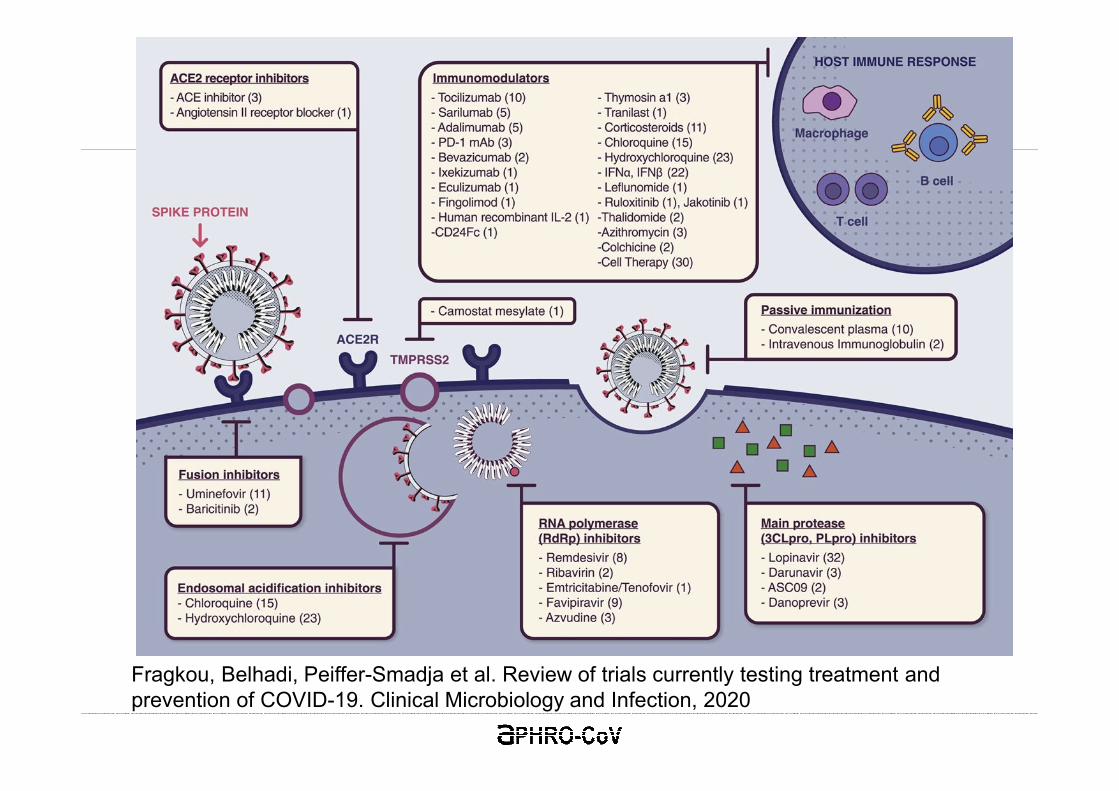
Fragkou, Belhadi, Peiffer-Smadja et al. Review of trials currently testing treatment and prevention of COVID-19. Clinical Microbiology and Infection, 2020
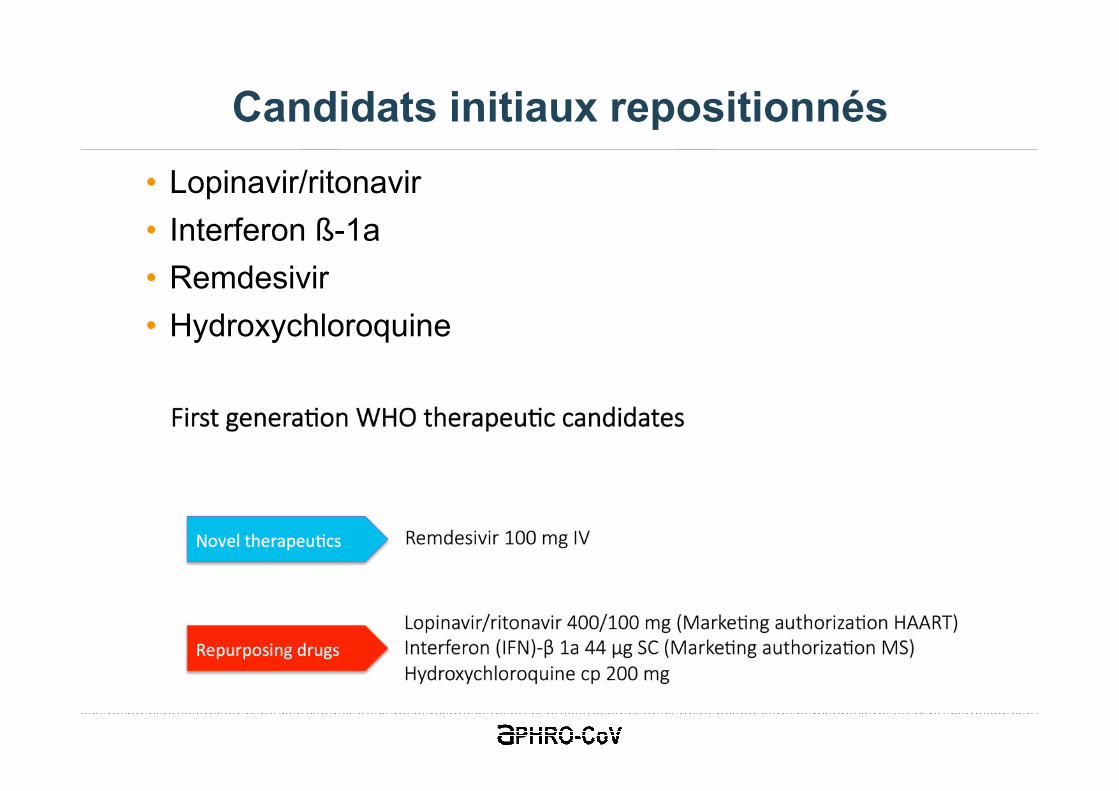
Candidats initiaux repositionnés
• Lopinavir/ritonavir
• Interferon ß-1a
• Remdesivir
• Hydroxychloroquine
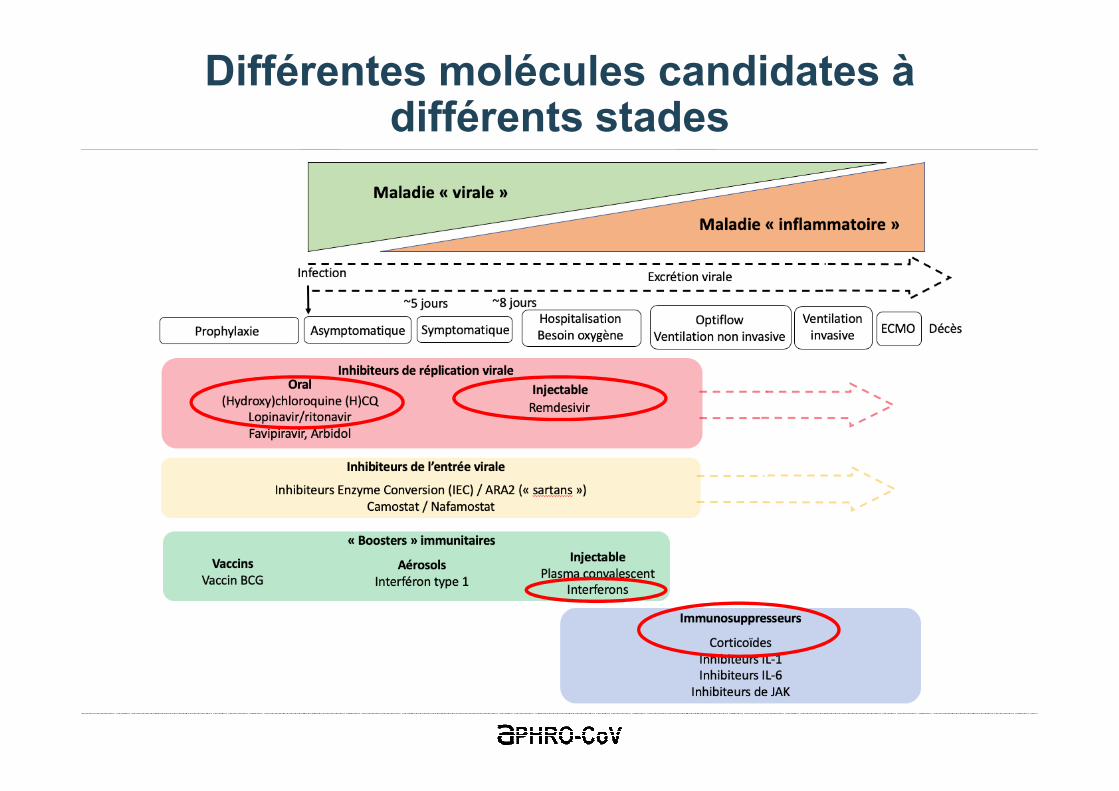
Différentes molécules candidates à différents stades
• Importance de larges collaborations pour les essais cliniques afin de finir le recrutement
• Importance de protocoles adaptatifs
Collaborations
Merci à Prof Florence Ader pour la diapositive
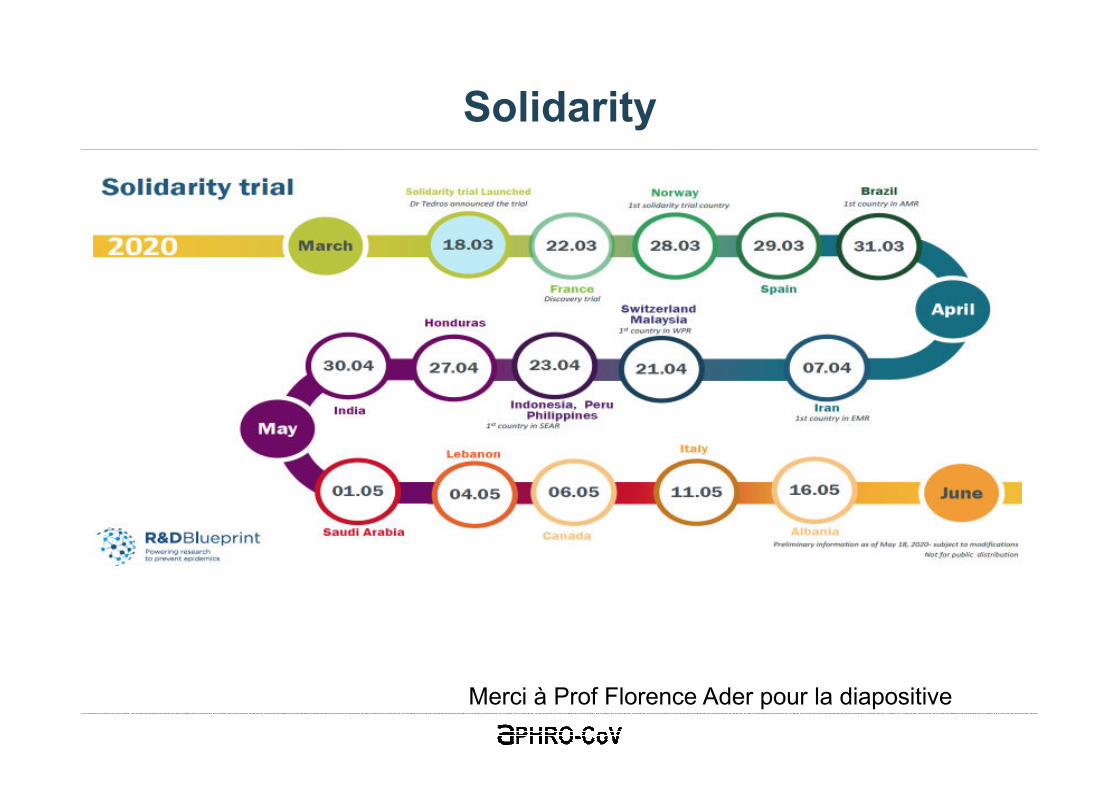
Solidarity
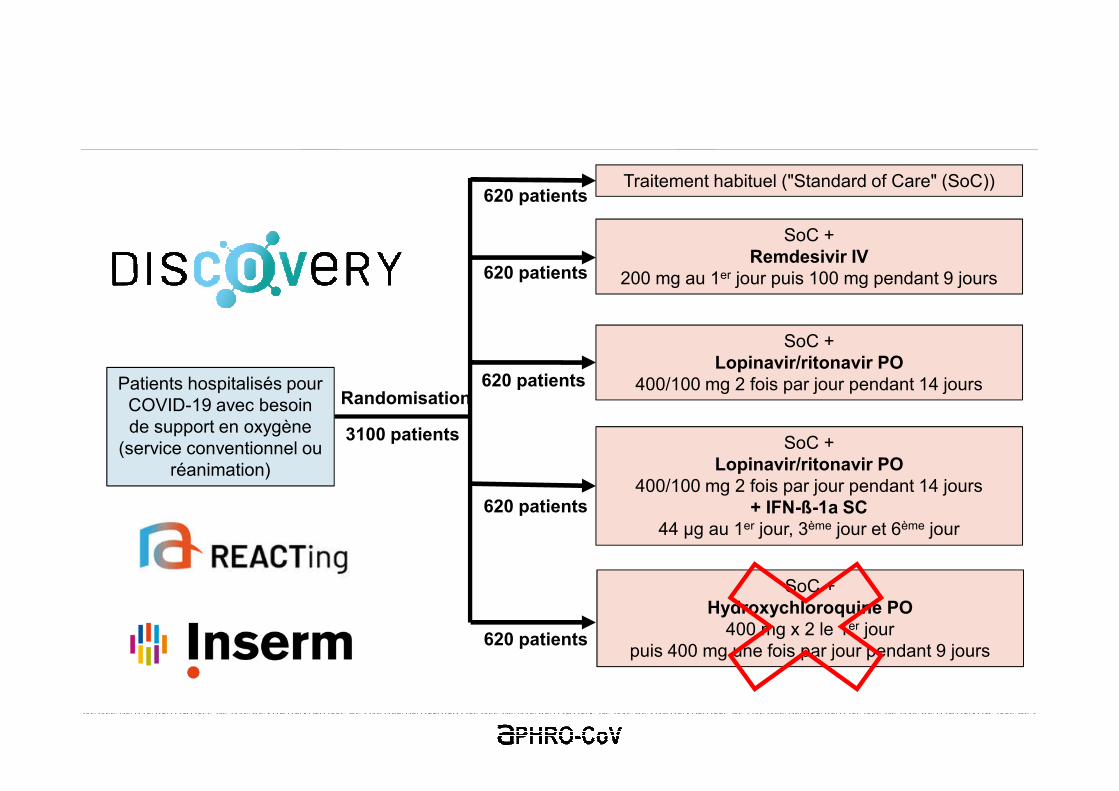
Patients hospitalisés pour COVID-19 avec besoin de support en oxygène
(service conventionnel ou réanimation)
Traitement habituel ("Standard of Care" (SoC))
SoC +Remdesivir IV
200 mg au 1er jour puis 100 mg pendant 9 jours
SoC +Lopinavir/ritonavir PO
400/100 mg 2 fois par jour pendant 14 jours
SoC +Lopinavir/ritonavir PO
400/100 mg 2 fois par jour pendant 14 jours+ IFN-ß-1a SC
44 μg au 1er jour, 3ème jour et 6ème jour
SoC +Hydroxychloroquine PO
400 mg x 2 le 1er jourpuis 400 mg une fois par jour pendant 9 jours
Randomisation
3100 patients
620 patients
620 patients
620 patients
620 patients
620 patients

Niveaux de preuve
Djulbegovic et al. The Lancet. 2017
Lopinavir / ritonavir - Interferon ß-1
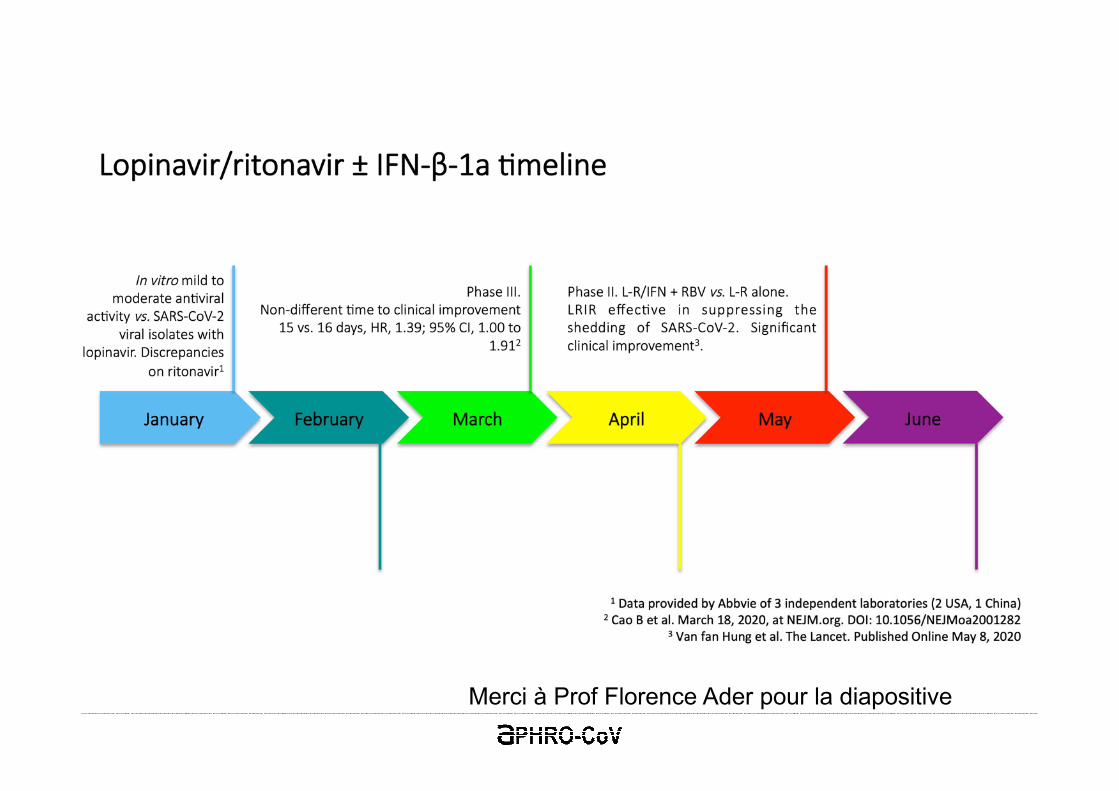
Merci à Prof Florence Ader pour la diapositive
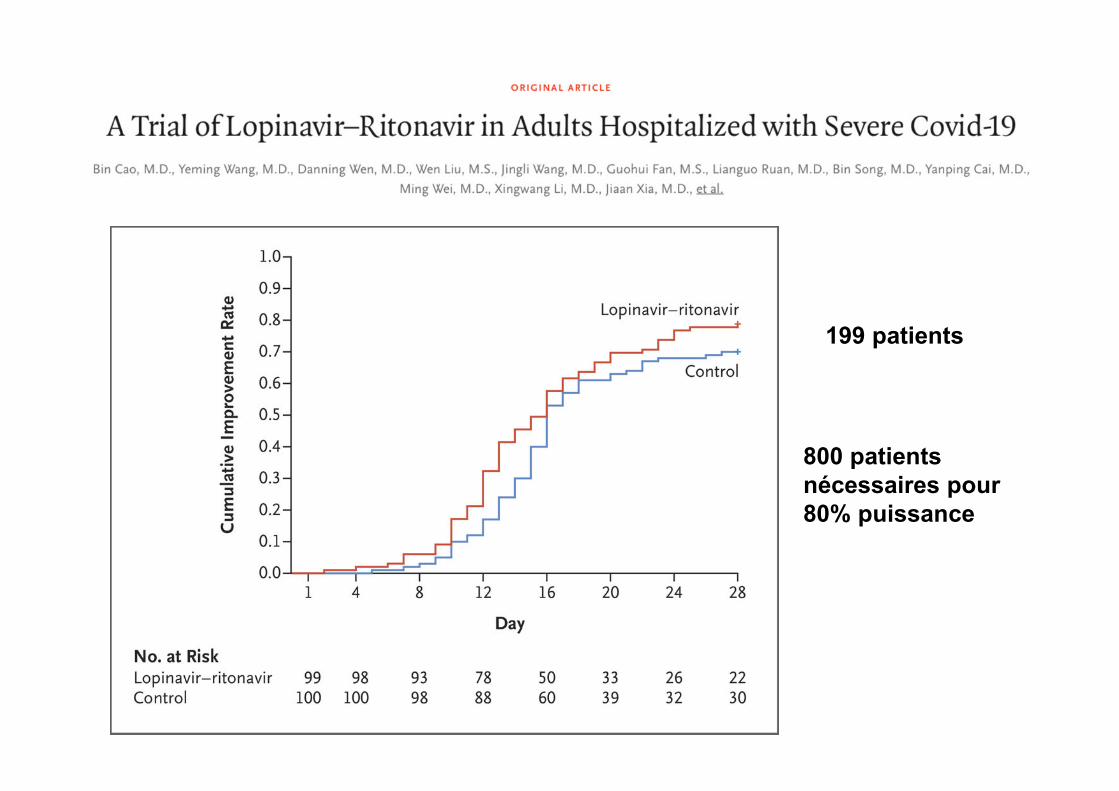
199 patients
800 patients
nécessaires pour
80% puissance
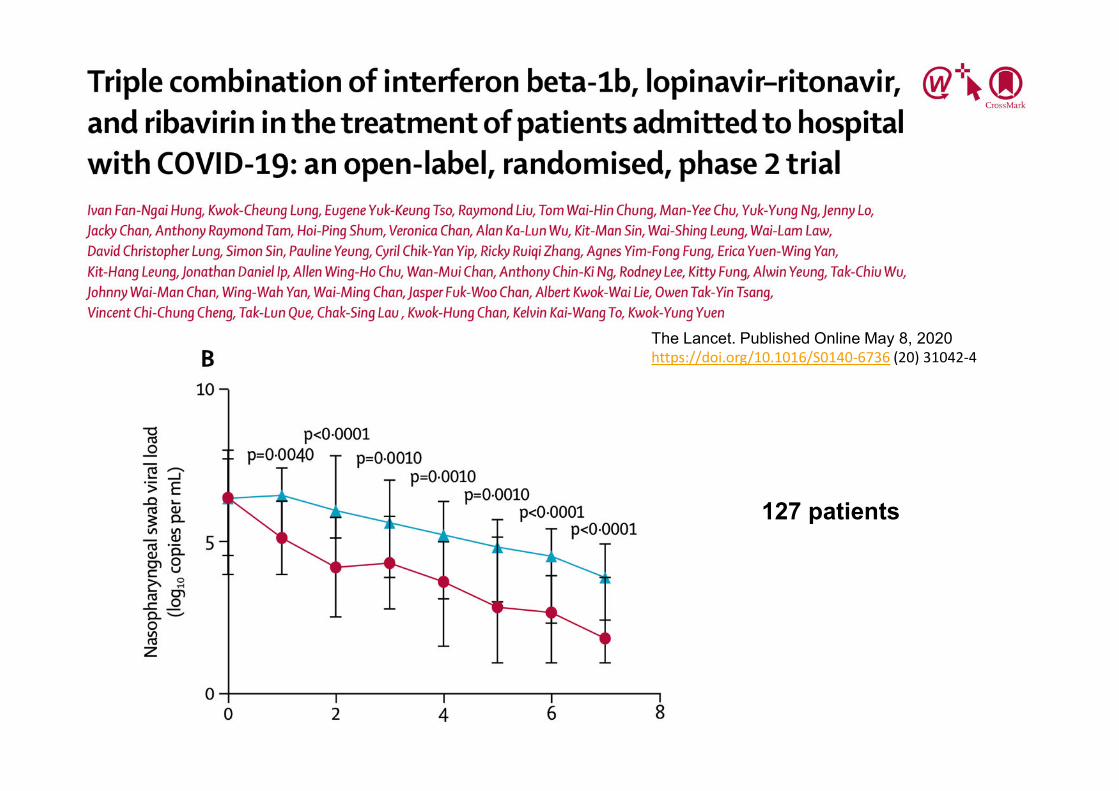
The Lancet. Published Online May 8, 2020https://doi.org/10.1016/S0140-6736 (20) 31042-4
127 patients
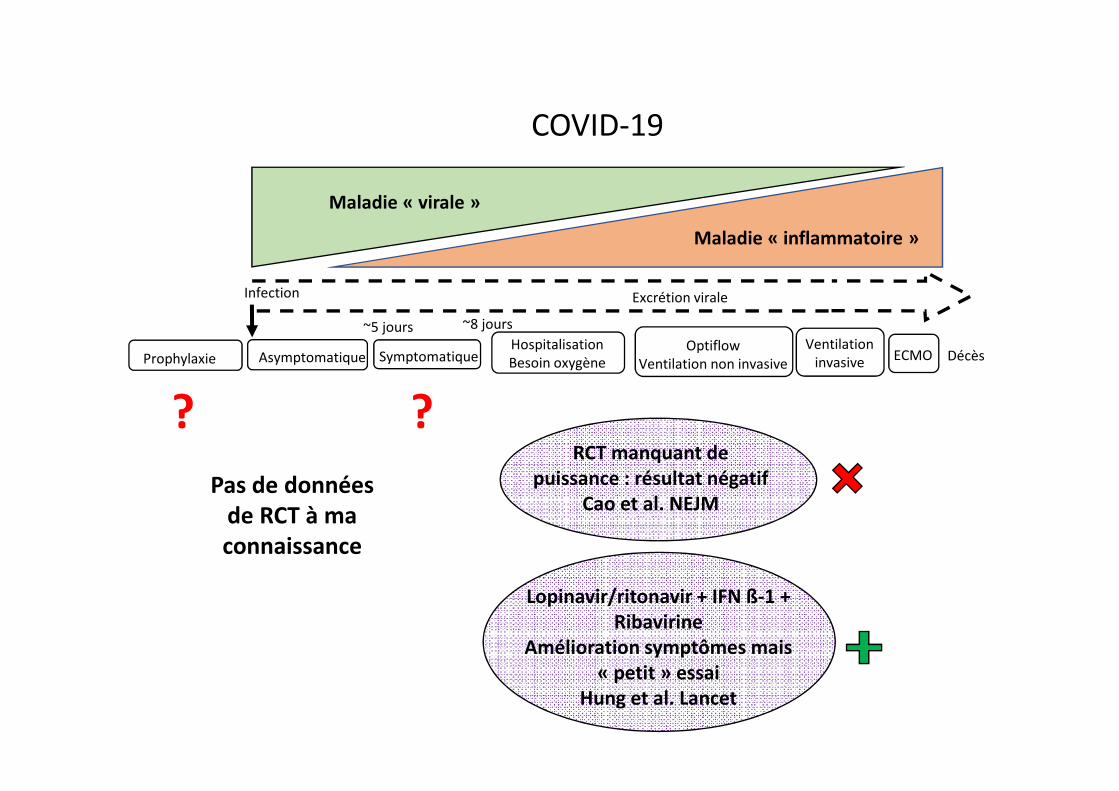
Infection
SymptomatiqueAsymptomatique
Excrétion virale
DécèsHospitalisation
Besoin oxygène
Optiflow
Ventilation non invasive
Ventilation
invasiveECMO
~5 jours ~8 jours
Prophylaxie
Maladie « virale »
Maladie « inflammatoire »
COVID-19
?RCT manquant de
puissance : résultat négatif
Cao et al. NEJM
?
Pas de données
de RCT à ma
connaissance
Lopinavir/ritonavir + IFN ß-1 +
Ribavirine
Amélioration symptômes mais
« petit » essai
Hung et al. Lancet
Hydroxychloroquine
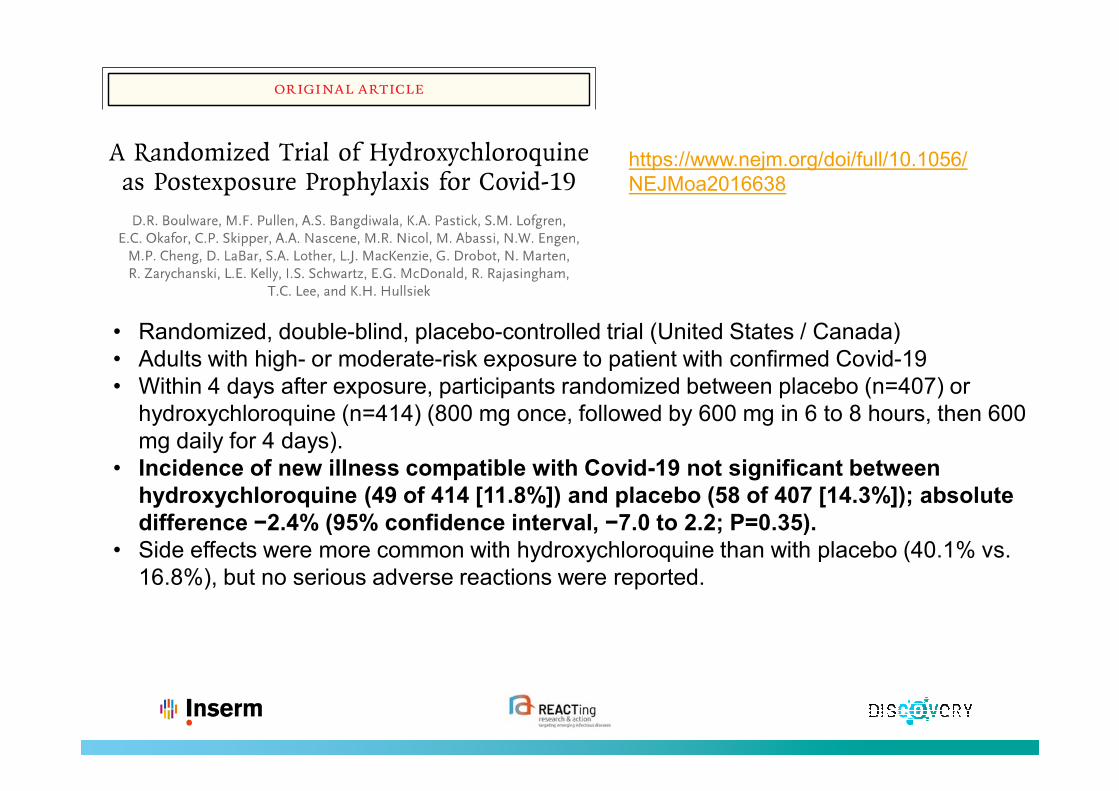
https://www.nejm.org/doi/full/10.1056/NEJMoa2016638
• Randomized, double-blind, placebo-controlled trial (United States / Canada)• Adults with high- or moderate-risk exposure to patient with confirmed Covid-19 • Within 4 days after exposure, participants randomized between placebo (n=407) or
hydroxychloroquine (n=414) (800 mg once, followed by 600 mg in 6 to 8 hours, then 600 mg daily for 4 days).
• Incidence of new illness compatible with Covid-19 not significant between
hydroxychloroquine (49 of 414 [11.8%]) and placebo (58 of 407 [14.3%]); absolute
difference −2.4% (95% confidence interval, −7.0 to 2.2; P=0.35).
• Side effects were more common with hydroxychloroquine than with placebo (40.1% vs. 16.8%), but no serious adverse reactions were reported.
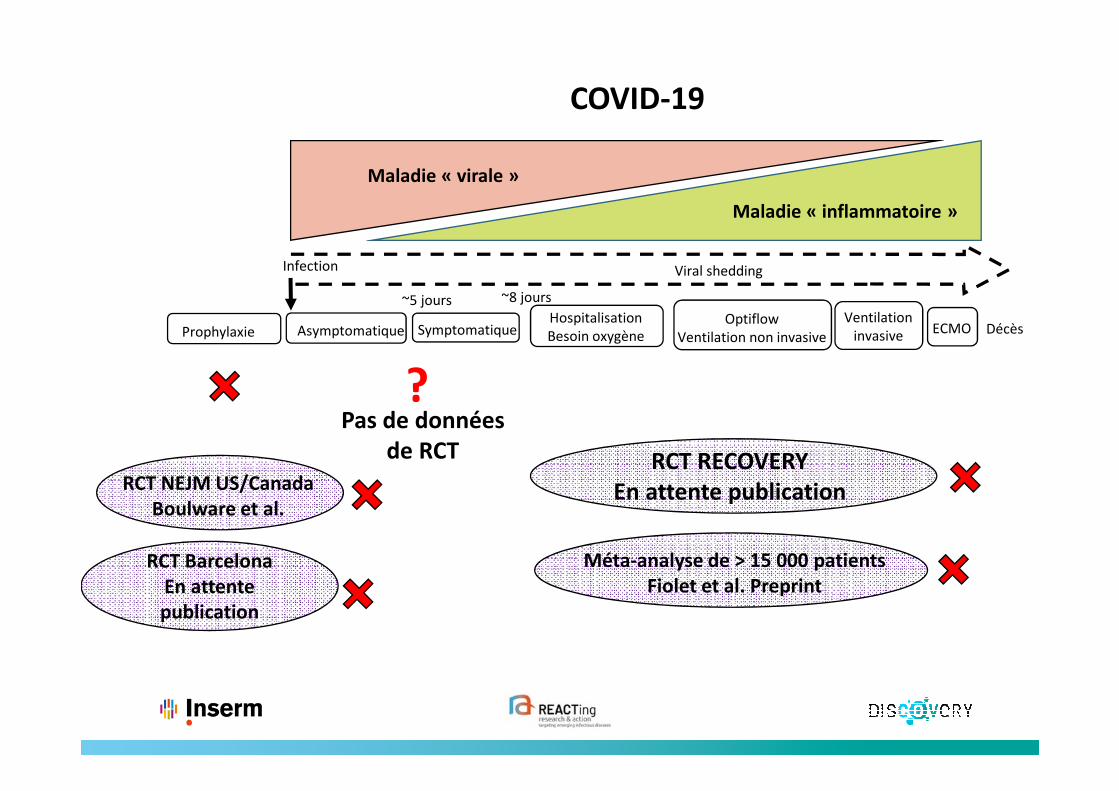
Infection
SymptomatiqueAsymptomatique
Viral shedding
DécèsHospitalisation
Besoin oxygène
Optiflow
Ventilation non invasive
Ventilation
invasiveECMO
~5 jours ~8 jours
Prophylaxie
Maladie « virale »
Maladie « inflammatoire »
RCT Barcelona
En attente
publication
COVID-19
?Pas de données
de RCT
RCT NEJM US/Canada
Boulware et al.
RCT RECOVERY
En attente publication
Méta-analyse de > 15 000 patients
Fiolet et al. Preprint

Remdesivir
Merci à Prof Florence Ader pour la diapositive
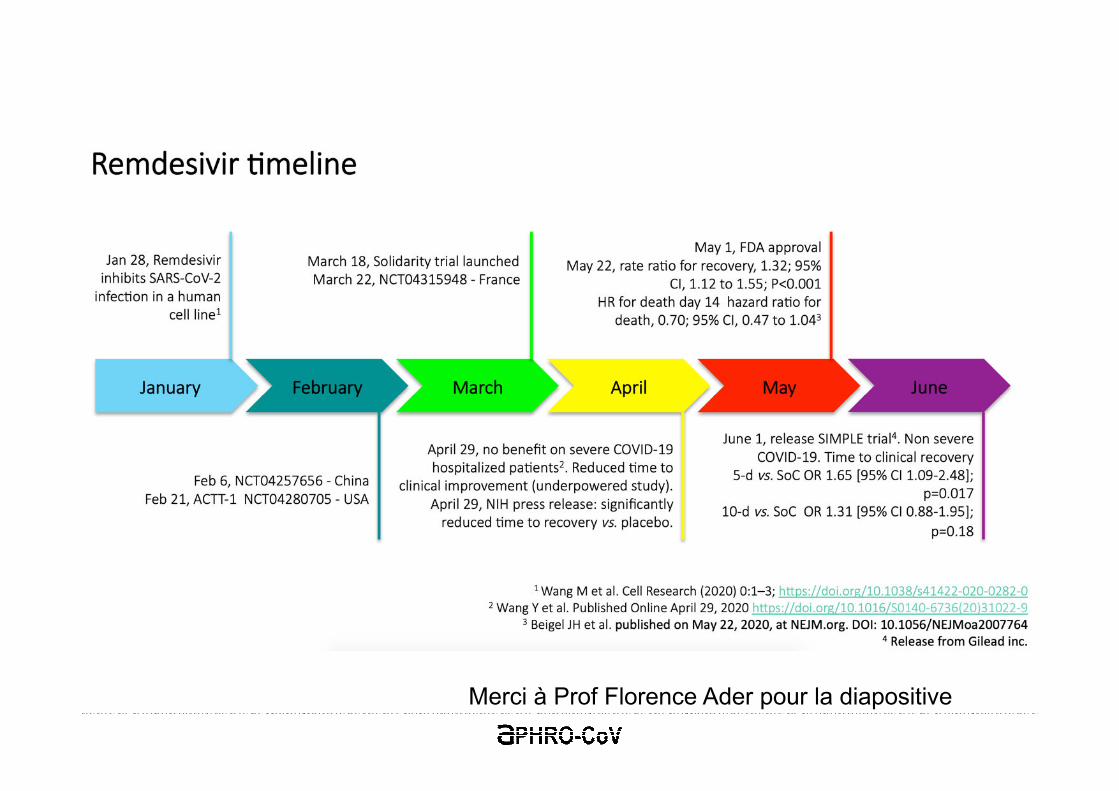
Randomised, double-blind, placebo-controlled, multicentre trial at ten hospitals in Hubei, China.
Eligible patients: adults hospitalized with COVID-19 and oxygen saturation of 94% or less on room air
237 patients enrolled and randomly assigned to a treatment group (158 to remdesivir and 79 to placebo)
Primary endpoint = time to clinical improvement up to day 28, defined as the time (days) fromrandomisation to two levels decline on six-point ordinal scale of clinical status
Early termination because of the lack of new patients, with the actual enrolment of 236 participants, statisticalpower was thus reduced from 80% to 58%
Remdesivir use was not associated with a difference in time to clinical improvement (median remdesivir21·0 days [IQR 13·0–28·0] vs placebo 23·0 days [15·0–28·0]; HR 1·23 [95% CI 0·87–1·75])
Although not statistically significant, patients receiving remdesivir had a numerically faster time to clinicalimprovement than those receiving placebo among patients with symptom duration of 10 days or less: median18·0 days[IQR 12·0–28·0]vs 23·0 days [15·0–28·0]; HR 1·52 [0·95–2·43]
28-day mortality was similar between the two groups (22 [14%] died in the remdesivir group vs 10 (13%) in the placebo group; difference 1·1% [95% CI –8·1 to 10·3])
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31022-9/fulltext
Merci à Prof Florence Ader pour la diapositive
Double-blind, randomized, multicentre placebo-controlled trial mainly in the USA
Adults hospitalized with Covid-19 and evidence of lower respiratory tract involvement
538 patients assigned to remdesivir and 521 to placebo
Primary outcome = the time to recovery, defined by either discharge from the hospital or hospitalization for infection-control purposes only
The data and safety monitoring board recommended early unblinding of the results on the basis of findings from an analysis that showed shortened time to recovery in the remdesivirgroup
Patients who received remdesivir had a median recovery time of 11 days (95% confidence interval [CI], 9 to 12), as compared with 15 days (95% CI, 13 to 19) in those who received placebo (rate ratio for recovery, 1.32; 95% CI, 1.12 to 1.55; P<0.001)
The Kaplan-Meier estimates of mortality by 14 days were 7.1% with remdesivir and 11.9% with placebo (hazard ratio for death, 0.70; 95% CI, 0.47 to 1.04).
https://www.nejm.org/doi/full/10.1056/NEJMoa2007764
ACTT-1
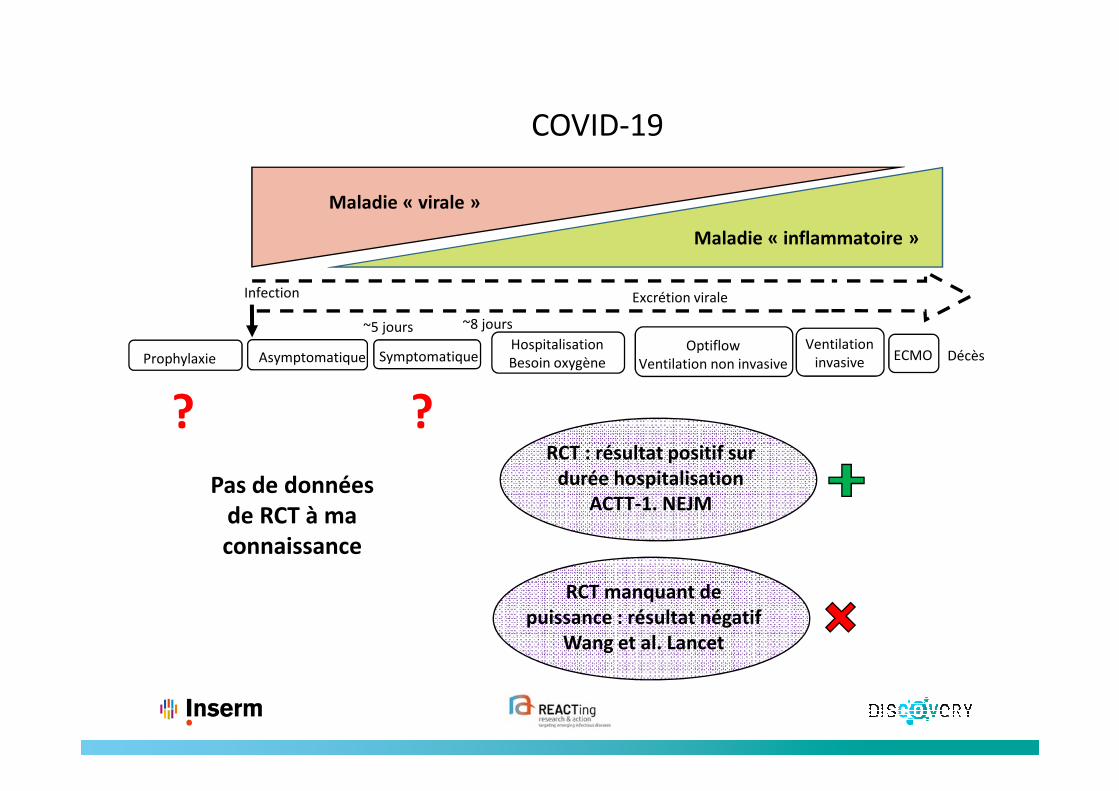
?RCT : résultat positif sur
durée hospitalisation
ACTT-1. NEJM
?
Pas de données
de RCT à ma
connaissance
RCT manquant de
puissance : résultat négatif
Wang et al. Lancet
Infection
SymptomatiqueAsymptomatique
Excrétion virale
DécèsHospitalisation
Besoin oxygène
Optiflow
Ventilation non invasive
Ventilation
invasiveECMO
~5 jours ~8 jours
Prophylaxie
Maladie « virale »
Maladie « inflammatoire »
COVID-19
Corticoïdes
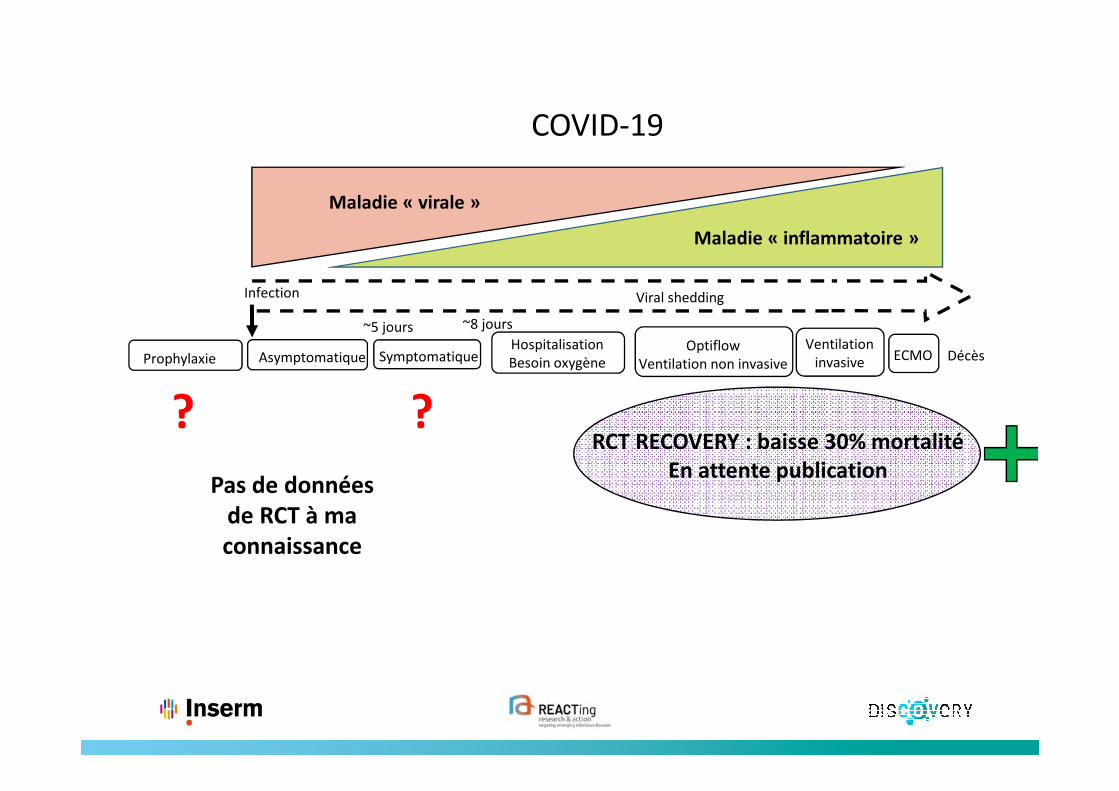
Infection
SymptomatiqueAsymptomatique
Viral shedding
DécèsHospitalisation
Besoin oxygène
Optiflow
Ventilation non invasive
Ventilation
invasiveECMO
~5 jours ~8 jours
Prophylaxie
Maladie « virale »
Maladie « inflammatoire »
COVID-19
? ?
Pas de données
de RCT à ma
connaissance
RCT RECOVERY : baisse 30% mortalité
En attente publication
Messages clés
• Nécessité de choisir des candidats thérapeutiques face à une maladie nouvelle• Précédentes maladies comparables• Données in vitro
• Mettre en place des études rigoureuses et fiables de petite taille en parallèle d’essais cliniques randomisés de bonne qualité
• Privilégier les larges collaborations nationales et internationales
• Attention à la communication des résultats en contexte pandémique