les mutations du promoteur de tert sont des … · immunohistochimie . biologie moléculaire ....
TRANSCRIPT

Dr Jean-Charles Nault Inserm U1162, Dir: Pr Jessica Zucman-Rossi
Service d’hépatologie, Hôpital Jean Verdier
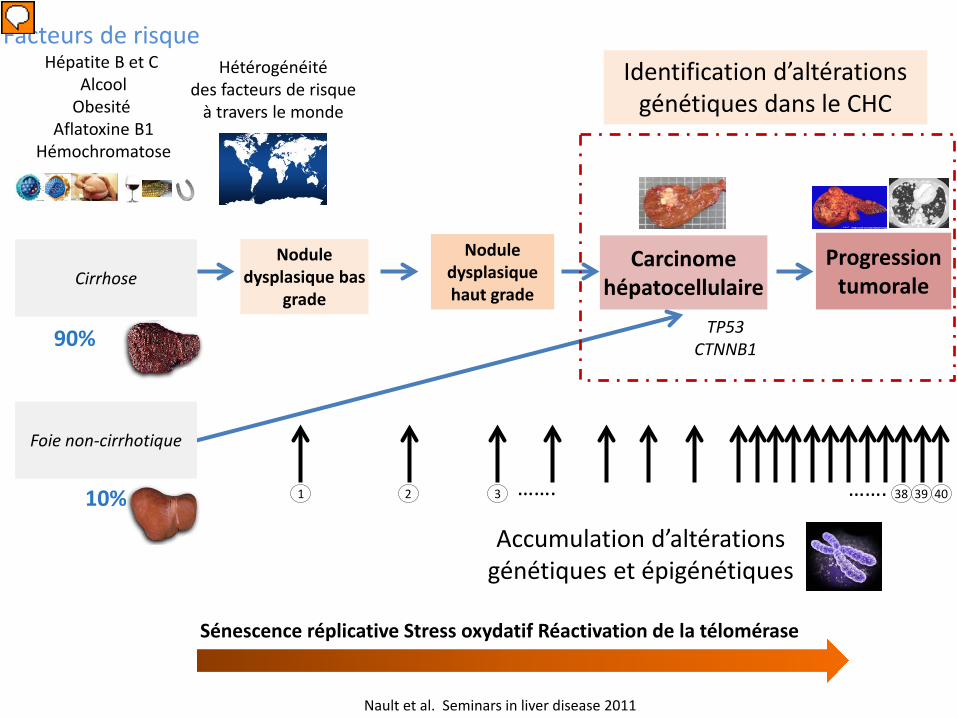
Les mutations du promoteur de TERT sont des altérations génétiques précoces de la
transformation maligne des nodules cirrhotiques en carcinome hépatocellulaire

Pas de conflits d’intérêt

Carcinome hépatocellulaire
Nodule dysplasique bas
grade
Nodule dysplasique haut grade
Cirrhose
90%
Progression tumorale
TP53 CTNNB1
Facteurs de risque Hépatite B et C
Alcool Obesité
Aflatoxine B1 Hémochromatose
Foie non-cirrhotique
10%
Hétérogénéité des facteurs de risque
à travers le monde
Accumulation d’altérations génétiques et épigénétiques
Sénescence réplicative Stress oxydatif Réactivation de la télomérase
Nault et al. Seminars in liver disease 2011
40 39 38 1 2 3 ……. …….
Carcinome hépatocellulaire
Nodule dysplasique bas
grade
Nodule dysplasique haut grade
Cirrhose
90%
Progression tumorale
TP53 CTNNB1
Facteurs de risque Hépatite B et C
Alcool Obesité
Aflatoxine B1 Hémochromatose
Foie non-cirrhotique
10%
Hétérogénéité des facteurs de risque
à travers le monde
Accumulation d’altérations génétiques et épigénétiques
Sénescence réplicative Stress oxydatif Réactivation de la télomérase
Nault et al. Seminars in liver disease 2011
40 39 38 1 2 3 ……. …….
Identification d’altérations génétiques dans le CHC

Voies de signalisation identifiées par le séquençage haut débit dans le CHC
WNT/β-Catenin P53 & Cell cycle
Chromatin remodeling PI3K/Ras Oxydative stress
Fréquence des altérations génétiques
49% 29% 25% 13% 7-8%
Guichard, Amaddeo, Imbeaud et al, Nature Genetics, 2012

WNT/β-Catenin P53 & Cell cycle
Chromatin remodeling PI3K/Ras Oxydative stress
Frequency of the pathway alteration
49% 29% 25% 13% 7-8%
Guichard, Amaddeo, Imbeaud et al, Nature Genetics, 2012 Nault JC, et al. Nature communications 2013
59%
TERT prom 59%
Telomere maintenance
Les mutations dans le promoteur de TERT sont les altérations génétiques somatiques
les plus fréquente du CHC

TERT gene TERT core promoter
ATG Transcription
start -100 pb -200 bp
G>A 6 %
Distribution des mutations 93 % 1 %
G>A G>T
Sequence of reference -GGGAGGGCCCAGGGGGCCGGGTCGGGGGAGGCCC- -146 bp -124 bp
Mutations somatiques dans 59% des CHC
Les mutations du promoteur de TERT sont exclusives
Nault et al. Nature Communications 2013
2 hot spots
Les mutations dans le promoteur de TERT sont les altérations génétiques somatiques les plus fréquente du CHC

TERT
TERC
Complexe télomérase
RNA template
Catalytic enzyme
Augmentation de l’activité télomérase
TERT promoter TERT gene
Synthèse des télomères
Prolifération, survie Echappement à la sénescence réplicative
Augmentation de l’activité de la télomérase secondaire aux mutations dans son promoteur
Augmentation de l’activité du promoteur
TERT mRNA
Mutation (substitution)
Calado R, et al. NEJM 2009 Huang FW, et al. Science 2013
TCF
TCF Création d’une séquence consensus Ets/TCF

Carcinome hépatocellulaire
Nodule dysplasique bas
grade
Nodule dysplasique haut grade
Cirrhose
90%
Progression tumorale
TP53 CTNNB1
Foie non-cirrhotique
10%
Accumulation d’altérations génétiques et épigénétiques
Sénescence réplicative Stress oxydatif Réactivation de la télomérase
Nault et al. Seminars in liver disease 2011
40 39 38 1 2 3 ……. …….
Carcinogénèse hépatique: un processus multi-étapes Génétique des lésions prénéoplasiques
et de la transformation maligne
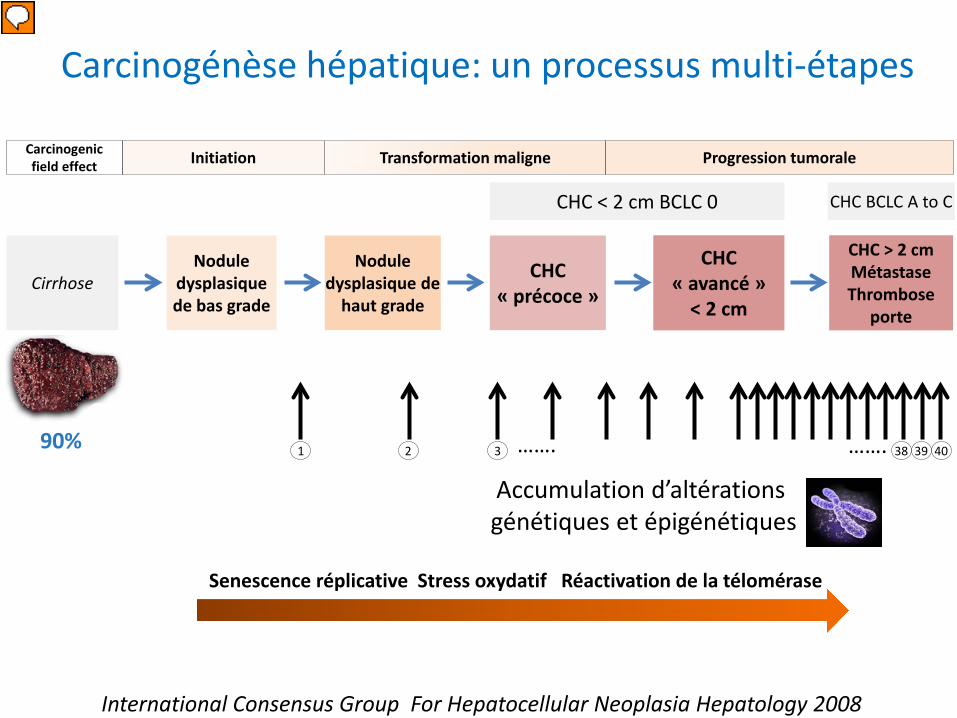
CHC « précoce »
Nodule dysplasique de bas grade
Nodule dysplasique de
haut grade Cirrhose
90%
CHC « avancé »
< 2 cm
Accumulation d’altérations génétiques et épigénétiques
Senescence réplicative Stress oxydatif Réactivation de la télomérase
CHC > 2 cm Métastase Thrombose
porte
CHC < 2 cm BCLC 0 CHC BCLC A to C
Transformation maligne Initiation Progression tumorale Carcinogenic field effect
International Consensus Group For Hepatocellular Neoplasia Hepatology 2008
40 39 38 1 2 3 ……. …….
Carcinogénèse hépatique: un processus multi-étapes

CHC « précoce »
Nodule dysplasique de bas grade
Nodule dysplasique de
haut grade Cirrhose
90%
CHC « avancé »
< 2 cm
CHC > 2 cm Métastase Thrombose
porte
CHC < 2 cm BCLC 0 CHC BCLC A to C
Transformation maligne Initiation Progression tumorale Carcinogenic field effect
Carcinogénèse hépatique: un processus multi-étapes
Difficulté diagnostique
Histologie Immunohistochimie Biologie moléculaire
Glypican 3 Glutamine synthase
Heat shock protein 70
Combinaison de 3 gènes (RT-PCR quantitative)
LYVE-1, GPC3 et SURVIVIN
Diagnostic de CHC « précoce »
Au moins 2 marqueurs positifs: Spécificité 100% sensibilité 33 à 72%
Invasion stromale Densité cellulaire, atypie nucléaire, artère isolée….
International Consensus Group Hepatology 2008 Di tomaso L Hepatology 2007 Llovet J, et al. Gastroenterology 2006

CHC « précoce »
Nodule dysplasique de bas grade
Nodule dysplasique de
haut grade Cirrhose
90%
CHC « avancé »
< 2 cm
Accumulation d’altérations génétiques et épigénétiques
CHC > 2 cm Métastase Thrombose
porte
CHC < 2 cm BCLC 0 CHC BCLC A to C
Transformation maligne Initiation Progression tumorale Carcinogenic field effect
40 39 38 1 2 3 ……. …….
Carcinogénèse hépatique: un processus multi-étapes
Nault et al. Nature Communications 2013
Mutations du promoteur de TERT dans 20% des nodules dysplasiques mais nombre
limité de cas (n=20)
But
• Décrire la fréquence des mutations du promoteur de TERT dans les nodules dysplasiques (bas grade et haut grade) sur cirrhose et dans la transformation maligne (en CHC précoce/early HCC)
• En utilisant une série de nodules développés sur cirrhose bien caractérisés au niveau histologique et immunohistochimique par un panel de 6 anatomopathologistes de 3 centres (Bordeaux, Créteil, Milan)

Méthodes • Séquençage du promoteur de TERT dans 96 nodules
cirrhotiques (37 nodules analysés en paraffine et 59 nodules avec tissu congelé) chez 58 patients dans 3 centres (Milan, Bordeaux, Créteil)
• 30 nodules sur 96 ont été séquencés pour 10 gènes impliqués dans la carcinogénèse hépatique (CTNNB1, TP53, AXIN1, ARID1A…..)
• 114 tissus cirrhotiques ont été screenés pour les
mutations dans le promoteur de TERT
Nault JC, Calderaro J, et al. Hepatology 2014 In press
Méthodes
Diagnostic à 3 niveaux
Diagnostic final= gold standard
Diagnostic dans le CR anapath
Diagnostic par consensus local entre 2
anatomopathologistes
Diagnostic par consensus final lors d’une séance de
relecture collective parles 6 anatomopathologistes
Nault JC, Calderaro J, et al. Hepatology 2014 In press

Méthodes
Séance collective de relecture par 6 anatomopathologistes des 96 nodules Histologie
Invasion stromale Atypie cellulaire
Artère isolée …..
Immunohistochimie
Glypican 3 (GPC3) Glutamine synthase (GS)
Heat Shock protein 70 (HSP70)
Nodules classés dans: Pas de consensus
Nodule dysplasique de bas grade (LGDN) Nodule dysplasique de haut grade (HGDN)
CHC « précoce » (eHCC) CHC avancé < 2 cm (spHCC)
Nault JC, Calderaro J, et al. Hepatology 2014 In press

Description des patients
114 cirrhoses supplémentaires 82% d’homme, âge moyen 61 ans
Alcool 40%, Hépatite B 16%, Hépatite C 46%, NASH 4%
58 patients avec 96 nodules développés
sur cirrhose Age 57 (47-70)
Gender (male) 40 (68%) Center Bordeaux 25 (42%)
Center Creteil 15 (26%) Center Milano 18 (32 %)
Resection 18 (31%) Liver transplantation 40 (69%)
Alcohol 26 (44%) Hepatitis B virus 5 (8%) Hepatitis C virus 24 (41%)
Hemochromatosis 2 (3%) NASH 4 (7%)
Primary biliary cirrhosis 1 (0.5%)
Nault JC, Calderaro J, et al. Hepatology 2014 In press
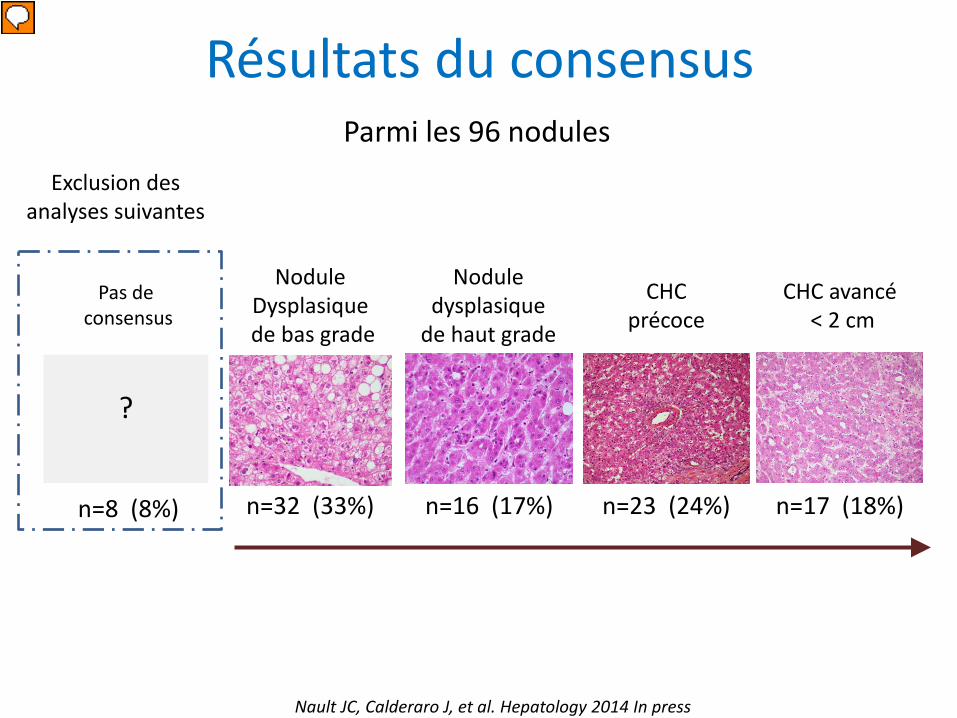
Résultats du consensus
CHC avancé < 2 cm
CHC précoce
Nodule dysplasique
de haut grade
Nodule Dysplasique
de bas grade
?
Pas de consensus
n=8 (8%) n=32 (33%) n=16 (17%) n=23 (24%) n=17 (18%)
Exclusion des analyses suivantes
Parmi les 96 nodules
Nault JC, Calderaro J, et al. Hepatology 2014 In press

Concordance interobservateur
Pour le diagnostic des nodules dysplasiques (LGDN/HGDN) par rapport aux CHC (précoce
et avancé < 2 cm)
Diagnostic consensus final
(6 anatomopathologistes)
Diagnostic CR anapath
Kappa=0.58 Moyen
Nault JC, Calderaro J, et al. Hepatology 2014 In press

Diagnostic Consensus local
(2 anatomopathologistes)
Kappa=0.744 Bon
Nault JC, Calderaro J, et al. Hepatology 2014 In press
Concordance interobservateur
Pour le diagnostic des nodules dysplasiques (LGDN/HGDN) par rapport aux CHC (précoce
et avancé < 2 cm)
Diagnostic consensus final
(6 anatomopathologistes)
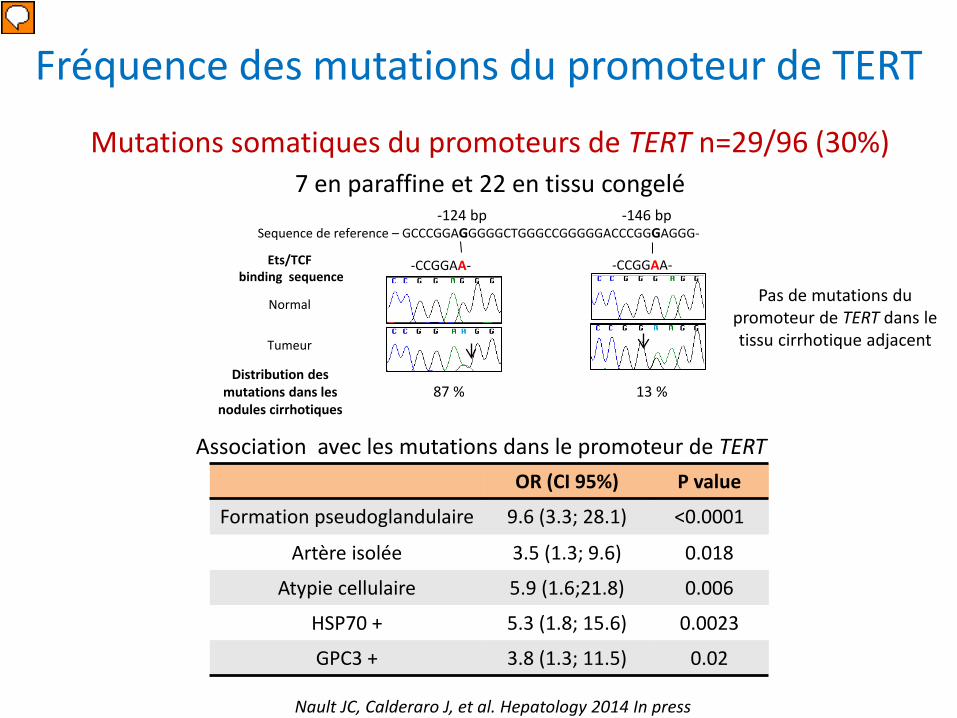
Fréquence des mutations du promoteur de TERT
Mutations somatiques du promoteurs de TERT n=29/96 (30%) 7 en paraffine et 22 en tissu congelé
OR (CI 95%) P value
Formation pseudoglandulaire 9.6 (3.3; 28.1) <0.0001
Artère isolée 3.5 (1.3; 9.6) 0.018
Atypie cellulaire 5.9 (1.6;21.8) 0.006
HSP70 + 5.3 (1.8; 15.6) 0.0023
GPC3 + 3.8 (1.3; 11.5) 0.02
Nault JC, Calderaro J, et al. Hepatology 2014 In press
Association avec les mutations dans le promoteur de TERT
Sequence de reference – GCCCGGAGGGGGCTGGGCCGGGGGACCCGGGAGGG-
-CCGGAA-
-146 bp
Ets/TCF binding sequence
Tumeur
Normal
Distribution des mutations dans les
nodules cirrhotiques 87 % 13 %
-124 bp
-CCGGAA-
Pas de mutations du promoteur de TERT dans le tissu cirrhotique adjacent
TERT promoter mutation
10 cancer genes (CTNNB1, TP53,…)
020406080
6% 19%
61% 42%
64%
Malignant transformation Initiation Tumor progression
0204060
0% 0% 0% 28%
56%
n=13 n=5 n=6 n=7 n=35
n=32 n=16 n=23 n=17 n=94
Carcinogenic field effect
0%
0%
n=172
n=172
0204060
IHC GS
020406080
IHC HSP70
020406080100IHC
GPC3
0%
0%
0% 0% 0%
4% 12% 30% 30%
7% 6% 35%
63%
56% 33%
n=58
n=58
n=58
n=26 n=16 n=23 n=15
n=26 n=16 n=23 n=15
n=26 n=16 n=23 n=15
n=22
59%
72%
n=22
70%
n=22
LGDN HGDN Early HCC
Small and progressed
HCC
HCC BCLC A to C
Cirrhotic liver
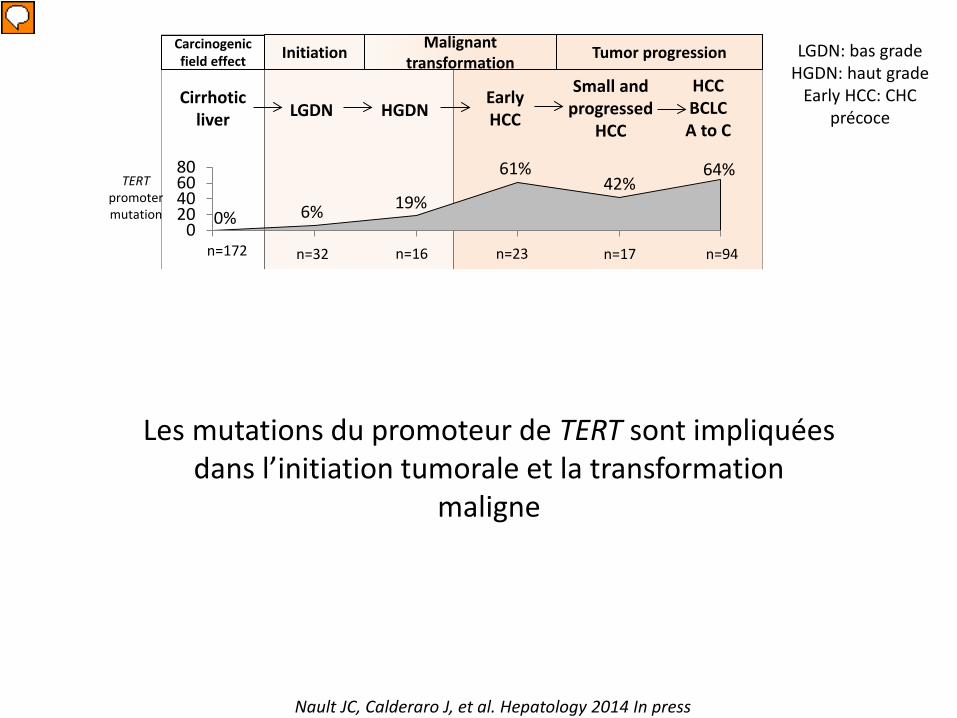
Nault JC, Calderaro J, et al. Hepatology 2014 In press
Les mutations du promoteur de TERT sont impliquées dans l’initiation tumorale et la transformation
maligne
LGDN: bas grade HGDN: haut grade
Early HCC: CHC précoce

TERT promoter mutation
10 cancer genes (CTNNB1, TP53,…)
020406080
6% 19%
61% 42%
64%
Malignant transformation Initiation Tumor progression
0204060
0% 0% 0% 28%
56%
n=13 n=5 n=6 n=7 n=35
n=32 n=16 n=23 n=17 n=94
Carcinogenic field effect
0%
0%
n=172
n=172
0204060
IHC GS
020406080
IHC HSP70
020406080100IHC
GPC3
0%
0%
0% 0% 0%
4% 12% 30% 30%
7% 6% 35%
63%
56% 33%
n=58
n=58
n=58
n=26 n=16 n=23 n=15
n=26 n=16 n=23 n=15
n=26 n=16 n=23 n=15
n=22
59%
72%
n=22
70%
n=22
LGDN HGDN Early HCC
Small and progressed
HCC
HCC BCLC A to C
Cirrhotic liver
10 gènes séquencés(CTNNB1, TP53, AXIN1, ARID1A, ARID2, NFE2L2, KEAP1, RPS6KA3, CDKN2A, PIK3CA)
Nault JC, Calderaro J, et al. Hepatology 2014 In press
Les mutations dans les autres gènes sont impliquées dans la progression tumorale
LGDN: bas grade HGDN: haut grade
Early HCC: CHC précoce

TERT promoter mutation
10 cancer genes (CTNNB1, TP53,…)
020406080
6% 19%
61% 42%
64%
Malignant transformation Initiation Tumor progression
0204060
0% 0% 0% 28%
56%
n=13 n=5 n=6 n=7 n=35
n=32 n=16 n=23 n=17 n=94
Carcinogenic field effect
0%
0%
n=172
n=172
0204060
IHC GS
020406080
IHC HSP70
020406080100IHC
GPC3
0%
0%
0% 0% 0%
4% 12% 30% 30%
7% 6% 35%
63%
56% 33%
n=58
n=58
n=58
n=26 n=16 n=23 n=15
n=26 n=16 n=23 n=15
n=26 n=16 n=23 n=15
n=22
59%
72%
n=22
70%
n=22
LGDN HGDN Early HCC
Small and progressed
HCC
HCC BCLC A to C
Cirrhotic liver
Nault JC, Calderaro J, et al. Hepatology 2014 In press
LGDN: bas grade HGDN: haut grade
Early HCC: CHC précoce

LGDN HGDN eHCC Small and progressed
HCC
DiagnosisTERT promoter mutation
Glypican 3HSP70
Glutamine synthaseCytologic atypia
Unpaired arteriesPseudoglandular
Nault JC, Calderaro J, et al. Hepatology 2014 In press
Distribution des caractéristiques histologiques, immunohistochimiques et génétiques
Dans les CHC « précoces » 61% de mutations du promoteur de TERT 39% avec au moins 2 marqueurs positifs à
l’immunohistochimie (HSP70, GPC3 and GS)

Cas sans consensus
8 cas sans consensus
diagnostique
3 cas haut grade VS CHC précoce
1 case bas grade VS CHC précoce
4 cas bas grade VS HGDN
2 cas avec mutations dans le promoteur de TERT
1 cas avec mutation dans le promoteur de TERT
HGDN vs eHCC ?
Mutation du promoteur de TERT +
HSP70 neg Glutamine synthase neg
Glypican 3 neg
Example: CHC1073T
Nault JC, Calderaro J, et al. Hepatology 2014 In press

Site internet
http://mnd-tert2014.inserm-u1162.fr/
Nault JC, Calderaro J, et al. Hepatology 2014 In press

Site internet
Nault JC, Calderaro J, et al. Hepatology 2014 In press
http://mnd-tert2014.inserm-u1162.fr/

Site internet
Nault JC, Calderaro J, et al. Hepatology 2014 In press
http://mnd-tert2014.inserm-u1162.fr/

Site internet
Nault JC, Calderaro J, et al. Hepatology 2014 In press
http://mnd-tert2014.inserm-u1162.fr/

Conclusion • Les mutations du promoteur de TERT sont les premières
altérations génétiques somatiques identifiées dans les nodules dysplasiques cirrhotiques
• Les mutations du promoteur de TERT sont impliquées dans la transformation maligne des nodules dysplasiques cirrhotiques
• Les nodules dysplasiques avec une mutation du promoteur de TERT pourraient être à risque de transformation maligne
• Les mutations dans le promoteur de TERT sont des
nouveaux biomarqueurs (paraffine et congelé) suggèrant une transformation maligne en cours ou déjà effectuée.
Nault JC, Calderaro J, et al. Hepatology 2014 In press

Inserm U1162, Paris Direction : Jessica Zucman-Rossi Julien Calderaro Sandrine Imbeaud Eric Letouze Shalini Data Gabrielle Couchy Karine Poussin Qian Cao Clément Meiller Sandra Rebouissou Andrea Fanconi
Clinicians Alexis Laurent Daniel Azoulay Laurence Chiche Jean-Frédéric Blanc
Pathologist team Massimo Roncalli Luca Di Tomaso Julien Calderaro Elie Serge Zafrani Charles Balabaud Paulette Bioulac-Sage
http://mnd-tert2014.inserm-u1162.fr/
HECAM