eccrine syringofibroadenoma (mascaro)
TRANSCRIPT
Volume 13Number 3September, 1985
scalp, odd ears and rudimentary nipples. Br I Dermatol99:423-430, 1978.
15. Bart BI, Gorlin RI, Anderson VE, Lynch FW; Congenitallocalized absence of skin and associated abnormalitiesresembling epidermolysis bullosa. Arch Dermatol 93:296-304, 1966.
Aplasia cutis congenita
16. Wojnarowska FT, Eady RA, Wells RS: Dystrophic epidermolysis bullosa presenting with congenital localizedabsence of skin; Report of four cases. Br I Dermatol108:477-483, 1983.
Eccrine syringofibroadenoma (Mascaro)
Report of two cases
Arnir H. Mehregan, M.D.,* Mehmet Marufi, M.D.,** andMaria Medenica, M.D. *** Monroe, MI, Sivas, Turkey, and Chicago, IL
We report two cases of eccrine syringafibroadenoma. Both patients had alarge, solitary hyperkeratotic nodular lesion over the extremities. Histologicsections showed spongelike masses of small cuboidal acrosyringeal cells.Fibrovascular connective tissue stroma resembling premalignant fibroepithelialtumor of Pinkus filled the spaces between the masses. (J AM ACAD
DERMATOL 13:433-436, 1985.)
Eccrine syringofibroadenoma was identified byMascaro I in 1963 among a series of lesions histologically diagnosed as premalignant fibroepithelial tumor of Pinkus, a relatively rare neoplasm ofeccrine glands. We report two cases with eccrinesyringofibroadenoma, bringing to eight the number of reported cases.
CASE REPORTSCase 1
A 78-year-old Oriental woman was seen for a growthon the lateral aspect of her right foot of several months'duration. The patient had had lepromatous leprosy andhad been treated successfully. There was, however, residual anesthesia on her feet, and a trophic ulcer was
From the Pinkus Dermatopathology Laboratory, Monroe,* the Department of Dermatology, Cumhuriyet University, Sivas,** andthe Department of Dermatology, University of Chicago.***
Accepted for publication April 25, 1985.
Reprint requests to: Dr. Amir H. Mehregan, P.O. Box 360, Monroe.MI48161.
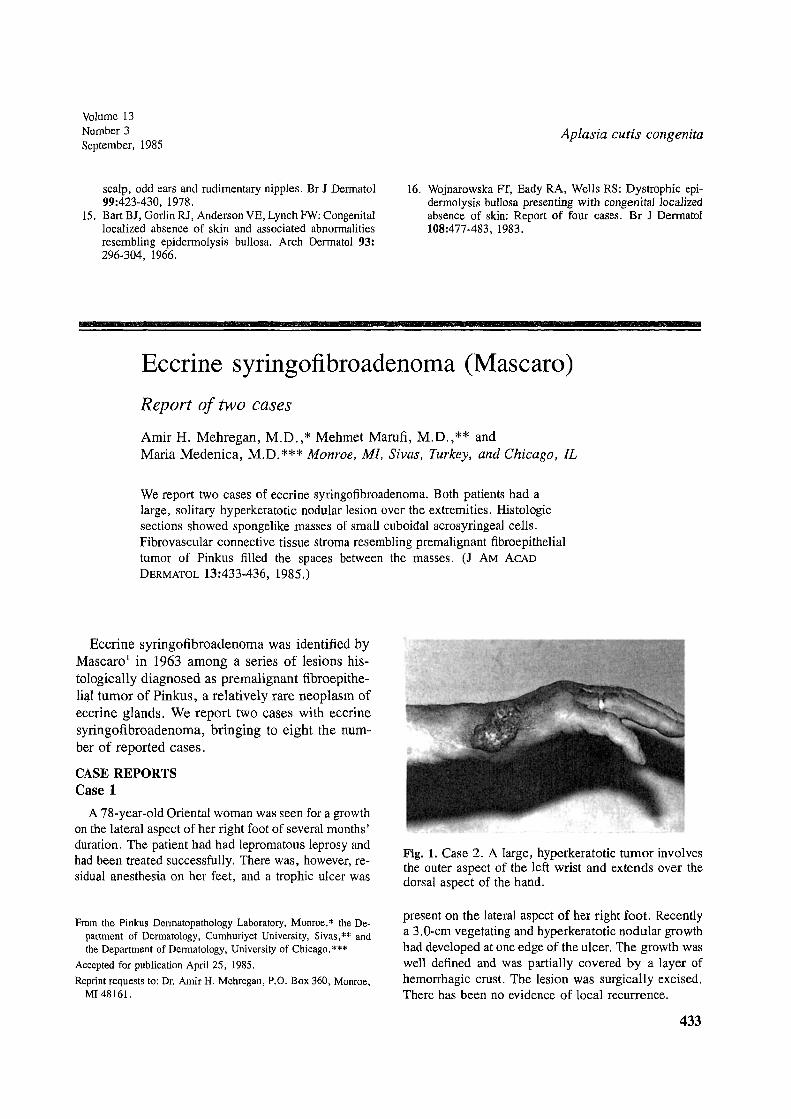
Fig. 1. Case 2. A large, hyperkeratotic tumor involvesthe outer aspect of the left wrist and extends over thedorsal aspect of the hand.
present on the lateral aspect of her right foot. Recentlya 3. a-em vegetating and hyperkeratotic nodular growthhad developed at one edge of the ulcer. The growth waswell defined and was partially covered by a layer ofhemorrhagic crust. The lesion was surgically excised.There has been no evidence of local recurrence.
433
434 Mehregan et al
Journal of theAmerican Academy of
Dermatology
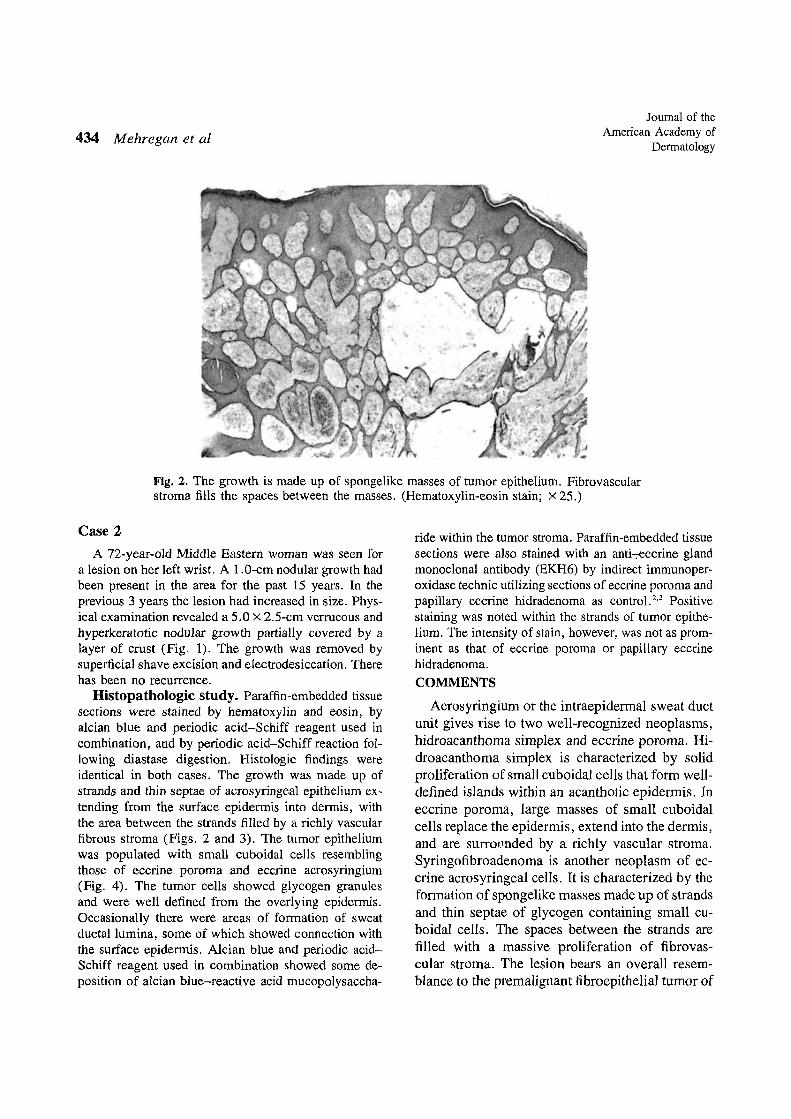
Fig. 2. The growth is made up of spongelike masses of tumor epithelium. Fibrovascularstroma fills the spaces between the masses. (Hematoxylin-eosin stain; X 25.)
Case 2A 72-year-old Middle Eastern woman was seen for
a lesion on her left wrist. A 1.a-em nodular growth hadbeen present in the area for the past 15 years. In theprevious 3 years the lesion had increased in size. Physical examination revealed a 5.0 X 2.5-cm verrucous andhyperkeratotic nodular growth partially covered by alayer of crust (Fig. 1). The growth was removed bysuperficial shave excision and electrodesiccation. Therehas been no recurrence.
Histopathologic study. Paraffin-embedded tissuesections were stained by hematoxylin and eosin, byalcian blue and periodic acid-Schiff reagent used incombination, and by periodic acid-Schiff reaction following diastase digestion. Histologic findings wereidentical in both cases. The growth was made up ofstrands and thin septae of acrosyringeal epithelium extending from the surface epidermis into dermis, withthe area between the strands filled by a richly vascularfibrous stroma (Figs. 2 and 3). The tumor epitheliumwas populated with small cuboidal cells resemblingthose of eccrine poroma and eccrine acrosyringium(Fig. 4). The tumor cells showed glycogen granulesand were well defined from the overlying epidermis.Occasionally there were areas of formation of sweatductal lumina, some of which showed connection withthe surface epidermis. Alcian blue and periodic acidSchiff reagent used in combination showed some deposition of alcian blue-reactive acid mucopolysaccha-
ride within the tumor stroma. Paraffin-embedded tissuesections were also stained with an anti-;-eccrine glandmonoclonal antibody (EKH6) by indirect immunoperoxidase technic utilizing sections of eccrine poroma andpapillary eccrine hidradenoma as control. 2,3 Positivestaining was noted within the strands of tumor epithelium. The intensity of stain, however, was not as prominent as that of eccrine poroma or papillary eccrinehidradenoma.COMMENTS
Acrosyringium or the intraepidermal sweat ductunit gives rise to two well-recognized neoplasms,hidroacanthoma simplex and eccrine poroma. Hidroacanthoma simplex is characterized by solidproliferation of small cuboidal cells that form welldefined islands within an acanthotic epidermis. Ineccrine poroma, large masses of small cuboidalcells replace the epidermis, extend into the dermis,and are sUITOl.lllded by a richly vascular stroma.Syringofibroadenoma is another neoplasm of eccrine acrosyringeal cells. Itis characterized by theformation of spongelike masses made up of strandsand thin septae of glycogen containing small cuboidal cells. The spaces between the strands arefilled with a massive proliferation of fibrovascular stroma. The lesion bears an overall resemblance to the premalignant fibroepitheliaJ tumor of
Volume 13Number 3September, 1985
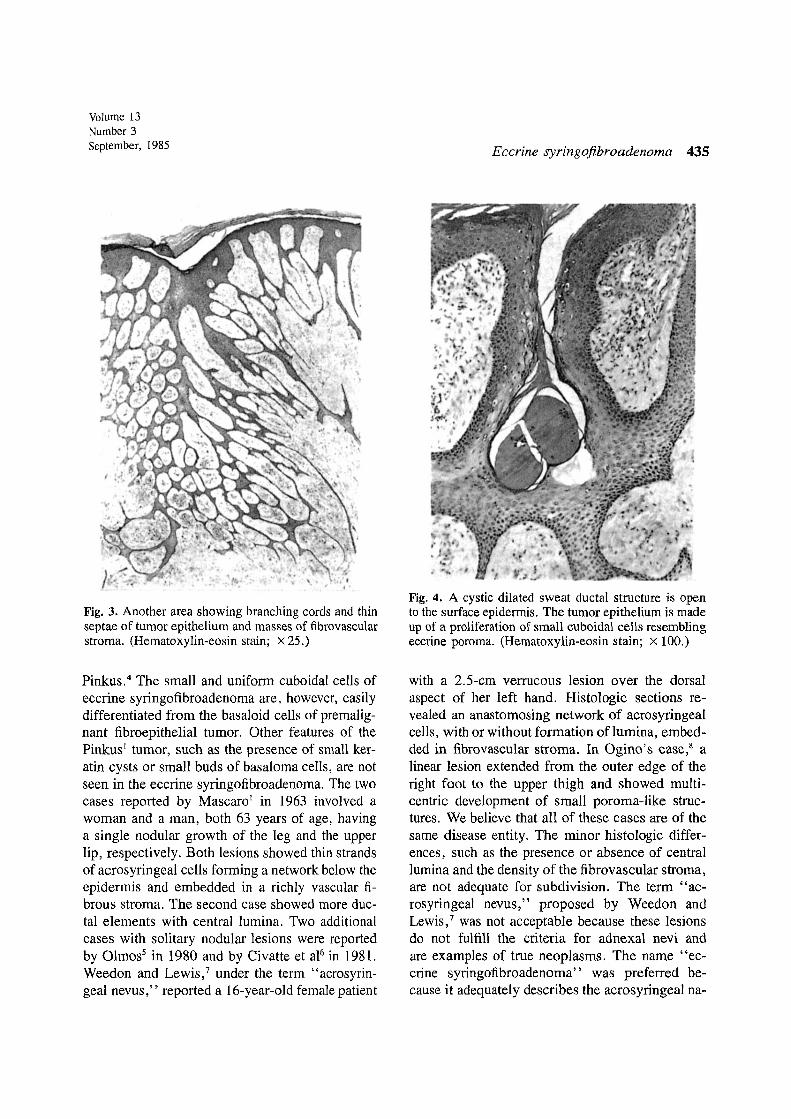
Fig. 3. Another area showing branching cords and thinseptae of tumor epithelium and masses of fibrovascularstroma. (Hematoxylin-eosin stain; x 25.)
Pinkus. 4 The small and uniform cuboidal cells ofeccrine syringofibroadenoma are, however, easilydifferentiated from the basaloid cells of premalignant fibroepithelial tumor. Other features of thePinkus l tumor, such as the presence of small keratin cysts or small buds of basaloma cells, are notseen in the eccrine syringofibroadenoma. The twocases reported by Mascaro l in 1963 involved awoman and a man, both 63 years of age, havinga single nodular growth of the leg and the upperlip, respectively. Both lesions showed thin strandsof acrosyringeal cells forming a network below theepidermis and embedded in a richly vascular fibrous stroma. The second case showed more ductal elements with central lumina. Two additionalcases with solitary nodular lesions were reportedby Olmos5 in 1980 and by Civatte et al6 in 198!.Weedon and Lewis,? under the term "acrosyringeal nevus," reported a 16-year-old female patient
Eccrine syringofibroadenoma 435
Fig. 4. A cystic dilated sweat ductal structure is opento the surface epidermis. The tumor epithelium is madeup of a proliferation of small cuboidal cells resemblingeccrine poroma. (Hematoxylin-eosin stain; X 100.)
with a 2.5-cm verrucous lesion over the dorsalaspect of her left hand. Histologic sections revealed an anastomosing network of acrosyringealcells, with or without formation of lumina, embedded in fibrovascular stroma. In Ogino's case,s alinear lesion extended from the outer edge of theright foot to the upper thigh and showed multicentric development of small poroma-like structures. We believe that all of these cases are of thesame disease entity. The minor histologic differences, such as the presence or absence of centrallumina and the density of the fibrovascular stroma,are not adequate for subdivision. The term "acrosyringeal nevus," proposed by Weedon andLewis,? was not acceptable because these lesionsdo not fulfill the criteria for adnexal nevi andare examples of true neoplasms. The name "eccrine syringofibroadenoma" was preferred because it adequately describes the acrosyringeal na-

436 Mehregan et al
ture and the prominent fibrous component of theselesions.
REFERENCES
1. Mascaro JM: Considerations sur les tumeurs fibro-epitMHales: Le syringofibroadenome eccrine. Ann Dermatol SyphiIigr 90:143-153, 1963.
2. Eto H, Matsumoto M, Kobayashi M, et al: Eccrine gIandassociated antigens: A demonstration by monoclonal antibodies. J Invest Dermatol 80:339, 1983.
3. Hashimoto K, Eto H, Matsumoto M, Hori K: Anti-keratin
Journal of theAmerican Academy of
Dermatology
monoclonal antibodies: Production specificities and applications. J Cutan PathollO:529-539, 1983.
4. Pinkus H: Premalignant fibroepithelial tumor of the skin.Arch Dermatol Syph 67:598-615, 1953.
5. Olmos L: Siringofibroadenoma ecrino de Mascaro. Citedby Civatte J, et al. 6
6. Civatte J, Jeanmougin M, Barrandon Y, Jimenez deFranch: Siringofibroadenoma ecrino de Mascaro: Discusian de un caso. Med Cutan Iber Lat Am 9:193-196, 1981.
7. Weedon D, Lewis J: Acrosyringeal nevus. J Cutan Pathol4:166-168, 1977.
8. Ogino A: Linear eccrine porema. Arch DermatoI112:841844, 1976.
ABSTRACTS
Melanose de friction
Hidano A, Mizuguchi M, Higaki Y: Ann DennatolVenereollll:1063-1071, 1984
From Tokyo comes the interesting observation of twentythree cases demonstrating an unusual pattern of hyperpigmentation localized over bony tissues such as the clavicle,vertebral column, and scapula. The pigmentary alteration often assumed such bizarre configurations as zebra-like stripingor a ripple-like aspect. Histologic examination of lesions revealed a pattern consistent with postinflammatory hyperpigmentation. The authors propose the term friction melanosisfor this unusual entity, which they feel develops as a consequence of repeated friction from the use of nylon brusheswhile bathing, a practice currently popular among young Japanese. Most cases could be related to an antecedent historyof daily usage of such brushes, and in several instances thepigmentation was observed to regress following cessation ofthis practice. This entity should be distinguished from otherdisorders ofhyperpigmentation, such as macular amyloidosis.
S. H.
The three viruses of non.A, non-B hepatitis
Tabor E: Lancet 1:743-745, 1985
Non-A, non-B hepatitis includes infections of the livercaused by at least three viruses. The viruses are provisionallydesignated "blood-transmitted," "coagulation-factor-transmitted," and "epidemic water-borne." Ifconfirmed, the report of a reverse transcriptase in blood-transmitted non-A,non-B hepatitis would mean that the etiologic agent is eithera retrovirus or closely resembles one.
J. G. S.
On the nature of a defect in cells from individualswith ataxia-telangiectasia
Cornforth MN, Bedford IS: Science 227:1589-1591,1985
Cells and tissues of patients with ataxis-telangiectasia areabnormally sensitive to ionizing radiation. Fibroblasts fromataxia-telangiectasia exposed to a dose of 6.0 grays had thesame initial frequency of breaks and the same rate for rejoining of the breaks in the chromosomes as controls but thefraction of breaks that did not rejoin was five to six timesgreater for the ataxia-telangiectasia cells.
J. G. S.
Erythema nodosum and circulating immunecomplexes in acne fulminans after treatment withisotretinoin
Kellett JK, Beck MH, Chalmers RJG: Br Med J290:820, 1985
Two patients with acne vulgaris treated with isotretinoin,1 mg/kg/day, after 3 weeks' therapy developed ulceratingcystic acne, fever, arthralgia, and erythema nodosum. Theplatelet aggregation tests for circulating IgG immune complexes were positive in both patients. Both responded rapidlyto prednisolone (25-30 mg daily) with a fall in titer of circulating immune complexes to normal within 4 weeks. Isotretinoin was continued at 1 mg/kg daily with excellent resultsin 3 to 4 months.
J. G. S.