Tumeur du Foie
Beno�t Gallix, Eric AssenatService d’Imagerie Abdominale et DigestiveH�pital Saint-�loi
Montpellier
SFR
LRM
ars2
013
Terrain du CHC
Foie cirrhotique > 90%
Foie non cirrhotique < 10%
Mal. chronique du foie +++
Foie sain exceptionnel
SFR
LRM
ars2
013
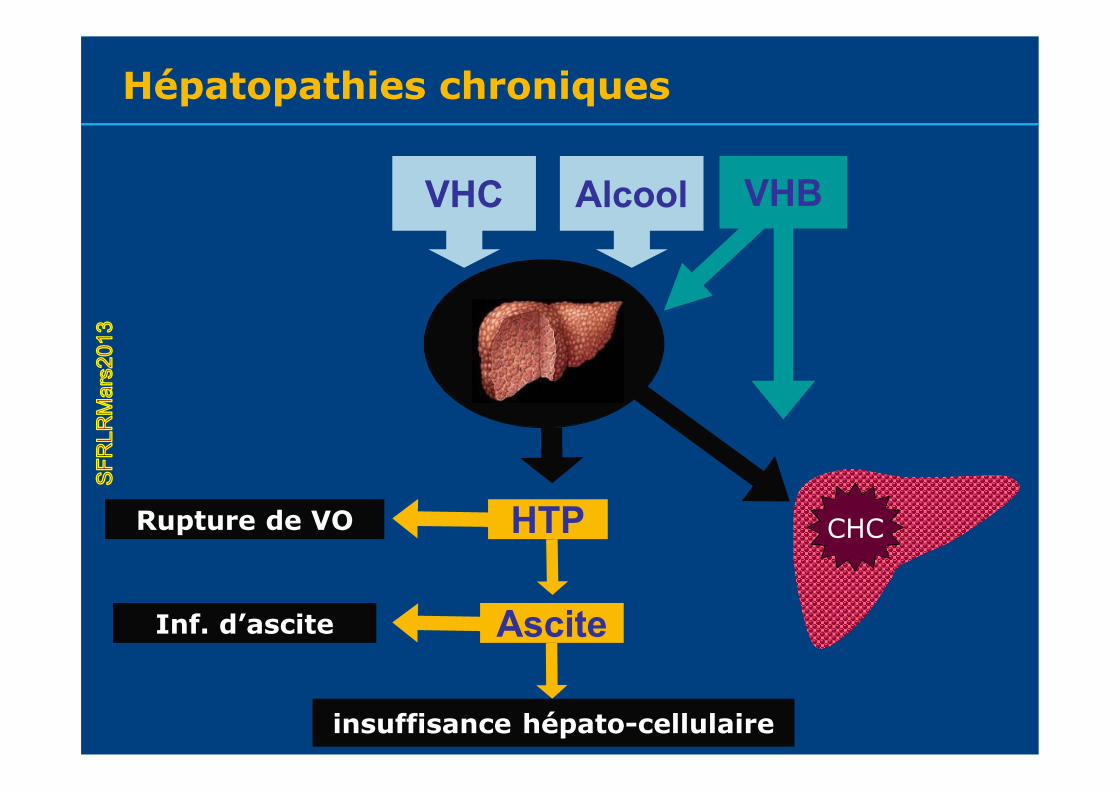
insuffisance h�pato-cellulaire
Rupture de VO
Inf. d’ascite
VHC Alcool
CHCHTP
Ascite
VHB
H�patopathies chroniquesS
FRLR
Mar
s201
3
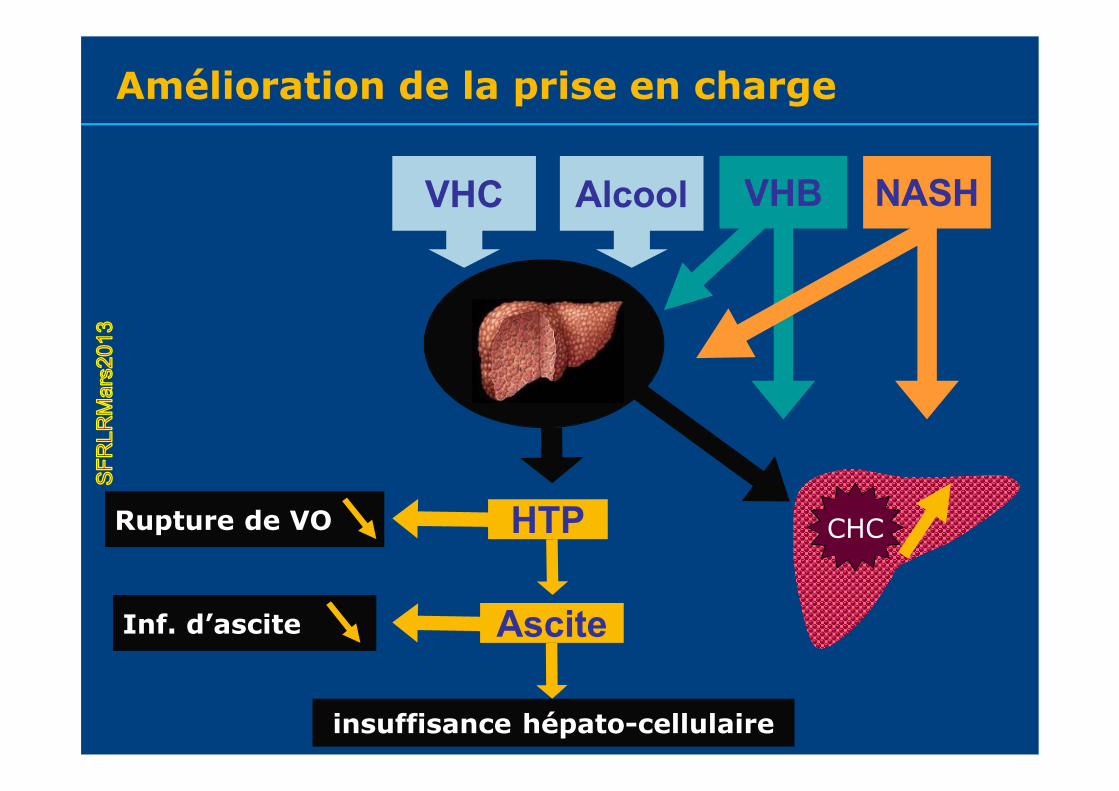
Am�lioration de la prise en charge
insuffisance h�pato-cellulaire
Rupture de VO
Inf. d’ascite
VHC Alcool
CHCHTP
Ascite
VHB NASH
SFR
LRM
ars2
013
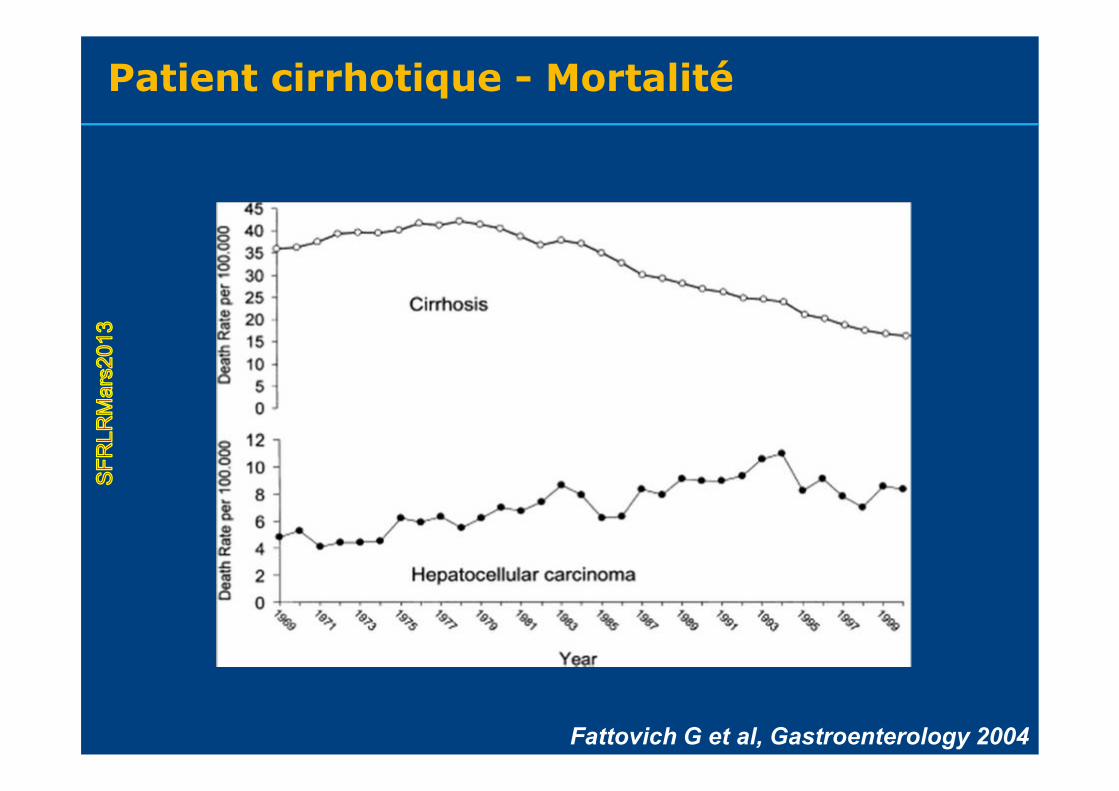
Patient cirrhotique - Mortalit�
Fattovich G et al, Gastroenterology 2004
SFR
LRM
ars2
013
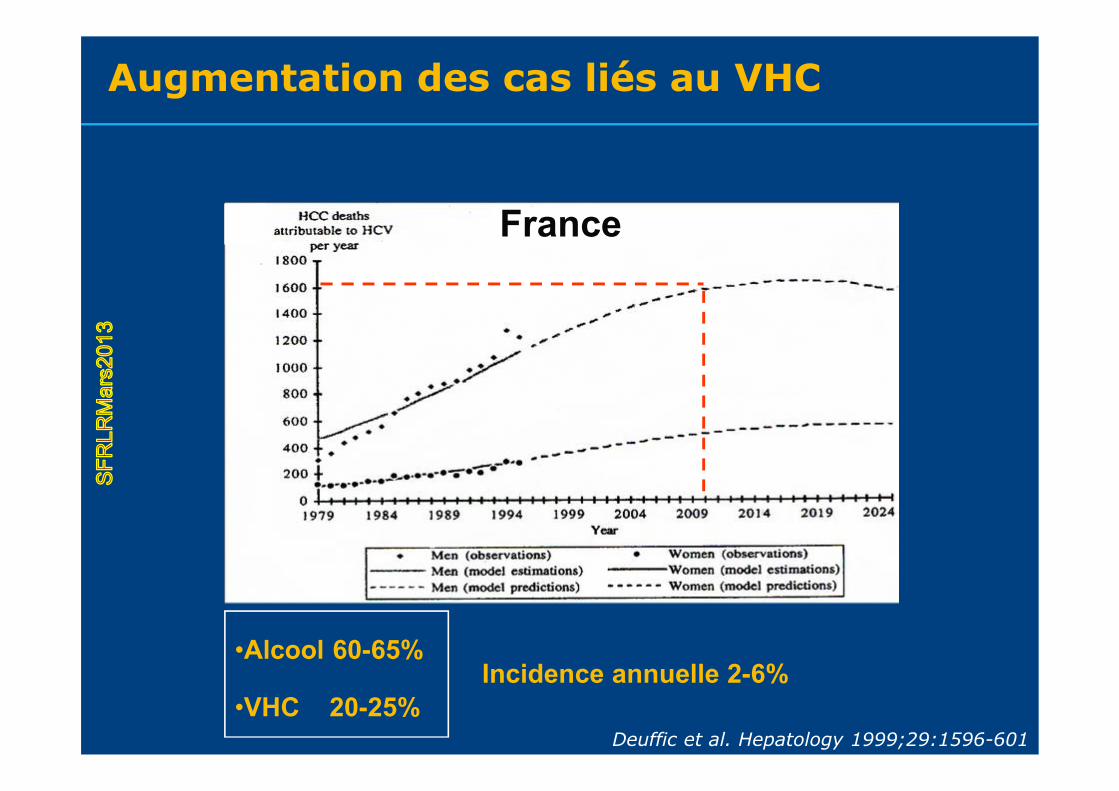
Augmentation des cas li�s au VHC
Deuffic et al. Hepatology 1999;29:1596-601
France
•Alcool 60-65%
•VHC 20-25%Incidence annuelle 2-6%
SFR
LRM
ars2
013

�pid�miologie du CHC
McGlynn et al. BPRCG 2005;19:3-23
SFR
LRM
ars2
013
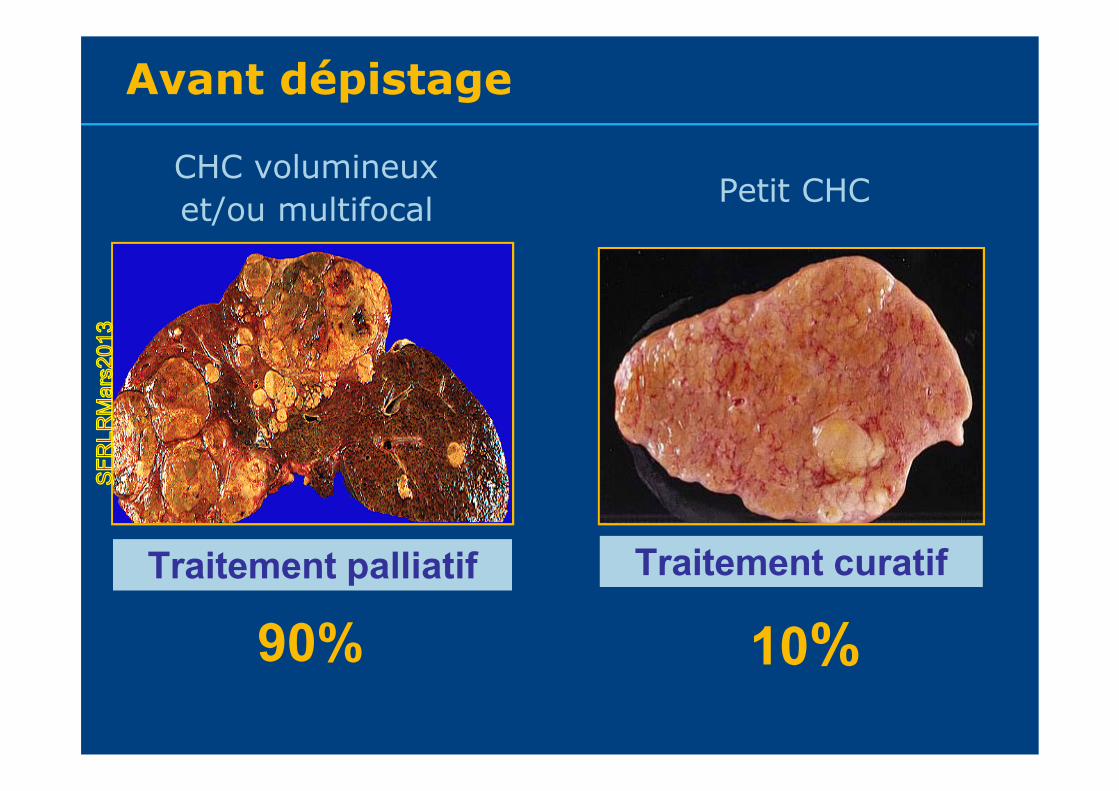
Avant d�pistage
Traitement palliatif Traitement curatif
CHC volumineux et/ou multifocal Petit CHC
90% 10%
SFR
LRM
ars2
013
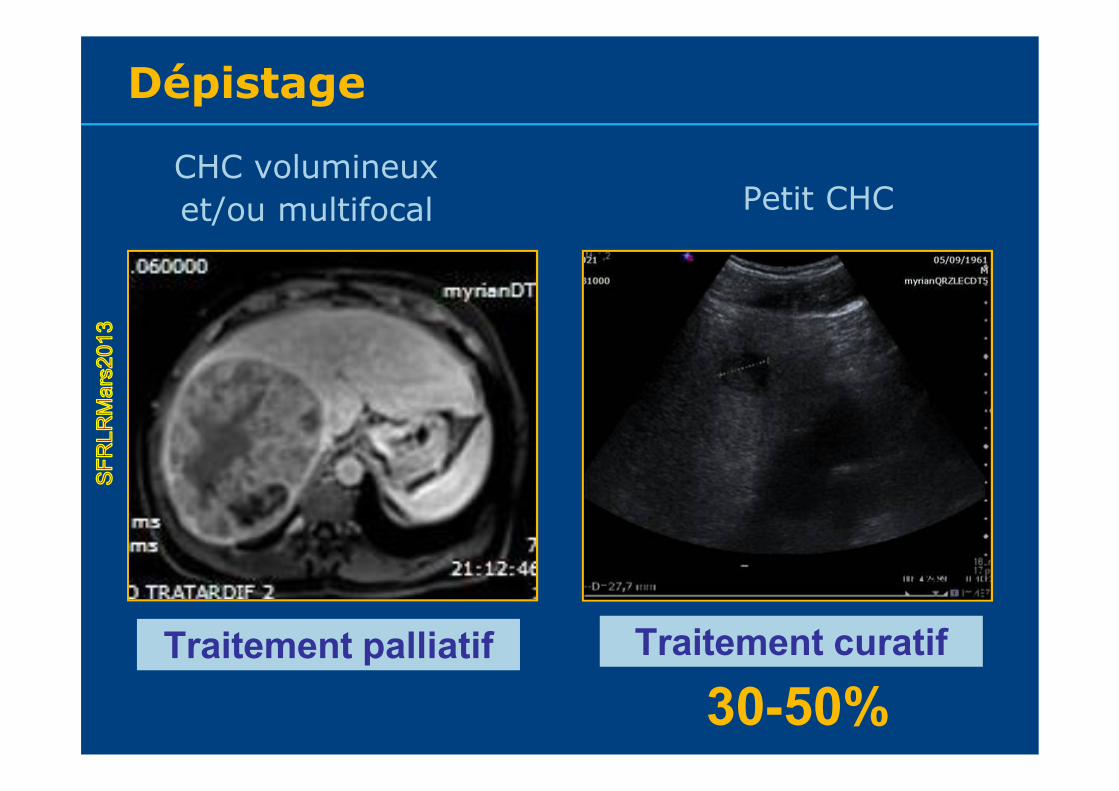
Traitement palliatif Traitement curatif
CHC volumineux et/ou multifocal Petit CHC
30-50%
D�pistageS
FRLR
Mar
s201
3
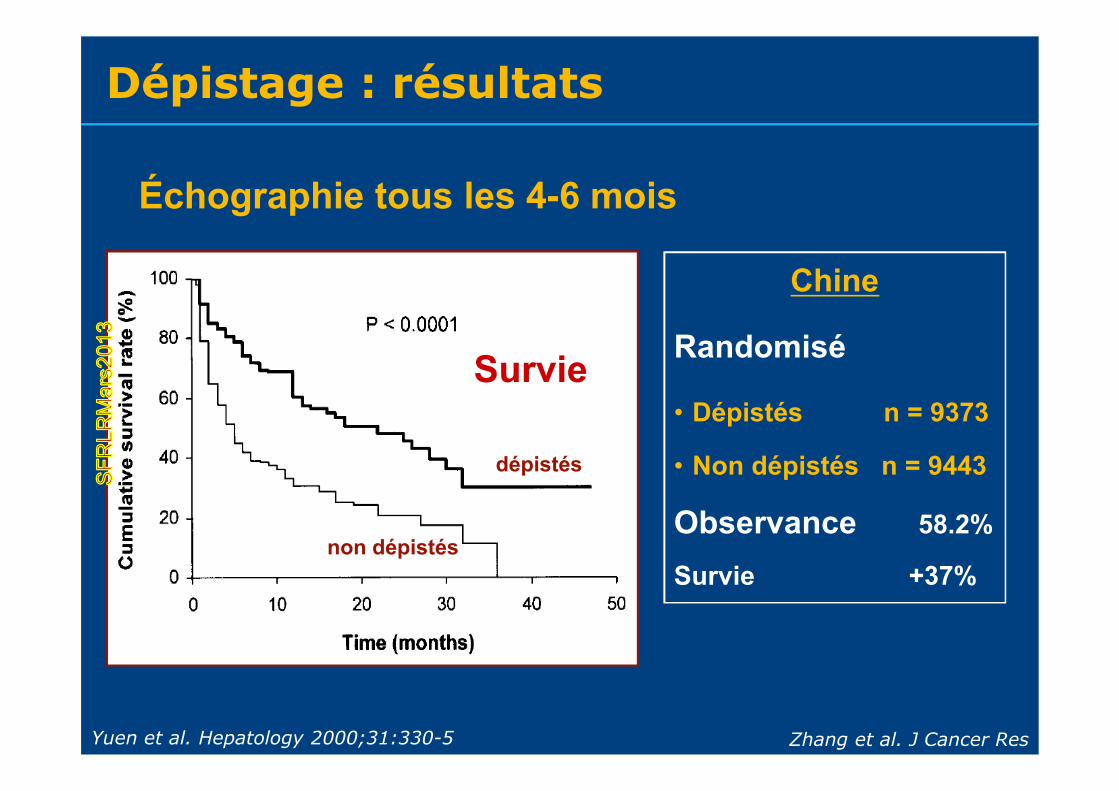
Yuen et al. Hepatology 2000;31:330-5
dÄpistÄs
non dÄpistÄs
Zhang et al. J Cancer Res
Chine
RandomisÄ
• DÄpistÄs n = 9373
• Non dÄpistÄs n = 9443
Observance 58.2%
Survie +37%
Åchographie tous les 4-6 mois
D�pistage : r�sultats
Survie
SFR
LRM
ars2
013
Donn�es anatomo-pathologiques
Analyse des pi�ces de THO ou r�section Diff�rentiation tumoraleGrade d’EdmondsonMicro-invasion vasculaire
SFR
LRM
ars2
013
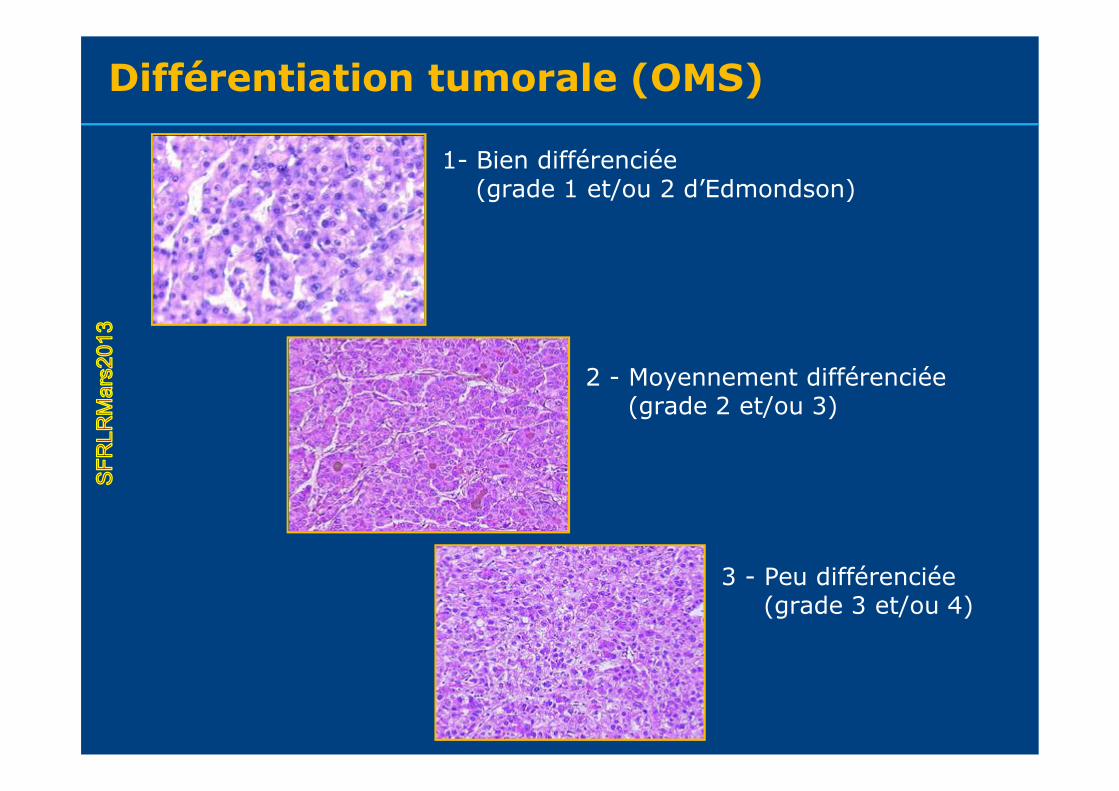
Diff�rentiation tumorale (OMS)
1- Bien diff�renci�e(grade 1 et/ou 2 d’Edmondson)
3 - Peu diff�renci�e(grade 3 et/ou 4)
2 - Moyennement diff�renci�e(grade 2 et/ou 3)
SFR
LRM
ars2
013
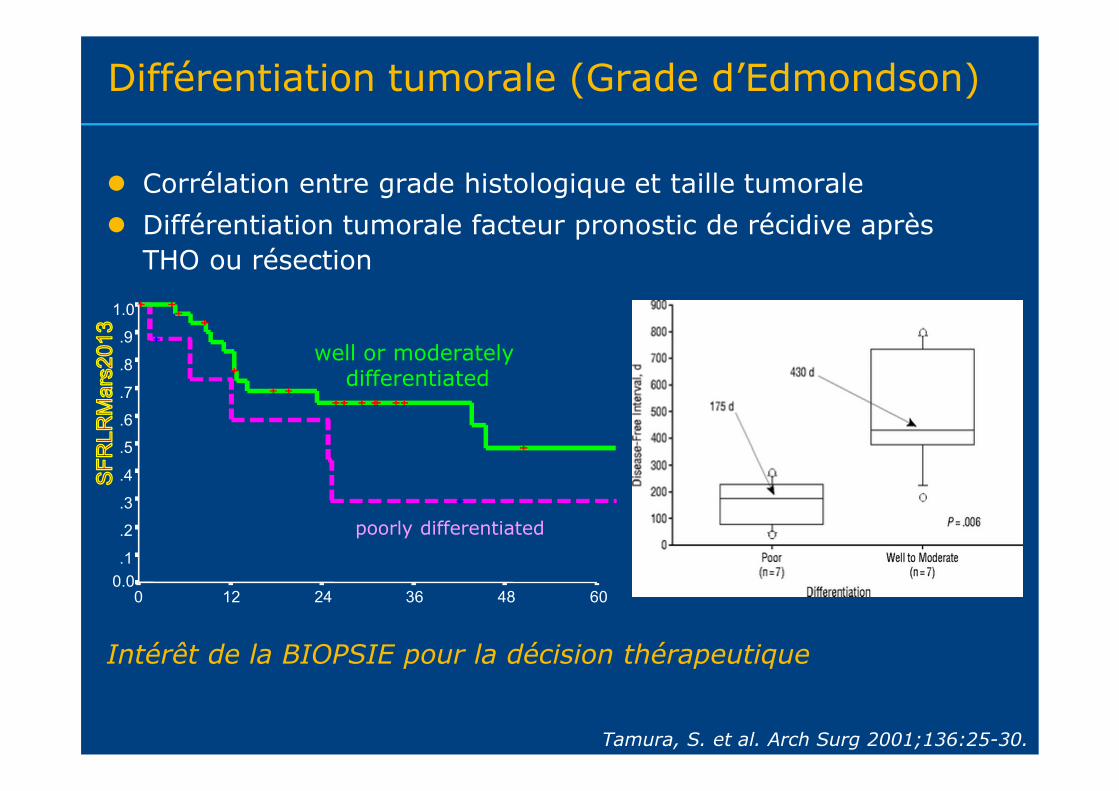
Diff�rentiation tumorale (Grade d’Edmondson)
Corr�lation entre grade histologique et taille tumorale Diff�rentiation tumorale facteur pronostic de r�cidive apr�s
THO ou r�section
IntÄrÅt de la BIOPSIE pour la dÄcision thÄrapeutique
Tamura, S. et al. Arch Surg 2001;136:25-30.
well or moderatelydifferentiated
60483624120
1.0
.9
.8
.7
.6
.5
.4
.3
.2
.10.0
poorly differentiated
SFR
LRM
ars2
013
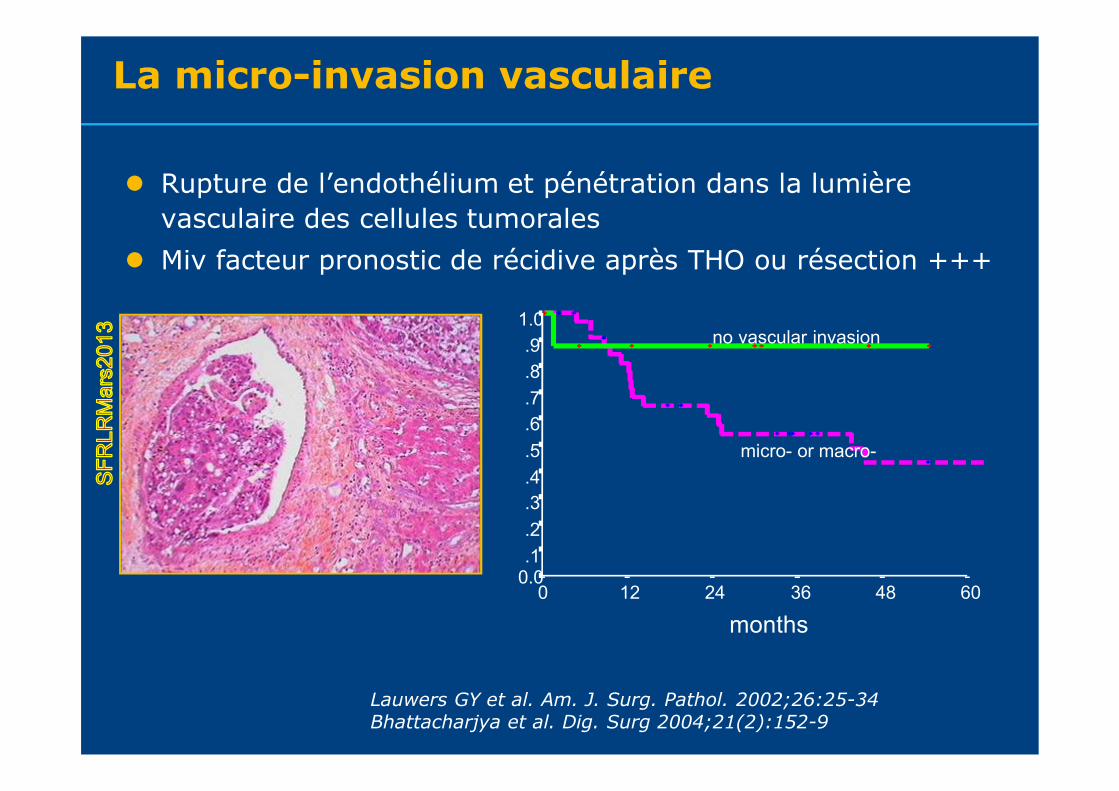
La micro-invasion vasculaire
Rupture de l’endoth�lium et p�n�tration dans la lumi�re vasculaire des cellules tumorales
Miv facteur pronostic de r�cidive apr�s THO ou r�section +++
Lauwers GY et al. Am. J. Surg. Pathol. 2002;26:25-34Bhattacharjya et al. Dig. Surg 2004;21(2):152-9
months60483624120
1.0.9.8.7.6.5.4.3.2.1
0.0
no vascular invasion
micro- or macro-
SFR
LRM
ars2
013
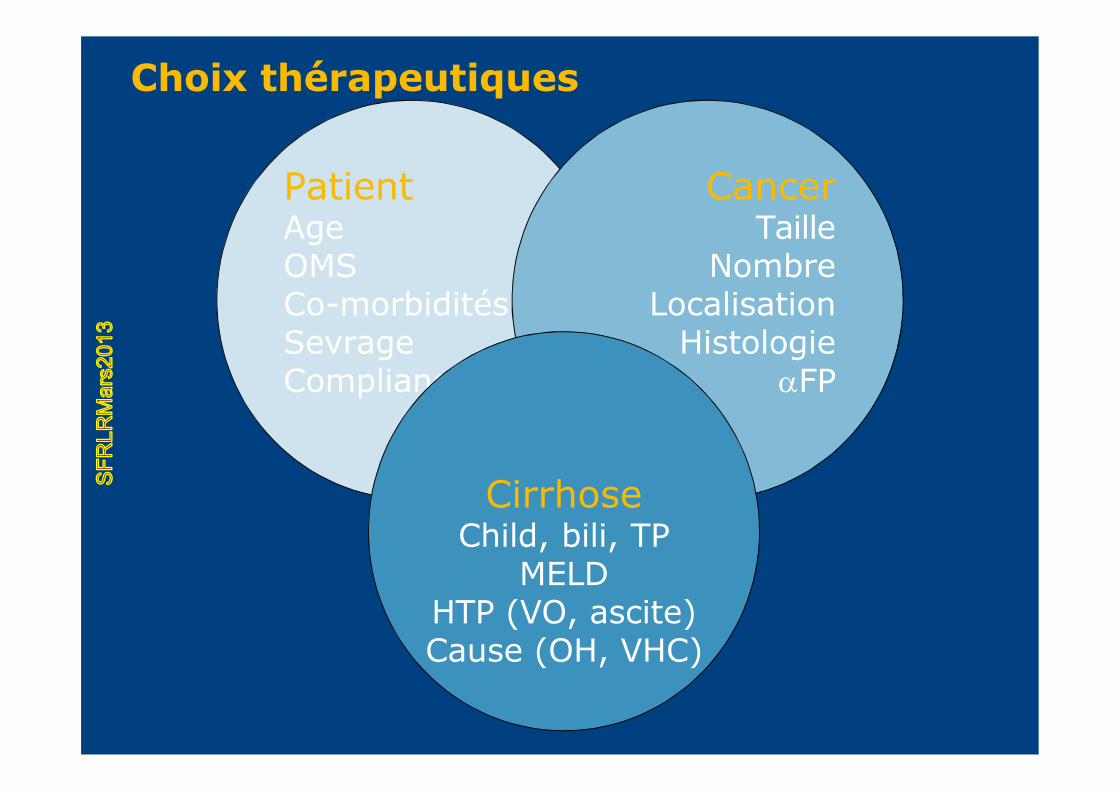
PatientAgeOMSCo-morbidit�sSevrageCompliance
CancerTaille
NombreLocalisation
HistologieFP
CirrhoseChild, bili, TP
MELDHTP (VO, ascite)Cause (OH, VHC)
Choix th�rapeutiquesS
FRLR
Mar
s201
3
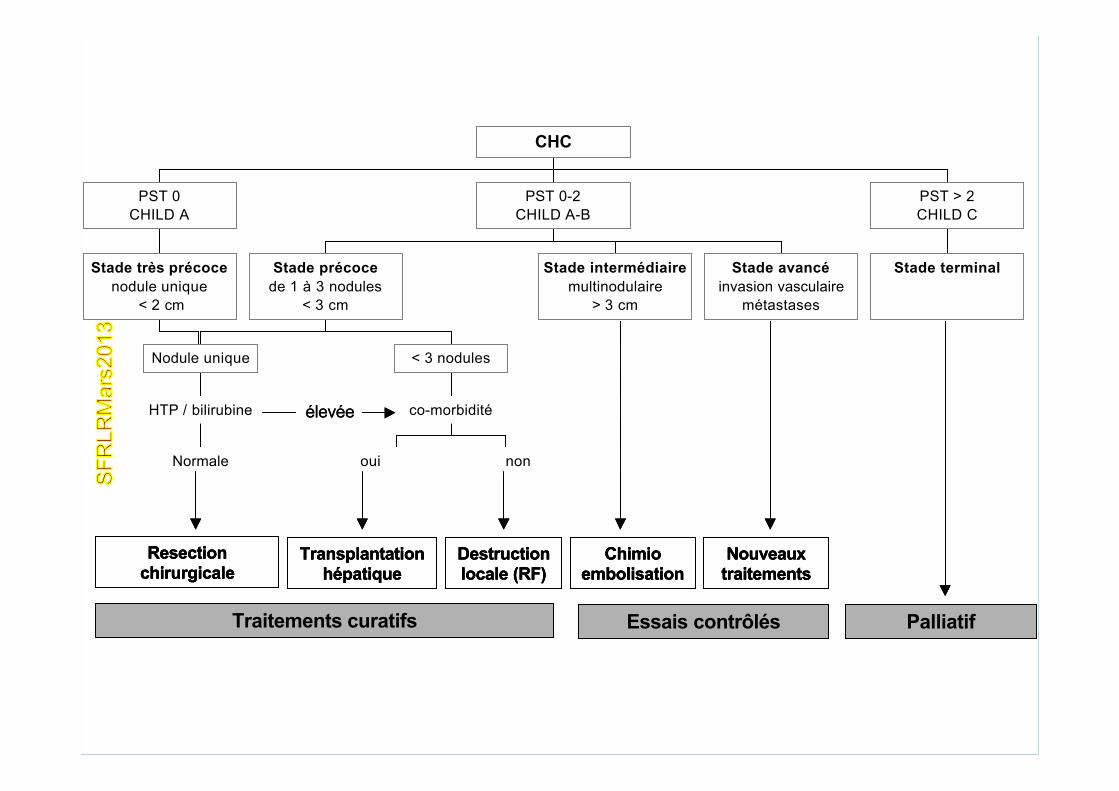
Stade trÇs prÄcocenodule unique
< 2 cm
PST 0CHILD A
Normale
HTP / bilirubine
Nodule unique
oui non
co-morbidit�
< 3 nodules
Stade prÄcocede 1 � 3 nodules
< 3 cm
Stade intermÄdiairemultinodulaire
> 3 cm
Stade avancÄinvasion vasculaire
m�tastases
PST 0-2CHILD A-B
Stade terminal
PST > 2CHILD C
CHC
Resectionchirurgicale
TransplantationhÄpatique
Destruction locale (RF)
Chimio embolisation
Nouveaux traitements
Traitements curatifs Essais contrÉlÄs Palliatif
�lev�e
Stade trÇs prÄcocenodule unique
< 2 cm
PST 0CHILD A
Normale
HTP / bilirubine
Nodule unique
oui non
co-morbidit�
< 3 nodules
Stade prÄcocede 1 � 3 nodules
< 3 cm
Stade intermÄdiairemultinodulaire
> 3 cm
Stade avancÄinvasion vasculaire
m�tastases
PST 0-2CHILD A-B
Stade terminal
PST > 2CHILD C
CHC
Resectionchirurgicale
TransplantationhÄpatique
Destruction locale (RF)
Chimio embolisation
Nouveaux traitements
Traitements curatifs Essais contrÉlÄs Palliatif
Stade trÇs prÄcocenodule unique
< 2 cm
PST 0CHILD A
Normale
HTP / bilirubine
Nodule unique
oui non
co-morbidit�
< 3 nodules
Stade prÄcocede 1 � 3 nodules
< 3 cm
Stade intermÄdiairemultinodulaire
> 3 cm
Stade avancÄinvasion vasculaire
m�tastases
PST 0-2CHILD A-B
Stade terminal
PST > 2CHILD C
CHC
Resectionchirurgicale
TransplantationhÄpatique
Destruction locale (RF)
Chimio embolisation
Nouveaux traitements
Traitements curatifs Essais contrÉlÄs Palliatif
�lev�e
SFR
LRM
ars2
013
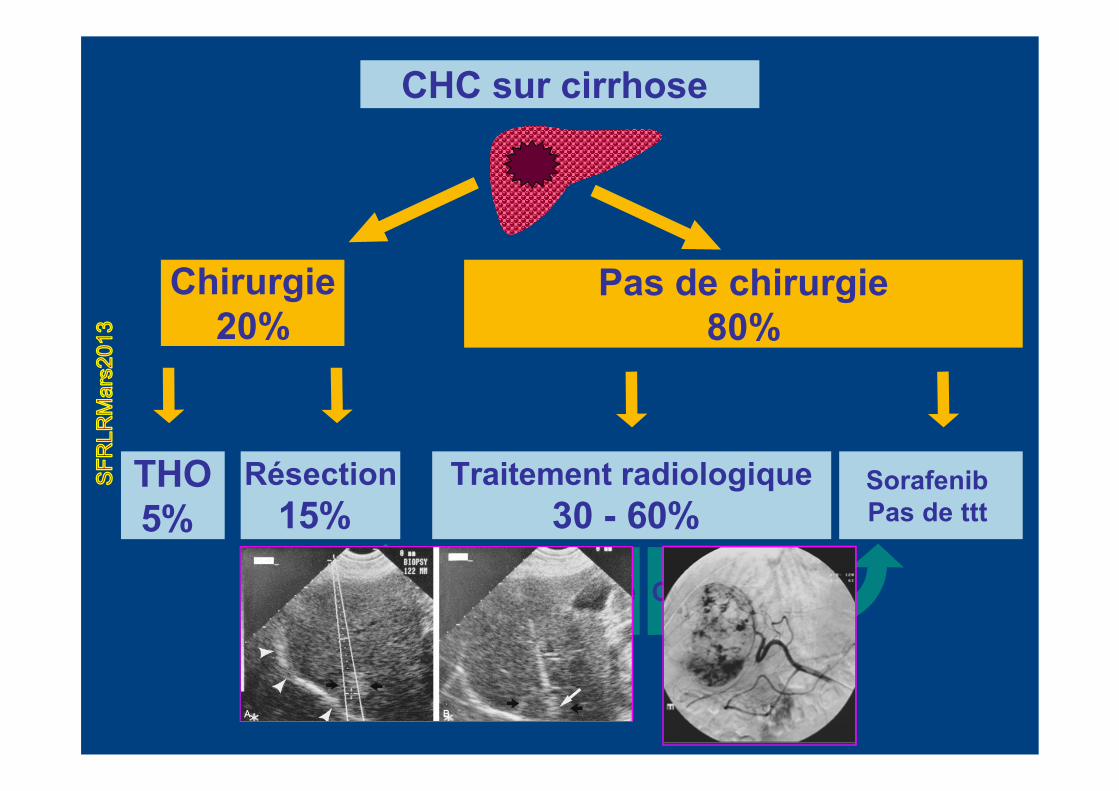
CHC sur cirrhose
Chirurgie20%
Pas de chirurgie80%
THO5%
RÄsection15%
Traitement radiologique30 - 60%
Sorafenib Pas de ttt
RadiofrÄquence Chimioembol
SFR
LRM
ars2
013
1. Est-ce un CHC vs nodule b�nin ?
Petit nodules +++
2. Pouvez-vous m’apporter une preuve histologique ?
3. Quel est la taille et le nombre de nodules ?
4. Y a-t-il des �l�ments p�joratifs ?
invasion vasculaire
Questions de l’Oncologue digestifPhase diagnostique
SFR
LRM
ars2
013
1. Pouvez traiter ce patient en RI ? RF, CHIMIOEMBOL, YTTRIUM, …
2. Comment �valuer la r�ponse ?
3. Comment �valuer la r�ponse pr�cocement ?
4. Comment surveiller les patients trait�s ?
Questions de l’Oncologue digestifPhase Th�rapeutique
SFR
LRM
ars2
013
M�tastases H�patique
SFR
LRM
ars2
013
CCR + L�sion h�patique
M�tastase ?M�tastase ?
R�s�cabilit� / Traitement
local ?
R�s�cabilit� / Traitement
local ?S�lection
Traitement
R�ponse th�rapeutique
?
R�ponse th�rapeutique
?
SFR
LRM
ars2
013
Bilan pr�-th�rapeutiqueLe test id�al (Guidelines 2003)
Y a t-il des l�sions h�patiques ?
S’agit-il vraiment de m�tastases h�patiques ?
Toutes les m�tastases h�patiques pr�sentes sont-elles d�tect�es ?
Les m�tastases d�tect�es sont-elles accessibles � une th�rapeutique � vis�e curative ?
Y-a-t-il une r�cidive loco-r�gionale ou des m�tastases extra-h�patiques ?
SFR
LRM
ars2
013
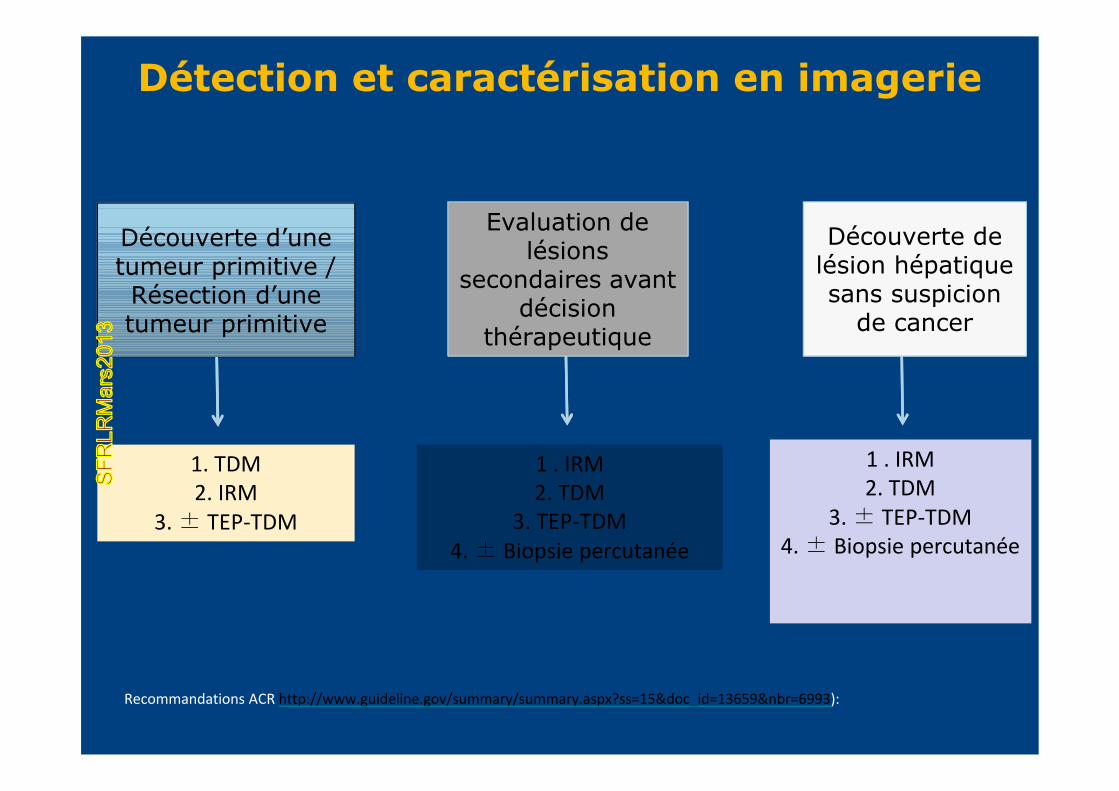
D�tection et caract�risation en imagerie
D�couverte d’une tumeur primitive / R�section d’une tumeur primitive
Evaluation de l�sions
secondaires avant d�cision
th�rapeutique
D�couverte de l�sion h�patique sans suspicion
de cancer
1. TDM2. IRM
3. Ä TEP-TDM
1 . IRM2. TDM
3. TEP-TDM4. Ä Biopsie percutanÄe
1 . IRM2. TDM
3. Ä TEP-TDM4. Ä Biopsie percutanÄe
Recommandations ACR http://www.guideline.gov/summary/summary.aspx?ss=15&doc_id=13659&nbr=6993):
SFR
LRM
ars2
013
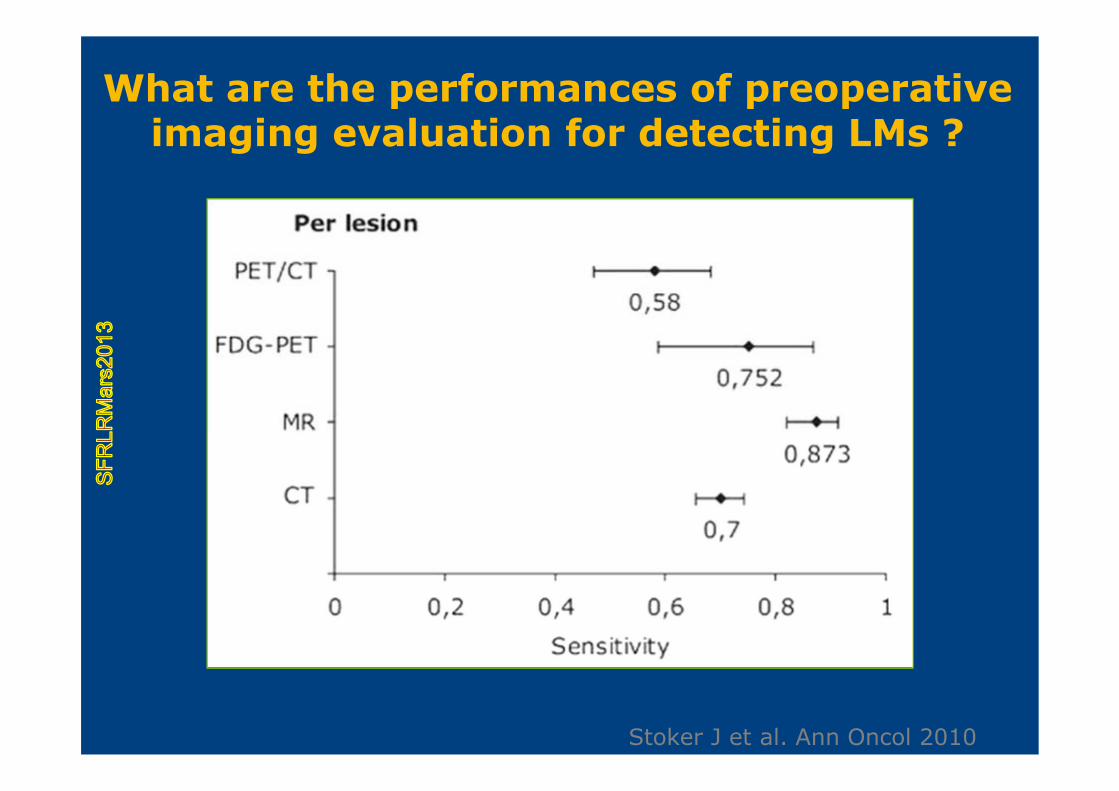
Stoker J et al. Ann Oncol 2010
What are the performances of preoperative imaging evaluation for detecting LMs ?
SFR
LRM
ars2
013
�valuation apr�s � Chimioth�rapie �
Faite une �valuation standardis� de la r�ponse simplement (RECIST)
Progression / Stable / RP / RC
Comment �valuer pr�cocement la r�ponse ?
SFR
LRM
ars2
013
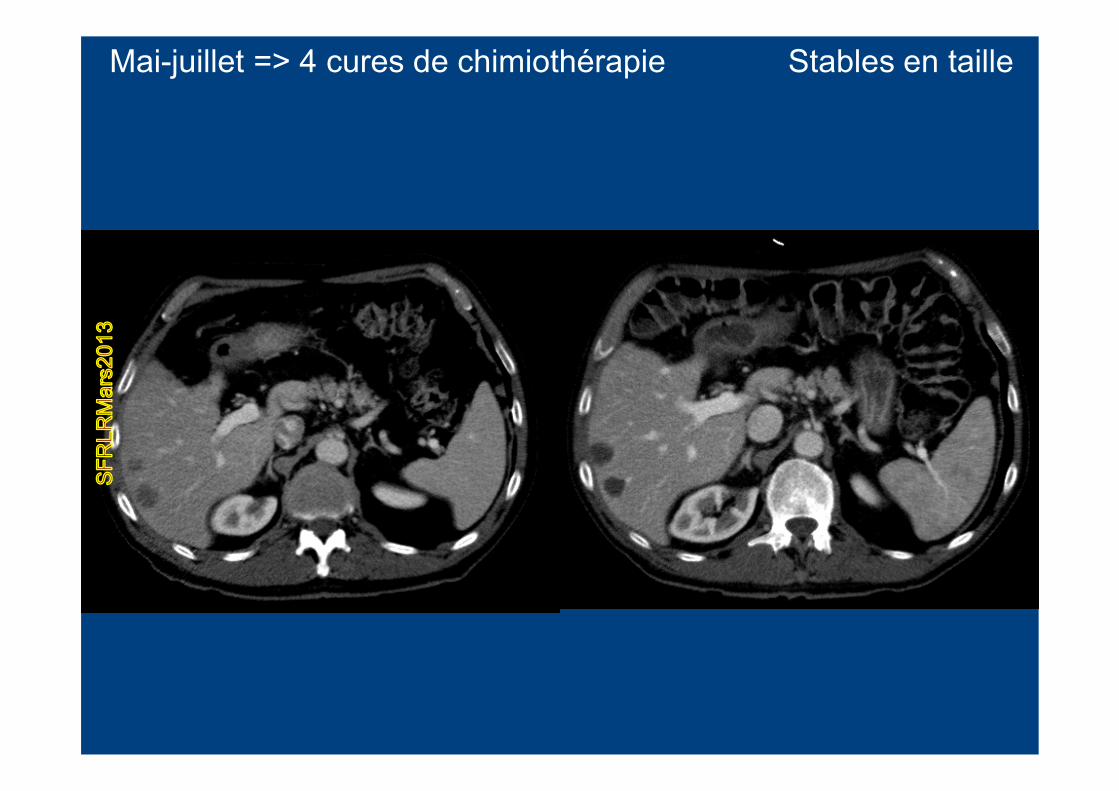
Mai-juillet => 4 cures de chimioth�rapie Stables en tailleS
FRLR
Mar
s201
3
�valuation apr�s � Chimioth�rapie �
Faite une �valuation standardis� de la r�ponse simplement (RECIST)
Progression / Stable / RP / RC
Comment �valuer pr�cocement la r�ponse ?
Les m�tastases d�tect�es sont-elles devenues accessibles � une th�rapeutique � vis�e curative ?
Les m�tastases ont elles disparues?
SFR
LRM
ars2
013
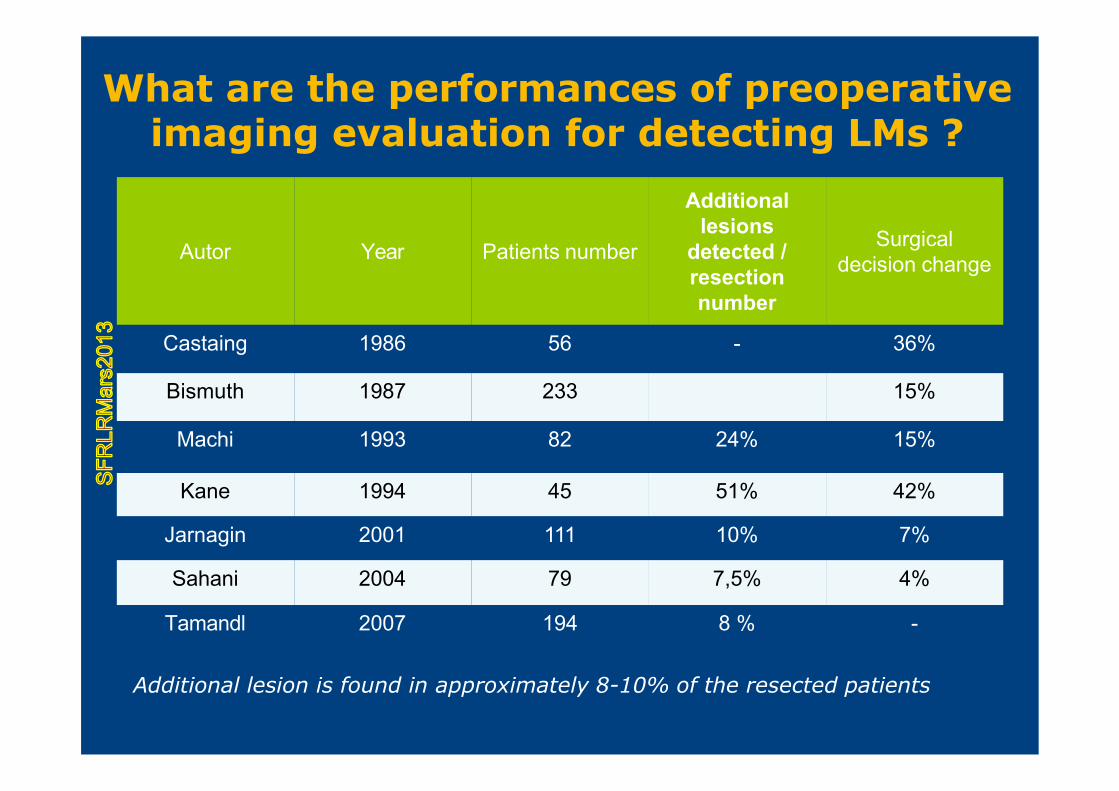
What are the performances of preoperative imaging evaluation for detecting LMs ?
Autor Year Patients number
Additional lesions
detected / resection number
Surgical decision change
Castaing 1986 56 - 36%
Bismuth 1987 233 15%
Machi 1993 82 24% 15%
Kane 1994 45 51% 42%
Jarnagin 2001 111 10% 7%
Sahani 2004 79 7,5% 4%
Tamandl 2007 194 8 % -
Additional lesion is found in approximately 8-10% of the resected patients
SFR
LRM
ars2
013
.
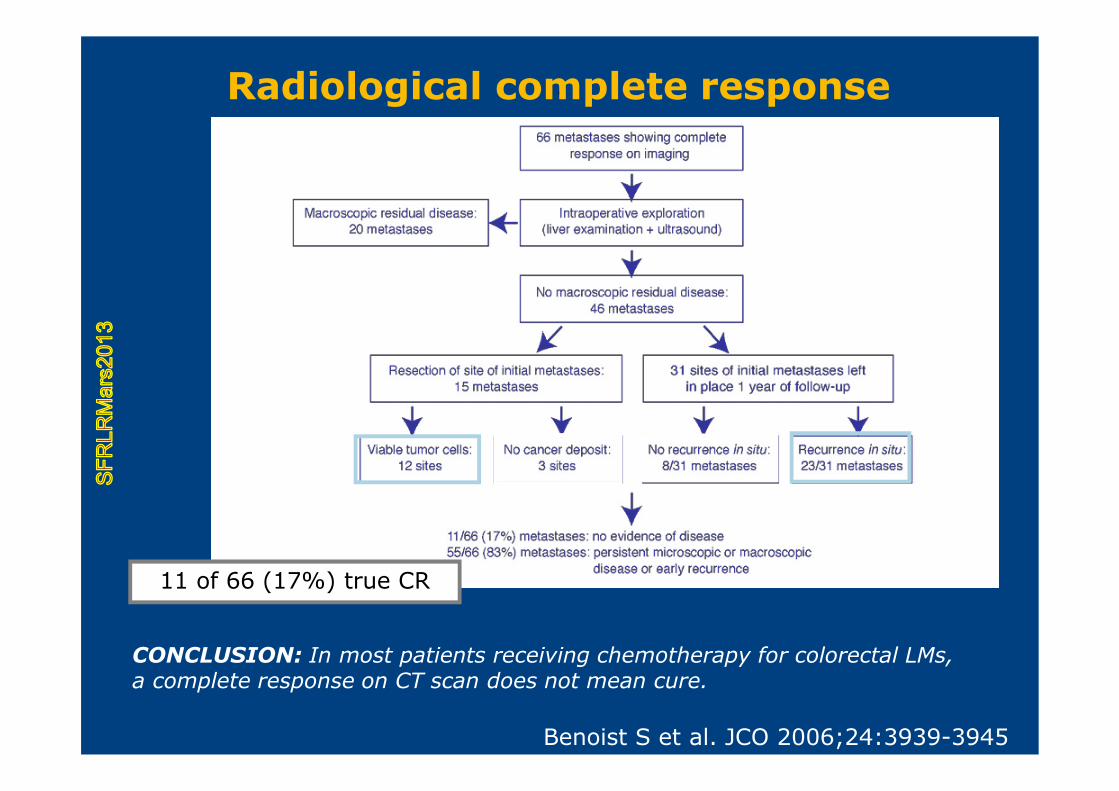
Benoist S et al. JCO 2006;24:3939-3945
11 of 66 (17%) true CR
CONCLUSION: In most patients receiving chemotherapy for colorectal LMs, a complete response on CT scan does not mean cure.
Radiological complete responseS
FRLR
Mar
s201
3
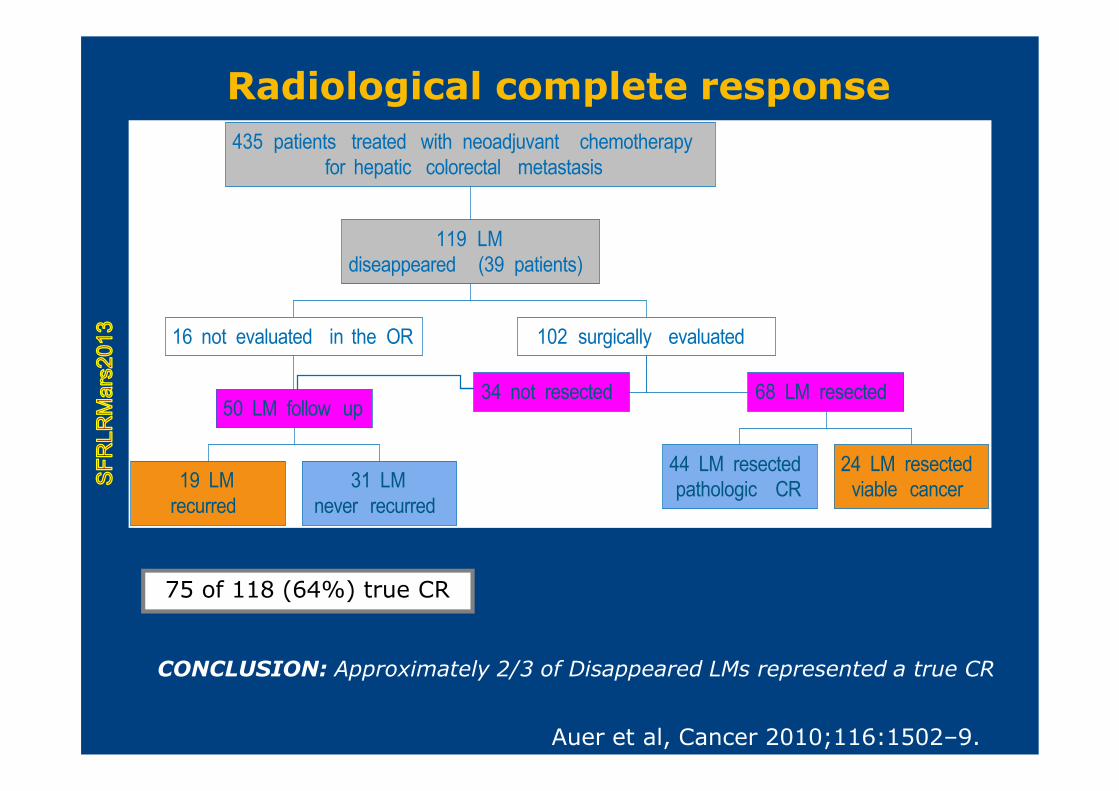
19 LMrecurred
31 LMnever recurred
50 LM follow up
16 not evaluated in the OR
34 not resected
44 LM resectedpathologic CR
24 LM resectedviable cancer
68 LM resected
102 surgically evaluated
119 LMdiseappeared (39 patients)
435 patients treated with neoadjuvant chemotherapyfor hepatic colorectal metastasis
Auer et al, Cancer 2010;116:1502–9.
75 of 118 (64%) true CR
CONCLUSION: Approximately 2/3 of Disappeared LMs represented a true CR
Radiological complete responseS
FRLR
Mar
s201
3
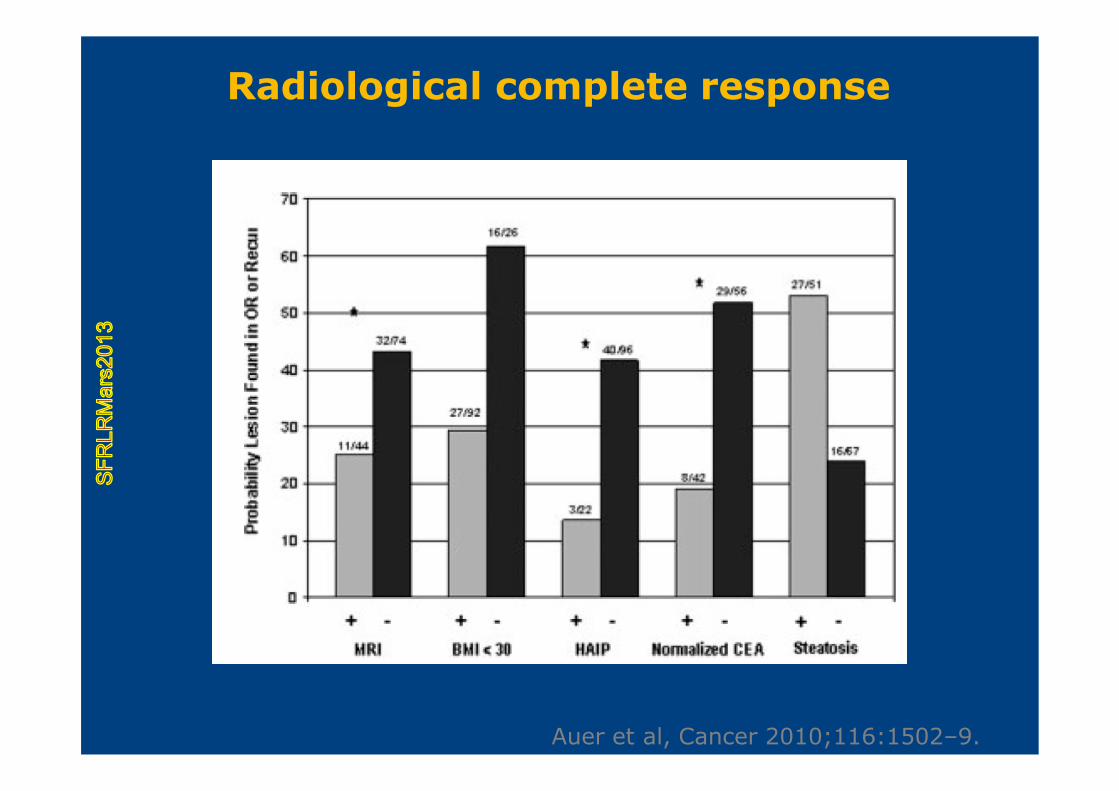
Auer et al, Cancer 2010;116:1502–9.
Radiological complete responseS
FRLR
Mar
s201
3

SFR
LRM
ars2
013







