01 introduction 1-4 02 aims and objective 5 03 reviwe of
TRANSCRIPT

I

II

III
BENEFICIAL CARDIAC ROLE OF BOERHAAVIA DIFFUSA AND
ASPARAGUS RACEMOSUS ON DOXORUBICIN INDUCED
CARDIOTOXICITY IN RATS
Ranjan Kumar Singh1*, Yogita Nirmal
2 and Mobin Ali
3
1*
Assistant Professor, Department of Pharmacology Sanjivani College of
Pharmaceutical Sciences Rajota, Khetri Jhunjhunu Rajasthan India- 333503.
2Assistant Professor, Sanjivani College of Pharmaceutical Sciences Jhunjhunu
Rajasthan- 333503.
3(M.Pharm Scholar) Arya College of Pharmacy, Jaipur, India.
TABLE OF CONTENT
S.NO CONTENT PAGE.NO.
01 INTRODUCTION 1-4
02 AIMS AND OBJECTIVE 5
03 REVIWE OF LITERATURE 06-60
04 MATERIALS AND METHODS 61-65
05 RESULT 66-75
06 DISCUSSION 76-78
07 SUMMARY AND CONCLUSION 79-80
08 REFERENCES 81-85
LIST OF ABBREVIATIONS
ALP - Alkaline Phosphate
ALT - Alanine Aminotransferase
AST - Aspartate Aminotransferase
CAT - Catalase
CNS - Central Nervous System
CHF - Congestive Heart failure
CK - Creatine Kinase
Dox - Doxorubicin
ECG - Electrocardiography
PX - Glutathione Peroxidase
GSH - Reduced Glutathione
LDH -Lactate Dehydrogenase
LPO - Lipid Peroxidase
MDA - Malondialdehyde

IV
NO - Nitric Oxide
ROS - Reactive Oxygen species
RNS - Reactive Nitrogen species
SO - Superoxide
SOD - Superoxide Dismutase
TBARS - Thiobarbituric Acid Reactive Substances
PSD- Punarnava, Satawari, With Doxorubicin.
LIST OF TABLES
S.NO TABLES PAGE. NO.
01 Experimental studies showing the use of antioxidants in the
prevention of the cardio toxic effect of doxorubicin. 33
02 Major differences between B. diffusa and Boerhaavia elegans. 44
03 LIST OF CHEMICALS USED 61
04 LIST OF DRUGS USED 61
05 MORTALITY RATE 66
06 HEART WEIGHT, BODY WEIGHT, ANDHEART / BODY
WEIGHT RATIO. 67
07 Estimation of ALP, CK, and LDH (Normal) 69
08 Estimation of ALP, CK, and LDH (DOX) 69
09 Estimation of ALP, CK, and LDH (PSD) 69
10 Estimation of ALP, CK, and LDH (PD) 69
11 Estimation of ALP, CK, and LDH (SD) 70
12 COMPARETIVE STUDY OF SERUM ENZYMES BIOMARKERS. 70
13 HEART RATE ANALYSIS 74
LIST OF FIGURE
S.NO FIGURE PAGE.NO.
1 Cardiotoxicity causing factors. 22
2 Free radical mechanism causing ROS stress 28
3 General overview of molecular mechanism and biological effects of
Anthracyclines. 31
4 Cardiotoxic and antitumor mechanisms of action of doxorubicin. 52
5 Cardio toxicity mechanisms and targets of doxorubicin. 53
6 ELECTROCARDIOGRAM. 64
7 Body weight of animal model 68
8 Heart weight of animal model 68
9 Graph of ALP of treated rats in myocardial toxicity. 70
10 Graph of CK of treated rats in myocardial toxicity 71
11 Graph of LDH of treated rats in myocardial toxicity. 71
12 NORMAL SALINE (NS) TREATED RAT. 72
13 DOXORUBICIN (DOX) TREATED RAT. 72
14 COMBINATION OD B.DIFFUSA AND ASPERGUS RACEMOSUS AND
DOXORUBICIN (PS+D) TREATED RAT. 73
15 BOARHEEBIA DFFUSA AND DOXORUBICIN (P+D) TREATED RAT. 73
16 ASPERGUS RACEMOSUS AND DOXORUBICIN (S+D) TREATED RAT. 74
17 COMPARISION OF HEART RATE OF DIFFERENT GROUP OF ANIMAL. 75
www.wjpr.net Vol 7, Issue 4, 2018. 1
Introduction
CHAPTER- 1
INTRODUCTION
Healthy human life is always cardinal for human being starting from his birth to the
end of life. The number of disease, minor level to major level, plays a key role in
disturbing the human life. Along with the modernization with the sophistication in the
life, human health faces challenges directly and indirectly from several diseases
resulting sometimes in survival and sometimes in surrender to diseases.[1]
Cancer,
remain the principal cause of death in both developed and developing countries.
Cancer known medically as malignant neoplasm is a broad group of various diseases,
all type of cancar involving unregulated cell growth. In cancer, cells divide and grow
uncontrollably and making malignant tumours, and invade nearby all parts of the
body. There are over lots of types known cancers those afflict human.
Cancer is usually treated with chemotherapy, radiation therapy and surgery. New
anticancer therapies have led to a long life expectancy for many patients; however,
treatment-related comorbities have become an issue for long-term cancer survivors.
Cardiac toxicity is one of the most feared side-effects of anticancer agents so that the
gain in life expectancy due to anticancer therapy might be countered by increased
mortality due to cardiac problems, above all heart failure, but also myocardial
ischaemia, arrhythmias, hypertension, thrombo embolism.[2]
Doxorubicin / Adriamycin (DOX) is a powerful, clinically well established and highly
efficacious anticancer agent. widely used in various neoplastic disease including
breast and oesophageal carcinomas, acute leukimias, solid tumours, kaposi’s sarcoma,
soft tissue sarcoma, Hodkin’s and non Hodkin’s lymphomas. But its clinical
usefulness is still restricted due to its specific toxicities to cardiac tissues. CHF,
Cardiac myopathy and ECG changes were demonstrated after cumulative Dox
administration.
The mechanisms proposed for cardio toxic effects of doxorubicin included
Free radical induced cardiac muscles damage.
Lipid per oxidation
Mitochondria damage
Iron-dependent oxidation damage to macromolecules

www.wjpr.net Vol 7, Issue 4, 2018. 2
Introduction
Inhibition of cardiac coenzyme Q.o
Decrease in cardiac adenylate charge
Although the mechanism underlying the severe toxicity of DOX and other
anthracylines are not fully understood, there is evidence that the drug toxicity may be
ensure through drug free radical formation and subsequent redox cycle with O2
resulting in the generation of reactive oxygen species that SOD anion, OH- radicals
and H2O2. Tissues with less defence antioxidant defences such as heart are
particularly susceptible to injury by DOX induced oxygen radicals because it has
relatively low antioxidant enzymes such as SOD dismutase and Catalase.[3,4,5,6]
Doxorubicin (dox) is a broad-spectrum anticancer drug.[7,8]
Despite its broad
therapeutic effective-ness, the clinical use of DOX is limited by a dose-dependent and
cumulative cardio toxicity.[9,10]
Doxorubicin an anthracycline is well established and
highly efficacious drug in the fight against many kinds of cancer, small cell carcinoma
of the lung and oesophageal carcinoma[11,12]
, but its clinical use is restricted because
its specific cardio toxicity[13]
, congestive heart failure, cardiomyopathy and ECG
changes were demonstrated after cumulative doxorubicin administration.[14]
The
mechanisms proposed for cardio toxic effects of doxorubicin include free radical
induced cardiac muscles injury, peroxidation of lipid, damageing in mitochondria and
redused activity of Na+
K+
ATPase, vasoactive amine release, impairment in
myocardial adrenergic regulation, increase in serum cholesterol, triglyceride and
lower density lipoproteins. Generation of reactive oxygen species like superoxide
anion and hydrogen peroxide by doxorubicin leads to causing impairment of cell
functioning and cytolysis, because of the presence of less developed antioxidant
defence system.[15,16,17,18]
Cellular damage induced by doxorubicin is mediated by the formation of an iron-
anthracycline complex that generates free radicals, which then cause severe damage to
the plasma membrane and interfere with the cytoskeleton structure.[14]
Due to the
presence of less developed antioxidant defence mechanisms, heart is particularly
vulnerable to injury by anthracycline induced reactive oxygen species. Because
liberation of free radicals is central to the mechanism of doxorubicin induced damage
to the myocardium, considerable efforts have been made to use antioxidants and iron
chelators to protect the heart against doxorubicin toxicity.[19]

www.wjpr.net Vol 7, Issue 4, 2018. 3
Introduction
Heart is particularly vulnerable to injury by anthracycline induced reactive oxygen
species. Liberation of free radical is central to the mechanisms of doxorubicin induced
damage to the serum enzyme like lactate dehydrogenise (LDH) and cretaine
phosohokinase (CPK). Endogenous antioxidant deficits have been suggested to play
an important role in doxorubicin induced cardiomyopathy and heart failure.[20,21,22]
Antioxidant compounds have shown protective effects in doxorubicin induced cardio
toxicity without affecting its therapeutic efficacy. There is a growing interest in the
usage of natural antioxidants as a protective strategy against the cardiovascular
problems. The antioxidant compound scavenges the free radicals produced and
protects the heart from oxidative stress.[23]
Herbal medicines are one of the important component and role of preparation of new
pharmaceutical products. A whole range of plant derived dietary supplements, plant
chemicals and pro-vitamins that assist in maintaining good health and combating
disease are now being described as functional parts. The role of medicinal plants in
disease prevention or control has been attributed to antioxidant properties of their
constituents. the main part of plant which are play important role in the protective
effect such as enzymes, proteins vitamins, caretenoides, flavonoids ,and many more
component.[24,25]
Combinations of herbal drugs, antioxidant compounds have shown protective effects
in doxorubicin induced cardiac toxicity without decresing its therapeutic efficacy.
additionally, there is a growing interest in the usage of natural antioxidants as a
protective strategy against the cardiovascular related problems in experiments such as
ischemia reperfusion and doxorubicin induced cardio toxicity.
Extracts of B. diffusa leaves have shown antioxidant and hepatoprotective properties
in pharmacological models. Punarnavine (an alkaloid isolated from of B. diffusa) has
shown some in vitro anticancer, anti-estrogenic, immune-modulators and anti-
amoebic activity (particularly against Entamoeba histolytic). Boerhavia diffusa is a
good source of antioxidants, minrals and vitamins, and may be effective against
arsenic trioxide induced cardio toxicity.[26,33]
Satavari is an important medicinal
hearbs of India. Its medicinal usage has been reported in the I.P and B.P and in
traditional systems of medicine for example; Ayurveda, Unani and Siddha. That’s

www.wjpr.net Vol 7, Issue 4, 2018. 4
Introduction
mainly known for its phytoestrogenic properties. In Ayurvedaic medicine system,
Asparagus racemosus has been shown as a rasayana, the plant has antioxidant,
immunestimulant and cardio protective effect anti-dyspepsia and antitussive
effects.[34]
According to the World Health Organization (WHO) Cancer is a leading cause of
death all over world, accounting for more than seven to eight million people’s deaths
in 2003 worldwide. In the United State, the canters for disease control and prevention
name it the second leading cause of death at more than half million people’s deaths in
2006-2007. Medical treatment continues to evolve in the fight against cancer as newer
and more effective drugs are sought with fewer side effects. Chemotherapy, is the
effective and relatively safe treatment, remains a very important part of cancer
treatment.

www.wjpr.net Vol 7, Issue 4, 2018.
5
Aims and Objectives
CHAPTER- 2
AIMS AND OBJECTIVES
To find out the preventive role of combination of Boerhavia diffusa and
Asparagus racemosus against doxorubicin induced cardio toxicity in albino rats.
Observing the animals of described model for the following parameters:
1. General observation.
2. Mortality.
To evaluate the effect of combination of Boerhavia diffusa and Asparagus
racemosus on various enzyme biomarkers.
1. Estimation of LDH.
2. Estimation of CPK.
3. Estimation of ALP
To study the heart rate analysis of the experimental animals.
To study the body weight, heart weight, and heart and body weight ratio.

www.wjpr.net Vol 7, Issue 4, 2018. 6
Review of Literature
CHAPTER- 3
REVIEW OF LITERATURE
Lipshultz SE et al.,[5]
explained the anthracycline associated cardiotoxicity in
survivors of childhood cancer that Anthracycline chemotherapy can lead to a broad
range of cardiovascular abnormalities, many of which are the progressive and of late
onset. It was concluded that with the increased success of paediatric cancer treatment,
cardiac care providers must a ssume their role in the prevention, diagnosis and
management of treatment related cardiovascular disease.
Pouna Paul et al.,[35]
developed the model of rat isolated perfused heart for the
evaluation of anthracycline cardiotoxicity and its circumvention. The anthracycline
studied were doxorubicin, pirarubicin and daunorubicin. After the all prescribed study
it was concluded that Epirubicin, pirarubicin and daunorubicin were less cardiotoxic
than doxorubicin.
Jensen RA et al.,[36]
evaluated the dose and time dependent effects of dox on the rat.
Electrocardiograph and have related the ECG alterations to cellular transmembrane
potential (TMP) changes and ultrastructural changes in preparations isolated for Dox
treated animals. It was concluded that electrophysiological changes were observed
with Dox in fact represent toxic changes.
Thippeswamy AHM et al.,[37]
investigated the effect of the aqueous extract of
phyllantus niruri against doxorubicin induced myocardial toxicity in rats. The general
observations like LDH, CPK, ALT, SOD, CAT etc were monitored after 3 weeks of
the last dose. It was concluded that the plant extract protects the myocardium from the
toxic effects of doxorubicin.
Swamy AV et al.,[38]
studied the preventive role of curcumin against dox-induced
myocardial toxicity in rats. It was concluded that the curcumin increased the level of
GSH, SOD and CAT & the biochemical and histopathological reports support the
cardioprotective effect of curcumin which could be attributed to antioxidant.
Karim S et al.,[39]
studied the protective effect of losartan, enalapril, vit. A, aspirin,
melatonin and a combination of melatonin and aspirin against doxorubicin induced
cardiotoxicity in rats. After studying the all prescribed parameters it was concluded
www.wjpr.net Vol 7, Issue 4, 2018. 7
Review of Literature
that the combined administration of melatonin and aspirin may offer better protections
as compared to melatonin alone against doxorubicin induced cardiotoxicity.
Shafik AN et al.,[40]
studied the role of protective agents against anthracycline
induced cardiotoxicity and nephrotoxicity by designing the animal model. After
studying all the prescribed parameters it was concluded that co administration of
either cravedilol or nebivolol was able to ameliorate up to almost contradict dox-
induced cardiac damage, glomerular filtration disturbance and renal tubular injure
with upper hand for nebivolol.
Olson DR et al.,[41]
explained that doxorubicin metabolite doxorubicinol causes
doxorubicin cardiotoxicity; that this highly toxic metabolite was produced by cardiac
tissue exposed to doxorubicin suggests that doxorubicinol could accumulate in the
heart and contribute significantly to the chronic cumulative cardiotoxicity of
doxorubicin therapy. It was concluded that the doxorubicin was more potent than
doxorubicinol in inhibiting tumour cell growth in vitro suggests that the cardiotoxicity
of doxorubicin is dissociable from its anticancer activity.
Minnoti G et al.,[42]
discussed about the double edge sword of anthracyclines;
molecular advances and pharmacologic developments in antitumour activity and
cardiotoxicity. It was also explained the recent advances that may serve as a
framework for reappraising the activity and toxicity of anthracyclines on basis of
clinical pharmacology grounds. It was concluded that anthracyclines remain
evergreen drugs with broad cinical indications but have still an improbable
therapeutic index.
Bovelli D et al.,[2]
discussed in his review about the cardiotoxicity of
chemotherapeutic agents radiotherapy related heart disease: ESMO clinical practice
guidelines. After studying all the necessary factors and parameters it was stated that;
although permanent complications tend to occur less frequently under a total dose of
40 mg, it is not a better plan to systematically limit treatment, which may be
insufficient to control the neoplastic disease.
Jaenke RS et al.,[43]
studied the six anthracyclin antibiotics with demonstrated
antitumor activity in human or experimental tumour systems. In this research

www.wjpr.net Vol 7, Issue 4, 2018. 8
Review of Literature
cardiotoxic potential of these compounds were compared and characterized the
myocardial pharmacokinetics in order to provide a possible explanation for
differences in cardiotoxicity. It was concluded that the degree of anthracycline
myocardial toxicity may be directly related to the relative qualitative and quantitative
accumulation of drug metabolites in the myocardium.
Bernard Y et al.,[44]
investigated the cardioprotective potential of synthetic flavagline
analogs FL1–4 in cellular and animal models of doxorubicin-induced cardiotoxicity
and explained the mechanism by which FL3 leads to cardioprotection. It was
concluded that flavaglines may protect other organs than heart against the damaging
effects of cancer chemotherapies.
Raskovic A et al.,[45]
investigated the potential cardioprotective and hepatoprotective
effects of administration of silymarin, affluent in silibinin, at a dose of 50 mg/kg
orally for a time-span of 12 days on doxorubicin induced toxicity in male Wistar rats.
According to physiological, pharmacological, microscopic and biochemical results, it
was confirmed that at the examine dose, silymarin exhibit a shielding influence on the
heart and liver tissue against toxicity induced by doxorubicin.
Rath SK et al.,[46]
explained the antioxidant activity of Rasayana herbs described in
the ayurveda. The available literature was screened and a comprehensive list of herbs
having Rasayana effect and potential anti-ageing effect was drawn. It was concluded
that the Ayurveda, the oldest documented organised system of health care has also
dealt this important health segment under aegis of Rasayana concept and also the
remaining plants should also be investigated for their anti-ageing effect.
Arola OJ et al.,[47]
studied the role of myocardial apoptosis following doxorubicin
administration; rats were exposed to 1.5, 2.5 and 5 mg/kg of. Doxorubicin and
terminated on days 1–7 in groups of five. It was concluded that the acute doxorubicin-
induced cardiotoxicity involves cardiac myocytes apoptosis, a possible preventable
form of cardiac myocytes tissue loss.
Nagy L et al.,[48]
determined a method for detection of doxorubicin-induced
cardiotoxicity by flow mediated vasodilation of the brachial artery. It was suggested
that the alterations in FMD after DOX allows for detection of patients with

www.wjpr.net Vol 7, Issue 4, 2018. 9
Review of Literature
insufficient antioxidant capacity and patients with insuffiecient antioxidant capacity
and patients at a higher risk of DOX-induced cardiotoxicity.
Vikrant A et al.,[6]
discussed about the various cardioprotective plants from ayurveda
and explained about 31 plants of ayurvedic origin with their various chemical
constituents and other biological activities. The review was focused on an overall
outline of plant used in ayurvedic drug for the further scientific investigation.
Koti BC et al.,[20]
determined the cardioprotective effect of lipistat against
doxorubicin induced myocardial toxicity in albino rats by doxorubicin administration
(15mg/kg for 2 weeks) and lipistat as pre-treatment (350mg/kg for 2 weeks) & then
for 2 weeks alternated with doxorubicin. It was concluded that lipid lowering and
antioxidant property of lipistat indicates the cardioprotective property against
doxorubicin induced cardiotoxicity.
Ikeda Y et al.,[50]
Reported that the androgen-androgen receptor (AR) system plays
important roles in cardiac growth and protection from angiotensin-II-induced cardio
remodelling. It was concluded that the androgen-AR system is thought to counteract
Dox-induced cardiotoxicity partly through activation of the AKt pathway and up-
regulation of Tfam to protect cardimyocytes from mitochondrial damage and
apoptosis.
Dolci a et al.,[51]
explained that the cardiotoxicity has a strong impact on patients with
cancer, in clinical and prognostic terms. Early detection was crucial for applying
preventive and supportive therapeutic strategies. The role of cardiac traponin
determination to stratify the cardiotoxicity risk was currently based on strong
evidence clearly suggesting the routine use of that biomarker.
Xin Yen-Fei et al.,[52]
explored the hypothesis that Lycium Barbarum (LB) may be
protective against DOX-induced cardiotoxicity through antioxidant-mediated
mechanisms using male SD rats. The results suggested that LB elicited a typical
cardioprotective effect on DOX-related oxidative stress and also it was concluded
that, in vitro cytotoxic study showed the antitumour activity of DOX was not
compromised by LB and it was possible that LB could be used as a useful adjunct in
combination with DOX chemotherapy.

www.wjpr.net Vol 7, Issue 4, 2018. 10
Review of Literature
Singh MK et al.,[53]
evaluated the combined effect of simvastin (SIM) and
hydroalcoholic seeds extract of Lagenaria Siceraria (H.L.S.S.E.) in doxorubicin
induced cardiotoxicity in Wistar rats. After performing all the necessary steps and
studying the parameters it was concluded that the pre treatment with SIM and HLSSE
may significantly reduced the DOX-induced cardiotoxicity.
CANCER
Cancer is also called malignant neoplasms in medically term. Cancer is a broad group
of different diseases, all types of cancer connecting to uncontroled cell growth. In
cancer, divide and growth of cell is uncontrollably and they form malignant tumours,
and infect nearby parts of the body. The cancer may also infected to more distant parts
of the body by the lymphatic system or by blood. Not all tumors are cancerous.
Tumor do not produce non stop, do not attack neighboring tissues and do not infect by
the body. There are over two hundred different identified cancers that badly affect
humans.[54]
Many things are known to increase the risk of cancer, use taobaccoo, certain infection,
by radiations, less physical exercise and environmental pollutants.[55]
These can
directly damage genes or combine with existing genetic faults within cells to cause
the disease.[56]
Approximately five to ten percent of cancers are entirely hereditary.
Cancer can be detected in a number of ways, including the presence of certain
symtoms and sign, diagnostic tests, or radiography and x-rays. Once a possible cancer
is detected it is diagnosed by various methods. The chances of surviving the disease
vary greatly by the type and location of the cancer and the extent of disease at the start
of treatment. While cancer can affect people any step of life. some type of cancer are
ordinary in Childs, the risk of beginning cancer normally increases with mature. In
2007, 15% people death due to cancer in all over world. Rates are rising as more
people live to an old age and as mass lifestyle changes occur in the developing
world.[57]
Cancer ills the body when injured cells divide uncontrollably to form lump or lots of
tissue called tumors. Except in the case of blood cancer where cancer prohibits normal
blood function by unusual cell distribution in the blood flow. Tumors can develop and
get in the way with the nervous system circulatory systems and digestive system and

www.wjpr.net Vol 7, Issue 4, 2018. 11
Review of Literature
they can release hormones that alter body function. Tumors that stay in one spot and
show limited growth are normally measured to be benign.
More dangerous, or malignant, tumours‟ form when two things occur:
1. A cancerous cell manages to move throughout the body using the blood or
lymphatic system, destroying healthy tissue, this process is called invasion.
2. That cell manages to divide and develop, making new blood vessels to nourish
itself in a process called angiogenesis.
As tumors successfully spreads to other parts of the body and grow, invade and
destroy other well tissues, it is said to have metastasized. This route itself is called
metastasis and the result is a solemn condition that is very hard to treat.
History
Father of morden chemotherapy is Sidney farber. The first use of drugs to treat cancer
was in the early 19th century, although it was not initially intended for that reason. In
the World War I mustred gas was used for chemical warfare agent. And that was
founded to be a potent suppressor production of blood. A similar family of
compounds known as nitrogen mustred were studied at the time of world war second,
at Yale University. It was reasoned that an agent that injured the fast growing WBCs
might have a same effect on cancer. Therefore, in Dec. 1942, many patients with
advanced lymphoma (cancers of WBCs) were the drug injected by intraveinous,
relatively than by breathing the nauseating gas. This development, although
provisional, was extraordinary. At the same time, during a military operation in World
war second, following a German air raidon the Bari, several hundred people were
accidentally exposed to mustard gas, which had been transported there by air force to
prepare for possible retaliation in the event of German use of chemical war. The
survivors were later found to have very low count of WBCs.[54,59]
After world war
second was over and the reports declassified, the experience converge and led
researchers to study for other substances that might have same effects alongside
cancer. The first chemotherapy drug mustine to be develop from this line of research.
Then lots of other medicines have been discovered for cancer treatment, and the drug
development has change into a billion‟s dollar industry, even though the ethics and
restrictions of chemotherapy open by the early researchers still apply.[60]

www.wjpr.net Vol 7, Issue 4, 2018. 12
Review of Literature
Causes of Cancer
Cancer is ultimately the result of cells that non stop develop and not die. Normal cells
in the body go behind on systematic path of development, multidivision and selfdeath.
the Apoptosis is the process is which cell death by a preprogrammed manner, this
type of cell death is called apoptosis and when this process break down, cancer strat to
form. Distinctly normal cells, cancer cells not experience preprogrammatic death and
instead continue to divide and grow. This leads to a group of anomalous cells that
produced out of control.
Classification of cancer
There are five broad groups that are used to classify cancer.
1. Carcinomas are categorized by cells that cover up internal and external parts of
the body. for example Mouth, liver, lymphomas, lung.
2. Sarcomas are characterized by cells that cover up, fatty tissue and tissue, muscle.
3. Lymphomas are cancers that begin in the lymphatic nodes and immune system
tissues.
4. Leukaemias are cancers that begin in the bone marrow and often accumulate in
the bloodstream.
5. Adenomas are cancers that arise in theglandular tissues of the body.
Treatment of cancer
Cancer treatment depends on the type of cancer, the stage of the cancer, age of
patient, health status and additional personal characteristics.in medical science not
single methods for treatment for cancer and patients often is given a mixture of
therapies and soothing care. Treatments of cancer usually following type: surgery,
radiation, chemotherapy, immunotherapy, hormonal therapy, or genetic therapy.
Surgery
Surgery is the oldest treatment process for cancer therapy. That is possible to totally
treat a patient by surgically removing the cancer from the body. This is generally seen
in the exclusion of the testicle, breast and prostate. After the infection has increase,
however, it is almost not possible to eliminate all of the cancer cells. Surgery may
also be helpful to control symptoms such as bowel obstruction or spinal cord
compression.

www.wjpr.net Vol 7, Issue 4, 2018. 13
Review of Literature
Radiation
Radiation treatment, is also called radiotherapy, destroys cancer by focusing high-
frequencys rays on the cancer cells. By the effect of incidend rays, the cancer cells
damage. In the radiotherapy utilization of high-energy, gamma-rays, that are emit
from metals such as radium or high-energy x-rays that are formed in a special
machine. Untimely radiation treatments show harsh side-effects due to the energy
beams would also damage normal, healthy tissue and other part of body, but due to
technologies, improvement that beams can be more perfectly embattled. Radiotherapy
is used as a separate treatment to contract a tumor. And destroy the cancer cells these
methods also associated with leukemia and lymphoma, and it also used in grouping
with other cancer treatments.
Chemotherapy
Chemotherapy use chemicals that interfere with the process of cell division, damaging
proteins, DNA. So that cancer cells destroy. These treatments target any rapidly
dividing cells, but normal cells generally can improve from any chemical-induced
injure while cancer cells cannot. Chemotherapy is normally used to care for cancer
that has increase or metastasized because the medicines travel throughout the entire
body. It is a essential management for some forms of leukemia and lymphoma.
Chemotherapy treatment occurs in intervals so the body has time to repair between
doses. On the other hand, there are still common side effects such as hair loss,
queasiness, weakness and sickness. Grouping therapies often include multiple types of
chemotherapy and chemotherapy combined with other treatment plan.
Immunotherapy
Immunotherapy targets to get the body's immune system to fight with the tumor.
Local immunotherapy injects a treatment into an infected area, for example, to cause
swelling that causes a tumor to reduce in size. General immunotherapy treats the
entire body by administer an agent such as the protein interferon alpha that can
contract tumors. Immunotherapy is able to as well be considered distracted if it
improve cancer-fighting ability by stimulating the whole immune system and it can be
well thought-out targeted if the cure specifically tells the immune system to destroy
cancer cells. These therapies are quite new, but researchers have had success with
treatments with antibodies to the body that reduce the enlargement of breast cancer
www.wjpr.net Vol 7, Issue 4, 2018. 14
Review of Literature
cells. Bone marrow transplantation can also be considered immunotherapy because
the donor's immune cells will often attack the tumor or cancer cells that are present in
the host.
Hormone therapy
A number of cancers have been linked to some types of hormones, most notably
prostate and breast cancer. Hormone treatment is planned to alter hormone production
in the body so that cancer cells stop increasing or are killed completely. in Breast
cancer, hormone therapies often aimed on decresing estrogen levels (a common drug
for this is tamoxifen) and prostate cancer hormone therapies often aim on decreseing
testosterone levels. In addition, some leukemeia and lymph cases can be treated with
the cortisone hormone.
Gene therapy
The aim of gene therapy is to replace injured genes with ones that work to address a
basic reason of cancer: injure to DNA. For example, researchers are work on the
replace the damaged gene that signals cells to stop dividing (P53 gene) with a copy of
a active gene. Other gene based therapies focus on more damaging cancer cell DNA
to the point where the cell self dead. Gene therapy is a very new area and has not until
resulted in any successful treatments.
Chemo is a type of treatment that includes a drug or combination of drugs to care for
cancer. The aim of chemo is to stop and decresed the rate of growth of cancer cells.
Chemotherapy is measured asystemic treatment. That means it may affect your whole
body. Chemo drugs target fast increasing cancer cells, but they can also affect healthy
other cells that grow rapidly. The effect of these drugs on both cells often causes
toxicity. For example:
A number of blood cells that divide quickly can be injured along with cancer cells
during chemo:
o WBCs help protect the body from disease. Low WBCs is known asneutrophils. If
WBCs gets too low you could get a serious infection.
o Red blood cells carry oxygen throughout your body. Low RBCs is known as
anemiea, chest pain and more serious complications.

www.wjpr.net Vol 7, Issue 4, 2018. 15
Review of Literature
o Platelets are structures in the blood that help stop bleeding. A low platelet cell
count is known as thrambocytopenia. A low platelet count can cause bruising and
bleeding.
Hairs that can be affected by chemo, leading to hair loss, also called alopecia.
Cells lining of stomach can also be affected by chemo. This can cause vomiting
and may be associated with nausea.
Chemotherapy is the treatment of cancer with one or more anti-cancer drugs
("chemotherapeutic agents"). Chemotherapy may be given with cure intent or it may
aim to long life. It is often used in conjunction with other cancer treatments. Certain
chemotherapeutic agents also have a role in the treatment of other conditions.
Traditional chemotherapeutic agent‟s act by killing cells that separate rapidly, one of
the main properties of the most cancer cells. That means chemotherapy also harms
cells that divide quickly under normal conditions: these cells present in GIT, in bone
and hair root cells. results in the most common side effects of chemotherapy:
Some newer anticancer drugs are not randomly cytotoxic, but slightly target proteins
that are abnormally expressed in cancer cells and that are necessary for their
development. These treatments are often referred to as distinct from classic
chemotherapy. And often used along established chemotherapeutic agents in
antineoplastic treatment regimen. An older and broader usage of the word
chemotherapy encompassed any chemical treatment of disease (for example,
treatment of infections with antimicrobs agents). On the other hand, this usage has
become archaicsm.
The Term Chemotherapy
The word "Chemotherapy" without a modifier usually refers to the cancer treatment,
but its chronological meaning is broader. The chemotherapy term was traditionally
used for the non-oncological references, such as the use of antibiotics (antibacterial
chemotherapy). Arsphenamine was the first modern chemotherapeutic agent and an
arsenic compound was discovered in 1909 and used to treat syphilis.[61]
This was later
followed by sulfonamides (sulfa drugs) and penicillin. There were some other uses
that have been termed as chemotherapy; such as the treatment of autoimmune diseases
such as polymyositis, multiple sclerosis, dermatomyositis, lupus and rheumatoid
arthritis.

www.wjpr.net Vol 7, Issue 4, 2018. 16
Review of Literature
Principles
Cancer is the uncontrolled growth of the cells which were associated with malignant
behavior: invasion and metastasis. It is thought that the interaction between genetic
susceptibility and environmental toxins causes cancer. Amongst all chemotherapeutic
agents, most of the chemotherapeutic drugs work by impairing cell division i.e.
mitosis, efficiently targeting fast-dividing cells. They are termed as cytotoxic because
these drugs cause damage to cells. There are some drugs which cause cells to undergo
apoptosis (so-called "self-programmed cell death").
Scientists have yet to identify specific features of malignant and immune cells that
would make them uniquely targetable (accepting some recent examples, for instance
the Philadelphia chromosome as embattled by imatinib), which means that other fast-
dividing cells, for example the cells those responsible for hair growth and for
replacement of the intestinal epithelium (lining), are also often affected. Though,
some drugs have a better side effect profile, enabling the doctors to regulate the
treatment regimens to the advantage of patients in certain situations.
As chemotherapy affects cell division, tumors with high growth fractions are more
sensitive to chemotherapy (such as acute myelogenous leukemia and the destructive
lymphomas, including Hodgkin's disease), as a larger fraction of the targeted cells are
undergoes division at any time. The malignancies with slower growth rates respond to
chemotherapy much more diffidently, such as indolent lymphomas.
Drugs affect "younger" tumors (i.e., more differentiated) more efficiently, due to the
mechanisms regulating cell growth are generally still conserved. With the subsequent
generations of tumor cells, delineation is typically vanished, growth becomes less
synchronized and tumors become less approachable to most of chemotherapeutic
agents. Close to the center of some solid tumors, cell division has successfully
finished, which makes them insensible to chemotherapy. There is an additional
problem with solid tumors is that the chemotherapeutic agent often does not reach the
core of the tumour. Radiation therapy (both brachytherapy and teletherapy) and
surgery is the solution for this problem.
Over time, cancer cells become more resistant to chemotherapy treatments. Lately,
scientists have recognized small pumps on the surface of cancer cells that actively
www.wjpr.net Vol 7, Issue 4, 2018. 17
Review of Literature
move chemotherapy from inside the cell to the outside of the cell. Investigation on p-
glycoprotein and some others like chemotherapy efflux pumps is currently in
progress. The medications to restrain the purpose of p-glycoprotein are undergoing
testing as of 2007 to improve the efficacy of chemotherapy.
Treatment schemes
There are a number of strategies in the administration of chemotherapeutic drugs
utilised today. This treatment may be given with a restorative target or it may aim to
prolong life or to palliate indications.
Combined modality chemotherapy is the use of drugs with other cancer treatments,
for example surgery or radiation therapy and most of the cancers are now treated in
the same way. Combinational chemotherapy is a similar exercise that involves
treating a patient with a number of different drugs concurrently. The drugs vary in
their mechanism and side effects. The major benefit is minimising the chances of
resistance developing to any one agent.
In neoadjuvant chemotherapy (preoperative treatment) initial chemotherapy is
designed to shrink the primary tumor, thereby rendering local therapy (surgery or
radiotherapy) less destructive or more effective.
Adjuvant chemotherapy (postoperative treatment) can be used when there is little
confirmation of cancer present; however there is risk of reappearance. This can help
diminish chances of relapse. It is furthermore helpful in killing any cancerous cells
that have spread to other parts of body. This is frequently efficient as the newly
growing tumours are fast-dividing, and so very susceptible.
Palliative chemotherapy is given without curative objective, although simply to
decrease tumor load and increase life expectancy. For these treatments, an improved
toxicity profile is generally expected.
All chemotherapy regimens require that the patient be capable of undergoing the
treatment. Concert position is frequently used as a measure to determine either a
patient can take delivery of chemotherapy, or either dose reduction is necessitated.
Repeated doses have to be administered continuously to reduce the size of tumour
because only a fraction of the cells in a tumour dies with each treatment i.e. fractional

www.wjpr.net Vol 7, Issue 4, 2018. 18
Review of Literature
killing.[62]
Current chemotherapy regimens apply drug treatment in sequences, with
the regularity and extent of treatments limited by toxicity to the patient.[62]
Types
The majority of chemotherapeutic drugs can be divided into anti-metabolites,
alkylating agents, anthracyclines, topoisomerase inhibiting agents, plant alkaloids and
other anti-tumour agents.[62]
All of these drugs affect cell division or interfere with
DNA synthesis and function in some way.
Some newer agents do not directly affect the synthesis of DNA. These include
monoclonal antibodies and the new tyrosine kinase inhibitors, which openly target the
abnormalities of molecule in certain types of cancer (chronic myelogenous leukemia,
gastrointestinal stromal tumours). These are examples of targeted therapies.
In addition, some drugs that modulate tumour cell behaviour without directly
attacking those cells may be used. Hormone treatments fall into this category.[62,63]
Alkylating agents
Alkylating agents are so named because of their ability to alkylate many nucleophilic
functional groups under conditions present in the cells. Carboplatin and Cisplatin, as
well as oxaliplatin, are the alkylating agents. These agents damage cell function by
forming covalent bonds with the carboxyl, amino, phosphate and sulfhydryl, groups in
biologically important molecules.[62]
Other agents are cyclophosphamide, mechlorethamine, ifosfamide, chlorambucil,
Thio-TEPA, Carmustine, Busulfan, Decarbazine, Lomustine, etc.[62]
They work by
chemically modifying a cell's DNA.
Anti-metabolites
Anti-metabolites masquerade as purines such as mercaptopurine, azathioprine or
pyrimidines; which becomes the building-blocks of DNA. They competitively inhibit
utilization of the normal substrate or get themselves incorporated forming
dysfunctional macromolecules. They prevent these substances from becoming
incorporated into DNA during the "S" phase of the cell cycle of cell growth, stopping
normal progress and division of the cell and also they affect the synthesis of RNA.
Due to their effectiveness, these drugs are the most widely used cytostatics.
www.wjpr.net Vol 7, Issue 4, 2018. 19
Review of Literature
Some anti metabolites are as
Methotraxate (Folate antagonist),
Mercapturine and thioguanine, azathiorine, fludarabine (Purine antagonist),
Fluorouracil, Cytarbine (Pyrimidine antagonist).
Plant alkaloids and terpenoids
These alkaloids are derived from plants and block cell division by avoiding
microtubule function. Microtubules are fundamental for cell division and devoid of
them, cell division cannot occur. The key examples are vinca alkaloids and taxanes.
Vinca alkaloids
Vinca alkaloids bind to specific sites of tubulin, reducing the assembly of tubulin into
microtubules (M phase of the cell cycle). The chromosomes fail to move apart during
mitosis: metaphase apprehends occurs. They act in mitotic phase of cell cycle. They
are derived from the Madagascar periwinkle, Catharanthus roseus (formerly known as
Vinca rosea). These include:
Vincristine
Vinblastine
Vinorelbine
Vindesine
Podophyllotoxin
Podophyllotoxin is a plant-derived compound that is said to help with digestion as
well as used to produce the two other cytostatic drugs, teniposide and etoposide. They
avoid the cell from entering the G1 phase (the start of DNA replication) and the
replication of DNA (the S phase of cell cycle). The actual mechanism of its action is
not however known.
The substance has been primarily obtained from the American Mayapple i.e.
Podophyllum peltatum. Recently it has been investigated that an uncommon
Himalayan Mayapple i.e. Podophyllum hexandrum contains it in a much larger
amount however, as the plant is rare, its supply is limited. Studies have to be
conducted to isolate the genes involved in the production of substances, so that it
could be acquired recombinantly.

www.wjpr.net Vol 7, Issue 4, 2018. 20
Review of Literature
Taxanes
The prototype taxane is the natural product i.e. paclitaxel originally recognized as
Taxol and first obtained from the bark of the Pacific Yew tree. The semi-synthetic
analogue of paclitaxel is Docetaxel. Taxanes increase the stability of the
microtubules, preventing the separation of the chromosomes during anaphase.
Examples of Taxanes are as
Paclitaxel
Docetaxel
Topoisomerase inhibitors
Topoisomerases are essential enzymes that maintain the topology of the DNA.
Reduction of type I or type II topoisomerases interferes with both transcription and
replication of DNA by upsetting proper DNA super coiling.
Some type I topoisomerase inhibitors are as irinotecan, camptothecins and
topotecan.
Examples of type II inhibitors are as etoposide, amsacrine, etoposide, teniposide
and phosphate. These are the semisynthetic derivatives of the
epipodophyllotoxins, substances that are naturally occurring in the root of
American Mayapple.
Cytotoxic antibiotics
These include
actinomycin
anthracyclines
doxorubicin
daunorubicin
valrubicin
idarubicin
epirubicin, which also inhibit topoisomerase II
other cytotoxic antibiotics
Bleomycin: The Bleomycin act in a exclusive way through oxidation of a DNA-
bleomycin- Fe (II) complex and producing the free radicals, which cause damage
and chromosomal aberrations.

www.wjpr.net Vol 7, Issue 4, 2018. 21
Review of Literature
plicamycin
mitomycin
Anthracyclines
Anthracyclines are well established as highly efficacious antineoplastic agents for
various hemopoietic and solid tumours. A clear dose-response relation for
anthracyclines in several curative chemotherapeutic regimens has been revealed. A
decreased dose causes consequences in the inferior survival and remission rates.
However, the cardio toxicity of their agents which has been recognized for more than
20 years continues to limit their therapeutic potential and threaten the cardiac
functions of many patients with cancer.[64]
Historical perspective
Daunorubicin the frist anthracyclin antibiotic to be used and it was isolated in 1963 in
Italy from culture method of streptomyces peucetius. It is showed demonstrable
activity against a wider range of tumours in children, including soft tissue and bone
sarcomas and lymphomas, as well as lymphoblastic and myeloid leukaemia. Early
phase 1 trial involved patients with widespread disease and reports of cardiotoxicity
could only uncertainly attribute toxicity to the drug rather than the disease. With
increasing use of anthracycline, however, it becomes apparent that daunorubicin and
doxorubicin were directly cardiotoxicity in children and adult.
Epidemiology
There is wide variation in the reported frequency of both clinical subclinical
cardiotoxicity. There is a relatively low rate of early clinical cardio toxicity, since
only 1.6% of all children treated with anthracyclines have cardio toxicity effects.[65]
The prevalence of the subclinical cardiac damage has been reported to be more than
57% at a median of 6.4 years after the treatment amongst the survivors of childhood
cancers[66]
and the incidence of clinical heart failure as high as 16%, 0.9 to 4.8 years
after treatment.[67]
Distinctions in study of the population, treatment protocols and
extent of follow up could account for this wide variability. The risk of cardio toxic
effect occurring about 15 to 20 year after treatment with cumulative doses
anthracycline of 400 mg/m2 is estimated to be approximate 5% (madam). in the
normal population risk of mortality from cardiac related events is 8 times higher for
long term survivors.

www.wjpr.net Vol 7, Issue 4, 2018. 22
Review of Literature
Pathology in biopsy of end myocardial layer of heart with treated with
anthracyclines, its shows following symptoms
Myofibril loss
Sarcoplasmic retiuculam inflammation,
Mitochondrial inflammation,
Cytoplasmic vacuolisation,
Wide spread damage with necrosis of myocytes.
The number of myocytes present in the adult heart. Myocytes lost by necrosis are not
replaced, but the remaining myocytes increased in size to compensate and there is also
increased in the amount of interesting tissue and fibrosis. The change seen in children
and adults are the same. For children sustaining anthracyclines cardio toxicity,
myocytes loss means the left ventricular wall becomes relatively thin and particularly
fails to keep pace with pubertal or growth hormones induced growth spurts,
occasionally causing subclinical damage to become clinically overt at this time.[68]
Cardiotoxicity
Figure 3.1: Cardiotoxicity causing factors.

www.wjpr.net Vol 7, Issue 4, 2018. 23
Review of Literature
Cardio toxicity is a condition when damage to the heart muscle occurs. Because of
cardiotoxicity, the heart may not be capable to pump the blood throughout whole of
the body and this may be due to chemotherapeutic drugs, or other medications which
may be taking to control the disease. Cardiotoxicity, if severe or harsh, could lead to
cardiomyopathy.
Cardiomyopathy
Is often a result of treatments with chemotherapeutic medications, or may be grounds
by a group of diseases or disorders, causes heart muscles damage. Heart muscle injury
may results in a disturbance of the heart's pumping action and consequent heart
failure.
Anthracyclines are tarnished for causing cardiotoxicity. It may be caused because of
many factors, such as interference with the ryanodine receptors of the sarcoplasmic
reticulum in the heart muscle cells, because of free radical formation in the heart, or
because of development of metabolic products of the anthracycline in the heart.
Cardiotoxicity frequently presents as ECG changes (especially change in the
frequency of QRS complex) and also as arrhythmias, or as a cardiomyopathy causing
to heart failure. This caused cardiotoxicity is associated with a patient's cumulative
lifetime dose. During the treatment, patient's lifetime dose is calculated and
anthracycline treatment is frequently stopped (or at least re-evaluated by the
oncologist) upon reaching the maximum cumulative dose of the particular
anthracycline.[69]
There exist facts that the results of cardiotoxicity increases in long-term survivors,
from 2% after 2 years to 5% after 15 years.[70]
Pathophysiology of Anthracycline-induced Cardio toxicity
Cardio-toxicity is subdivided into three categories based on the time of onset: acute,
early onset chronic progressive cardio-myopathy and late-onset progressive cardio-
myopathy.[71]
Acute anthracycline-induced cardio-toxicity
Acute anthracycline-induced cardiotoxicity occurs in less than 1% of childhood
cancer patients and is defined as a severe, but temporary decrease in LV contractility

www.wjpr.net Vol 7, Issue 4, 2018. 24
Review of Literature
seen immediately after anthracycline administration.[72]
Symptoms usually occur
within 1 week of treatment and may range from arrhythmias and electrocardiographic
abnormalities to myocarditis-pericarditis syndrome or congestive heart failure.[73]
Sinus tachycardia, possibly as a result of autonomic dysfunction, an arrhythmia, but
decrease in the QRS amplitude, causes prolongation in QTc interval and also results
in nonspecific ST segment and T-wave changes.[65]
Serum cardiac biomarker
elevations are considerably more common during this window.[77]
Discontinuing the therapy generally results in reduction in the symptoms initially,
although in many patients, particularly who received a greater cumulative
anthracycline dose, shows the permanent cardiac damage and are more likely to
develop late signs of cardiotoxicity.[65]
Early Onset of Anthracycline-induced Cardiotoxicity
Anthracycline-induced cardiotoxicity that develops during therapy or within the first
year after treatment and persists is referred to as early onset chronic progressive
cardiotoxicity and is observed in 1.6%[74]
to 2.1%[66]
of all anthracycline treated
children. In near the beginning onset of cardiotoxicity occurs, LV contractility is
reduced, most probably from anthracycline-induced damage or death of
cardiomyocytes.[65,66,71]
In addition to the positive correlation between higher cumulative anthracycline doses
and the incidence of the cardiotoxicity and the other factors are associated with a
distinctly increased risk of developing early onset anthracycline induced
cardiotoxicity. These factors include trisomy, black race and female sex, additionally
to concomitant mediastinal irradiation, or treatment with amsacrine.[65,75]
Late onset of Anthracycline induced Cardiotoxicity
Cardiotoxicity presenting at least a year after the completion of anthracycline therapy
is classified as late-onset cardiotoxicity and typically follows a chronic, progressive
course.[76,78]
Lipshultz et al., investigated that 6 years after end of anthracycline
treatment approximately 65% of survivors of childhood cancer have detectable left
ventricular abnormalities, either structural or functional.[76,77]

www.wjpr.net Vol 7, Issue 4, 2018. 25
Review of Literature
Late-onset anthracycline-induced cardiac failure may evolve from the inability of the
remaining cardiomyocytes to meet the demands of normal growth or other cardiac
stresses, such as pregnancy or acute viral infection.[79,80]
The resulting
cardiomyopathy may depend on the age during which the survivor was treated with
anthracyclines.[76]
Treatment before the completion of physiological growth and
development would leave fewer cardiomyocytes available for compensatory
hypertrophic remodeling of the LV.
The Clinical Presentations of Cardiotoxicity
Interestingly, although adult cancer survivors who experience cardiomyopathy as a
result of their exposure to anthracyclines generally have dilated cardiomyopathic
disease and childhood cancer survivors frequently present with a combination of both
dilated and restrictive cardiomyopathy.[72,81]
The type of cardiomyopathy that
develops in these young patients is influenced by whether they also received radiation
treatment that includes the heart. In Dilated cardiomyopathy, LV systolic dysfunction
occurs and which is more common among patients who received only anthracyclines,
but cardiomyopathy may developed from exposure to both anthracyclines and cardiac
radiation; may also occur in the later stages of patients. Initially, the patients who
taking both the cardiac radiation and also the anthracyclines present with restrictive
cardiomyopathy and therefore diastolic dysfunction, which much may afterwards
developed to systolic dysfunction.[79,82,83]
Risk Factors for Developing the Anthracycline induced Cardiotoxicity
The risk of developing clinical cardiotoxicity in both children and adults coincides
with increases in the cumulative dose of anthracycline.[81,84]
While avoiding the use of
anthracyclines in the treatment of certain cancers would be the most adequate strategy
to prevent cardiotoxicity[85]
this may negatively influence tumor response and
ultimately the survivals. The most severe cardiac discrepancy associated with
anthracycline toxicity occurs at the highest cumulative doses. Though, lower doses
are not totally safe either, as the symptoms of cardiotoxicity occurs even been
reported in patients receiving only low doses of anthracyclines.[78]
This variability in
susceptibility may be partially explained by genetic polymorphisms of certain genes,
although a few numbers of studies have discoverd this possibility and have reported
conflicting results.[84,86,87,88]

www.wjpr.net Vol 7, Issue 4, 2018. 26
Review of Literature
One study found that children with a cumulative anthracycline dose greater than 550
mg/m2 were more than five-times as likely to occurrence of cardiotoxicity, than the
children who received low cumulative doses[65]
van Dalen et al. reported that the
estimated incidence of developing anthracycline-induced clinical heart failure
increased with both time since treatment and cumulative anthracycline dose (5.5% at
20 years after the start of anthracycline therapy if treated with a cumulative dose less
than 300 mg/m2 and 9.8% if treated with a cumulative dose exceeding 300 mg/m
2),
over a mean of 8.5 years (median: 7.1 years; range: 0.01–28.4 years).[89]
The
incidence of anthracycline-induced clinical heart failure in this cohort was 2.5% and a
cumulative anthracycline dose of 300 mg/m2 or more was the only independent risk
factor (relative risk [RR]: 8.0). The authors concluded that 10% of children receiving
a cumulative anthracycline dose of 300 mg/m2 or more will eventually experience
anthracycline-induced clinical heart failure.
Lipshultz et al. reported that a higher cumulative anthracycline dose was associated
with worsened LV structure and function with regard to both afterload and
contractility.[76]
More precisely, several studies have noted that cardiac dysfunction
becomes more noticeable in patients who received a cumulative anthracycline dose
that exceeds approximately 250 mg/m2.[90,91]
Additionally, a higher dose rate,
previously treatment with anthracyclines, longer action, younger age at diagnosis and
radiation therapy involving the heart have all been identified as risk factors for
developing late cardiotoxicity. Another risk factor for developing anthracycline-
induced clinical heart failure in children is being female. For the girls, this risk is
approximately increased by 4 times as great as it is for male childhood cancer
survivors treated with anthracyclines.[92]
Lipshultz et al. reported that LV contractility
of female childhood cancer survivors 8 years after completing doxorubicin treatment
was significantly worse than that of their male counterparts. A few explanations have
been posited for this difference. The Doxorubicin clearance is lower in those patients
with higher BMI, which usually associates with increases in the percentage of body
fat.[74]
Girls, on average, have a larger body-fat: lean-mass ratio than the males, which
possibly will increase the amount of anthracyclines and stored in adipose tissue,
consequently exposing nonadipose tissues to higher concentrations of anthracyclines
for a longer period of time.[75,93]
www.wjpr.net Vol 7, Issue 4, 2018. 27
Review of Literature
It is important to note that not all of the presented risk factors are identified by all of
the studies that considered them. Though, differences in the study proposed and
sample size between these studies may partially explain the different results. For
instance, some studies only observed the high-risk subgroup of the survivors, or more
aggressive form of the cancer, a priori. These children are liable to take delivery of
higher doses of doxorubicin in order to treat the cancer more aggressively, while the
standard risk children do not get such high doses.[75,76,78]
Mechanisms of the Anthracycline induced Cardiotoxicity
Despite more than three decades of the use, it is yet unclear actually that how
anthracyclines exert their chemotherapeutic activity and induce the cardiotoxic
changes. Antineoplastic activities of the doxorubicin can be derived from the
inhibition of topoisomerase II, free-radical generation, activation of signalling
pathways, DNA intercalation and binding and apoptosis. Similarly, causes of
anthracycline-induced cardiotoxicity appear to be multifactorial. A significant
component may cause production of free radicals and the presence of the redox
related damage, which happen through both the enzymatic and the nonenzymatic
pathways and result in the accumulation of iron. Anthracycline-generated free radicals
induce lipid peroxidation, which ultimately produces membrane damage. In addition,
mitochondrial damage, increased Ca2+
current along with inhibition of sarcoplasmic
reticulum function and decreased activity of Na, K-ATPase, have all been implicated
in doxorubicin-induced cardiotoxicity. The down regulation of myocardial TNF-α and
doxorubicin binding to bivalent cations (Ca2+
, Mg2+
, Cu2+
and Zn2+
) may also be
contributively.
Mechanism of the Anthracycline toxicity in Cardiomyocyte
Anthracyclines enter cardiomyocytes by passive diffusion and stimulate the
production of free radicals, which leads to cell damage. The Anthracyclines also
directly and indirectly inhibit the gene transcription; also inhibit the mitochondrial
functioning and also energy production within the cell. Compared with other organs,
the heart is especially susceptible to the anthracycline induced damage, in part, due to
anthracyclines high affinity for the cardiolipin. Cardiolipin is a unique mitochondrial
phospholipids involved in various stages of mitochondrial membrane dynamics and
the mitochondrial apoptotic process. During the initial stages of apoptosis, apparently

www.wjpr.net Vol 7, Issue 4, 2018. 28
Review of Literature
in synchronization with death receptor stimulation and the generation of reactive
oxygen species (ROS) cardiolipin can become peroxidised. Peroxidation of
cardiolipin can interfere with the localization of heme iron of cytochrome C and
results in its release and also the release of additional apoptogenic factors, from
mitochondria. While it appears that peroxidation of cardiolipin plays a critical role in
releasing cytochrome C from the inner part of mitochondrial membrane, the
cytochrome C itself be able to catalyze cardiolipin peroxidation. Cardiolipin's cellular
role is multifaceted and further investigation into its contribution to apoptosis is
warranted.
Anthracycline exposure activates both ROS-dependent and ROS-independent
pathways that may ultimately lead to a sizeable loss of cardiomyocytes through
necrosis and apoptosis. Other types of cell death, including senescence and the
autophagy, may also put in to the anthracycline induced cardiomyopathy. Myofibrillar
loss and cytoplasmic vacuolization, can be caused by the dilation of the sarcoplasmic
reticulum in the myocardial cells, these are the most common chronological findings
in patients with anthracycline-induced cardiomyopathy. The degree of cellular
damage corresponds with the cumulative anthracycline dose administered. The
primary compensatory mechanism for anthracycline-induced cardiomyocyte loss is
the cardiomyocyte hypertrophy, which finally results in a series of physiological
changes that lead to the development of the cardiomyopathy. These types of changes
include the decrease in left ventricular (LV) contractility, the thinning of the LV wall,
increase in LV afterload, fibrosis all of which are cause to reduced LV function.[24]
Figure 3.2: Free radical mechanism causing ROS stress.

www.wjpr.net Vol 7, Issue 4, 2018. 29
Review of Literature
In addition, the heart's relative lack of strong antioxidant defence mechanisms and
high rate of oxidative metabolism make it particularly vulnerable to damage by iron
and free radicals, which consecutively, can increase the permeability of the cell
membrane. Substantial experimental data supports the involvement of iron in
anthracycline-induced cardiotoxicity, which includes the ability of an iron chelator
and dexrazoxane, to alleviate anthracycline-induced cardiotoxicity. In this
investigation of Cascales et al. was investigated that whether anthracyclines increases
the iron concentration in the heart and if it done then whether the HFE genotype
helping to regulate iron deposition. They retrospectively examined the cardiac iron
concentrations, HFE genotype and the cardiac events in 97 consecutive necroscopies
from adults with hematological and the solid neoplasms. From these, about 48
patients had been treated with anthracyclines and the other 49 patients had been
received either some other type of the chemotherapy (24 patients) or some
nonchemotherapeutic form of therapy (25 patients) and were used as the controls.
When the tests compared with the control group, the cumulative doxorubicin dose
greater than 200 mg/m2 was associated with increased cardiac concentrations of iron
(490 vs 240 µg/g; p = 0.01), regardless of the patient's transfusion history or level of
iron into the liver. Some mutated haplotypes were associated with greater iron
deposition (282C/63D, p = 0.049; 282Y/63H, p = 0.03) and the haplotype C282Y-
Y/H63D-H actually increased cardiac iron accumulation through its interactions with
anthracyclines. The investigators from all studies stated that the HFE helps regulate
iron accumulation after exposure to anthracyclines and that this iron accumulation is
independent of a patient's systemic iron load.
Other possible contributors to anthracycline-induced cardiotoxicity include reduced
expression of mRNA encoding for the sarcoplasmic reticulum Ca2+
-ATPase, which
results in diminished cardiac contractility and transcriptional changes in intracellular
cardiomyocyte ATP production. In addition, prolonged exposure to anthracyclines
may also lead to DNA damage resulting from depressed cardiac glutathione
peroxidase (GSHPx) activity and respiratory chain defects. Respiratory chain defects
are associated with the production of the free radicals and also which can continue to
produce even after the anthracycline treatment, ultimately causal to late anthracycline
induced cardiomyopathy. This production of radicals may also release cytochrome C
from mitochondria, ultimately leading to apoptosis.[9]

www.wjpr.net Vol 7, Issue 4, 2018. 30
Review of Literature
Focusing on liver and cardiac tissue, in his study Doroshow et al. determined the
alterations in concentrations of catalase, superoxide dismutase and GSHPx (all
enzymes noted for their ability to detoxify activated oxygen) in response to treatment
with doxorubicin administered through intraperitoneal injection. Experiments in
murine models suggested that the GSHPx in cardiac tissue was the selenium
dependent. The superoxidase and Catalase concentrations in the cardiac tissue were
<0.6% and about 27% of that found in the liver tissue, correspondingly, but the
GSHPx concentrations were similar in the both types of tissues. Though, after the 6
weeks of selenium reduction, the GSHPx activity was decreased to less than 20% of
the baseline and in this selenium depleted condition, marked doxorubicin induced
toxicity found in animals receiving only 15 mg/kg intraperitoneally. Distinctly,
neither the the level of cardiac superoxide dismutase, nor the concentrations of
hepatic superoxide dismutase or GSHPx were affected at the same dose. From all the
studies the authors stated that the selenium dependent GSHPx, collectively with
superoxide dismutase, to a great extent helps detoxify ROS in the cardiac tissues and
that the doxorubicin or diet induced reduction of selenium would impair the heart's
ability to efficiently dispose of lipid peroxides and hydrogen peroxide.
Although redox-induced damage is likely involved in anthracycline-induced
cardiotoxicity, a number of verification proposed that it is not only the mechanism.
Numerous studies of a variety of redox inhibitors, or the ROS scavengers, given
concurrently with anthracycline treatments have found no statistically significant
levels of the cardioprotection. The incapability of these agents to improve
anthracycline-generated cardiotoxic damage does not substantiate redox-induced
damage as a stand-alone cause of anthracycline-induced cardiotoxicity.[107]
Pointon et al. compared the cardio-toxicity induced by doxorubicin with that induced
by 2,3-dimethoxy-1,4-naphtoquinone (DMNQ) in murine models to investigate the
adequacy of the redox hypothesis of anthraxcycline-induced cardio-toxicity.[107]
DMNQ has limited ability to stop DNA replication or gene transcription but it is a
superior redox cycling agent than doxorubicin (-183 mV compared with doxorubicin's
redox potential of -328 mV). The investigators postulated that if redox damage was
the primary cause of anthracycline induced cardiotoxicity, then the DMNQ should
cause considerably more cardiac damage than the doxorubicin. Acute results to

www.wjpr.net Vol 7, Issue 4, 2018. 31
Review of Literature
DMNQ or doxorubicin introduction proposed that anthracycline-induced
cardiotoxicity is not primarily a result of general redox stress, however somewhat
from the reduction of the electron transport chain in the mitochondria. In his study,
Pointon et al. stated similar responses in a chronic revelation murine model, although
they did not contain the supporting data.
General overview
Figure 3.3: General overview of molecular mechanism and biological effects of
Anthracyclines.[52]
From the analysis of above figure, it seems that some of these interactions are directly
responsible for the mitochondrial dysfunctions, other are consequence of a general
modification of these drugs in a cellular system. As shown in the fig. 3.3 overview in
mainly four factors are responsible for the mitochondrial dysfunction.
a. Anthracycline determine a release of some mitochondrial enzyme, probable
through membrane disruption. The release of cytochrome cis the beginning of a
cascade that‟s lead to the cell apoptosis.
b. The high affinity of anthracyclines to lipids leads to disorder to itochondrial
membrane and to an indirect inhibition of lipid bound enzymes.
c. A direct inhibition of mitochondrial enzymes could be demonstrated only in the
case of cytochrome c oxidase.
d. Production of free radicals, in particular in mitochondria enzyme systems, lead to
a huge number of cells injure, as calcium release, as lipid peroxidation and
oxidative stress in general. This ability can be enhanced in the presence of metal
ion able to form reactive complex with the Anthracyclines.
www.wjpr.net Vol 7, Issue 4, 2018. 32
Review of Literature
Strategies to reduce the cardio toxicity of Anthracyclines[12]
In the treatment of chemotherapy, anthracyclines are use over 40 year and depict
intensive research efforts; no significant progress has been made in improving their
cardiac safety. It is presumed that the postulated cardio toxic mechanisms in
anthracyclines are not the same effects as those operating in tomour toxicity. This
allows hopes that it might be possible to achieve cardio protection without loss of
antineoplastic efficacy.
Effort in this direction as so far focused on
a. Reducing the total cumulative doses.
b. Co therapy with protective agents.
c. Changing the chemical structure of the anthracyclines moiety.
d. Encapsulation of anthracycline in liposomes.
e. Development of new safe derivative.
Reducing the total cumulative doses
Chronic cardiotoxicity and heart failure may any time competition of doses of
anthracyclines drugs and occurs more frequently in patients given cumulative doses of
doxorubicin 550mg/m2.[12]
A lower doses limit would reduce the incidence of serious
cardiotoxicity, but these strategies would deny treatment with a potent and effective
agent to many who would tolerate much higher doses and potentially benefits from its
maximum antineoplastic therapeutic effects and the present approach is to administer
the Dox up to point beyond which further therapy would result in cardiotoxicity. This
required an ability to monitor for cardio toxicity and the safety the cumulative doses
of doxorubicin.[22]
By this approach the significant reduction in the incidence severe
doxorubicin cardio toxicity has been achieved.
Co therapy with protective agents
An anthracyclines have very potent anti-tumour effects and their extensive use will
persist until effective and safer alternative have been identified. An extensive array of
compounds has been evaluative in various experimental models for their potential to
reduced dox cardio toxicity. On the basis of a perceived ability to modulated some of
the biochemical alternations that accompany dox administration. Most research in this
area has focused on antioxidant agent or iron chelotors. Antioxidant enzymes such as

www.wjpr.net Vol 7, Issue 4, 2018. 33
Review of Literature
SOD or Catalases, Vitamin E, lycopene, sulfer containing antioxidents are shown to
protect against the cardio toxicity of anthracyclines in several experimental modals.
Table 3.1: Experimental studies showing the use of antioxidants in the
prevention of the cardio toxic effect of doxorubicin.
ANTIOXIDANT MODEL RESULT
Vit.E Rat
Abolition of ST segment
evaluation, reduction of cardiac
enzymes. (CPK, LDH)[23]
Vit. E and N-acetyl
cysteine Rat
Protection to word lipid tissue
cardiac and hepatic paroxidation.
Protection of action potentials
and cardiac activity.[24]
N-(2-mercapto-
propionylglycine) Rat
Protection towards lipid tissue
cardiac peroxidation[25]
Lyopene Rat
Reduction of cardiac tissue lipid
peroxidetion and cardiac enzyme
release.[26]
Gluthione Rat
Protection towards hepatic and
cardiac lipid tissue peroxidation.
And cardiac enzymes release.
Reduction of cardiac histological
ultreation.[27,28]
Sod,catalase Rat
Prevention of dox-induced
reduction of cardiac myocytes
contractility.[29]
Changing in the chemical structure of the anthracyclines moiety[67]
Anthracyclines determine a release of some mitochondrial enzymes, propbly through
the membrane distruction. The discharge of cytochrome C is the commencement
(starting) of a cascade that‟s lead to cell apoptosis. Slightly structural change can
determine a completely changed reactivity of these drugs with enzymes or metal ions
and therefore change the ability to produced free redicals. These changes can also lead
to change affinity constant to certain and lipophlic characters.
The encapsulation of anthracyclines in liposomes
The Liposomal encapsulated anthracyclines are used in preclinical studies and result
in a different pharmacokinetics profiles. pegylated liposome‟s used for clinical
applications(caetly, doxil) resulted in longer circulation times and a higher anti-tumor
activity with respective to the free drug. The changed pharmacokinitics and
distribution of liposomal encapsulated anthracyclines allow rising the administrative
www.wjpr.net Vol 7, Issue 4, 2018. 34
Review of Literature
doses in chemotherapy without increasing the cardio toxicity. The resulting higher
cumulative drug concentrations, led to an increase of other dose dependent side
effects, that‟s less dramatic with respect to the cardiomyopathy but also therapy
restraining. There is one of the main serious problems during the anthracycline
chemotherapy is PPE. These ulcer active cutaneous lesions on hand and feet strongly
through to be related to a free radical induced damage of endothelial cells and
keratinocytes. It is important to note this severe side effect occurs also during the
administration of the free drug and is not related to the concomitant presence of the
liposome. The knowledge of the affinity of the chemotherapies to certain lipids, i.e.
cardiolipin, in the preparation formulation of the liposomes could be exploited in
order to avoid the intreaction with mitochondrial membrane. The ability to generate
free radicals scavengers inside the liposome.
Development of new safe derivatives
Many attempts have been made to be finding new anthracyclines with lower toxicity
than daunorubicin and doxorubicin. Thousands of analogous have been synthesised
and tested, but few have found their way into clinical use. Among these so called
second generation anthracyclines are epribucin and idarrubucin.
Epribucin is the semi synthetic derivative of doxorubicin with a similar mechanisms
and scope of efficacy to its mother component. epirubicin can be given at a higher
cumulative doses. Its shows no reduction in toxicity, compare to doxorubicin, when
given therapeutically equal doses. Despite an improvement in therupatic index, the
cardiac risk remains. The daunorubicin derivative idrabucine has a wide spectrum of
efficacy and can give orally. However, dispute some promising finding any reabile
improvement in cardiac safety is in dought.[131]
PLANT PROFILE
Introduction
It is been recorded in history that herbal Medicine have been used as form of
treatment for the pain. The exploration of the chemical contents from herbs,
pharmacological action and phyto-chemical screening would provide the basis for
producing the new lead molecules in strategic favour of herbal product drug
discovery. The objective of researchers is the discovery and development of isolating
a new less toxic, active and efficient molecule for systemic activities. The biologically

www.wjpr.net Vol 7, Issue 4, 2018. 35
Review of Literature
active agents from natural sources have always been of great interest to working on
various diseases. Since hundred yeras ago tribal community are using these traditional
knowledge system to medicate various type of diseases. They use different parts of
plant as a source of drug through trial and error method and the process is experienced
over hundreds of years, which says that the medicinal plants have been in the focus as
life saving drugs right from the beginning of the human life. The medicinal plants
have been the object of research in both systematic and advanced areas of plant
sciences. The traditional knowledge of these herbal recipes is popular among the
indigenous and local communities. Even present scenario the Tribal communities are
solely dependent on herbal medicines for their medication. So they are using herbs
against different. They have preserved the wealth of traditional knowledge as a part of
their belief and customs. They are practicing these methods, generation after
generation, successfully. Apart from medicinal uses phytochemical components
which are environment friendly, economical and effectively shows anti corrosive
properties and also phyto-compounds are used as biofuels.
Plant 1
Boerhaavia Diffusa
Boerhaavia Diffusa Linn. (Nyctaginaceae), common name is punarnava. In the Indian
system of medicine, is a permanent steal herb found throughout the waste land of
India. The roots are reputed to be diuretic and laxative and are given for the treatment
of various diseases. The Boerhaavia Diffusa has ancient medicinal use in different
societies from the times of the B.C. The herbal medicine has evolved and changed
through the years. A number of plant products have been identified through phyto-
chemistry and the extract of their different plant parts are useful in many diseases
without any side effects.
Geographical Distribution and Habitat
Boerhaavia diffusa, consisting of more than 40 species is distributed in tropical, sub-
tropical regions and warm climate. It‟s found in, America, Australia and Malay
Peninsula, Sudan extending to China and Islands of the Pacific. Among 40 species of
Boerhaavia, 6 species are found in India, namely B. diffusa, B. erecta, B. rependa, B.
chinensis, B.Hirsute and B. rubicund.

www.wjpr.net Vol 7, Issue 4, 2018. 36
Review of Literature
Boerhaavia diffusa in India is found in warm regions of the country and throughout up
to 2,100 m altitude in the Himalayan region. It is a permanent, distribution hogweed,
commonly occurring abundantly in misuse places, ditches and marshy places for the
period of rains. The plant is also cultivated to some extent in West Bengal.
Pharmacognosy
Scientific Name: Boerhaavia diffusa Linn. Syn.; B. repens vare. Diffusa
Family: Nyctaginaceae
Family Name: Hogweed, Horse Purslane Common Indian Names
Gujarati: Dholia-saturdo, Moto-satoda.
Hindi: Snathikari
Canarese: Kommegida
Marathi: Tambadivasu
Sanskrit: Punarnava, Raktakanda
Bengali: Punurnava
Tamil: Mukaratee-Kirei
Telugu: Punernava
Useful Parts: Root leaves and seeds.
Phytochemistry
The Boerhaavia diffusa plant contains a large amount of following compounds. For
example, Steroids, Alkaloids, flavonoids, lignins lipids, triterpenoids, carbohydrates,
proteins and glycoproteins. Punarnavine C17H22N2O. Melting point: 236–237°C.[43,44]
Boeravinone A-F. hypoxanthine 9-Larabino furanoside, ursolic acid, punarnavoside,
lirodendrin and a glycoprotein having a molecular weight of 16– 20 kDa have been
isolatedand studied in detail for their biological activity. Punarnava also contains
arachidic acid, α-2-sitoesterol, palmitic acid, tetracosanoic, stearic, urosil acid,
Hentriacontane, β -Ecdysone, triacontnol etc. Phytochemical screening of the roots
from garden-grown in vivo plants of B. Diffusa of different ages shown that the
highest alkaloid content 2% accumulate in the roots of 3-yearold mature plants. The
herb and roots are wealthy in proteins and fats. The herbal contains 17 amino acids,
with 7 essential amino acids and the root contains 15 amino acids, including 6
essential amino acids. Plant contained large amount of potassium nitrate, as well
punarnavine also. Previous researchs show the presence of flavonoid, alkaloid,
www.wjpr.net Vol 7, Issue 4, 2018. 37
Review of Literature
steroid, triterpenoid, lipid, lignin, carbohydrate, proteins and glycoprotein in B.
Diffusa.[45,55]
Other Chemical Constituents
Many rotenoids have been isolated from the roots of the Boerhaavia diffusa. Plant
also includes a series Pharmacological Potential of Boerhaavia diffusa boeravinones
viz., boeravinone A, B, C, D, E, F. Punarnavoside, a phenol glycoside, is reportedly
present in roots. C-methyl flavone also has been isolated from Boerhaavia diffusa
roots. Two known lignans viz., liriodendrin and syringaresinol mono-β-D-glycoside
have been isolated. Presence of a purine nucleoside hypoxanthine 9-L-arabinose,
dihydroisofuroxanthone-borhavine, phytosterols, have been isolated from the plant. It
contains about 0.04% of alkaloids known as punarnavine and punernavoside, an anti-
fibrinolytic agent. It also contains about 6% of potassium nitrate, an oily substance
and ursolic acid. The seeds of this plant contain fatty acids and allantoin and the roots
contain alkaloids. The green stalk of the plant has also been reported to contain
boerhavin and boerhaavic acid.
Medicinal Uses
According to Ayurveda, Punarnava is in biter test, astringent to bowels, leucorrhoea,
anaemia, inflammations, heart illness, asthma. The leaves are useful in indigestion,
cancer, spleen swelling and abdominal pains. According to Unani medicine, the
leaves are appetizer, alexiteric, useful in opthalmic, in joint pains. Seeds are tonic
expectorant, carminative, useful in backache, scabies. The seeds are considered as
promising blood purifier.
Boerhavia diffusa is believed to get better and guard eyesight. B. diffusa has diuretic
properties and is used by diabetics to decresed blood sugar. Boerhavia diffusa has
shown antibacterial activity, mainly against G- bectriea. Extracts of B.diffusa leaves
have demonstrate antioxidant and hepatoprotective properties in pharmacological
models. Punarnavine has shown some in vitro anticancer, anti-estrogenic, immune-
modulatory and anti-amoebic activity B. diffusa is a source of anti-oxidants and may
be efficient against arsenic tri oxide (an effective drug used against acute
promyelocytic leukemia) induced cardio toxicity.

www.wjpr.net Vol 7, Issue 4, 2018. 38
Review of Literature
Pharmacological and biological activity
The plant has gained lot of importance in the field of phytochemistry because of its
various pharmacological and biological activities such as immune-modulatory effects,
immunosuppressive activity, anti-metastatic activity, antioxidant activity, anti diabetic
activity anti proliferative and anti-estrogenic activity, analgesic and anti-inflammatory
activity, antibacterial activity, antistress and adoptogenic activity,
antilymphoproliferative activity, nitric oxide scavenging activity, hepatoprotective
activity, anti-viral activity, bronchial asthma, anti fibrinolytic activity,
chemopreventive action, genetic diversity analysis, anticonvulsant activity.
Antitumor Activity
Cancer chemo-preventive effect of B. diffusa was evaluated on 7 12-dimethyl
benz(a)anthracen (DMBA) induced skin papillomagenesis in male Swiss albino mice
(6-7 weeks old). The cancer chemo-preventive efficacy was assessed by its ability to
modulate the actions of enzymes allied with drug metabolism and biefficient
modulators reduced the availability of ultimate carcinogen metabolites in the
epithelial phase. the important enlargement in the activities of hepatic phase I & II
system. enzymes and antioxidant enzymes, glutathione peroxidase, glutathione
reductase, superoxide dismutase, catalase and glutathione level were observed when
rat were fed by oral gavage with B. diffusa extract at a dose level of 125 mg and 250
mg/kg body weight for a period of 15 days in laboratory. This lead to an assumption
that the inhibition of tumorigenesis by the plant extract might have been executed
either by preventing the formation of active carcinogens from their precursors or by
augmenting detoxification process, prevent promotional trial in the mouse skin
through free radical scavenging mechanism.
Antioxidant Activity
The evaluation of the antioxidant potential of ethanolic extract of Andrographis
echioides and B. diffusa was carry out by determining the levels of enzymatic and
non-enzymatic antioxidants. The results showed that both the plant extracts possessed
significant levels of enzymatic and non-enzymatic antioxidants. The results of the
enzymatic and non-enzymatic antioxidants in Andrographis echioides and Boerhavia
diffusa exhibits that they possess preventive and productive role to maintain the cell
survival, cellular interaction and maintenance of cell membrane architecture.

www.wjpr.net Vol 7, Issue 4, 2018. 39
Review of Literature
Andrographis echioides and B.diffusa have effective and therapeutic antioxidant
potential against various inflammatory diseases 61. The study was undertaken to
evaluate antioxidant activity of Chloroform, Ethanol and Ethyl acetate fraction of
Boerhaavia Diffusa L roots which might have improved its hepatoprotective action.
Invitro nitric oxide search activity, the percentage inhibition was 71.36%, 33.75%,
23.88%. in the extracts of ethanol, chloroform and ethyl acetate at 250mg/ml. when
compared with Curcumin at 62 mg/ml showed only 84.7% inhibition respectively.
The ethanol extract and ethyl acetate extrats showed a biphasic response whereas the
chloroform extract showed a dose dependent relative increase. In DPPH radial
scavenging activity, the ethanol extract showed 81.94% inhibition and the chloroform
extract showed 42.58% inhibition at 1000mcg/ml compared with 88.02% inhibition
by Quercetin. The present results propose that roots of B.diffusa were found to make
known antioxidant potential which supports the use of this plant in traditional
medicine.
Cytological activity
The extract of B. diffusa exhibited a strong depressive effect on the mitosis of C.
Jagus roots. The study was conducted using B. diffusa extract, the mitotic index of the
control experiment was found to be 5.27. There was a negative correlation between
the concentrations of the treatment extracts and the mitotic indices obtained from their
action. This points to an inhibition of mitosis by this extract. Inhibition of the mitotic
index increased significantly with an increase in the concentration of treatment
solution of B.diffusa. This again shows a very negative correlation between the
concentration of the extract and the mitotic indices produced by the observed action.
Owing to the ability of the root extracts of B. diffusa toaccumulate metaphase and
hence inhibit mitosis, it is possible to use these extracts as an alternative to the rather
expensive colchicine for cytological studies.
Bronchial Asthma
Dried leaves of Punernevacan be used in dhoomapana in treatment of bronchial
asthma. The leaf decoction is said to be an excellent expectorant when decocted with
punarnava (Boerhaavia diffusa) and then combined with ginger juice and black
pepper.

www.wjpr.net Vol 7, Issue 4, 2018. 40
Review of Literature
Anti Fibrinolytic Activity
A study evaluated the effect of anti-fibrinolytic agents; α-aminocaproic acid (α-ACA),
tranexamic acid (AMCA); anti-inflammatory drugs (indomethacin, ibuprofen,
naproxen); and root extract of B. diffusa on endometrial histology of IUD-fitted
menstruation of monkeys. It is effective in reducing edema, swelling and in increase
the amount of deposition of fibrin and platelets in the vessel lumen.
Anti-Convulsant Activity
The study was carrired out to investigate the alcoholic root extract of B.diffusa and its
various fractions as well as liriodendrin fraction for exploring the possible role of
liriodendrin in its anti-convulsant action. Air dried roots of B. diffusa was extracted
with methanol by cold maceration process. The methanol soluble fraction of extract
thus obtained was successively extracted to obtain liriodendrin fraction and two side
fraction, that is, chloroform division and phenolic compound division. Anti-
convulsant activity of methanolic extract and its different division, that is liriodendrin
division and phenolic compound division were studied in pentylenetetrazol-induced
seizure. The crude methanolic extract of B.diffusa and its liriodendrin division
showed a dose-dependent protection against PTZ-induced convulsions. The
liriodendrin fraction showed important protection in opposition to seizures induced by
BAY k-8544. These findings reiterate the anti-convulsant action of methanolic extract
of B. diffusa roots and also it can be concluded that the observed anticonvulsant
activity was due to its calcium channel opposit action, as this action was reserved only
in the liodendrin division, which has additionally been complete by important anti-
convulsant activity of liriodendrin division in BAY k-8644-induced seizures55. That
Study showed the crude methanolic extract of B. diffusa and its liriodendrin fraction
showed a dose-dependent protection against PTZ-induced convulsion.
Anti-proliferative and Anti-estrogenic Activity
Antiproliferative and antiestrogenic properties of methanol extract of Boerhaavia
diffusa (BME) in MCF-7 breast cancer cell lines. Boerhaavia diffusa extracts
exhibited a strong inhibitory effect on the proliferation of human breast cancer cells in
vitro and the antiestrogenic effects are mediated by ER. Phytochemical studies have
revealed the presence of alkaloids, flavonoids, phenols and saponins in BME. The

www.wjpr.net Vol 7, Issue 4, 2018. 41
Review of Literature
antiestrogenic activity shown by the extract may be attributed to these diverse
compounds.
Antidiabetic Activity
The study indicates that Boerhaavia diffusa and ethanolic extracts exhibit significant
anti-hyperglycemic activities in alloxan induced as well as streptazotocin induced
dieabitic rats. They can also recover the condition of diabetes as indicate by
parameters like body weight with serum cholesterol and triglyceride levels. The
number of functionally intact β-cells in the islet of langerhance organ is of decisive
importance for the development route and result of diabetes. The renewal of β-cells in
diabetes has been studied in several animals. The all β-cell mass reproduce the
balance in between the renewal and loss of these cells. It was also suggested that
renewal of islet β-cells following destruction by alloxan may be the primary cause of
the recovery of alloxan-injected guinea pigs from the effects of the drug. In alloxan-
induced diabetes, Epicatechin and Vinca rosea extracts has also been shown to act by
β- cells renewal. Comparable effects in streptozotocin treated diabetic animals were
details report by pancreas tonic, sylvestre leaf extracts. In the present studies, injure of
pancreas in streptazotocin treated diabetic control rats and regeneration of β-cells by
glibenclamide was observed. The comparable renewal was also shown by methanolic
extracts of Boerhavia diffusa. A study was carried out to investigate the effects of
daily oral administration of aqueous solution of Boerhaavia diffusa L. leaf extract
(BLEt) (200 mg/kg) for 4 weeks on blood glucose concentration and hepatic enzymes
in normal and alloxan induced diabetic rats. A imperative decrease in blood glucose
and significant increase in plasma insulin levels were observed in normal and diabetic
rats treated with BLEt42. Chloroform extract of B. diffusa leaf produced dose-
dependent reduction in blood glucose in streptozotocin-induced NIDDM rats
comparable to that of glibenclamide. The results indicate that the decrease in blood
glucose produced by the extract is probably through renewal of pancreatic beta-cells
action.
Antibacterial Activity
A effective anti-bacterial activity against gram+ and gram
- bacteria publicized by the
leaves of B.diffusa may be due to the plants chemicals present in the leaves. Ethanol
extract show inhibitory a cause on gram + bacteria, and all gram
-- bacteria selected for

www.wjpr.net Vol 7, Issue 4, 2018. 42
Review of Literature
the study. Methanol extract showed inhibitory effect against all gram+ bacteria
selected for the present study except M. luteus and gram-negative bacteria. The anti-
bacterial activity of the different extracts of the stem bark of Prosopis cineraria (Linn.)
Druce was estimate by the agar on form diffusion method. The aqueous and ethanolic
extracts of B.diffusa leaves had action on E. coli, S. Aureus and P. Aeruginosa. This
activity happen at changing concentration, representing that the plant extracts limited
active principle with broad antibacterial spectrum. E.coli show the highest
receptiveness in ethanolic extract, go after by S.aureus and the least at risk was P.
Aeruginosa. In aqueous extract P. aeruginosa explain the chief resistance, followed by
S. aureus and E.coli exhibited the least susceptibility. The antimicrobial action of the
different extracts increased with increase in concentration. The results of the
investigations support the ethnomedicinal use of this plant by local practitioners.
Results from that study showed that the aqueous and ethanolic extracts of B. diffusa
had antibacterial action on E. coli and P. Aeruginosa.
Antistress / Adaptogenic / Immunomodulatory Activity
Hydroethanolic extract (70%) of B.diffusa and an herbal formulation PHF-09 contain
B. Diffusa was compared for their stress free action using cold self-control strain
model. Stress was inducing by subjecting to cold restraint. Due to cold restraint
pressure there was an difference in the intensity of biochemical factor like glucose,
triglycerides, cholesterol, which were by regularize subsequent the administration of
HEBD and PHF-09. HEBD and PHF-09 were found to have similar anti-stress action.
The ethanol extract of roots of B. diffusa was estimate for antistress, adoptogenic
action in mice, by spin endurance test and cold restrains stress and the extract showed
superior load patience in immunomodulatory action was revealed by increased carbon
relase, indicating stimulus of the reticuloendothelial method. There was an raise in
DTH response to SRBC in mice, matching to cell referee immunity and representative
stimulatory effects on lymphocytes and accessory cell types.
Adaptogens is useful in both adrenal hyperstress as well as adrenal hypo tiredness. By
definition, an adaptogen involve the means for bidirectional or regularize property.
The most important adaptogens for the adrenals consist of Panax and siberian
Ginseng, withaniea sominfera, B. diffusa and tulsil Leaf Extract. B.diffusa has the
capability to carry both adrenal over and under activation. In stressful situation it has

www.wjpr.net Vol 7, Issue 4, 2018. 43
Review of Literature
established the capability to barrier the elevation of serum cortisol and prevents the
inhibition of the immune system that takes place with eminent cortisol. Then again, B.
diffusa has also demonstrated the ability to improve cortisol levels with end stage
adrenal exhaustion.
Hepatoprotective Activity
The hepatoprotective activity of roots of different diameters were collected in three
seasons, rainy, summer and winter and examined in thioacetamide in poisonous rats.
The results showed that an aqueous extract (2 ml/kg) of roots of diameter 1-3 cm,
collected in the month of May (summer), exhibited marked protection of a majority of
serum parameters, LDH,CK,ALP thereby suggesting the proper size and time of
collection of Bd L. Roots for the most attractive results. Further, the studies as well
prove that the aqueous form of drug (2 ml/kg) administration has more
hepatoprotective activity than the powder form; this is probably due to the better
absorption of the liquid form through the intestinal tract. The hepatic protective
activity of Boerhaavia diffusa L. roots showed marked protection of serum parameters
in thioacetamide toxicity in animals. besides, the aqueous extract of thin roots
collected in the summer has more activity suggesting the proper time and type of root
collection for the most desirable result. The investigation also validates the use of B.
diffusa L. roots in hepatic ailments by the several tribes in India.[180]
An alcoholic
extract of whole plant Boerhaavia diffusa given orally exhibited hepatoprotective
activity against experimentally induced carbon tetrachloride hepatotoxicity in rats.
The extract as well formed an enhance in normal bile flow in rats suggesting a strong
choleretic activity. The extracts do not explain any signs of toxicity up to an oral dose
of 2 g/kg in mice.
Analgesic / Anti-Inflammatory Activity
The Decoction (DE) or Juice (JE) of the leaves of Boerhaavia diffusa were used to
study the antinociceptive effect in chemical (acetic acid) and thermal (hot Plate)
models of hyperalgesia in Mice. The DE, raised the pain thresholds during the first
period (30 min) of observation. In the acetic acid-induced abdominal writhing in rat,
pretreatment of the animals by naloxone (6 mg/kg.) considerably reversed the
analgesic effect of morphine and JE but not that of DE. The experiment shows that the
lively antinociceptive standard of B. diffusa is mainly in the juice of leaves and has a

www.wjpr.net Vol 7, Issue 4, 2018. 44
Review of Literature
significant antinociceptive effect when assessed in these pain models.[182]
Ethanol
extract of leaves at dose of 400mg/kg exhibitedmaximum anti-inflammatory effect
with 30.4, 32.2, 33.9 and 32% with serotonin, carrageenin, dextran, histamine and
induce rat paw edema experimental, respectively. Ethanol extract of stem bark also
exhibited COX-1 and IC50 value of 100 mg/ml proving the drug use in the treatment
of inflammatory condition. Anti-inflammatory activity was assessed using extract of
latex of plant by using a carragenan induced inflammatory mode.
Anti-inflammatory activity
Ethanol extract of leaves at dose of 400mg/kg exhibited maximum anti-inflammatory
effect with and 32% with carrageenin, serotonin, histamine and dextran are effect on
rat paw oedema experiment method, respectively. Ethanol extract of stem bark also
exhibited COX-1 and IC50 value of 100ng/ml proving the drug use in the treatment of
inflammatory condition. Anti-inflammatory activity was assessed using extract of
latex of plant by using a carragenan induced inflammatory model.
Table 3.2.: Major differences between B. diffusa and Boerhaavia elegans.
Characters Boerhaavia diffusa Boerhaavia elegans
Plant A perennial herb from a fusiform root An erect glabrous shrub
Stem
Prostrate, decumbent or ascending, 4-
10mlong,rather slender, divaricately
branched
Annual, woody below,
glabrous above, thinly
pubescent close to the support.
Leaves
Opposite, two of a node unequal,
broadly ovate or orbicular, obtuse to
rounded or cordate at the support.
Or blong-lanceolate, obtuse
and often mucronulate at the
top
Flowers
In pendunculate, glomerulate clusters
arranged in slender, long stalkcked,
axillary or terminal corymbs
In large, lax, much branched,
leafless, glabrous compound
cymes above the leaves
Fruit
Obovoid or sub-ellipsoid, curved
over, a little cuneate, under, broadly
and bluntly 4-ribbed, awfully
glandular throughout
Flowering and Fruiting Throughout the year in Indian
conditions
September to December in
Indian conditions
PLANT 2
Asparagus racemosus
In recent years shatavari herb has become a popular ayurvadic medicine in all over
world. Women in the West have been using it ever since studies showed that it
contains phyto-estrogens hormones, the precursors of estrogen hormones. Its finding

www.wjpr.net Vol 7, Issue 4, 2018. 45
Review of Literature
made it popular all over world. Shatavari aretwo types which are widely used,
Asparagus racemosus wild that called shatavari, and the vegetable, Asparagas
officinalis linn.
Shatavari is widely use in Ayurvedaic medicine system. According to the Ayurveda
texts like the Charak Samhita, Susruta Samhita, and Astanga Samgraha, shows its
ancient use as early as Vedic Time. Shatavari is highly appreciated in Ayurvedaic
formuation, due to its potential not only menopausal health, but health in all stages of
a female‟s life cycle. Ayurvedic record literally claims that shatavari strengthen a
female to the point where she is capable, of producing, thousands of healthy ovam.
Long before current studies were published, the great commentator “Pandit Hem Raj
Sharma”, In the Kashyap Sahita”, it‟s clearly says that shatavari effective in female
health. In particular, noted the advantage of shatavari as a galactagogue. As such, it‟s
also affecting the infant‟s health indirectly. Shatavari suitably exemplifies a central
principal of Ayurveda; the use of this herbal drug as both, medicine and food.
Asparagus racemosus (Shatavari) is recommended in Ayurvedic texts for the
prevention and treatment of ulcers, gastric problems and galactogogue. A. racemosus
has also been used successfully by some Ayurvedic practitioners for nervous
disorders. Shatawari has different names in the different Indian languages. In Nepal it
iis called kurilo.the name shatawari means “curer of hundred diseases” (shat:
hundred”; vari:” curer”).
HABITAT
This climber growing in low jungles is found all over India; especially in Northern
India. The plant is a climber growing to 1-2m in length found all over India.
DESCRIPTION
Asparagus racemosus is plant with a woody stem that sends runners out, has pinpoint
like leaves with white flowers, Scandant, much branched spinous under shrub with
tuberou, small root, stock bearing numerous fusi form tuberous roots 30-100cm thick
leaves reduced to minute chaffy scales & spines. Cladodes acicular 2-6 hate, falcate
finely acuminate flower white, berries 7mm in diameter, globose, 1-seeded, red
(Sharma et al., 2000). The Himalayas up to an altitude of 1500 m.

www.wjpr.net Vol 7, Issue 4, 2018. 46
Review of Literature
Leaves, flowers and fruits
Satavar has small needle like phylloclades (photosynthetic branches) that are equal
and shine green. In July, it produces minute, white flowers on stem, prickly stems,
and September it fruiting time, producing blackish-purple, globular berry.
Roots
It has an adventitious root system with tuberous roots that measure about 2m in
length, tapering at both sides, with bunch in plant.
Pharmacological activity
Asparagus racemosus has been shown to mitigate the discomfort due to Amlapitta
(Acid dyspepsia with or without ulcer) on 109 cases in a clinical Study at CRIA
DEHLI.
Antibacterial activity
Anti secretory and antiulcer activity
Antidepressant activity of Asparagus racemosus in rodent models.
Anti-inflammatory effects
Anti-cancer
Antioxidant
Antitissuve
Enhances memory and protects against amnesia in rodent models.
Antilithiatic
Hepatoprotective effects in mice fed a high-fat diet.
Aphrodisiac.
Diuretic
Teratogenic
Immune modulators (extract), Immune adjuvant,
Oestrogenic effect
Neuroprotective
Anti-Stress

www.wjpr.net Vol 7, Issue 4, 2018. 47
Review of Literature
Chemical constituents
Asparagamine A
Alkaloid with antitumor activity, against a variety of cell lines was isolated from the
dried roots and subsequently synthesized to allow for the construction of analogs.
Saponins: Shatavaroside A and shatavaroside B, mutually with a saponin
filiasparoside C, it was isolated from the roots of Asparagus racemosus.
5 steroidal saponins, shatavarins6-10, with 5 more, shatavarin I, shatavarin IV,
shatavarin V, immunomodulator have been collect by the roots of satahvari.
Medicinal Uses
Asparagus racemosus is an important medicinal plant of tropical India. Its medicinal
usage has been statement in the Indian in traditional systems of medicine such as
Ayurveda, Unani and Siddha. It is mainly known for its plant estrogenic properties. In
Ayurveda, A. racemosus has been described as a rasayana herb and has been used
extensively as an adaptogen to increase the non-specific resistance of organisms
against a variety of stresses. As well use in the treatment of motion problem, the plant
also has antioxidant, antidyspepsia and anti-tussive effects. Plants for a in future can‟t
take any responsibility for any adverse effects from the use of plants. Always ask for
advice from a trained sooner than using a plant medicinally. Antispasmodic,
Aphrodisiac, Demulcent, Digestive, Diuretic, Galactogogue (to improve breast milk),
Infertility, Women‟scomplaints. Root is use in Diarrhea as well as in cases of chronic
colic and dysentery. The root was boiled with some bland oil and it is used in various
skin diseases „root is boiled in milk and the milk is administered to Shatavari (this is
an Indian world meaning a woman who has a hundred husbands) is the most
important herb in ayurvedic medicine for dealing with problems connected women‟s
fertility. It is taken internally in the treatment of loss of libido, infertility, menopausal
problem, threatened miscarriage, stomach ulcer, hyperacidity and bronchial infection.
Externally, it is used to treat the stiffness in the joints. The fresh root is taken for the
treatment of dysentery. The whole satavari plant is utilized in the treatment of brain
complaints, diabetes, diarrhea and rheumatism. It is also Used in Management of
behavioral disorder and minimal brain dysfunction. The rhizome is a soothing tonic
that acts mainly on the digestive, circulatory, respiratory, female reproductive organs
etc, antispasmodic, aphrodisiac, demulcent, diuretic, galactogogue and refrigerants.

www.wjpr.net Vol 7, Issue 4, 2018. 48
Review of Literature
DRUG PROFILE
Doxorubicin Hydrochloride
Discovery of doxorubicin an antitumor antibiotic, in the early 1960 represented a
major advancement fight against cancer. As the drug found to be very effective in a
verity of solid and soft human malginancy, however, the cardio toxicity is well
recognizes side effect of doxorubicin (anthracycline). that limit the total amount of
drug administrated and can cause heart failure in some patient. Early retrospective
study from the 1970sdemonstrted the heart failure and doxorubicin are related. with
the incidence of complication increasing sharply when the cumulative dose increased
550mg/m2. of the body surface. The incident of heart failure was 4% when the
cumulative dose of dox in between 500 to 550mg/m2. but its increased 18% when dox
is 551mg/m2 to 600mg/m2.and to as much as 36% when the total dose was at least
601%mg/m.
The ECG changes associated with doxorubicin cardio toxicity include various
arrhythmias, most commonly sinus trachcardiya, flatting of t waves, prolongation of
qt intervals and loss of r wave voltage. The incidence of these changes has been
reported to be 11% to 29%.
Myocardial damage as seen on myocardial biopsy, increase liner with increasing
cumulative dose of dox. but clinically the incidence of cardio toxicity is more
apparent at cumulative dose greater then 400-450mg/m2. This study is also made is
clear that CHF was a dose dependent phenomena. an incidence of >5%. was seen at a
500-550mg/m2 body surface are, increasing to >30%. at over 601%mg/m
2. Thus, the
dose of 500mg was considered the upper limit in order to minimize the risk of dox
cardio toxicity and CHF. Subsequent studies showed that cardio toxicity could occurs
at a much smaller dose of doxorubicin in patients with risk factor such as age, some
underlying heart condition, pervious and concurrent radiation therapy and
concomitant chemotherapy.
Doxorubicin has still remained in use because of its high antitumor activity. It also
forms a valuable component of various regimen of chemotherapy. There is still a need
to find ways to minimize the cardio toxic effects.

www.wjpr.net Vol 7, Issue 4, 2018. 49
Review of Literature
Description[193]
Doxorubicin (doxorubicin hydrochloride.C27H29NO11. HCL) cytotoxic anthracycline
antibiotic isolated from the culture of streptomyces paucities ver. caesius. In the
chemical structure of doxorubicin we found a naphthacenequinonone nucleus linked
through a glycosides bond at ring atom to amino sugar, daunosamine.
Chemical description: chemically, doxorubicin hydrochloride is: 5, 12-
napthoacenedione, 10-[(3-amino-2,3,6-trideoxy-α-L-lyxohexopyranosyl)oxy]-,8,9,10-
tetrahydroxy-8-(hydroxyacetyl)-1-methoxy, hydrochloride(8S-cis). Mol. weight of
doxorubicin: 579.99.
Doxorubicin binds to nucleic acids and specific interaction of the planar anthracycline
nucleus with the DNA double helix. The saturated end of the ring contains abundant
hydroxyl groups adjacent to the amino sugar; the anthracycline ring is lipophilic in
nature. Producing a hydrophilic canter. The molecule of doxorubicin is amphoteric in
nature, containing acid in the phenol ring groups and a basic purpose in the sugar
containing amino group. Its binds to cell membranes and plasma proteins.
Doxorubicin hydrochloride (Doxorex, doxorubicin hydrochloride for injection. USP)
is a sterile, red-orange in colour, lyophilized powered for intravenous or in the case of
local regional treatment of tumours by slow intra-arterial infusion. Doxorubicin
hydrochloride for injection is available in 10mg, 20mg and 50 mg single dose vials.

www.wjpr.net Vol 7, Issue 4, 2018. 50
Review of Literature
Each 10, 20 and 50 mg of Doxorubicin HCL, USP. And its presentation id each vial
contains 10 mg of doxorubicin hydrochloride as a freeze-dried powder, to be
dissolved in 5ml of water for injection (WFI) and its packaged in either single dose
polypropylene vials. And preservative-free, ready to use solution. Each millilitre of
solution contains 2 mg of doxorubicin HCL. Inactive ingredients sodium chloride
0.9%. I.P.
Biological activity
The mode of action of doxorubicin is connected to the ability of the antibiotic, to bind
to DNA and inhibit the synthesis of nuclide acid. The cell culture studies have
verified swiftly cell penetration by the antibiotic and main localization is in the
perinucleolar chromatin rapid inhibition of mitotic activity and nucleic acid synthesis
have also been demonstrated together with the appearance of chromosomal
aberrations.
Animal study on doxorubicin has shown that the cytotoxic agent is active in a
spectrum of experimental tumour and is immunosuppressive. However it does give
rice to a verity of toxic effects such as cardiac toxicity in rats.
Mechanisms of action of doxorubicin
The mechanisms of action of doxorubicin induced cardiac toxicity remains unknown,
but it has become possible to distinguish between the mechanisms underlying
doxorubicin antitumor effect and the mechanisms responsible for cardiac toxicity. The
proposed mechanisms for dox induced injury are cellular damage mediated by
reactive oxygen and nitrogen species. The discordance is probably associated with
different mechanisms mediating the acute and chronic cardio toxicity. In fact, a
number of studies using antioxidant supplements have failed to show a relevant
protective effect against chronic cardio toxicity. Therefore, cardiac toxicity may also
be related to some unknown non- ROS mechanisms. For example a decrease in the
mitochondrial calcium release channel and fatty acid metabolism in the myocardium.
The exact causal mechanisms of doxorubicin induced cardio myopathy remain
unclear, but most of the evidence indicates that free radicals are involved. The
chemical structure of doxorubicin is level to the generation of free radical and the
oxidative strain that results connect with cellular injury. Increases oxidative stress
may lead to a variety of sub cellular change in the myocardium, including the slow

www.wjpr.net Vol 7, Issue 4, 2018. 51
Review of Literature
loss of myofibrils and vacuolization of myocardial cells, changes typical of
doxorubicin induced cardio myopathy. And administration of doxorubicin is
associated with a decrease in the presence of the endogenous antioxidants and an
increases in free radicals, that‟s by oxidative stress also increased, which is followed
by the development of cardio myopathy and heart failure.
DOXORUBICIN MECHANISM
Antitumor action and cardiac toxicity
The sub cellular basis for doxorubicin induced cardiomyopathy as well as its
antitumor action was earlier thought to involve a common pathway. Though, more
recently it has become possible to differentiate the mechanisms underline these dual
effect of doxorubicin.
1. Antitumor action
Free radical injury might be a mechanism of doxorubicin anti tumour action because
doxorubicin administration has been shown to produce free radicals. Another in point
supporting the concept of free radicals-mediated anti-tumour action is that
doxorubicin forms an adarimycin-iron complex by binding with iron. This binding
can also form a complex with DNA and these complexes can stimulate the production
of oxygen (partially reduced forms). Because of free radical production in
neighbourhood of DNA strands, DNA damage as well as breaking of strands occurs.
In various literatures it was revealed that relatively high in vitro concentration of dox
was used to demonstrate the free radicals-medicated DNA damage in tumour cells.
The dox use in vivo condition were much lower, suggested that a free radicals
mechanisms might not be the primary cause of the antitumor activity of doxorubicin.
This point was supported by a multitude of studies in which the addition of different
anti-oxidants dose not compromises doxorubicin cytotoxicity in a variety of tumour
cells.
There were the other mechanisms which explain the inhibition of DNA replication by
dox and thus its cyto toxicity and anti tumour action, without involvement of free
radicals.

www.wjpr.net Vol 7, Issue 4, 2018. 52
Review of Literature
A direct intercalation of dox between DNA base pairs interferes with DNA
replication; that was a cooperative interaction between dox and DNA. Dox mediated
inhibition of DNA topoisomerase II was also shown to inhibit the DNA replication.
Adriamycin topoisomerase II – DNA complex prevents repairing of the broken DNA
strands.[201]
Antitumor action of doxorubicin at low concentrations, independent of free radical
mediation was reconciled with the free radical mediated cardio-toxic effect of the
drug seen at higher cumulative doses in a scheme shown in figure 3.4.
Fig. no. 3.4: Cardiotoxic and antitumor mechanisms of action of doxorubicin.[203]
Molecular mechanisms
Existing evidence points to a complex situation with a multitude of molecular
mechanisms involved in doxorubicin induced impairment of cardiac energetic and
other cellular targets, finally lead to cardiac dysfunction.

www.wjpr.net Vol 7, Issue 4, 2018. 53
Review of Literature
Fig. 3.5: Cardio toxicity mechanisms and targets of doxorubicin.
An important factor, which can mediate toxic action of doxorubicin, especially in
mitochondria, was high affinity binding of dox to cardiolipin, anionic Phospholipids
in eukaryotic energy metabolism. cardiolipin with its particular ability to interact
more or less specifically with many protein was very important not only for
mitochondrial structure and purpose, but also for in general cardiac energy
metabolism as well as for cell survival. 88 87. binding of doxorubicin would modify
membrane properties and changes the Phospholipids‟ environment and function of
numerous crucial mitochondrial integral membrane proteins which depends upon
cardiolipin in their function.
Cardiolipin bounded doxorubicin would also induced dissociation of cardiolipin
associated peripheral proteins from the inner mitochondrial membrane, e.g.
Cytochrom C and CK. That would affect electron transport chain and energy
channelling as well as a favour of initiation of program cell death. Toxicity of
mitochondrial, mostly cardiolipin bounded dox was mediated by oxidative stress,
www.wjpr.net Vol 7, Issue 4, 2018. 54
Review of Literature
which was represented a particular threat to cellular energetic in the myocardium and
was considered as the name mediator of doxorubicin cardio toxic action.
Heart tissue is rich in mitochondriathats by they heavily relies on oxidative
metabolism and thus produced significant amount of free radicals. Accumulation of
redox active adriamycin in these organelles would enhance mitochondrial production
of free radicals of oxygen and as more recently evidenced also of nitrogen species.
Quinine present in Dox compound can be converted in to the semiquinone form by
the reaction of one electron reduction. The Dox semiquinone can consequently
transfer an electron to the oxygen molecule (O2) to form superoxide anion radicals
(O2-).
[203] The latter can dismutateto form hydrogen peroxide (H2O2) and further
hydroxyl radicals or may react with nitric oxide to form peroxynitrite (ONOO-). The
noxious action of these reactive compounds could explain phenomena such as:
The triggering of apoptosis in mitochondrial cells.
Membrane damage (peroxidation of lipids)
Effects on genetic expression.
Changes in protein activity.
Damage to DNA.
The particular susceptibility of the myocardium relative to other tissue rests on its
relative lack of enzymes such as dismutase and catalases, which are responsible for
the breakdown of reactive oxygen species. The heart is particularly protected against
the oxidative stress.
Per oxidation of membrane phospholipids associated with decrease in the membrane
fluidity and also oxidation or nitration of proteins has been reported after Dox
treatment. Oxidative and nitrostative stress interfere with many aspects of cardiac
purpose, inducing between others energetic inequality, mitochondrial permeability
transition and apoptosis and activation of various related signalling pathways. In
particular the response of cardiac Ca2+
to DOX can be closely related with the
perturbation of heart energy homeostasis. Dox induced alterations in Ca2+
ion
handling and their possible consequence are already reported.

www.wjpr.net Vol 7, Issue 4, 2018. 55
Review of Literature
It is to note, that the actual extent and impact of oxidative and nitrostative stress
produced by Dox in different toxicity models and in patients, are a matter of
discussion. Interestingly, quinine-containing molecules can exert their effect
independently of free radicals by directly affecting some sensible protein residue, e.g.
reactive sulfahydryl groups and because of this group Dox can interact with the
cardiac gene expression as they contains sulfahydryl groups, in particular by down
regulating genes of several enzymes implicated in energy metabolism.
Even though such interference with DNA is considered important for the anticancer
action of the drug and it may also affect macromolecular biosynthesis of the heart.
Additionally, oxidative stress has been implicated in Dox-impaired gene expressions.
Fragmentations and proteolysis of Dox modified proteins were shown to occur in Dox
treated mitochondrial preparations. And also, to lower biosynthetic rate and enhanced
degradation rate, compact cellular levels of soluble proteins and metabolites in
doxorubicin challenged cells can occurs through leakage. This is well known for
cytosolic, CK, the plasma level of which serve as clinical markers of different cardiac
pathologies, including Dox toxicity.
On the other hand, it should be noted that certain gene and coding proteins implicated
in energy metabolism have been found unregulated in a mice model of chronic
Doxorubicin cardiac toxicity. This may imitate induction of a protective or
compensatory reply. additional mechanism some part to the toxic effect of
doxorubicin in cardiac tissue can be mediated by iron or Dox metabolites and by an
important damage of endothelial origin.
Communally, the response of cardiac energetic to DOX involves a complex crosstalk
between different pathways and mechanisms.
Clinical pharmacology
Pharmacokinetics study has shown that intravenous administration of labelled
doxorubicin is followed by a rapid fall in the plasma levels, accompanied however by
slow urinary and binary excreta. this is probably due to binding of the antibiotic to
tissues. the initial distribution have life of approximately 5.0 min suggests rapid tissue
uptake of doxorubicin, while its slow elimination form tissue from tissue is reflected

www.wjpr.net Vol 7, Issue 4, 2018. 56
Review of Literature
by a terminal half life of 20 to 4 hour. Steady-state distribution volumes exceed 20 to
30 l/kg and are indicate of extensive drug uptake into tissues. Urinary excretion as
determined by flourimetric methods accounts for approximately 5% of the
administration dose in 5 days; biliary excretion is the major elimination route, with
40-50% of the administered dose recovered in the bile or faeces. In seven days:
impaired liver function causes slower excretion of the drug and in consequence
increased accumulation in plasma and tissues dox dose not cross the blood brain
barrier.
Pharmacokinetics
The Pharmacokinetic study, determined in patients with various type of tumours
undergoing either single or multi-agent therapy have shown that doxorubicin follows
a multiphase disposition after intravenous injection.
Distribution: The primary division half-life of approximately 5 minutes suggests
rapid tissue uptake of doxorubicin, while its slow elimination from tissue reflected by
a terminal half-life of 20 to 48 hours.
Binding of doxorubicin and its major metabolite, doxorubicin, to plasma proteins is
about 74 to 76% and is independent of plasma concentration of doxorubicin up to
1.1g/ml. Doxorubicin was detectable in the milk up to 72 hour after therapy with
70mg/m2 of doxorubicin given as a 15-minute intravenous infusion and 100mg/m
2 of
cisplatin as a 26 hour i.v. mixture. The peak absorption of doxorubicinol in milk at 24
hour was 0.12g/ml and AUC up to 24 hours was 9.0g/ml while the AUG for
doxorubicin was 5.4g/ml. doxorubicin dose not the blood brain barrier.
Metabolism
Enzymatic reduction at the seventh position and cleavage of the daunsamine sugar
yields aglycone which is accompanied by free radical arrangement, the general
making of which may contribute to the cardio toxic activity of doxorubicin.
Disposition of doxorubicinol in patients is formation rate limited, with the terminal
half-life of doxorubicinol being similar to doxorubicin. The relative exposure of
doxorubicinol, i.e., the ratio between the AUG of doxorubicinol and the AUG of
doxorubicin, compared between the doxorubicin range of 0.3 to 0.7.

www.wjpr.net Vol 7, Issue 4, 2018. 57
Review of Literature
Execration
Plasma clearance is in the range 324 to 809 ml/min/m2 and is predominately by
metabolism and biliary excretion. approximately 40% of the dose appears in the bile
in 5 days, while only 5 to 12% of the drug and its metabolites appear in the urine
during the systemic clearance of doxorubicin is significantly reduced in obese women
with ideal body weight greater than 130%.there was a significant reduction in
clearance without any change in volume of distribution in patients when compared
with normal patients with less than 115% ideal body weight.
Contraindication
Patients should not be treated with doxorubicin if they have any of the following
conditions, baseline neutrophil count <1550 cells/mm3.; major liver injury; recent MI,
severe myocardial lack, major arrhythmias, earlier treatment with complete
cumulative doses of doxorubicin and other anthracycline or hypersensitivity to
doxorubicin, any of its excipients, or other anthracycline or anthracenediones.
INDICATIONS AND USAGE
Doxorubicin hydrochloride Injection, USP and Doxorubicin HCl for Injection, USP
have been used successfully to produce regression in disseminated neoplastic
conditions such as acute lymphoblastic leukaemia, acute myeloblastic leukaemia,
Wilms tumour, neuroblastoma, soft tissue and bone sarcomas, breast carcinoma,
ovarian carcinoma, transitional cell bladder carcinoma, thyroid carcinoma, gastric
carcinoma, Hodgkin‟s disease, malignant lymphoma and bronchogenic carcinoma in
which the small cell histological type is the most responsive compared to other cell
types.
Doxorubicin is as well show for use as a component of adjuvant therapy in women
with evidence of axillaries lymph node involvement following resection of primary
breast cancer.
Drug interactions
Doxorubicin is extensively metabolized by the liver. Change in hepatic function
induced by concomitant therapies may affected doxorubicin metabolism,
pharmacokinetic, therapeutic and GIT actions, may be increased when doxorubicin is
used in combination with other cytotoxic drugs.

www.wjpr.net Vol 7, Issue 4, 2018. 58
Review of Literature
Drug Intreaction
Dabigatran etexilate
P-Glycoprotein inducers i.e. doxorubicin can
reduce the serum concentration of dabigatran
etexilate.
Digoxin The anti neoplastic agent decreased the effect
of digoxin.
Telithromycin Telithromycin may reduce clearance of
Doxorubicin.
Terbinafine Terbinafine may reduce the metabolism of
Doxorubicin.
Cyclosporine
Cyclosporine results in increases in AUG for
both doxorubicin and doxorubicinol possibly
decreases in clearance of parent drug.
Progesterone
Progesterone was given intravenously to
patients with advanced malignancies at high
doses .its enhanced doxorubicin-induced
neutropenia and thrombocytopenia was
observed.
Verapamil
A learn of the effects of verapamil on the acute
toxicity of dox in mice relevative higher initial
peak concentrations of dox in the heart with a
higher incidence and severity of degenerative
changes in cardiac tissue resulting in a shorter
survival.
Phenobarbiton Increcses the elimination of doxorubicin.
Streptozocin That inhibit hepatic metabolism of doxorubicin.
Cytarabine
Necrotizing colitis manifested by typhlitis,
bloody stool. and severe and some time fetal
infection have been associated with a
combination of doxorubicin given by i.v.
ADVERSE REACTIONS
Dose limiting toxicities of therapy are myelosuppression and cardiotoxicity. There are
other reactions which were reported as:
Cardiac
Cardiotoxicity is a known risk of treatment with anthracycline. Anthracycline induced
cardiotoxicity can be apparented by early (or acute) or late events. Early cardiotoxity
includes mainly sinus tachycardia and/or electrocardiogram (ECG) abnormalities such
as non-specific changes in ST-T wave. Tachyarrhythmia includes premature
ventricular contractions and bradycardia, ventricular tachycardia and also
atrioventricular and bundle-branch block have also been described. These type of
effects generally does‟nt predict consequent development of delayed cardiotoxicity,
www.wjpr.net Vol 7, Issue 4, 2018. 59
Review of Literature
are infrequently of clinical importance, and are usually not well thought-out a
suggestion for the suspension of doxorubicin treatment.
Delayed cardiotoxicity usually develops late in the course of therapy with doxorubicin
or within 2 to 3 months after the termination of treatment, but in later events, it takes
several months to years after completion of treatment. Later cardiomyopathy is
manifested by a reduction in LVEF and/or signs and symptoms of congestive heart
failure (CHF) such as tachycardia, pulmonary edema, cardiomegaly and
hepatomegaly, oliguria, pleural effusion, etc and also subacute effects i.e.
pericarditis/myocarditis also investigated. Life intimidating CHF is the most sterning
form of anthracycline-induced cardiomyopathy and represents the cumulative
doselimiting toxicity of the drug.
Cutaneous
Reversible complete alopecia occurs in most of the cases. Hyperpigmentation of
nailbeds and dermal creases and onycholysis have been described in a several cases.
Rash, itching, or photosensitivity may also occur.
Gastrointestinal
Acute nausea and vomiting occurs frequently and severly and can be improved by
antiemetic therapy. Mucositis (stomatitis and esophagitis) may occur within 5 to 10
days after starting of therapy and most of the patients get well from this adverse
reaction within the another 5 to 10 days or may be severe leading to ulceration and
origin of severe infections.
Hematologic
As with other cytotoxic agents, doxorubicin may cause myelosuppression.
Myelosuppression requires cautious monitoring. Total and differential WBC, red
blood cell (RBC) and platelet counts should be considered before and during each
cycle of therapy with the drug doxorubicin. Clinical effects of severe
myelosuppression include fever, infections, sepsis, septic shock, hemorrhage, tissue
hypoxia, or death.

www.wjpr.net Vol 7, Issue 4, 2018. 60
Review of Literature
Hypersensitivity
Fever, chills and urticaria have been reported and it was considered that Anaphylaxis
can occur. A case of obvious cross sensitivity to lincomycin has been reported.
Neurological
Peripheral neurotoxicity in the form of local-regional sensory and/or motor
disturbances have been reported in patients treated intra-arterially with doxorubicin
and/or with cisplatin. In animal studies it was inestigated that; seizures and coma in
rodents and dogs treated with intra-carotid doxorubicin occurs.
Ocular
Keratitis, Conjunctivitis and lacrimation occur usually.

www.wjpr.net Vol 7, Issue 4, 2018. 61
Matrial and Methods
CHAPTER 4
MATRIAL AND METHODS
List of Chamicals Used
Table No. 4.1 List of Chemicals Used.
S.No Chemicals
01 ETHYL ALCOHOL(AR)
02 Formaldhyde solution 10%
03 Rat feed
04 Sodiun chloride(ar)
05 Ketamine.HCL. inj. For i.m.,slow i.v.,i.v. infusion: Aneket
06 Anaethetic ether i.p.500 ml
LIST OF DRUGS USED
Table No. 4.2: List of Drugs Used.
S.No Drugs
01 Doxorubicin HCL
02 Boerhaavia Diffusa
03 Asparagus Racemosus
DOSE SELECTION AND PREPATION
Prepation of doxorubicin and dose selection
Doxorubicin Hydrochloride (DOX): Doxorubicin was supplied as a reddish orange,
hygroscopic in nature, crystalline powder form. DOX solution shoul be freshly
prepared and protected from light and was dissolved in saline solution. dosage of the
doxorubicin administration intraperitional was prepared in (0.9%) sodium chloride
saline solution.
Dose of doxorubicin each dose contining 2.5mg/kg body wt. for a cumalitive dose of
15 mg/kg body wt. for the present study, were chosen based on the previous reports.
Prepation of combination of harbal drug
Boerhaavia Diffusa(P) and Asparagus Racemosus(S) powder was suspended in 0.9%
saline sodium chloride and each animals belonging to two groups recieved 4ml of PS.
at a dose of 250 mg/kg body weight everyday respectively by the intragastric
intubation.
Route of administration: Oral and intrapenitional.

www.wjpr.net Vol 7, Issue 4, 2018. 62
Matrial and Methods
EXPERIMENTAL ANIMALS
Wister albino rats of either sex weighing 150-200 grams, were procured from animal
house, Arya College of pharmacy, Jaipur. The animals were housed under standard
laboratory conditions of 25 ±2C temperature, relative humidity of 55% and 12:12 hour
light : dark cycle maintain during the study. The animal were given standred rat pellet
and tap ad libitum. The experimental protocol was approve by institutional animal
ethical committee(IAEC), committee for purpous of control and supervision of
experiments on animals (CPCSEA).
II. METHOD
Experimental Design And Protocol
Dox induced myocardial toxicity
Group I:- CONTROL (Control group): Animals were treated with normal saline
5ml/kg.
Group II:- DOX (Doxorubicin treated): Doxorubicin was administered
intraperitonially in each dose containing 2.5mg / kg of the body weight for a
cumulative dose of 15mg/kg of the body weight.
Group III: PS+DOX
Pretreated daily (200mg/kg/oral) for 2 weeks and after pretreatment then alternatively
with Doxorubicin injection (for a cumulative dose of 15mg/kg body weight) for next
2 weeks. At the last treatment, blood samples were obtained under ether anesthesia
using heparin treated micro capillaries for the estimation of enzyme biomarkers (ALP,
LDH and CPK). Control and treated animals was observed for a period of 4 weeks
after the last injection, for the appearance, behavior and mortality. At the end of 4
weeks post treatment period, animals were anaesthetized with anesthetic ether and
ECG parameters were recorded using BPL 05 cardiart. The animal were killed under
ether anesthesia and a midline abdominal incision was performed and heart tissue was
quickly dissect out, washed in cold normal saline, dried on filter paper and weighed.
Group IV: B.diffusa(P): was pretreated daily (200mg/kg/ oral) mix with 0.9% normal
saline for 2 weeks and then with doxorubicin alternatively for next 2 weeks.

www.wjpr.net Vol 7, Issue 4, 2018. 63
Matrial and Methods
Group V: A.racemosus(S): S was pretreated daily (200mg/kg/ oral) with 0.9%
normal saline for 2 weeks and then with doxorubicin alternatively with normal saline
0.9% for next 2 weeks.
At the end of experiment, the animals were subjected to:-
Mortality: Death rate was determined.
Behaviour: Changes in behaviour was observed.
BODY WEIGHT PARAMETERS
Body weight of each rat was recorded every 15 days till the completion of 30 day
study.
Serum parameters
All the animals were fasted overnight but allowed to free access to water. on the last
day of drug administion, animals was anaesthetized with ether and blood sample was
collected by the retro-orbital plexus of each rat. then serum was seprated; Alkaline
phosphate (ALP), lactate dehydrogenase(LDH) and creatine phosphokinaase-MB
isoenzyam, (CPK-MB) were measured by kits or tested in pathology lab.
A. Estimation of Alkaline phosphate (ALP)
Clinical significance: The high concentrations of ALP in liver, bone, placenta,
intestine and certain tumours’.
Increases: High level of ALP, the enzyme occurs in liver diseases, bone diseases,
Hodgkin’s disease or congestive heart failure.
Decreases: Low levels of ALP occur in hypophosphatasia and malnourished patients.
B. estimation of lactate dehydrogenise (LDH)
Clinical significant
The enzyme LDH is concentrated in cardiac, renal, liver, muscle and other body
tissue.
When LDH increased in body then following disordered generate myocardial
infarction, kidney damage and other muscle disease.

www.wjpr.net Vol 7, Issue 4, 2018. 64
Matrial and Methods
C. Estimation of Creatine Kinase (CPK)
Clinical significance: Creatine kinase is found in skeletal muscle, cardiac muscle and
cerebral muscle tissues.
Increases: CPK levels increases in body then cause myocardial infarction, acute
cerebra-vascular disease and muscular injury. Following a myocardial infarction, CK
activity begins to rise within 3 to 5 hours, peaks between 20 and 30 hours and returns
to normal by the third day.
ELECTROCARDIOGRAPHIC PARAMETERS
Fig. No. 4.1: Electrocardiogram.
ECG was recorded at the end of the treatment after the last dosing. BPL 05 cardioart
ECG machine was used to record and monitor ECG tracings. take one Rats from each
group were anesthetized with ketamine (aneket) anesthesia, needle electrodes were
inserted under the skin for the limb lead. For each ECG tracing ST, QT interval, QRS
complex and heart rate were measured.

www.wjpr.net Vol 7, Issue 4, 2018. 65
Matrial and Methods
At the time of ecg recording ecg graph paper speed is 25 milliM/sec.
Heart rate: Heart rate canbe easily determined y the counting the number of large
squars between two consecutive QRS complexs. Ecg tracing covers 5 large squars or
one large squar is equal to 0.2 sec. one small squar is equal to 0.04 beat/sec. normal
heart rate is 60 to 100/min.
STATISTICAL ANALYSIS
All result are expressed as MEAN±S.E.M. statistical significance is calculated using
studdent’s t-test which was employed for comparison of control group and other test
groups.
P<0.05 was considered as significant.
P value less then 0.05 and greter then 0.01 is significant.
P value less then 0.01 and greater then 0.001 is very significant.
P value less then 0.001 is concidered to be extremely significant.

www.wjpr.net Vol 7, Issue 4, 2018. 66
General Obesrvation and Mortality
CHAPTER 5
GENERAL OBESRVATION AND MORTALITY
A. GENERAL APPERANCE
In the general appearance all group of animals was throughout the study/experiment
period. In the experimental period animals are shows following characters by each
group.
1. Doxorubicin treated animals fur become scruffy, soft watery faces and enlargement
abdomen. This condition is more severe at the end of the experiment period. And the
other hand these types of symptoms are not observed in other group (B. Diffusa, A.
Racemosus, normal saline group and combination group.
2. Mortality
In the doxorubicin group 50% mortality observed. But there were no mortality
observed in the normal saline, B. Diffusa, A. Racemosus and there combination of
the.
Table No 5.1: Mortality Rate.
S.NO TREATMENT MORTALITY % VALUE
1 GROUP I (N.S) 0/6 0%
2 GROUP II(DOX) 3/6 50%
3 GROUP III (P+S+DOX) 0/6 0%
4 GROUP IV(P+DOX) 0/6 0%
5 GROUP V (S+DOX) 0/6 0%
(N.S-NORMAL SALINE, DOX-DOXORUBICIN, P-PUNARNAVA, S-
SATAVARI).
3. Doxorubicin treated animals showed gradually decreased in food and water
consumption, as compare to normal saline. But this consumption was improved in the
pre-treatment duration in each group.
Heart weight, body weight and ratio of heart and body
The result shown from table no. and fig.no...shows that the heart weight in the NS,
DOX, PS+D, P+D, S+D (n=6) treated rat were 0.76±0.004, 0.94±0.006,a,
0.77±0.003,ns
0.82±0.04 and 0.80±0.03gm, respectively. The heart weight in
doxorubicin treated rat was significantly increased compare with normal rat. The heart
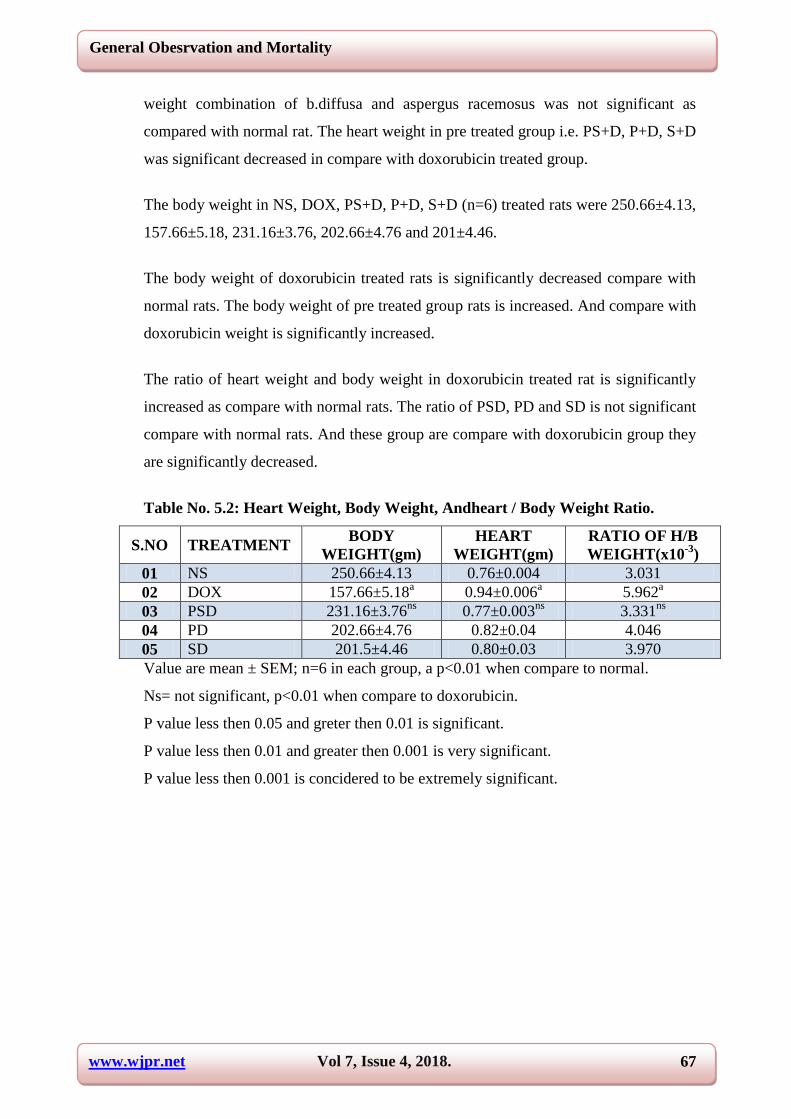
www.wjpr.net Vol 7, Issue 4, 2018. 67
General Obesrvation and Mortality
weight combination of b.diffusa and aspergus racemosus was not significant as
compared with normal rat. The heart weight in pre treated group i.e. PS+D, P+D, S+D
was significant decreased in compare with doxorubicin treated group.
The body weight in NS, DOX, PS+D, P+D, S+D (n=6) treated rats were 250.66±4.13,
157.66±5.18, 231.16±3.76, 202.66±4.76 and 201±4.46.
The body weight of doxorubicin treated rats is significantly decreased compare with
normal rats. The body weight of pre treated group rats is increased. And compare with
doxorubicin weight is significantly increased.
The ratio of heart weight and body weight in doxorubicin treated rat is significantly
increased as compare with normal rats. The ratio of PSD, PD and SD is not significant
compare with normal rats. And these group are compare with doxorubicin group they
are significantly decreased.
Table No. 5.2: Heart Weight, Body Weight, Andheart / Body Weight Ratio.
S.NO TREATMENT BODY
WEIGHT(gm)
HEART
WEIGHT(gm)
RATIO OF H/B
WEIGHT(x10-3
)
01 NS 250.66±4.13 0.76±0.004 3.031
02 DOX 157.66±5.18a 0.94±0.006
a 5.962
a
03 PSD 231.16±3.76ns
0.77±0.003ns
3.331ns
04 PD 202.66±4.76 0.82±0.04 4.046
05 SD 201.5±4.46 0.80±0.03 3.970
Value are mean ± SEM; n=6 in each group, a p<0.01 when compare to normal.
Ns= not significant, p<0.01 when compare to doxorubicin.
P value less then 0.05 and greter then 0.01 is significant.
P value less then 0.01 and greater then 0.001 is very significant.
P value less then 0.001 is concidered to be extremely significant.

www.wjpr.net Vol 7, Issue 4, 2018. 68
General Obesrvation and Mortality
Fig. no. 5.1: Body weight of animal model.
Figure 5.2: Heart weight of animal model.
Estimation of enzyme biomarker
ALP, CK, LDH
It’s depicted from table no. and fig. no. that the ALP level in the NS, DOX, PS+D,
P+D, S+D. (n=6). Treated rats were 142.16±3.43, 270.83±5.74, 216.83±5.19,
199.83±5.38 and 207.33±5.08 respectively.
It is evident from table no... And the fig.no...that the CK level of NS, DOX, PS+D,
P+D, S+D treated rat were 2607±6.44, 3011.16±7.41, 2691.66±6.21, 2729.83±3.43,
2753.5±5.12 respectively.

www.wjpr.net Vol 7, Issue 4, 2018. 69
General Obesrvation and Mortality
It is evident from table no. And the fig.no. Observation for the LDH level of NS,
DOX, PS+D, P+D, S+D treated rats were 152.33 ± 6.68, 357.5 ± 6.44, 307 ± 6.87,
207.66 ± 5.50 and 285.5 ± 5.4 respectively.
Doxorubicin treated rats shown a significant increased in the levels of ALP, CK, LDH
as compare to normal group.
Table no. 5.3: Estimation of ALP, CK and LDH (Normal).
S.NO ALP(IU/L) CK(IU/L) LDH(IU/L)
01 142 2610 153
02 147 2602 146
03 138 2615 163
04 139 2598 147
05 145 2612 157
06 142 2605 148
MEAN±SEM 142±3.43 2607±6.44 152.33±6.68
Table no. 5.4: Estimation of ALP, CK and LDH (DOX).
S.NO ALP(IU/L) CK(IU/L) LDH(IU/L)
01 273 3015 350
02 279 2998 356
03 269 3018 360
04 275 3009 359
05 268 3017 368
06 265 3010 352
MEAN±SEM 270.83±5.74 3011.16±7.41 357.5±6.44
Table no. 5.5: Estimation of ALP, CK and LDH (PS+D).
S.NO ALP(IU/L) CK(IU/L) LDH(IU/L)
01 216 2695 310
02 210 2690 316
03 218 2688 298
04 213 2696 305
05 219 2682 301
06 225 2699 312
MEAN±SEM 216.83±5.19 2691.6±6.21 307±6.8
Table no. 5.6: Estimation of ALP, CK and LDH (P+D).
S.NO ALP(IU/L) CK(IU/L) LDH(IU/L)
01 198 2730 210
02 204 2725 215
03 194 2732 200
04 208 2728 207
05 195 2735 203
06 200 2729 211
MEAN±SEM 199.83±5.38 2729.83±3.43 207.66±5.5

www.wjpr.net Vol 7, Issue 4, 2018. 70
General Obesrvation and Mortality
Table no. 5.7: Estimation of ALP, CK and LDH (S+D).
S.NO ALP(IU/L) CK(IU/L) LDH(IU/L)
01 210 2756 280
02 205 2750 289
03 214 2758 278
04 201 2748 285
05 211 2760 291
06 203 2749 290
MEAN±SEM 207.3±5.08 2753.5±5.1 285.5±5.4
Table no. 5.8: Comparetive Study of Serum Enzymes Biomarkers.
S.NO TREATMENT ALP(IU/L) CK(IU/L) LDH(IU/L)
01 NS 142±3.43 2607±6.44 152.33±6.68
02 DOX 270.83±5.74 3011.16±7.41 357.5±6.44
03 PS+D 216.83±5.19 2691.6±6.21 307±6.8
04 P+D 199.83±5.38 2729.83±3.43 207.66±5.5
05 S+D 207.3±5.08 2753.5±5.1 285.5±5.4
P.VALUE P<0.0001 P<0.0001 P<0.0001
Figure 5.3: Graph of ALP of treated rats in myocardial toxicity.
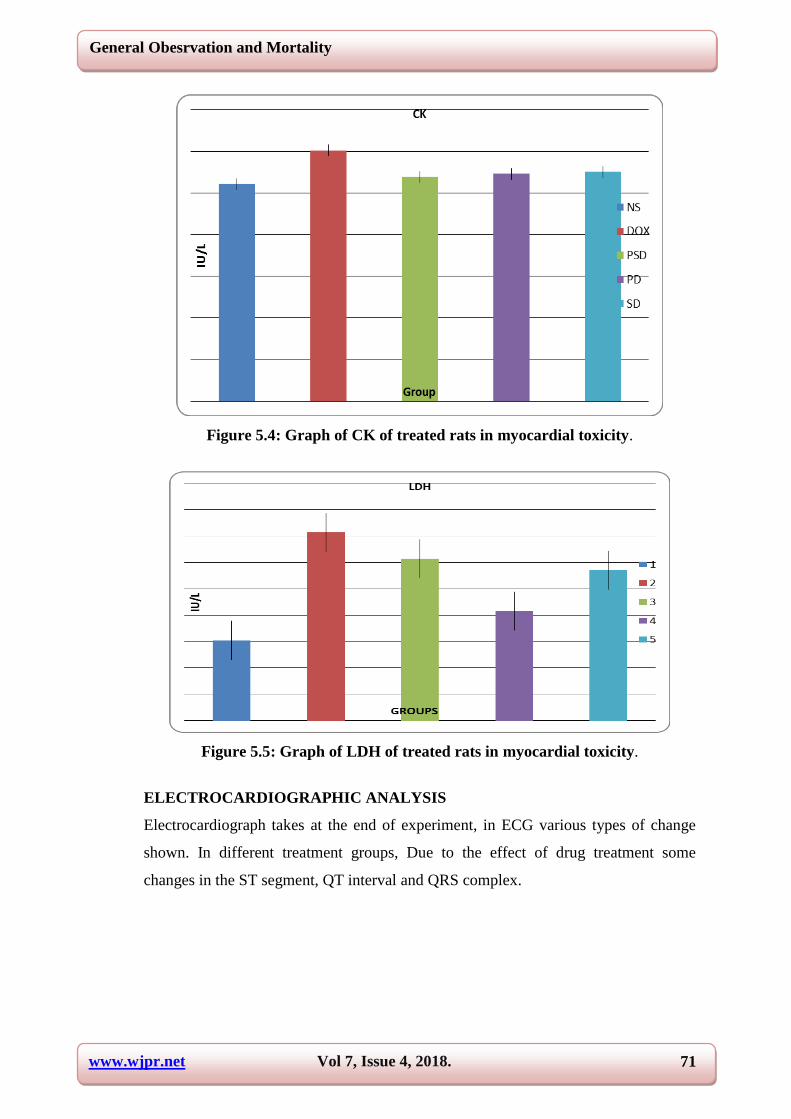
www.wjpr.net Vol 7, Issue 4, 2018. 71
General Obesrvation and Mortality
Figure 5.4: Graph of CK of treated rats in myocardial toxicity.
Figure 5.5: Graph of LDH of treated rats in myocardial toxicity.
ELECTROCARDIOGRAPHIC ANALYSIS
Electrocardiograph takes at the end of experiment, in ECG various types of change
shown. In different treatment groups, Due to the effect of drug treatment some
changes in the ST segment, QT interval and QRS complex.

www.wjpr.net Vol 7, Issue 4, 2018. 72
General Obesrvation and Mortality
Figure 5.6: Normal Saline (Ns) Treated Rat.
In the normal saline treated rat groups ECG consist of P, QRS and T waves. the onset
of arterial activation to the ventricular activation is calculated by PR interval. The
conduction pathways through the ventricules are represented by the QRS complex.
And at the time interval during the ventricular myocardium is depolarized and
isoelectric line is normal conditions is denoted by ST segment.
Figure 5.7: Doxorubicin (Dox) Treated Rat.
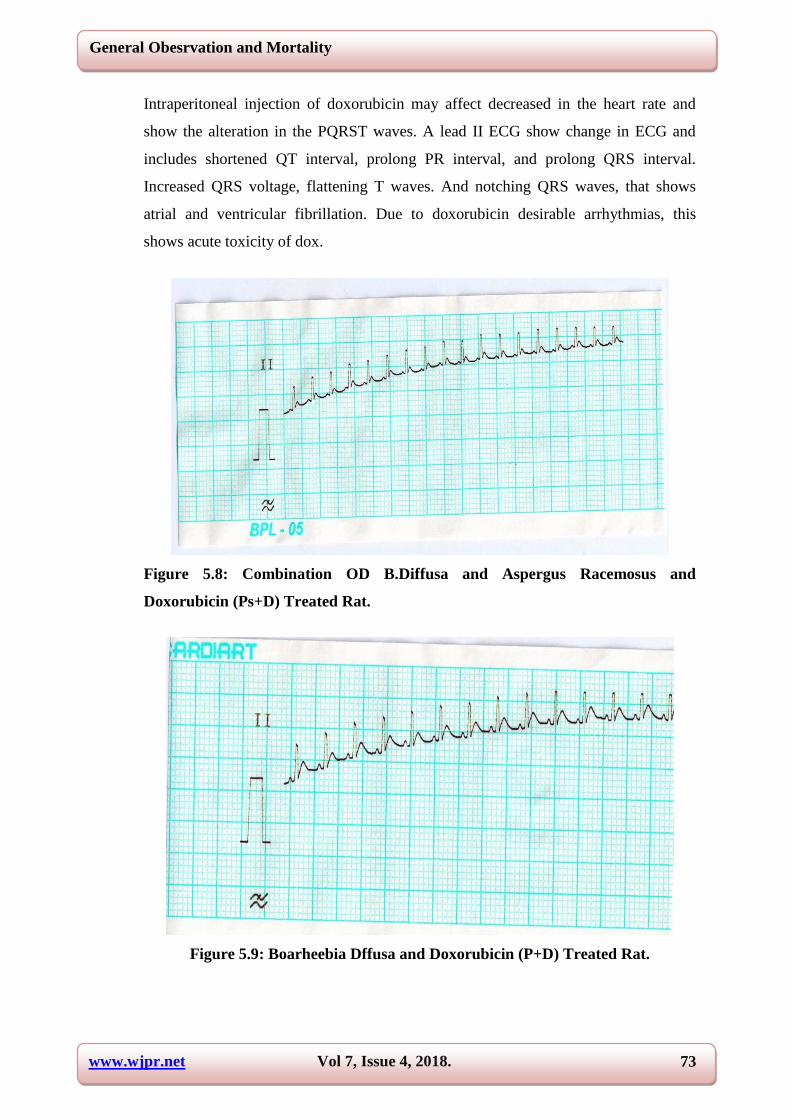
www.wjpr.net Vol 7, Issue 4, 2018. 73
General Obesrvation and Mortality
Intraperitoneal injection of doxorubicin may affect decreased in the heart rate and
show the alteration in the PQRST waves. A lead II ECG show change in ECG and
includes shortened QT interval, prolong PR interval, and prolong QRS interval.
Increased QRS voltage, flattening T waves. And notching QRS waves, that shows
atrial and ventricular fibrillation. Due to doxorubicin desirable arrhythmias, this
shows acute toxicity of dox.
Figure 5.8: Combination OD B.Diffusa and Aspergus Racemosus and
Doxorubicin (Ps+D) Treated Rat.
Figure 5.9: Boarheebia Dffusa and Doxorubicin (P+D) Treated Rat.

www.wjpr.net Vol 7, Issue 4, 2018. 74
General Obesrvation and Mortality
Figure 5.10: Aspergus Racemosus and Doxorubicin (S+D) Treated Rat.
Upon administration of herbal drug (orally), administration of combination of herbal
drugs (orally) and administration of doxorubicin in animal body. The herbal drug
normalizes the PQRST waves and hence atrial and ventricular fibrillation. Also the
heart rate was increased as compare to doxorubicin treated group.
Table 5.9: Heart Rate Analysis.
S.NO ANIMAL GROUP HEART RATE(beats/min)
01. NS 323.33±6.31
02 DOX 168.83±4.26
03 PS+D 252.84±4.96
04 P+D 261.16±7.80
05 S+D 258.15±5.91
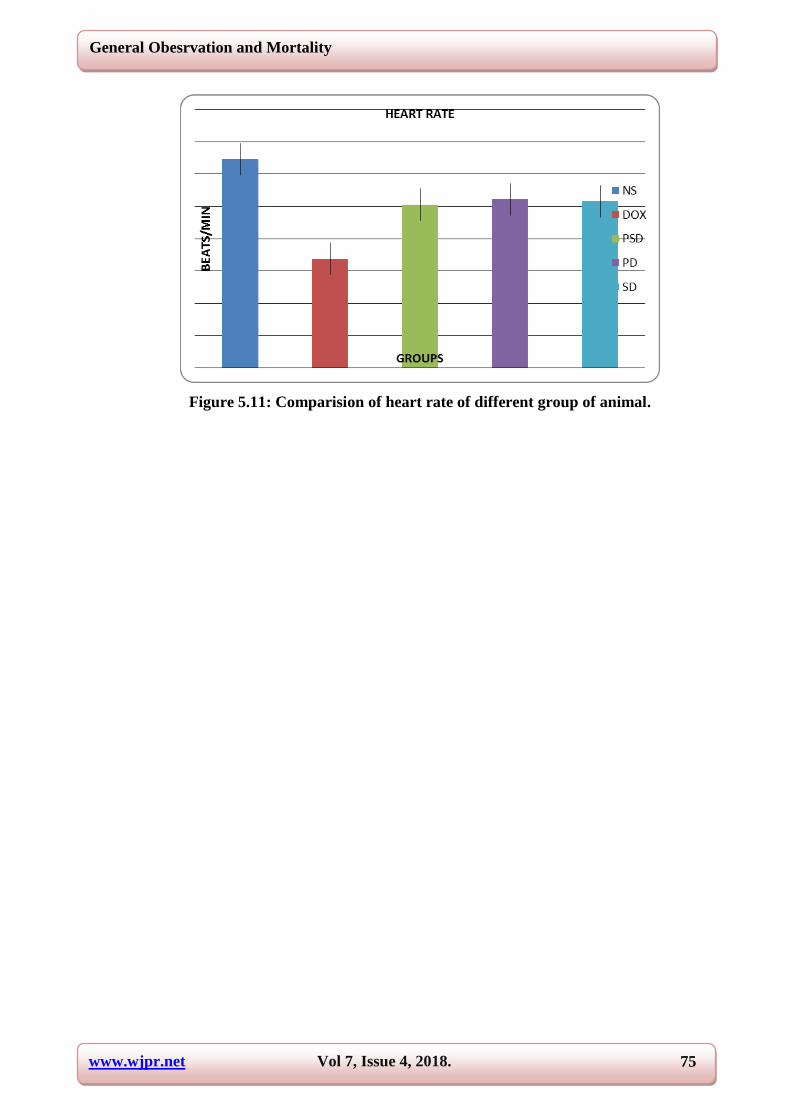
www.wjpr.net Vol 7, Issue 4, 2018. 75
General Obesrvation and Mortality
Figure 5.11: Comparision of heart rate of different group of animal.

www.wjpr.net Vol 7, Issue 4, 2018. 76
Discussion
CHAPTER 6
DISCUSSION
Doxorubicin-induced cardiac toxicity changes the group of the cardiomyocyte and
induces apoptosis, which is a potentially modifiable and preventable form of
myocardial tissue loss.[217]
This potentially novel mechanism is transient, but it may
be of a key importance to the ensuing heart failure. The results of this study have
confirmed that a single dose of dox (15 mg/kg) induces acute cardiac toxicity in rats.
This is in conformity with previous studies 218. Doxorubicin induced myocardial
toxicity have been well documented in experimental animal. The present study was
done to investigate the influence of Boerhavia diffusa and Asparagus Racemosus and
their combination on Dox-induced cardiotoxicity in albino rats. Following lines of
evidence can be emphasized from the present study.
1) General observation
A) In Dox treated group following changes were observed
The animal fur becomes scruffy.
Necrosis observed at the site of Dox injection.
There was 50% mortality in Dox treated group.
Animal becomes lazy.
B) In pretreated group with B. Diffusa, A. Racemosus and their combination.
No necrosis observed.
No any mortality.
No effect on animal activity.
2) Heart and body weight
The Dox treated rats showed increase in the heart weight and also decrease in body
weight. The body weight may be decreased due to the reduced intake of food. And the
heart weight may be increased due to the loss of myofibrils, increased number of
Liposomes, mitochondrial swelling, sarcoplasmic reticulum dilation. The gross
anatomically change of the heart treated with Doxorubicin showed a typical chronic
toxic response including cardiac hypertrophy and overall enlargement of heart. That
was determined by heart weight and ratio of heart weight and body weight.

www.wjpr.net Vol 7, Issue 4, 2018. 77
Discussion
3) Serum enzyme biomarker
The study reveals rigorous biochemical changes with oxidative injury in the cardiac
tissue after the chronic treatment with Doxorubicin (cumulative dose of 15mg/kg).
Doxorubicin is a well known cardiac toxic drug due to its ability. It will damaged
myocardial cells. As a result of this, ALP, Lactate Dehydrogenase (LDH) and
Creatine kinase (CK) was released into the blood stream and provided as the
diagnostic markers of myocardial tissue damage.[219,220,221]
The quantity of these
cellular enzymes present in the blood reflects the alteration in plasma membrane
integrity and permeability.
In present study the biochemical changes as well as oxidative damage in cardiac
tissue after the treatment of cumulative dose of 15mg/kg of body weight with
Doxorubicin. Doxorubicin is a cardiac toxic agent because of its destructive ability for
myocardial cells because of which ALP, Lactate Dehydrogenase (LDH) and
Creatinine Kinase (CK) were released into blood stream and serve as the diagnostic
biomarker of myocardial tissue damage. The amount of these cellular enzymes in
blood effects the alteration in plasma membrane integrity and permeability.
In this study, Doxorubicin treated shows the significant elevation in the level of these
diagnostic biomarker enzymes (ALP, CK and LDH). Moreover, elevated levels of
these enzymes are indicator of the severity of Doxorubicin induced cardiotoxicity.
The prior administration of combination of B. Diffusa and A. Racemosus showed
significant reduction in Doxorubicin induced elevated serum biomarker enzymes.
This reduction in the enzyme level confirms that combination of the same is
responsible for maintenance of normal structural cardiac myocytes.
4) Electrocardiographic parameters
Electrocardiograph abnormalities are the main criteria generally used for the definite
diagnosis of the myocardial injury. The study shows a significant variation of ECG
patterns on Dox administered rats as compared with the normal control rats. The
attributed findings were elevation of the ST segment, reduction in the P waves, in
QRS complex and R-R interval. In addition there was a prolongation of the QT
interval. Furthermore ECG changes are the indicators of the severity of Doxorubicin
induced the myocardial damage and which is in line with an earlier report. The
successive loss of cellular membrane damage due to oxidative stress might be
www.wjpr.net Vol 7, Issue 4, 2018. 78
Discussion
characterized by ST elevation. Treatment of combination of B. diffusa showed a
protective effect against Doxorubicin induced changed ECG parameter and eliminated
the acute fatal complication by protecting the cell membrane damage.
The data of the present study clearly show that combination of B. Diffusa and A.
Racemosus, modulated most of the electrophysiological, biochemical and
histopathological parameters were maintained to near normal status in Dox treated
rats, suggesting the beneficial action of combination of B. Diffusa and A. Racemosus
as a cardiac protective agent.

www.wjpr.net Vol 7, Issue 4, 2018. 79
Summery and Conclusion
CHAPTER 7
SUMMERY AND CONCLUSION
In the present study we observed the effect of combination of B.Diffussa and A.
Racemosus on doxorubicin induced cardio-toxicity in rats. The result suggest that in
doxorubicin treated animals, significant decrease in the body weight and increased in
the heart weight and heart and body weight takes place. There was 50% mortality
found in the doxorubicin group. but in the pre-treated group no mortality found. And
body weight increased and heart weight decreased, the observation in the results
suggests that the combination of B.diffusa and A.racemosus significant the dox
induced free radicals mediated cardio-toxicity.
The data collected in the present study show that the cumulative administration of
doxorubicin increased the serum cardio-toxicity indices ALP, CK, LDH activity.
According to experiment result the combination of B.Diffusa and A.Racemosus
protect the myocardium from doxorubicin mediated damage as evident from the near
normal value of these markers enzymes. This can be show as higher oxidative stress
in the cardiac tissue from rats following a cumulative dose of doxorubicin and this
enhance oxidant injury was prevented by combination therapy.
Electrocardiograph abnormalities are the main criteria generally used for the define
diagnosis of myocardial injury. The experiment show signification alterations of ECG
pattern were observed in the doxorubicin administrated rats as compare to normal
control rats. The characteristic finding were elevation of ST segment, reduction of P
segment, QRS complex and R-R interval. In addition there was prolongation of QT
interval. The consecutive loss of cellular membrane damage due to oxidative stress
might be characterized by the ST elevation, combination of b.diffusa and a.recimosus
administration shown a protective effect agenised the doxorubicin induced alter ECG
parameters and eliminated the acute fatal complication by protecting the cell
membrane damage.
The enhance generation of oxygen radicals may directly damage cellular structure as
seen in histological slides. Pre treatment with combination of B.Diffusa and
A.Racemousu effectively inhibits doxorubicin induced cardiac damage by reversal of
infiltration of inflammatory cell and fragmentation of myofibrils.
www.wjpr.net Vol 7, Issue 4, 2018. 80
Summery and Conclusion
Collectively these all parameters as electrocardiographic, biochemical, result provide
a possible and potential cardioprotection against doxorubicin cardio-toxicity.
Finally we concluded that the cardio-toxicity induced by the doxorubicin is in
relationship with oxidative stress and biochemical changes in heart cells and tissues.
Combination of B.Diffusa and A. Racemosus has shown to be most effective in
functional recovery of the heart and restoring the biochemical and histopathological
alteration which may be associated with its potent antioxidant property. This
experiment suggested that combination of B. Diffusa and A. Racemousu may be
considered as a potentially useful drug in the combination with doxorubicin to limit
free radical mediated the organ injury. Additionally molecular level of the
investigation is to be done using different animal’s modal and using different
biochemical parameters to assess the possible mode of action of B.Diffusa and A.
Racemosus as cardio-protective agent.

www.wjpr.net Vol 7, Issue 3, 2018. 81
References
CHAPTER 8
REFERENCES
1. Upaganlawar A, Gandhi H, R Balaraman. Isoproterenol induced Myocardial
infarction: Protective role of natural products. J. Pharaco. Toxico., 2011; 6(1):
1-17.
2. Bovelli D, G Plataniotis, F Rolia. Crdiotoxicity of Chemotherapeutic agent. Anals
of Oncology, 2010; 21(5): 277-282.
3. Gharib I, Burnett AK. Chemotherapy-induced cardiotoxicity: Current practice and
prospects of prophylaxis. Eurp. J. Heart Failure, 2002; 4: 235-242.
4. Nagy l, Szabo F, Ivanyi J. A method for detection of Doxorubicin-induced
cardiotoxicity: Flow-mediated vasodilation of the brachial artery. Exp. Clin.
Cardiol, 2001; 6(2): 87-92.
5. Lipshultz SE, Alvarez J A, Scully RE. Anthracycline related cardiotoxicity in
survivors of childhood cancer. Educ. Heart, 2008; 94: 525-533.
6. Arya V, Gupta VK. Review on some cardioprotective plants from ayurveda. Int. J.
Res. Ayur. Parma, 2011; 2(1): 80-83.
7. Blum RH, Carter SK: Adriamycin: a new anticancer drug with significant clinical
action. An Intern Med, 1974; 80: 248–258.
8. Chabner BA, Ryan DP, Paz-Arez L, Gracia-Carbonero R, Calabresi P: Anti
neoplastic agent. In: Goodman & Gilman’s The Pharmacological Basis of
Therapeutics. Ed. Hardman JG, Limbird LE, Gilman AG, McGraw-Hill Co
Newyork, USA, 2001; 1390–1469.
9. Hrdina R, Gersl V, Simunek T, Machackova J, Adamcova M: Anthracycline-
induced cardiomyopathy. Act Medi, 2000; 43: 75–80.
10. Singal PK, Iliskovic N: Doxorubicin-induced cardio -myopathy. N Engl J Med,
1998; 339: 900–905.
11. Arola OJ, Saraste A, Kallajoki M, Parvinen M, Voipio-Pulkki LM: Acute dox
cardio toxicity in-volves cardiomyocyte apoptosis. Can Res., 2000; 60:
1790–1792.
12. Baker KM, Booz GW, and Dostal DE: Cardiac actions of angiotensin II: role of an
intracardiac rennin-angiotensin system. Annu Rev Physiol, 1992; 54: 227–241.

www.wjpr.net Vol 7, Issue 3, 2018. 82
References
13. Balachandar AV, Malarkodi KP, Varalakshmi P: Protec-tive role of DL -lipoic
acid against adriamycin-induced cardiac lipid per oxidation. Human Exp Toxicol,
2003; 22: 248–255.
14. Billingham ME, Mason J W, Daniels J R: Anthracycline cardio myopathy
monitored by morpho-logical changes. Can Treat Rep., 1978; 62: 864–872.
15. Blum RH, Carter SK: Adriamycin: a new anticancer drug with significant medical
activity. Ann Intern Med, 1974; 80: 249–259.
16. Boucek RJ Jr, Miracle A, Anderson M, Engelman R, Atkinson J, Dodd D:
Persistent effects of doxorubicin on cardiac gene expression. Cardiol J Moll Cell,
1999; 31: 1435–1446.
17. Buyukokuroglu ME, Taysi S, Buyukavci M: Prevention of acute Adriamycin
cardio toxicity by dantro-lene in rats. Huma Exp Toxicol, 2004; 23: 250–256.
18. Chabner BA, Ryan DP, Paz-Arez L, Gracia-Carbonero R, Calabresi P: Anti
neoplasticagents. Goodman and Gilman’s: The Pharmacol Basis of Therapeutics.
Ed. Hardman J G, Limbird L E, Gilman A G, McGraw-Hill Co, USA, 2001;
1389–1459.
19. Potemski P, Polakowski P, Wiktorowska-Owczarek AK, Owczarek J, P³u¿añska
A, Orszulak-Michalak D: Ami-fostine improves hemodynamic parameters in
doxo-rubicin-pretreated rabbits. Pharmacol Rep, 2006; 58: 966–972.
20. Koti BC, Vishwanathswamy AHM, Thippeswamy AHM. Cardioprotective effect
of Lipistat against doxorubicin induces myocardial toxicity in albino rats. Ind. J.
Exp. Bio., 2009; 47: 41-46.
21. Abd-Alah AR, Al-Majed AA, Mostafa AM, Din AG. Protective effect of Arabic
gum against cardiotoxicity induced by doxorubicin in mice: A possible
mechanism of protection. J. Bioche. Mol. Toxicol, 2002; 16: 254.
22. Hanna H A, Fathia M, Gamal A E, Senot H D. Cardioprotective activity of
melatonin and its novel synthesized derivatives on doxorubicin induced
cardiotoxicity. Bioorg. Med Chem., 2005; 13: 1849.
23. Siveski-Iliskovic N, Hill M, Chow DA, and Singal PK. Probucol protects against
Adriamycin cardiomyopathy without interfering with antitumor effect, 1995; 91:
10-15.
24. Halliwell B. Ascorbic acid in the prevention and treatment of cancer. Alter. Med.
Rev., 1996; 3: 174-186.

www.wjpr.net Vol 7, Issue 3, 2018. 83
References
25. Ivanova D, Gerova D, Chervenko T. Polyphenols and antioxidant capacity of
Bulgarian medicinal plants. J. Ethnopharmacol, 2005; 97: 145-150.
26. Olaleye M.T., Akinmoladun A C., Akindahunsi A.A. Antioxidant activity and
hepatoprotective property of leaf extracts of B.diffusa L. against acetaminophen-
induced liver injure in rats. Food and Chem. Toxicology, 2010; 48(8-9):
2201–2205.
27. Punarnavine. Comparative Toxico genomics Database. Mount Desert Island Bio
Lab., 2013.
28. Manu K.A., Kuttan G. Punarnavine induces apoptosis in B16F-10 melanoma cells
by inhibiting NF-kappa B signaling. Asian Pacific Journal of Cancer Prevention,
2009; 10(6): 1031–1037.
29. Sreeja S., Sreeja S. An in vitro study on antiproliferative and antiestrogenic effects
of Boerhaavia diffusa L. extracts. J. Ethno. Pharmacol, 2009; 126(2): 221–225.
30. Manu K.A., Kuttan G. Immuno modulatory activities of Punarnavine, an alkaloid
from Boerhaavia diffusa. Imm.pharmacol and Immtoxicol, 2009; 31(3): 377–387.
31. Sohni Y R., Kaimal P, Bhatt R M, The antiamoebic effect of a crude drug
formulation of herbal extracts against Entamoeba histolytica in vitro and in vivo.
Ethphrcol, 1995; 45(1): 43–52.
32. A. Prathapan, M.K Singh, D.R Sobankumar, A. Sundaresan & K.G Raghu. Anti
peroxidative, free radical scavenging and metal chelating activities of B.diffusa L.
Jou of Food Biochem, 1995; 35: 1548–1554.
33. V.P Vineetha, A. Prathapan, R.S Soumya & K.G Raghu. Arsenic Trioxide
Toxicity in H9c2 Myoblasts-Damage to Cell Organelles and Possible
Amelioration with Boerhavia diffusa. Cardiovascular Toxicology, 2012.
34. Asparagus racemosus--ethnopharmacological evaluation and conservation needs.
[Review] [77 refs] Bopana N. Saxena S. Jou. Ethnopharmacol, 2007; 110(1):
1-15, 1.
35. Pouna P, Simone BA, Gouverneur G, Tariosse L. Development of the model of rat
isolated perfused heart for the evaluation of anthracycline cardiotoxicity and its
circumvention. British J. Pharmacol, 1996; 117: 1593-1599.
36. Jensen R A, Acton E M, Peters J H. Dox cardiotoxicity in the rat: Comparison of
ECG, transmemb. potential and Stru effects. J. Cardiovasc. Pharmacol, 1984; 6(1):
180-200.

www.wjpr.net Vol 7, Issue 3, 2018. 84
References
37. Thippeswamy AHM, Shirodkar A, Koti BC. Protective role of Phyllanthus Niruri
extract in doxorubicin induced myocardial toxicity in rats. Ind. J. Pharmacol,
2011; 43(1): 31-35.
38. Swamy AV, Gulliya S, Thippeswamy A. Cardioprotective effect of curcumin
aginst doxorubicin-induced myocardial toxicity in albino rats. Ind. J. Pharmacol,
2012; 44(1): 73-77.
39. Karim S, Bhandari U, Kumar H. Doxorubicin induced cardiotoxicity and its
modulation by drugs. Ind. J. Pharmacol, 2001; 33: 203-207.
40. Shafik AM, Khodeir MM, Fadel MS. Animal study of anthracycline induce
cardiotoxicity and Nephrotoxicity and evaluation of protective agents. J. Cancer
Sci. Ther., 2011; 3(5): 096-103.
41. Olson RD, Mushlin PS, Brenner DE. Doxorubicin cardiotoxicity may be caused
by its metabolite, doxorubicinol. Proc. Natl. Acad. Sci., 1988; 85: 3585-3589.
42. Minotti G, Menna P, Anthracyclines: Molecular advances and pharmacologic
developments in antitumour activity and cardiotoxicity. Pharmacol. Rev., 2004;
56: 184-229.
43. Jaenke R S, Trouet A. Cardio toxicity and comparative pharmacokinetics of six
anthracyclines in the rabbit. Can. Res., 1980; 40: 3531-3536.
44. Bernard Y, Reibiro N, Frederic T. Flavaglines alleviate Doxorubicin
cardiotoxicity: Implication of Hsp27. Plos One., 2011; 6(10): 1-9.
45. Raskovic A, Stilinovic N, Kolarovic J. The protective effects of Silymarin against
Dox-induced cardio toxicity and hepato toxicity in rats. Mol., 2011; 16:
8600-8613.
46. Rath SK, Shinde A, Gahunge P. Review of antioxidant activity of Rasayana herbs
described in Ayurveda. Int. J. Ayur. Herbal Med., 2012; 2(1): 202-217.
47. Arola OJ, Saraste A, acute dox cardio toxicity involves cardio myocyte apoptosis.
Can Res., 2000; 60: 1788-1792.
48. Nagy l, Szabo F, Ivanyi J. A method for detection of Doxorubicin-induced
cardiotoxicity: Flow-mediated vasodilation of the brachial artery. Exp. Clin.
Cardiol., 2001; 6(2): 87-92.
49. Arya V, Gupta VK. Review on some cardioprotective plants from ayurveda. Int. J.
Res. Ayur. Parma., 2011; 2(1): 80-83.
50. Ikeda Y, Aihara K. Androgen receptor counteracts doxorubicin-induced
cardiotoxicity in mice. Mol. Endocrinol, 2010; 24(7): 1337-1348.
www.wjpr.net Vol 7, Issue 3, 2018. 85
References
51. Dolci A, Dominci R, Cardinale D. Biochemical markers for prediction of
chemotherapy-induced cardio toxicity. Am. J. Clin. Pathol., 2008; 130: 686-695.
52. Xin YF, Zhou G, Chen Y. Protective effect of Lycium barbarum on doxorubicin-
induced cardiotoxicity. Phytother. Res., 2007; 21: 1020-1024.