rapport abkhazie ang - médecin sans frontières...abkhazia is a caucasian territory on the shores...
TRANSCRIPT
Abkhazia Old and frail
in the shadow of the embargo
Report
Released by Médecins Sans Frontières in december 2002
Document en provenance du site internet de Médecins Sans Frontièreshttp://www.msf.fr
Tous droits de reproduction et/ou de diffusion, totale ou partielle, sous quelque forme que ce soit, réservés pour tous pays, sauf autorisation préalable et écrite de l’auteur et/ou de Médecins Sans
Frontières et/ou de la publication d’origine. Toute mise en réseau, même partielle, interdite.

Abkhazia is a Caucasian territory on the shores of the Black Sea.Ravaged by war ten years ago, the embargo imposed by Russia andGeorgia continues ever since. The international community will notconsider any development activities in Abkhazia until there is lastingpeace…
Old and Frail in the Shadow of the Embargo
M É D E C I N S S A N S F R O N T I È R E S – D E C E M B E R 2 0 0 2
Abkhazia

…Yet the 18,000 people, i.e. probably one-tenth of the inhabitants,who live on Abkhazian territory in extremely precarious conditions,are in need of emergency humanitarian aid. Today, most of theemergency assistance is provided by Médecins Sans Frontières andInternational Committee of the Red Cross. International presence isgravely inadequate to respond to the needs of this strickenpopulation.This report describes the living conditions of the indigent people inAbkhazia and their emergency needs. It is based on the experiences,as well as the social and medical data, collected by the MédecinsSans Frontières teams.The objective of this report is to draw attention to the disastrousconsequences of the embargo for the indigent population and toraise increased aid from donors and aid organisations.
Text: Laurence Binet
All the photographs in this document weretaken by Serge Sibert during his travels in
Abkhazia in Autumn 2001. copyright S. Sibert / Cosmos.

3A b k h a z i a – D e c e m b e r 2 0 0 2
4
6
9
21
22
c o n t e n t s
Abkhazia in PurgatoryA land of plenty… scarred by History
Médecins Sans Frontières and Indigent people
Life as an Indigent in Abkhazia…10 Access to healthcare14 Housing and Food18 Access to psychological support
Conclusion
MSF in the Caucasus
Abkhazia( )
Russia( )
Georgia( )
The map presented in this document do not imply the expression of any opinion whatsoever on the part ofMSF concerning the legal status of any country, territory city or area or of its autorities or concerning thedelimitations of its frontiers, boundaries or denomination of the place.
Abkhazian territory
A b k h a z i a – D e c e m b e r 2 0 0 24
AAbkhaziabkhaziaIIN PUN PURRGAGATTORORYY
The present borders of Abkhazia territory werefixed during the first years of the Soviet Unionand delimit a area of 8600 km2, bordered by theCaucasus Mountains to the North and the BlackSea to the South, by the Georgian Transcaucasusplains to the west and by the region of Krasnodarto the east where the Caucasus gradually givesway to the plains of Southern Russia.Abkhazia, with its Mediterranean climate, isknown as a land of plenty in a part of the worldwhere the climate is harsh. This region hadalways been looked upon with envy: it is theprivileged axis of communication betweenMoscow and the southern Caucasus, has a longcoastline, a natural fortification line, and is rich inagricultural, mining and tourist resources. In July 1992, the Abkhazian parliament
unilaterally declared the sovereignty ofAbkhazia. Georgia, which was itself in the gripof a civil war, reacted by occupying Abkhazianterritory as far as Sukhumi. The Russian troopsdrove the Georgians back across the IngouriRiver into the Georgian plains.A cease-fire was agreed in May 1994 underthe auspices of the UN. The Moscowagreement set up a peace-keeping force ofRussian troops responsible for neutralising anarea of 20 km across the border between thetwo part in conflit. United Nations observerswere also deployed.The war had left an estimated 10,000 dead in13 months and resulted in the fleeing of240,000 (according to UNHCR) Georgiansliving in Abkhazia to Georgia. An agreementwas also signed between the Abkhazians, theGeorgians and the United Nations HighCommissioner for refugees (UNHCR) and theRussian Federation so as to facilitate thevoluntary return of refugees to Abkhazia. Thiswas not followed by any lasting result.A coordinating council, led by a specialrepresentative to the United Nations Secretary inGeorgia, with representatives from the OSCE
Marked with centuries of invasion and subjectedto various political, cultural and religiousinfluences, this region, like the whole of theCaucasus, found itself under the guardianship ofthe Tsarist empire at the end of the 19th century.The empire strived to erase the cultural andhistorical specificities of Abkhazia, provokingstrong nationalist claims. At the same time inGeorgia, a strong nationalist movement wasdeveloping with the aim of breaking free fromRussian rule.When the Bolshevik revolution overthrew theTsarist empire in 1917, the Caucasusexperienced a brief period of political upheaval.This led to the birth of the Republic of Georgiawhich sought to keep Abkhazia within itsborders, despite the demands of independenceby the Abkhazian nationalist. Meanwhile, thenew government in Moscow had no intention of
giving up the territories inherited from the Tsars.In 1922, the Red Army regained entire control ofthe southern region.In 1931, the Soviet constitution grantedAbkhazia the status of an autonomous republicwithin Georgia. This territorial decree wasaccompanied, as in all of the Soviet Union, by agrowing communitarisation of the elites in theregion.In 1991, after the collapse of the Soviet regime,Georgia became independent. The regionalnomenclatures could not agree on the status ofAbkhazia.
A land of plenty…
The price ofindependence
…scarred by History
This piece on the historical situation is intended to help the reader understand the context in which MSF undertakes its mssions in Abkhazia. It does not represent
in any way that MSF has taken a position in favour of one of the parties.

5A b k h a z i a – D e c e m b e r 2 0 0 2
(Organization for Security and Cooperation inEurope), the Russian Federation, France,Germany, the United States and the UnitedKingdom, has been attempting to facilitatenegotiations between the two parties since 1997without signifiant success.In the southern Abkhazian border region of Gali,the insecurity that continues to prevail restrictsthe humanitarian aid provided to its inhabitants.In October 2001 and then in April 2002,fighting broke out in the upper reaches of theKodori valley, situated about fifty kilometresfrom the capital and occupied by the Georgians.The population who have not yet recoveredfrom the disastrous effects of the 1992-94conflict, feel constantly under threat.
Abkhazia has a current population of 200,000 2
inhabitants, the majority of whom areAbkhazians.Abkhazia is subjected to a naval and land tradeembargo, imposed by its two neighboursGeorgia and Russia, which prevents anyeconomic development. The absence of a peaceagreement and its international non-recognitionas a state prevents it from benefiting from anyform of aid for development.A small clandestine and seasonal economy ofselling mandarins and hazelnuts along theborder, although still officially closed, providesthe bare minimum to survive for a few people.Trade in timber, iron and coal is also limited toclandestine transactions. The remaining tourisminfrastructure, which used to be a veryimportant source of income before the war,today mainly caters for a few Russians inholiday villages around Sukhumi and Gagra.Although Moscow maintains an embargo onAbkhazia, it has granted Russian Federationcitizenship to Abkhazian nationals was launched,leading some to believe that the country mayone day be integrated into the Federation.In the meantime, the majority of the populationthat does not have the means to leave thecountry lives in poverty with no future prospects,dependent upon the limited assistance of a fewaid organisations.1 And also for the Georgian population displaced from
Abkhazia who continue to live in intolerable conditions eight
years after the conflict.2 This figure is an approximation generally accepted by
organisations working in Abkhazia; it does not represent a
political opinion on the part of MSF.
The collapse of the Soviet system, the war anddiplomatic isolation have had terribleconsequences on the population of Abkhazia 1.Before the war, Abkhazia had a population of525,000 inhabitants (according to the census of1989) which included 46% of Georgian ethnicorigin, 18% Abkhazian, 16.5% Russian, but alsoArmenian, Adjar, Juive, Estonian, Ukrainian, andGreek. According to official Abkhazian figures,
The populationfaced a socio-economicdisaster

6A b k h a z i a – D e c e m b e r 2 0 0 2
S ingle mothers, the elderly, thebedridden, those suffering fromchronic illness, or invalidity, and large
families in economic difficulty – these are thecriteria derived from the Soviet indigentclassification system used for the people whobenefit from the Health Access Programmes(HAP) run by Médecins Sans Frontières since1993 2.After organising a regular supply of drugs,Médecins Sans Frontières began rehabilitatingand running the Pushkin health centre inSukhumi. In these small premises, two doctors,a pharmacist and a secretary providedhealthcare, a sympathetic ear and freemedication to all the indigent people whoturned up, often having been sent by an MSFsocial worker. In 1999, the same facilities were set up inGagra, Tkvarcheli and Gali for peoplereceiving food aid from the ICRC canteens.
In the spring of 2000, a social worker startedworking in Gagra. Then from December2000, a dozen MSF social workers workedfor six months in seven regions of Akbhaziaand identified individuals who had no accessto healthcare. Each person identifiedreceived a card that gave them access to freehealthcare in the MSF assisted healthfacilities. This exchange of informationbetween the two organisations continues ona daily basis.In September 2002, MSF and the ICRC hadthus registered 18,700 indigent people,roughly one in ten inhabitants ofAbkhazia, including 39% of whom livein the capital, Sukhumi. More than 1,400of them cannot leave their homes, manybedridden, unable to survive without outsidehelp.2 The criteria were defined in agreement with the Ministry of
Health of Abkhazia.
Médecins Sans Médecins Sans FFrontières androntières andIINNDDIIGGEENT PENT PEOPLEOPLE
Vulnerable identified by ICRC 2001
0
10002000
30004000
50006000
70008000
GAG
RA
GUDAU
TA
SUKH
UMI
GULR
IPSC
H
TKVA
R
OTC
HGAL
I
7A b k h a z i a – D e c e m b e r 2 0 0 2
Tkwarc
heli
Otcham
chira Gali
Gulrips
ch
Sukh
umi
Gagra
Gudau
ta
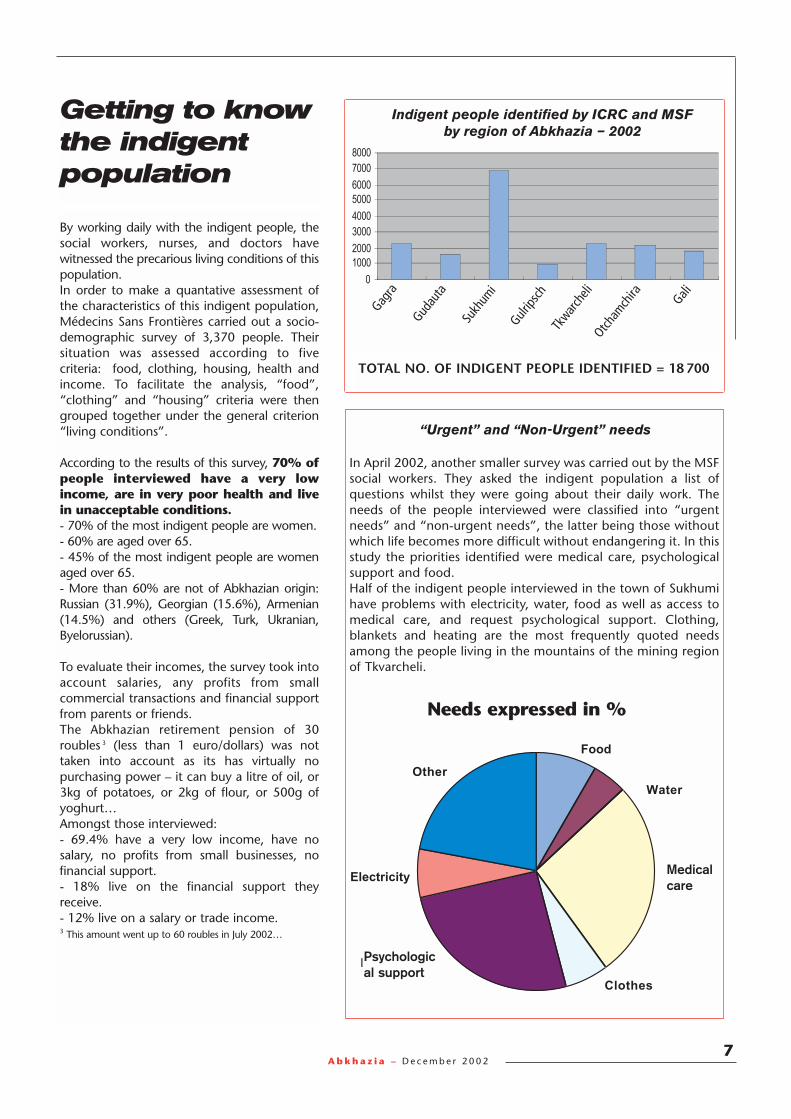
TOTAL NO. OF INDIGENT PEOPLE IDENTIFIED = 18 700
Indigent people identified by ICRC and MSF by region of Abkhazia – 2002
Getting to knowthe indigentpopulation
By working daily with the indigent people, thesocial workers, nurses, and doctors havewitnessed the precarious living conditions of thispopulation.In order to make a quantative assessment ofthe characteristics of this indigent population,Médecins Sans Frontières carried out a socio-demographic survey of 3,370 people. Theirsituation was assessed according to fivecriteria: food, clothing, housing, health andincome. To facilitate the analysis, “food”,“clothing” and “housing” criteria were thengrouped together under the general criterion“living conditions”.
According to the results of this survey, 70% ofpeople interviewed have a very lowincome, are in very poor health and live in unacceptable conditions.- 70% of the most indigent people are women.- 60% are aged over 65.- 45% of the most indigent people are womenaged over 65.- More than 60% are not of Abkhazian origin:Russian (31.9%), Georgian (15.6%), Armenian(14.5%) and others (Greek, Turk, Ukranian,Byelorussian).
To evaluate their incomes, the survey took intoaccount salaries, any profits from smallcommercial transactions and financial supportfrom parents or friends.The Abkhazian retirement pension of 30roubles 3 (less than 1 euro/dollars) was nottaken into account as its has virtually nopurchasing power – it can buy a litre of oil, or3kg of potatoes, or 2kg of flour, or 500g ofyoghurt…Amongst those interviewed:- 69.4% have a very low income, have nosalary, no profits from small businesses, nofinancial support.- 18% live on the financial support theyreceive.- 12% live on a salary or trade income.3 This amount went up to 60 roubles in July 2002…
In April 2002, another smaller survey was carried out by the MSFsocial workers. They asked the indigent population a list ofquestions whilst they were going about their daily work. Theneeds of the people interviewed were classified into “urgentneeds” and “non-urgent needs”, the latter being those withoutwhich life becomes more difficult without endangering it. In thisstudy the priorities identified were medical care, psychologicalsupport and food.Half of the indigent people interviewed in the town of Sukhumihave problems with electricity, water, food as well as access tomedical care, and request psychological support. Clothing,blankets and heating are the most frequently quoted needsamong the people living in the mountains of the mining regionof Tkvarcheli.
“Urgent” and “Non-Urgent” needs
% of needs
Illness
Other
Electricity
Psycho supp
Clothes
Water
Food
Needs expressed in %
Medicalcare
Psychological support
8A b k h a z i a – D e c e m b e r 2 0 0 2
Louisa’s flat is gradually emptying. Located in a decrepit building in the old mining town of Tkvarcheli, all that remains is a stove, an old sewing machine, a pile of clothes that is turningmouldy and a few books. The 81-year-old woman of Greek origin was married to a Georgian whodied during the war. Her children have left the country. They are not in touch with her. “When myson left, he told me to sell all my belongings to survive and that is precisely what I did. I sold myblanket yesterday. Today I am drying this cloth to sell it. I’m keeping the sewing machine as a lastresort…and I still have a few books left…I used to be a librarian. I come from a wealthy familyand I like nice things. I used to be a good housewife. I have never been poor.” Today, Louisasurvives thanks to the daily meal provided by the ICRC. She spends part of her day lying down because she gets dizzy. The flat smells musty. Electricityand water are only supplied at intervals. “I don’t need anything apart from new glasses.” shesighs. “Mine aren’t strong enough. I can no longer read.”
Olga, an 80 year-old woman of Russian origin born in Abkhazia, has no relatives. She is blindand paralysed in both legs and survives on the occasional bowl of soup her neighbour bringsher. When the Médecins Sans Frontières team visited Olga for the first time, the door waslocked. Olga had to pass the key through the window. Inside, the smell was unbearable: theroom was filthy and the floor was covered in mud. There were rats scampering around the room.There was no water, electricity or heating. Olga’s legs were swollen and infected. She keptrepeating that her only wish was to die. Olga was very conscious of her appalling state. As agynaecologist-obstetrician, she brought half the town of Sukhumi into the world. “But I did nothave any children of my own”, she sighed, “and today I don’t have anyone to take care of me”.The teams of Médecins Sans Frontières, ICRC and Première Urgence made arrangements totake care of her.
Louisa& Olga

9A b k h a z i a – D e c e m b e r 2 0 0 2
Life as an Life as an IndigentIndigent
IIN ABN ABKKHAHAZZIAIAThe essential needs are acces to healthcare, accomodation, food and psychological help.

A b k h a z i a – D e c e m b e r 2 0 0 2
Nine years ago, at the end of the war and after her studies at Moscow University, DoctorIrina Achouba returned to her country to take the helm of the neurology department atSukhumi’s “City Hospital”, the only department of its kind in the whole of Abkhazia. Shefound the hospital in a pitiful state and it has remained as such due to the lack of means to repair it. Leaking pipes mean that the toilets cannot be used, so the nurses pass aroundplastic washbowls to be used as bedpans by patients. The latter take turns to sleep on thefew proper beds with a mattress. The others make do with tattered mattresses on boards; a nightmare for patients who are physically handicapped and the majority of whom, agedbetween 50 and 80, suffer from serious cardiovascular problems. With no money to buy the drugs prescribed by their doctor and which the hospital has nomeans of providing, the patients arrive at the last minute when there is little chance of curingthem. “Even those who receive a Russian pension are unable to pay for the treatments. Isometimes pay for them myself,” says Doctor Irina who does her best to carry on providingcare, in spite of not having the means: “I do what I can. I’m the neurologist, psychologist and general practitioner rolled into one. I try to give them some support…” The patients dieat the hospital or spend their last days at home. Only those who are indigent, and who haveno relatives, profit from staying at the hospital – the bustle of staff and visitors pacing up anddown fills their loneliness…
10
Access to Healthcare

11A b k h a z i a – D e c e m b e r 2 0 0 2
72-year-old Raïssa is bedridden. She can no longer moveher legs or her left arm. Ten days ago this woman, wholives a dilapidated flat in Ochamchira, shouted,“Something’s wrong, I’m not well.” Her neighbour foundher partially paralysed and unable to speak having suffereda stroke. Raïssa is Russian. She was married to a Russianwho passed away. Her only son lives in Russia and is nolonger in touch with her. Her neighbour who lives on thefloor above with her son, who suffers from tuberculosis,takes care of her as much as she possibly can. “As longas I am here, she will not die of hunger”, she assures. “But I have neither the energy or the skills to give her thecare she needs. Yesterday, when I needed to turn her over,I had to ask a soldier who was walking by to help me. I put cooking oil on her bedsores to soothe them…I don’t have anything else.”
The eldery inpoor health…
…Faced with acrumblinghealth system…
According to the study carried out byMédecins Sans Frontières, 81% of theindigent people interviewed suffer from achronic illness and are therefore in need ofregular medical care.The diseases that MSF doctors encountermost frequently are: hypertension andcardio-vascular diseases, respiratory diseases,gastro-intestinal diseases, bacterial infectionsas well as certain musculo-skeletal diseases.These diseases represent 70% of thosediagnosed among the indigent population.
Having fallen apart after the collapse of theSoviet system, then ravaged by war andasphyxiated by the trade embargo, theAbkhazian health system struggles to function.Some of the hospitals and health centres weredamaged or destroyed during the conflicts.Only a few of them have been rehabilitated.Given the lack of resources, only a handful areproperly maintained.There is an alarming lack of equipment anddrugs. The main pharmacy is not supplied.Apart from the donations from relieforganisations, the only drugs available arefrom private supply circuits and the indigentpopulation cannot afford them. There are not enough medical staff andmany of them are getting on in years. Non-Abkhazian doctors and nurses who weredriven away during the war have not beenreplaced. Young people who are studyingabroad hesitate to return to a country whichseems to offer a future without prospects. Itis therefore common to find doctors overthe age of 80 as managers of hospitaldepartments, dedicated to a job that barelyenables them to survive. The low salariesand irregularity of payments force themedical staff to be absent from their jobs soas to try to make a living elsewhere.Finally, the regionalisation of the healthsystem means that local administrations are incharge of managing the hospital budgets, butthe regions have even less resources than the
The young surgeons of “City Hospital” in Sukhumi take usinto the room of a patient they have already operated ontwice and whom they plan to amputate within the week assoon as the equipment and the drugs supplied byMédecins Sans Frontières arrive. 73-year-old Taïssa is nota stranger in this hospital. She worked there as a nursefor forty-nine years. She has been suffering from diabetesand vascular difficulties for twenty years and used to treatherself with drugs that she bought herself. When sheretired with a pension of 30 roubles, she no longer hadthe means to pay for them. She was admitted to thehospital a few weeks ago after injuring herself whilecutting a toenail. The tissue on her leg has becomenecrotic. She is in pain and threatens to take her own life if she is not given something to relieve her pain. Herneighbours once bought her some medication beforeleaving the country. She can’t return home, as there is noone to take care of her. Her Georgian husband haspassed away. Her daughter got married and she has not heard from her since.
government. It is thus impossible to findspecialist care outside Sukhumi. Patients haveto travel to the capital to consult anophthalmologist. This is a very difficult for theisolated elderly who often suffer from eyesightproblems, particularly cataracts.In short, access to medical care in Abkhaziarequires a considerable income and anetwork of relations, requirements that theindigent population does not have.

12A b k h a z i a – D e c e m b e r 2 0 0 2
…Kept on lifesupport by relieforganisations
The majority of indigent people need medicalcare. Médecins Sans Frontières has thereforeset up a programme which endeavours to finda solution to the three major problemsidentified by its teams – the difficulties ofaccess to medical care, including surgery, theshortage of drugs and the lack of autonomyamong patients confined to their home as aresult of their illnesses.In 2002, Médecins Sans Frontières reorganisedits medical care programme. The programmehas two main objectives – providing freemedical care to the indigent population andreducing the mortality rate of emergencyhospitalisations. A consultation room has beenrehabilitated in hospitals of the country’s eightmain towns. A hospital doctor, who receivesindigent patients free of charge and makeshouse calls to those who are bedridden, hasbeen identified in each hospital. In Sukhumi, where there is the largestconcentration of indigent people, patients areable to attend consultations at the Abasinskaïahealth centre that has been rehabilitated tothis effect and run entirely by MSF. A mobileteam consisting of a doctor and a nurse,
employed by MSF, is dedicated to makinghouse calls to indigent patients who are unableto travel to the health facilities. Three otherhealth dispensaries treat people free of charge.In all these facilities, Médecins Sans Frontièresprovides drugs for the most common diseases4
encountered among the indigent population.Today, most of the drug requirements for thesediseases are met by donations from MSF.The organisation also supplies drugs toindigent patients via the regional hospitalsand “City Hospital”, the central hospital inSukhumi. A stock of drugs to stabilise thecondition of newly hospitalised patients forforty-eight hours following their admissioncompletes this activity.MSF also donates drugs and medical equipmentmonthly to the surgical department of “CityHospital” in Sukhumi, which should allow theteam to carry out about twenty free operationseach month. The whole programme is entirelyfinanced by private funds. The budget for theyear 2002 is estimated at 221,734 euros. TheICRC provides the surgical departments in fivehospitals with medical equipment and drugsfor the treatment of indigent patients for thefirst forty-eight hours. It also finances thecountry’s four blood banks. Lastly, in the region of Gali, given theinstability in this area, the United Nationsorganises free consultations for the benefit ofthe indigent population.4 Respiratory diseases, gastro-intestinal diseases, infections
and some musculo-skeletal diseases.

13A b k h a z i a – D e c e m b e r 2 0 0 2
Little Healthcareoutside themain cities
Today, the majority of the 18,700 indigentpeople identified by MSF and the ICRC live inurban areas and thus have a minimum access tohealthcare, although only through the healthcentres supported by these organisations in themain cities.However, transport difficulties make access tohealthcare much more difficult for indigentpeople living outside the towns. In order to focuson the quality of treatment and its relationshipwith its patients, MSF decided to focus its effortin places where the numbers of indigent peopleare the highest. As there are no other partners,this has further compounded the problem ofaccess to medical care for the rural population.The supply of essential drugs to rural healthcentres (“Felcher points”) has therefore beenstopped. However, the inadequacy of thetransport infrastructure means that it is difficultfor the indigent people living in these areas toget to the regional capitals and thus they nowfind themselves without medical care.It is therefore urgent that the Ministry ofHealth or another medical organisationreceive the funding to take over andsupply medications to these healthfacilities.
Akamara is a ghost town, a curious mix of miningand spas, a sulphur spring in the depths of theAbkhazian mountains, twenty minutes by car fromTkvarcheli, the regional capital. In front of thebuilding where the person in charge of the healthcentre (Felcher point) lives, a man dressed in a darkshirt and trousers that looked worn-out but clean andironed, came up to the MSF volunteers. He was inhis 40s, very thin with a gaunt face and dark ringsaround his eyes, and was very out of breath. He washaving an asthma attack and was on the verge ofsuffocating. He grabbed the salbutamol puffer thatthe doctor had taken out of his emergency aid kit.When he got his breath back, he explained that hehad run out of his medication and had walked twokilometres to find some. However, the nurse was not there and in any case,there were no medications in stock. He was anxiousand angry, he blamed Médecins Sans Frontières forno longer supplying drugs to the Felcher points. Asa former miner, he has been suffering from asthmafor 15 years and must take salbutamol everyday, andan adrenaline injection when he has an acuteasthma attack. He must henceforth walk twelvekilometres to Tkvarcheli to receive his treatment.
Medical care of chronicdiseases: an unattainableluxury?
22-year-old Nasik has always been epileptic. Beforethe war broke out, she used to take medication everyday which stabilised her illness and her seizures hadalmost completely stopped. However her conditiondeteriorated during the war when treatment was nolonger available. Today Nasik does not have all her witsabout her. She has regular seizures which her mothertries to quell by taking Nasik in her arms and calmingher. “I can’t let her out of my sight. It’s disastrous if I’m away when she has a seizure. She has alreadybeen admitted into hospital five times but even at thehospital there are often no drugs.” The treatment thatwould prevent Nasik from having seizures costs tworoubles (0.06 euro) a day.
The Abkhazian health system does not have themeans to provide medical care or surgery forpatients suffering from major diseases such ascancer. The drugs needed to treat these diseasesare not supplied by Médecins Sans Frontières astheir prescription would require a follow-up thatthe organisation cannot provide.Similarly, drugs for the treatment of diseasessuch as epilepsy, which do not affect a largenumber of people, are not provided. However,
this lack of treatment has drastic consequencesfor people suffering from such diseases. Surgicalservices that are already struggling to provideemergency interventions, cannot carry outoperations, which although not vital, wouldnevertheless improve the health and autonomyof patients considerably.
A b k h a z i a – D e c e m b e r 2 0 0 214
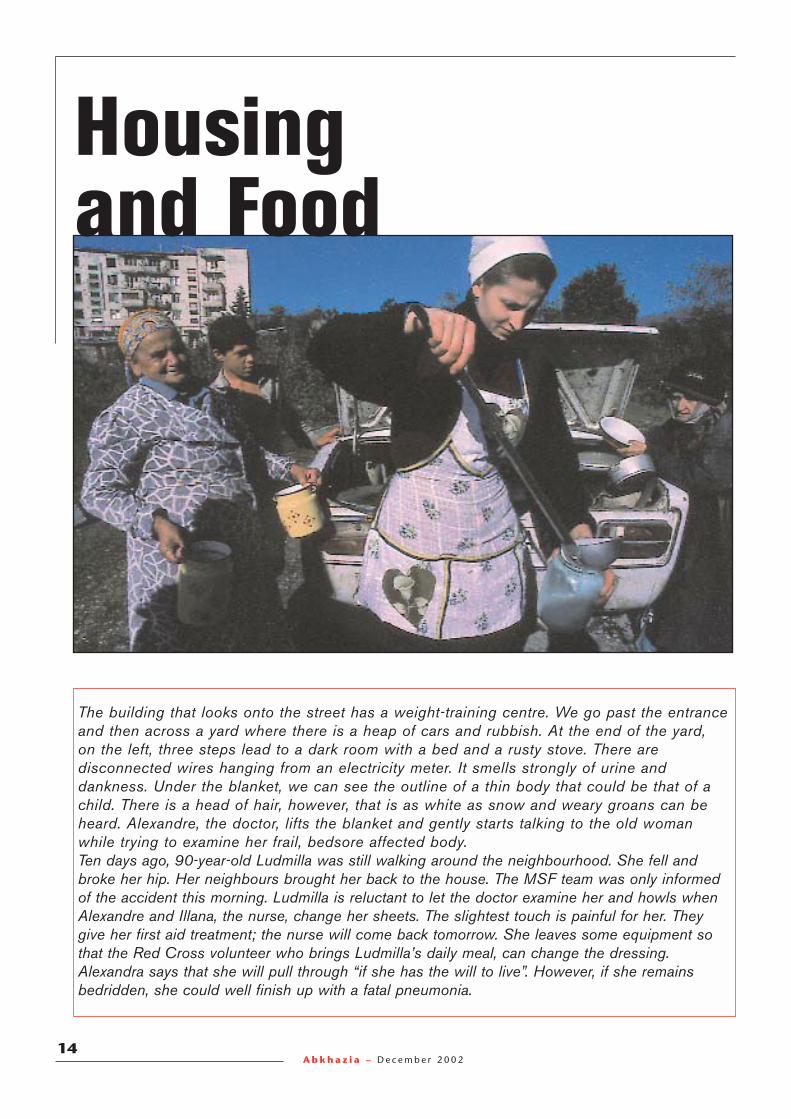
Housingand Food
The building that looks onto the street has a weight-training centre. We go past the entranceand then across a yard where there is a heap of cars and rubbish. At the end of the yard, on the left, three steps lead to a dark room with a bed and a rusty stove. There aredisconnected wires hanging from an electricity meter. It smells strongly of urine anddankness. Under the blanket, we can see the outline of a thin body that could be that of achild. There is a head of hair, however, that is as white as snow and weary groans can beheard. Alexandre, the doctor, lifts the blanket and gently starts talking to the old womanwhile trying to examine her frail, bedsore affected body. Ten days ago, 90-year-old Ludmilla was still walking around the neighbourhood. She fell andbroke her hip. Her neighbours brought her back to the house. The MSF team was only informedof the accident this morning. Ludmilla is reluctant to let the doctor examine her and howls whenAlexandre and Illana, the nurse, change her sheets. The slightest touch is painful for her. Theygive her first aid treatment; the nurse will come back tomorrow. She leaves some equipment sothat the Red Cross volunteer who brings Ludmilla’s daily meal, can change the dressing.Alexandra says that she will pull through “if she has the will to live”. However, if she remainsbedridden, she could well finish up with a fatal pneumonia.
15A b k h a z i a – D e c e m b e r 2 0 0 2
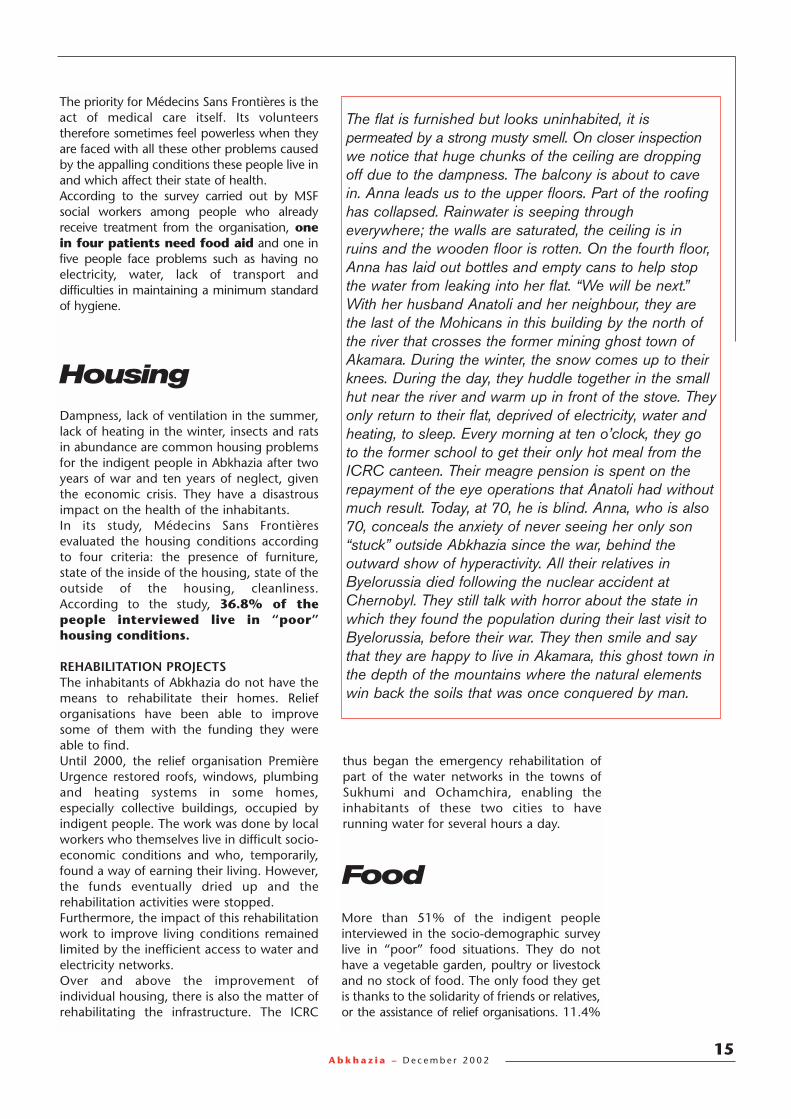
The priority for Médecins Sans Frontières is theact of medical care itself. Its volunteerstherefore sometimes feel powerless when theyare faced with all these other problems causedby the appalling conditions these people live inand which affect their state of health.According to the survey carried out by MSFsocial workers among people who alreadyreceive treatment from the organisation, onein four patients need food aid and one infive people face problems such as having noelectricity, water, lack of transport anddifficulties in maintaining a minimum standardof hygiene.
Dampness, lack of ventilation in the summer,lack of heating in the winter, insects and ratsin abundance are common housing problemsfor the indigent people in Abkhazia after twoyears of war and ten years of neglect, giventhe economic crisis. They have a disastrousimpact on the health of the inhabitants.In its study, Médecins Sans Frontièresevaluated the housing conditions accordingto four criteria: the presence of furniture,state of the inside of the housing, state of theoutside of the housing, cleanliness.According to the study, 36.8% of the people interviewed live in “poor”housing conditions.
REHABILITATION PROJECTSThe inhabitants of Abkhazia do not have themeans to rehabilitate their homes. Relieforganisations have been able to improvesome of them with the funding they wereable to find.Until 2000, the relief organisation PremièreUrgence restored roofs, windows, plumbingand heating systems in some homes,especially collective buildings, occupied byindigent people. The work was done by localworkers who themselves live in difficult socio-economic conditions and who, temporarily,found a way of earning their living. However,the funds eventually dried up and therehabilitation activities were stopped.Furthermore, the impact of this rehabilitationwork to improve living conditions remainedlimited by the inefficient access to water andelectricity networks.Over and above the improvement ofindividual housing, there is also the matter ofrehabilitating the infrastructure. The ICRC
Housing
thus began the emergency rehabilitation ofpart of the water networks in the towns ofSukhumi and Ochamchira, enabling theinhabitants of these two cities to haverunning water for several hours a day.
The flat is furnished but looks uninhabited, it ispermeated by a strong musty smell. On closer inspectionwe notice that huge chunks of the ceiling are droppingoff due to the dampness. The balcony is about to cavein. Anna leads us to the upper floors. Part of the roofinghas collapsed. Rainwater is seeping througheverywhere; the walls are saturated, the ceiling is inruins and the wooden floor is rotten. On the fourth floor,Anna has laid out bottles and empty cans to help stopthe water from leaking into her flat. “We will be next.”With her husband Anatoli and her neighbour, they arethe last of the Mohicans in this building by the north ofthe river that crosses the former mining ghost town ofAkamara. During the winter, the snow comes up to theirknees. During the day, they huddle together in the smallhut near the river and warm up in front of the stove. Theyonly return to their flat, deprived of electricity, water andheating, to sleep. Every morning at ten o’clock, they goto the former school to get their only hot meal from theICRC canteen. Their meagre pension is spent on therepayment of the eye operations that Anatoli had withoutmuch result. Today, at 70, he is blind. Anna, who is also70, conceals the anxiety of never seeing her only son“stuck” outside Abkhazia since the war, behind theoutward show of hyperactivity. All their relatives inByelorussia died following the nuclear accident atChernobyl. They still talk with horror about the state inwhich they found the population during their last visit toByelorussia, before their war. They then smile and say that they are happy to live in Akamara, this ghost town inthe depth of the mountains where the natural elementswin back the soils that was once conquered by man.
More than 51% of the indigent peopleinterviewed in the socio-demographic surveylive in “poor” food situations. They do nothave a vegetable garden, poultry or livestockand no stock of food. The only food they getis thanks to the solidarity of friends or relatives,or the assistance of relief organisations. 11.4%
Food

A b k h a z i a – D e c e m b e r 2 0 0 216
have an even more serious food situation thatthe study considers as “very poor” – they donot receive any assistance whatsoever 5.
EMERGENCY AIDToday the ICRC ensures food security for morethan 19,000 indigent people in Abkhazia.5,351 people receive hot meals that areprepared and distributed through a networkof 21 canteens spread all over the country.Seven mobile teams take food to the homesof 1,411 people who cannot move. It is thevolunteers of the Abkhazian Red Cross whocarry out this task. They also bring theindigent people their pensions andmedications, do the house work, but moreespecially they break the loneliness byensuring a connection with the outside world.These volunteers live they themselves in verydifficult socio-economic conditions.2,316 people living in rural areas too far fromthe canteen sites receive a monthly foodparcel providing them with the necessaryamount of calories for survival. 11,355 otherswho can partly provide for their own needs,receive a parcel every two months to add totheir everyday fare.Without this assistance, one third of thebeneficiaries, i.e. 6,000 people, would havedied of hunger. Yet, while this majorassistance prevents thousands of people fromdying of hunger, it does not cover all theirfood requirements. Only 70% of MSF’spatients receive food assistance from relieforganisations.Those who do not receiving anything at all aregenerally those who can obtain part of theirfood requirement by themselves. Unfortunatelyit is rarely in sufficient quantity or quality. Not
85-year-old Anastasia tells the doctor that she is hungry. She complains that she only eats oncedaily, every morning around 10 o’clock, a plate of beans or some porridge, brought to her by theRed Cross volunteer. She shows us with regret the empty bag in which she used to get hersugar. This small token of sweetness has been snatched away. “It was the only pleasure I hadleft. What am I going to put in my tea?” 80-year-old Nebia, who is almost blind, is trying to sellher ration of beans, which give her stomach ache, so that can buy some sugar. Raïssa, who isbedridden, cannot cook the monthly parcel of food provided by the ICRC and her stomachcannot take the daily ration of beans. From time to time, a former neighbour brings some softwhite cheese and some hard-boiled eggs. Galina, bedridden and blind, also gets some soft cheese on lucky days when her husbandVladimir, who is bent double as a result of his poliomyelitis, has made a few roubles by repairing a clock. Anastasia, Raïssa, Galina, Vladimir and thousands of other indigent people survive thanksto the ICRC’s rations, set up to provide the necessary daily amount of calories for an adult.
receiving food aid, they are permanentlyunder or malnourished. As the populationcontinues to age and the economic situationflounders, the number of people who areunable to feed themselves will probablycontinue to increase.
SUPPORT TO AGRICULTURALDEVELOPMENT PROJECTSApart from emergency food aid, other typesof assistance programmes have been set upin Abkhazia to help sustain food security.From January 1995 to autumn 2000, inaddition to the daily distribution of meals andfood rations for the benefit of 3700 indigentpeople, the Spanish organisation, Accioncontra el Hambre, provided technicalassistance and distributed seeds for vegetablegardens. In this way, it helped families to re-cultivate the plots of land allocated by theauthorities. These programmes were stoppedin autumn 2000 6 due to the shortage offunds. If additional funds are provided, the“food security” agricultural activities shouldresume in 2003 within the scope of a projectwhich would include 1,500 to 2,000 peoplein the region of Gali: food cultivated on asmall scale by people on a low income anddistributed to the most indigent people viaan economic network of solidarity. This typeof project would enable the peopleconcerned to ensure their autonomy, withrespect to food, and also give them a glimpseof a possible job prospect and to once againbe able to plan for the future.5 These people, identified during the survey, most probably
now receive assistance from the ICRC programme. 6 The 3700 beneficiaries of food distributions are now being
helped by the ICRC programme.

17A b k h a z i a – D e c e m b e r 2 0 0 2
One of the solutions to improve the livingconditions of the elderly who are indigent andisolated, is to offer them the possibility to staywith other people in a building where foodand care are provided daily. There are tworesidences of this type in Abkhazia, bothbased in Sukhumi.The first residence, set up in a building of thehospital for infectious diseases, accommodatesabout fifteen people, men and women, half ofwhom can no longer move around bythemselves. The toilets, however are on thefloor below the bedrooms. Running water isobtained from a tap by the entrance of the
building. A young woman is responsible fortaking care of all the residents during the day.At night, they are left by themselves and cancontact the hospital by phone. The UnitedNations High Commissioner for Refugees isfunding the running of the establishment upto the end of 2002. The other residence is aone-storey house, rehabilitated by UnitedNation Volonteers and has running water, akitchen, a terrace looking on to a courtyardgarden, toilets and a bathroom, a bigdormitory bedroom where five women live.They receive food from ICRC and are regularlyvisited by Médecins Sans Frontières. There isalways someone to watch over them.Other establishments of this type can becreated. About a hundred indigent elderly,who would be relieved to live in theseresidences, have already been identified bythe MSF and ICRC social workers.
Residences for the elderly
It is a small house in the middle of a yard, with a small garden. It can be accessed via a terrace,followed by a veranda, which the residents use depending on the season. The kitchen, bathroom,and toilets are clean. In the main big sunny room, there are five beds with their bedside tablescluttered with small, precious bits and pieces belonging to those who do not own much –photos, icons, alarm clocks, pill boxes etc. Four elderly women are sitting quietly on their bedswaiting, with restrained impatience, to tell their tales to the visitors who add some excitement to their routine.80-year-old Natalia, a Russian veteran of the Second World War suffers from heart disease and is losing her sight. She used to live in an area that was so isolated that even the ICRCvolunteer could not deliver her meals. She worked in an orphanage all her life but has nochildren of her own to take care of her. The other Natalia, who is 75, does not have any childreneither. The doctor advised her against having children as she suffers from rheumatic heartdisease. Ten days ago, she was still living with water around her ankles, in a wooden hut in the middle of a marsh.70-year-old Vira takes her medications but she is not aware that the disease that is ravaging herstomach is cancer. Her sadness is entirely focused on the loss of her children who died duringthe war. The searches carried out by the Red Cross to trace them were unsuccessful.72-year-old Marina annoys the women who share the room with her. She smokes and drinks toforget the misfortunes of her life. Born in Leningrad, she lost all the members of her familyduring the blockade of the town between 1941 and 1943. Orphaned at 13, she managed toescape Stalin’s purges in which all her friends lost their lives. She lost her only child when hewas 3 years old to diphtheria and fell into depression. In 1973 she rebuilt her life and a housewith her husband in Abkhazia. The bombardments during the war left her a widow and withouta roof over her head.97-year-old Alexandra has gone for her walk into town. The women who share the room withher say “She can’t sit still.” She is Ukrainian. She witnessed her children die during the faminein 1933 and the rest of her relatives during the Second World War. When she was sent to workin the tea plantations in Abkhazia, famine and bombardments caught up with her during the waragainst Georgia. In a picture on the bedside table, she is wearing a coat and scarf. She has ahappy smile on her face, and is full of life.
A b k h a z i a – D e c e m b e r 2 0 0 218
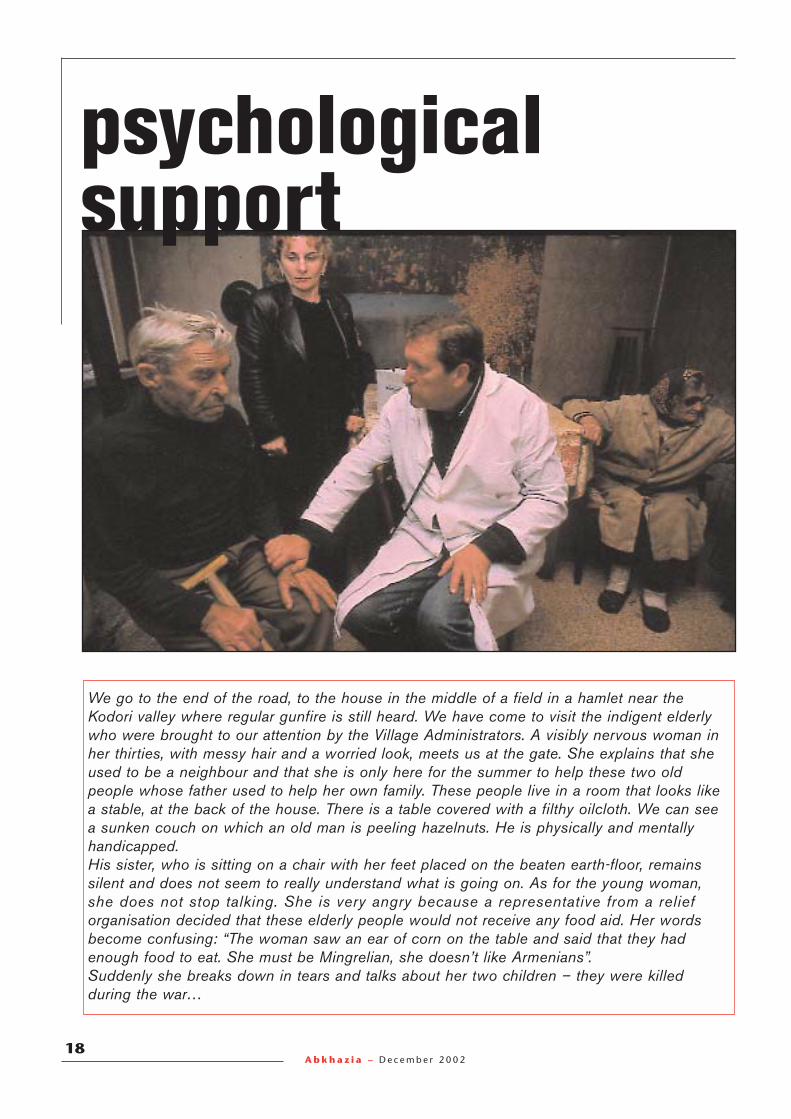
psychological support
We go to the end of the road, to the house in the middle of a field in a hamlet near theKodori valley where regular gunfire is still heard. We have come to visit the indigent elderlywho were brought to our attention by the Village Administrators. A visibly nervous woman inher thirties, with messy hair and a worried look, meets us at the gate. She explains that sheused to be a neighbour and that she is only here for the summer to help these two oldpeople whose father used to help her own family. These people live in a room that looks likea stable, at the back of the house. There is a table covered with a filthy oilcloth. We can seea sunken couch on which an old man is peeling hazelnuts. He is physically and mentallyhandicapped. His sister, who is sitting on a chair with her feet placed on the beaten earth-floor, remainssilent and does not seem to really understand what is going on. As for the young woman,she does not stop talking. She is very angry because a representative from a relieforganisation decided that these elderly people would not receive any food aid. Her wordsbecome confusing: “The woman saw an ear of corn on the table and said that they hadenough food to eat. She must be Mingrelian, she doesn’t like Armenians”. Suddenly she breaks down in tears and talks about her two children – they were killedduring the war…

19A b k h a z i a – D e c e m b e r 2 0 0 2
A traumatisedpopulation
Psychologicaldistress, above all in theelderly
“THE RIGHT WORD OF COMFORT, A VISIT ATTHE RIGHT MOMENT, A FEELING THAT THEREIS SOMEONE WHO IS NOT INDIFFERENT TOYOUR PROBLEMS CAN SOMETIMES BE MOREUSEFUL THAN DRUGS.”Asida Lomia, social worker for Médecins SansFrontières, Sukhumi.
“Ten years ago, the population was mainlysuffering from the traumas of the war. Today,on top of their traumas, there is the despaircaused by social distress and lack of futureprospects,” notes Abkhaze psychologist, ArdaInal-Ipa.The fear that the war might start again, fuelledby the different episodes of conflict during thelast few years, sustains the traumas. When thesound of gunfire can be heard from the KodoriValley, situated about fifty kilometres awayfrom Sukhumi, the inhabitants of the capitaldread the worst. “The headmistress of my son’sschool could not bear the situation. She left thecountry, leaving helpless the children to whomher activities brought invaluable equilibrium.”Arda says regretfully.“Former soldiers, who were important peopleduring the war, are today reduced to beggingto buy cigarettes” deplores the psychologist.Unemployed and denied any control over theirfuture and that of their family, they areeconomically dependent on their wives. It isthe wives who support their families throughsmall transactions across the border withRussia.Men aged between 25 and 30, who wereadolescents during the war, are particularlyaffected. “At that age, the psyche is not verystable” Arda notes. “The trauma caused by thewar prevents it from developing. As adults,many suffer from psychological disorders”.Men suffer the most from psychologicalproblems, but they do not go for consultationsbecause of their culture and because theycan’t afford it. It is the women who talk abouttheir family problems.The drift towards drug and alcoholconsumption in order to relieve the sufferingas a result of these post-traumatic disorderscreates conflict within the families andperpetuates the spiral of psychological distress. Drug addiction is often collective.Psychological assistance, along with medicalcare, is often needed to break the addiction.
The socio-economic difficulties together withthe trauma caused by the war, reinforce thepsychological distress of the indigent people.The indigent elderly, who were oncerelatively protected are those that find it themost difficult to adjust to the changesimposed by the collapse of the Sovietsystem, the war and the embargo.Most of them are abandoned, not only bytheir families, but also by a society that nolonger takes care of themIn the survey carried out among indigentpeople in April 2002 by the social workers ofMédecins Sans Frontières, the demand forpsychological support ranked second place,just after medical care.After Sukhumi which has the largest indigentpopulation in the country, the biggestdemand for psychological support fromindigent people was from the regions ofGagra and Goudaouta. Traditionally wealthyareas, these former sea resorts today remainrelatively less affected by poverty than otherareas. The smaller numbers of indigentpeople in these regions therefore feel evenmore isolated and neglected.
Yeva is in a state of depression. She lives in a villageabout ten kilometres away from Sukhumi. When wevisit her with the MSF social worker, she becomesangry and then bursts into tears. She has been deniedfood aid because she is supposed to be able to feedherself with the food from her garden. But she saysthat she suffers from hypertension and does not havethe energy to cultivate her garden. Her husband diedfrom cancer, and she lives with her three children. Theeldest is epileptic and must be continually watched, asthe treatment that would stabilise her condition is tooexpensive. While she was having a seizure, she fell inthe fire and burnt her thigh badly. The middle child isblind and the youngest suffers from asthma. “You seehow we live! My children are suffering under my owneyes and I can’t do anything for them. I want to die to end my torture.”

A b k h a z i a – D e c e m b e r 2 0 0 220
An indigentpsychologicalprogramme
The psychiatric hospital in Sukhumi is mainlyoccupied by patients who use to receivecorrect medical care before the war andwhose condition has deteriorated since, dueto lack of treatment. As in all the hospitals,there is a shortage of drugs.A small detoxification clinic, founded by apsychiatrist, treats around a dozen peopleaddicted to alcohol and drugs. It is funded bythe state, but the patients have to pay for theirmedications that are extremely expensive.There are currently only three professionalsqualified in providing psychological supportand treatment in Abkhazia which has 180,000inhabitants. There are a few students currentlystudying in Russia but who will return topractice their career in Abkhazia… providedthat they can earn a living from it.Today the MSF teams refer the patients inneed of psychological support to Arda Inal-Ipa,who is overworked, who gives consultationswithin the framework of the very few activeorganisations involved in this area:
- The centre for young people of Sukhumi,which only takes children.- The centre for humanitarian programmes, inaddition to the usual routine consultations,provides psychological support services bytelephone. Four “listeners” have been trainedin Russia for this purpose. They have receivedmore than 2,400 phone calls and providedmore than 500 consultations. Unfortunately,the funding for this programme is due to endat the end of 2002.- The Gali Women’s Association is particularlydedicated to students of this region, which isstill particularly fragile as it is unstablepolitically and in the military sector.Arda Inal-Ipa suggests that while waiting forthe next generation of qualified psychotherapists,helpers should be trained to help peoplesuffering from psychological distress toexpress their traumas and to relax.She adds: “But no psychological treatmentwill teach people not to worry about theirfinancial problems.” Giving the populationback the means to make plans, have workand to be successful, seems to her, to be away of markedly relieving the psychologicaldistress which is draining the country. Asystem of micro-credits enabling individualsto set up small businesses would fulfil thisobjective to some extent, while developingthe economic situation.
21A b k h a z i a – D e c e m b e r 2 0 0 2
Conclusion
Today, the International Committee of the Red Cross and Médecins Sans Frontières are the onlyorganisations providing vital food and healthcare for more than 18,000 indigent people. However,despite working in close collaboration, they cannot meet all the essential needs of a population thatlives in dire socio-economic and psychological distress. Housing unfit for habitation, lack of heatingand clothing worsen their sanitary situations. For ten years now, the survival of one in ten people livingin Abkhazia depends on the help of relief organisations. Meanwhile, the majority of organisations whocould provide assistance in these areas have had to stop their operations due to the shortage ofinternational funding. Theoretically, all these operations should be implemented by the state andbecome part of development aid. However, as long as Abkhazia remains banished by the internationalcommunity in a “non-war/non-peace/non-state” situation, this aid remains hypothetical.Today, in order to survive, the indigent people of Abkhazia need emergency aid. However, due to a lackof projects and funding with far-reaching impacts, their problems are not widely known and there arefew independent evaluations.In turn, lack of information leads to a lack of interest to fund projects. This vicious cycle contributesto the maintenance of a form of humanitarian embargo on top of the trade and military embargoimposed to Abkhazia. Nevertheless, since the cease-fire, Georgia has always supported Médecins SansFrontières’ humanitarian activities in Abkhazia.The emergency humanitarian needs which would improve the population’s condition have beenidentified, and there are organisations ready to intervene, provided that they have the means.The provision of essential drugs to rural health centres could be resumed by a medical organisationwhich would thus reinforce Médecins Sans Frontières’ activities. A network of trained agents could becreated to bring psychological support to the indigent population. Other organisations could continueand develop the rehabilitation of the housing that is most unfit for habitation. Several small residencescould therefore be restored to house elderly people who are the most distressed and in which theywould also receive food and healthcare from different organisations.Cut off from the rest of the world, living in precarious conditions, with no governmental or foreign aidto help them meet their needs, the population of Abkhazia today need particular attention andassistance. Now.
MSF in the CaucasusMédecins Sans Frontières is a private, non-profitinternational humanitarian relief organisationwhose objective is to provide medical assistanceto populations in crisis. The organisation is basedon voluntary participation and is independent ofall States and institutions, as well as of allpolitical, economic or religious influences. Theorganisation was created in 1971 by doctorswho decided to provide emergency medicalassistance wherever there are victims of wars andnatural or man-made catastrophes. Assistance isprovided to populations in distress regardless ofrace, religion, creed or political affiliation.More than 2,000 volunteers join theorganisation every year. At present, more than1,000 expatriates are working in over 80countries. Most of MSF’s financing is derivedfrom private donations. The rest comes frominstitutional donors (ECHO, UNHCR).In 1999, Médecins Sans Frontières was awardedthe Nobel Peace prize.
The Dutch, Greek and Spanish sections ofMédecins Sans Frontières worked in Georgiauntil 2000. In 2002, the French section ofMédecins Sans Frontières has been running twoprogrammes in Georgia:- A medical consultation programme for theindigent population in a district of Tbilisi- A programme providing support to the surgicaldepartment of Akhmeta Hospital near the PankisiValley.
Médecins Sans Frontières intervened for the firsttime in Abkhazia during the war in 1992 byassisting in surgical activities. Since then, manyother programmes have been set up. Today,some have been completed while others are inprogress:- The Enlarged Programme of immunisation(EPI), which was started in 1994, was completedin 1997.- The Tuberculosis Programme launched in1995, today has 200 patients at GuliripchiHospital, including 10 who are being treated formulti-resistant tuberculosis.The drugs and medical equipment distributionand healthcare assistance to medical facilitiesprogramme. This programme was opened in1993 during the conflict. In January 2002 it wasreadapted to meet the needs of the indigentpopulation. It provides free medical consultationsin health centres or during house calls, hospitalreferrals and free medications.
Médecins Sans Frontières undertook its first reliefoperation in the region of Caucasus after theearthquake in Leninakan in Armenia in 1988.Since then, the organisation has intervened toassist war wounded, refugees and displacedpersons as well as victims of conflicts which haveshaken this region between opposing Georgiansand Southern Ossetians, Georgians andAbkhazians, Northern Ossetians and Ingush,Armenians and Azeris, Russians and Chechensetc.Since 1994, the conflicts have ceased or havebeen contained, with the exception ofChechnya. However, there are still hundreds ofthousands of war victims, refugees, and peoplewith no means of support living in an extremelyprecarious situation in countries that have beenbled dry, where the institutions are unable to
meet the most basic needs of the population.Médecins Sans Frontières is therefore still inArmenia and Nagorno-Karabagh, Ingushetia,Chechnya, Georgia and Abkhazia.
In Georgia
In AbkhaziaIn the Caucasus
Médecins Sans Frontières in Georgia19a, Taboukachvili Street380008 Tbilissi00.995.32.99.95.1600.995.32.99.94.19msff-tbilissi@access.sanet.ge
Médecins Sans Frontières in ParisDr Christopher Brasher8, rue Saint-Sabin75011 [email protected]