obésité et métabolisme protéique -...
TRANSCRIPT
Obésité et métabolismeprotéique
3 octobre 2017
Pr. Yves BoirieService de Nutrition Clinique, CHU de Clermont-FerrandCentre de Recherche en Nutrition HumaineClermont-Ferrand
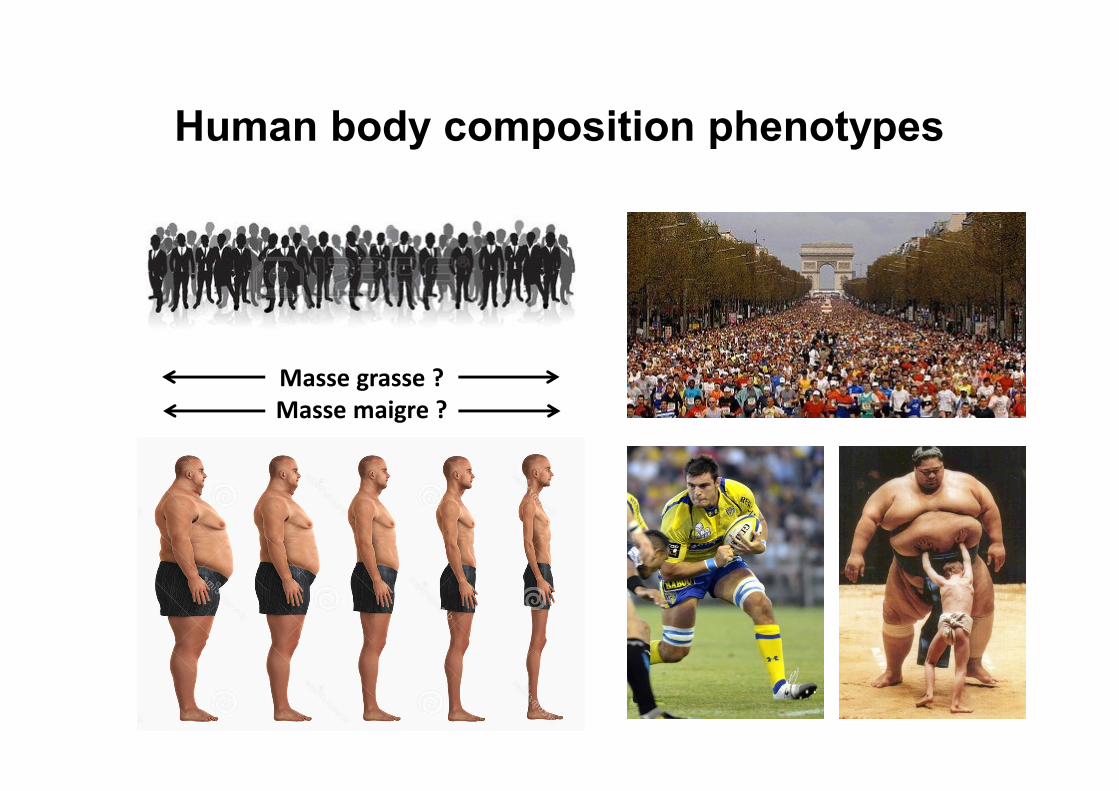
Human body composition phenotypes
Masse grasse ?Masse maigre ?
Obésité et Métabolisme protéique
• Trop de gras ou trop peu de maigre ?
• Masse maigre, moteur du renouvellement
protéique : spécificités de l’obésité
• Applications cliniques potentielles
Obésité et Métabolisme protéique
• Trop de gras ou trop peu de maigre ?
• Masse maigre, moteur du renouvellement
protéique : spécificités de l’obésité
• Applications cliniques potentielles
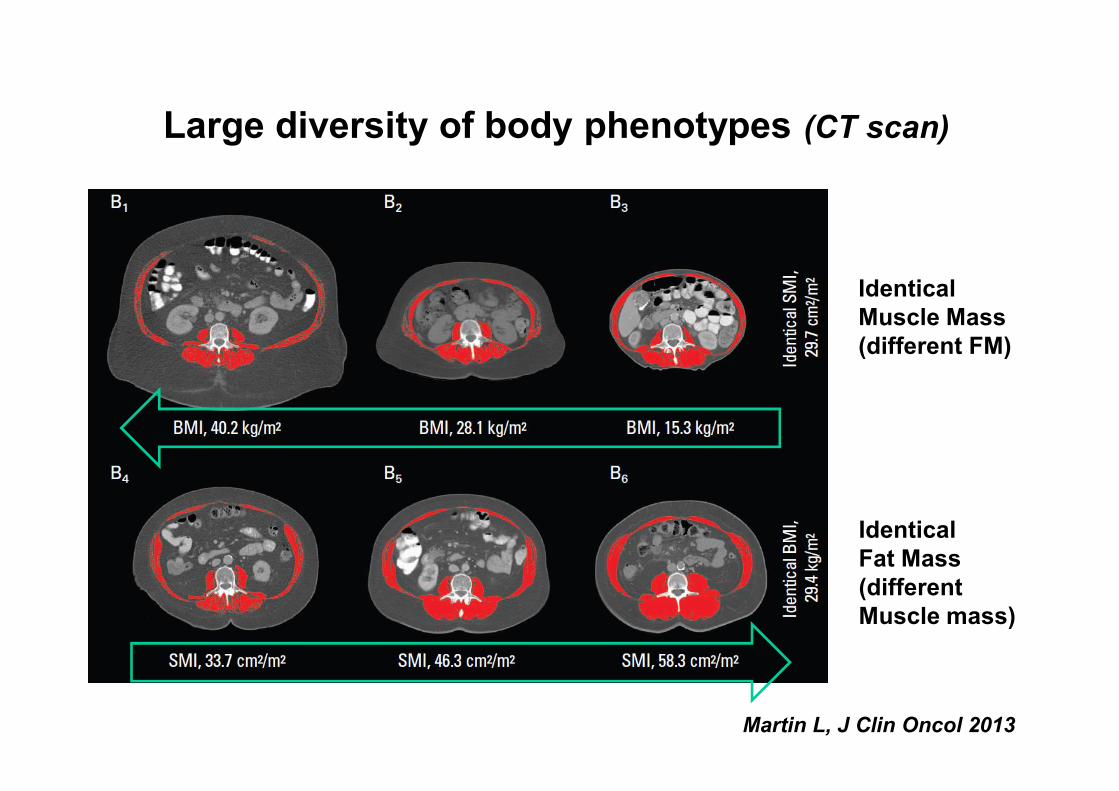
Large diversity of body phenotypes (CT scan)
IdenticalMuscle Mass(different FM)
IdenticalFat Mass(differentMuscle mass)
Martin L, J Clin Oncol 2013
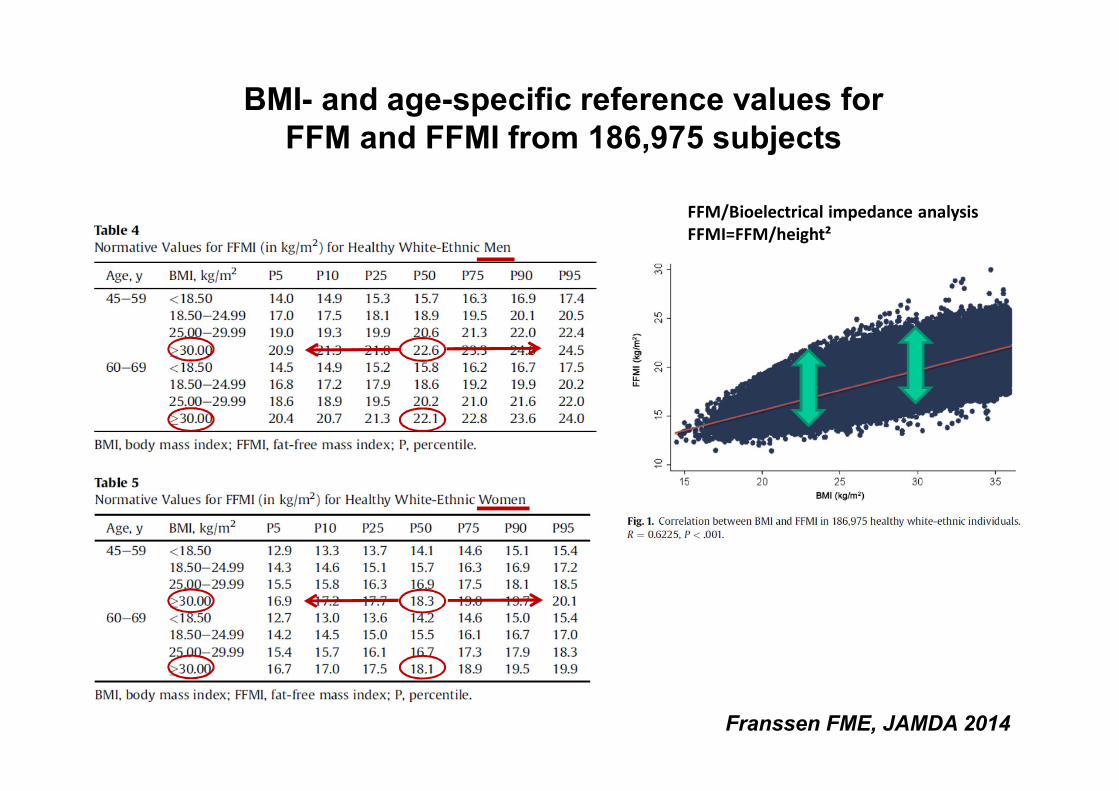
BMI- and age-specific reference values for FFM and FFMI from 186,975 subjects
Franssen FME, JAMDA 2014
FFM/Bioelectrical impedance analysisFFMI=FFM/height²
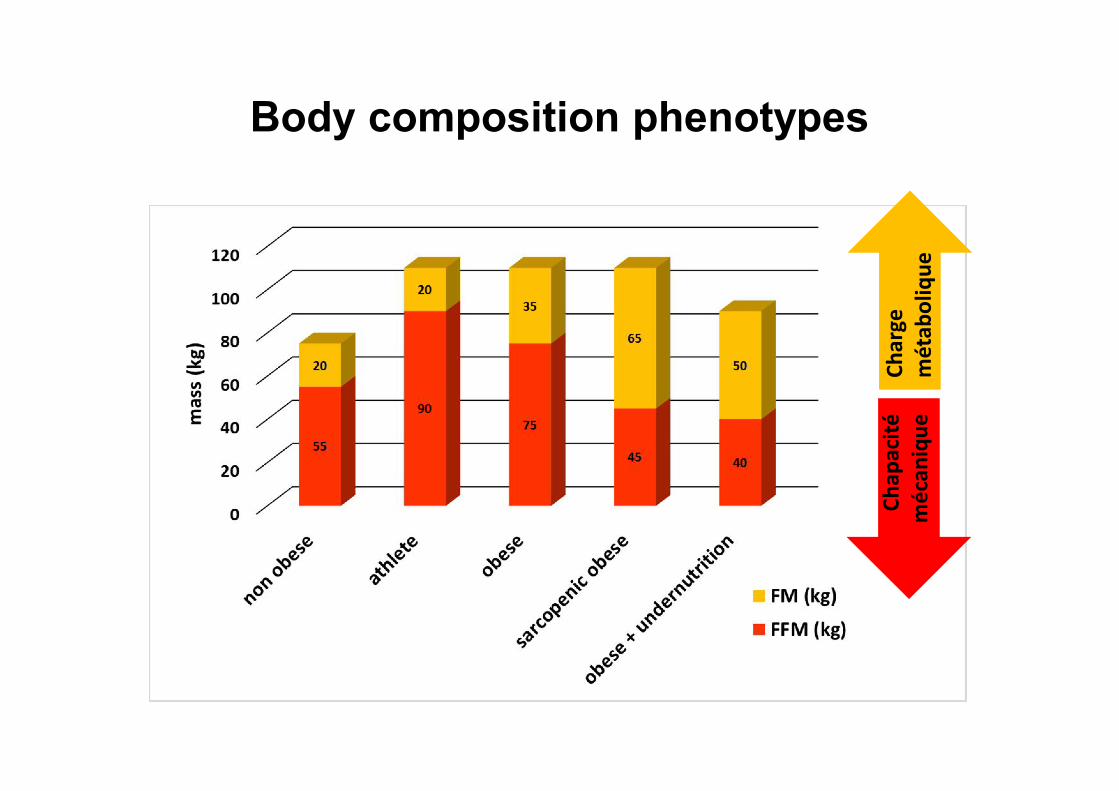
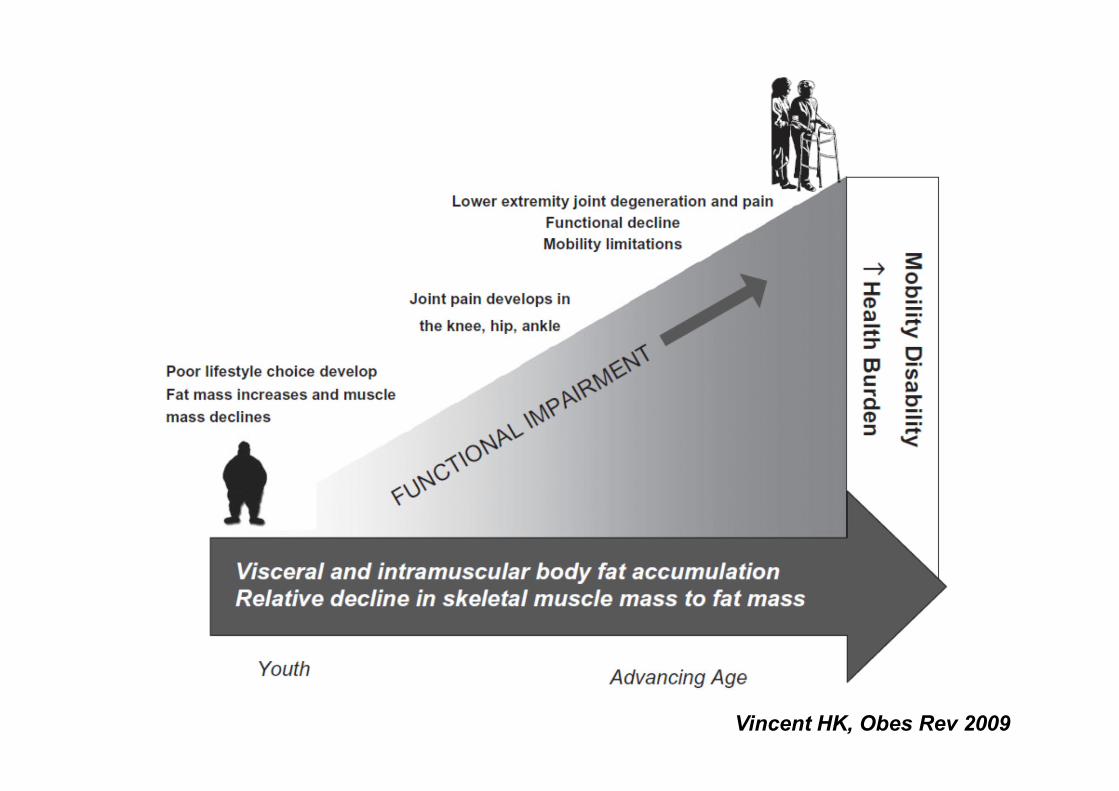
Body composition phenotypes
Char
ge
mét
abol
ique
Chap
acité
méc
aniq
ue
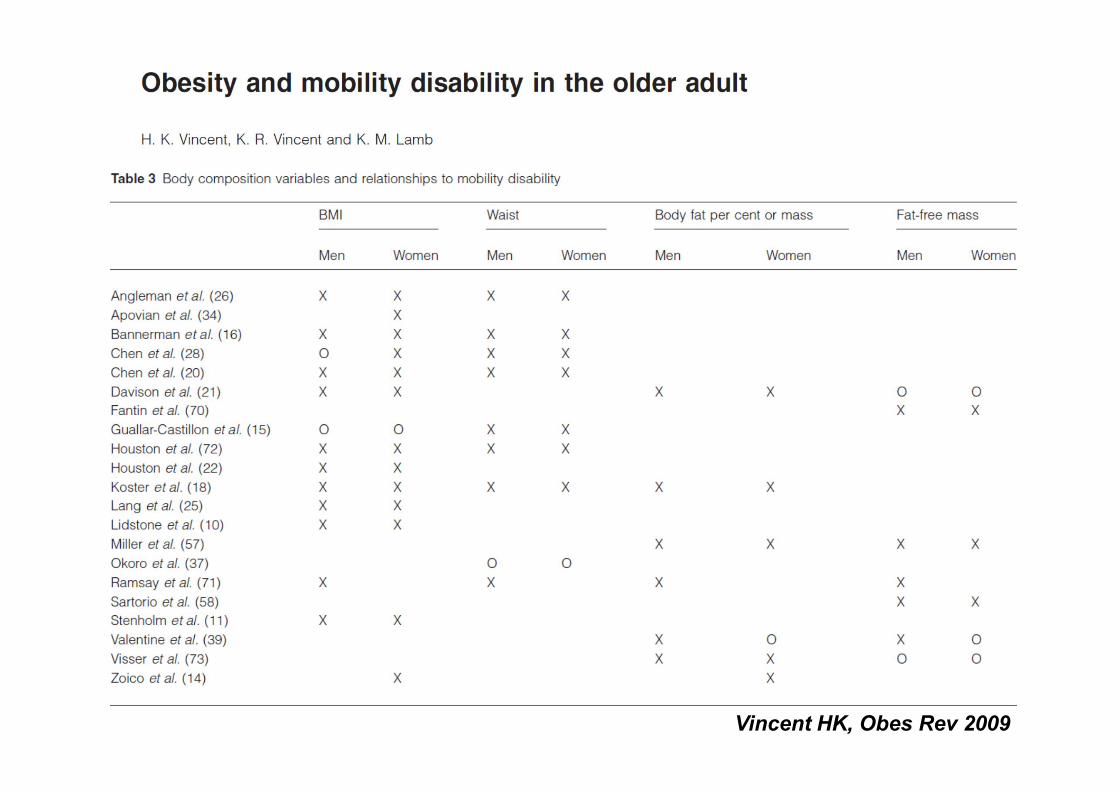
Vincent HK, Obes Rev 2009
Vincent HK, Obes Rev 2009
Obésité et Métabolisme protéique
• Trop de gras ou trop peu de maigre ?
• Masse maigre, moteur du renouvellement
protéique : spécificités de l’obésité
• Applications cliniques potentielles
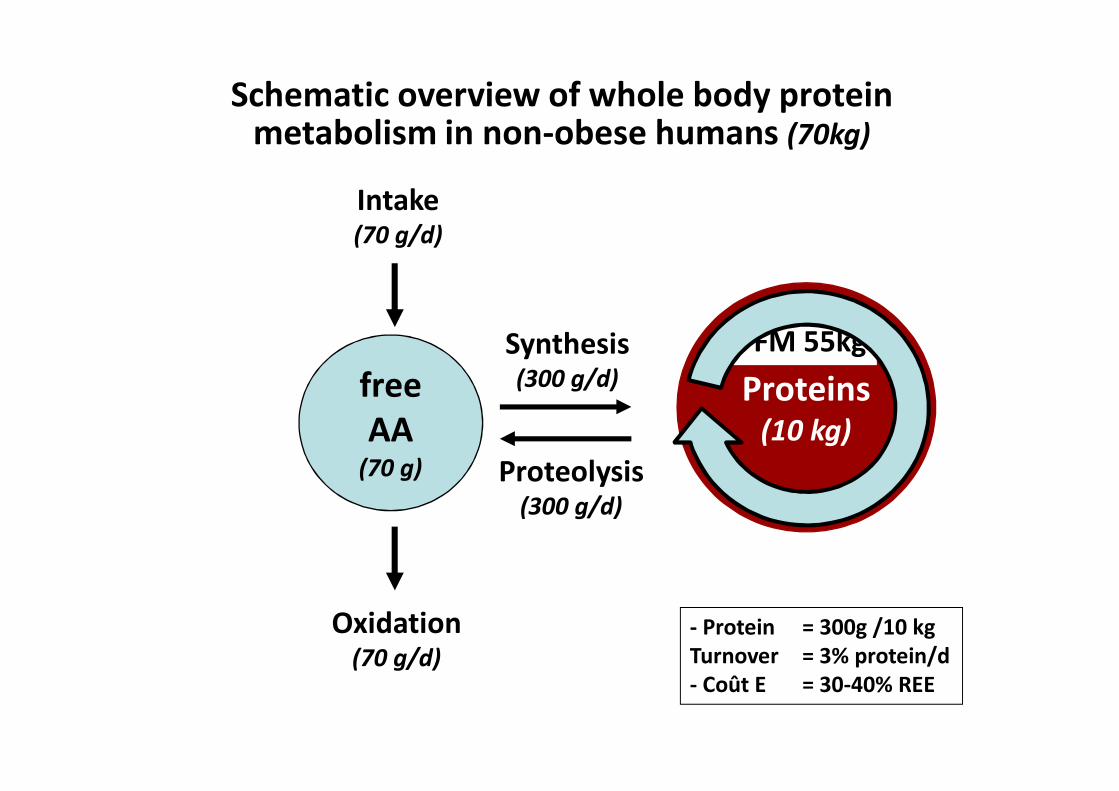
Synthesis (300 g/d)
Proteolysis (300 g/d)
Schematic overview of whole body proteinmetabolism in non-obese humans (70kg)
Intake (70 g/d)
Oxidation (70 g/d)
- Protein = 300g /10 kgTurnover = 3% protein/d- Coût E = 30-40% REE
Proteins(10 kg)
FFM 55kgfreeAA
(70 g)
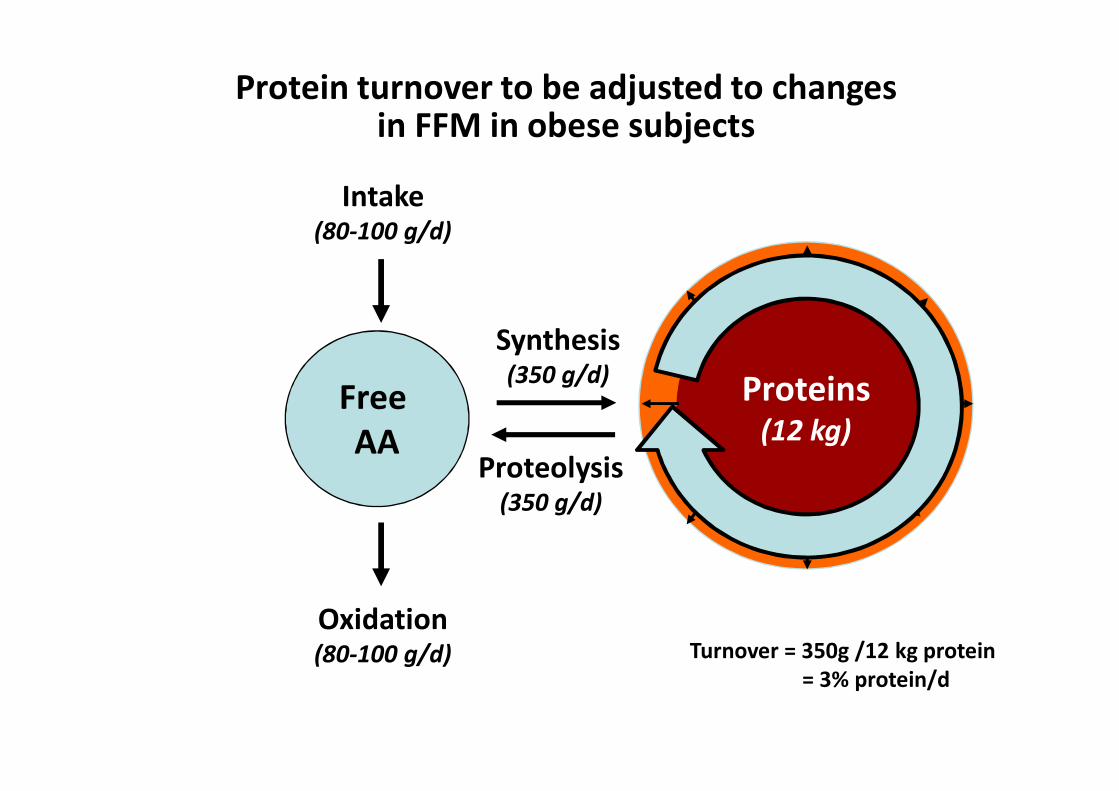
Free AA
Proteins(10 kg)
Synthesis (350 g/d)
Intake (80-100 g/d)
Proteolysis (350 g/d)
Oxidation (80-100 g/d)
Protein turnover to be adjusted to changes in FFM in obese subjects
Proteins(12 kg)
Turnover = 350g /12 kg protein= 3% protein/d
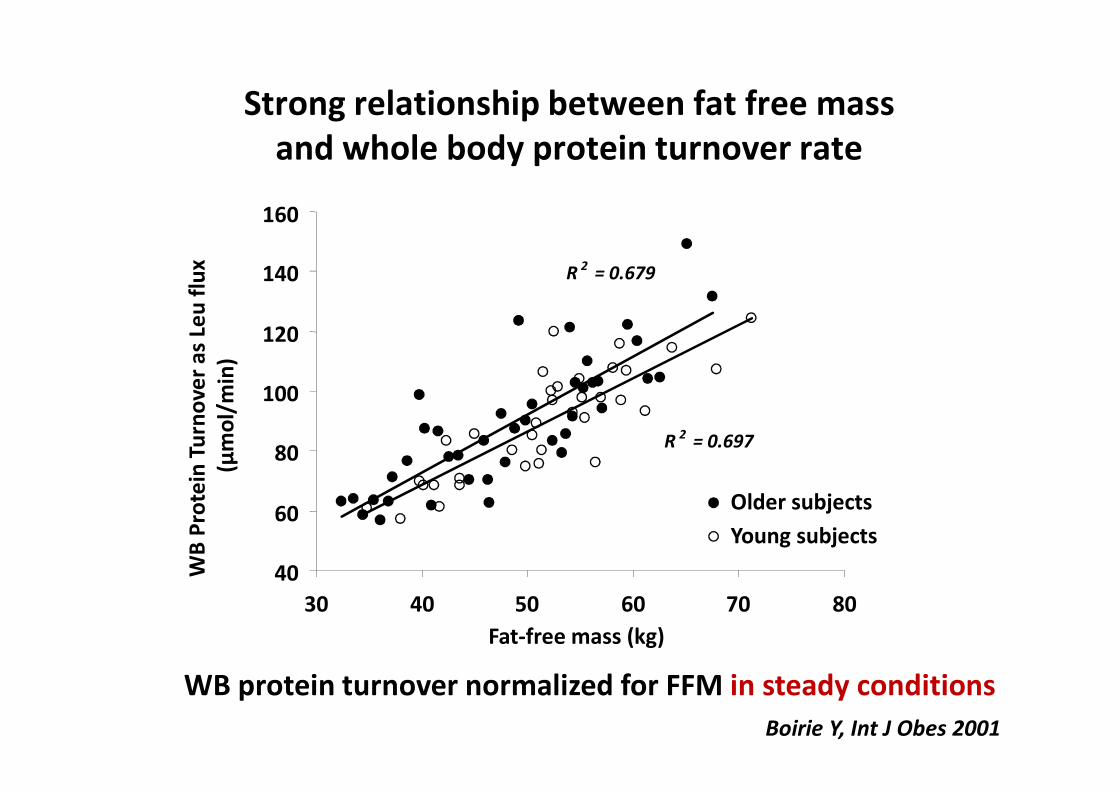
Strong relationship between fat free mass and whole body protein turnover rate
R 2 = 0.679
R 2 = 0.697
40
60
80
100
120
140
160
30 40 50 60 70 80Fat-free mass (kg)
WB
Prot
ein
Turn
over
as L
eu fl
ux
(µm
ol/m
in)
Older subjectsYoung subjects
Boirie Y, Int J Obes 2001
WB protein turnover normalized for FFM in steady conditions
?
Protein turnover rate may be affected by metabolic alterations associated with obesity
• Impaired glucose metabolism
• Insulin resistance
• Low-grade inflammation
• Higher FFA flux
• Adipokines production
Impact on WB protein metabolism: response to anabolic factors like insulin or meal intake?
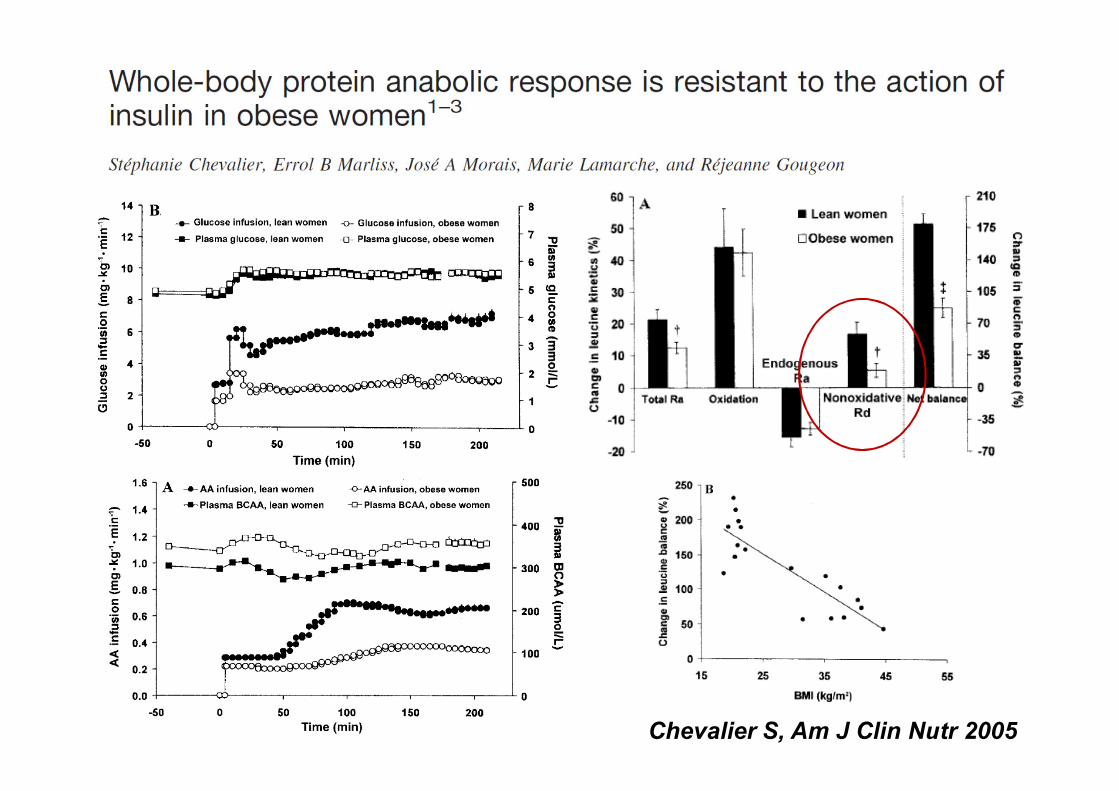
Chevalier S, Am J Clin Nutr 2005
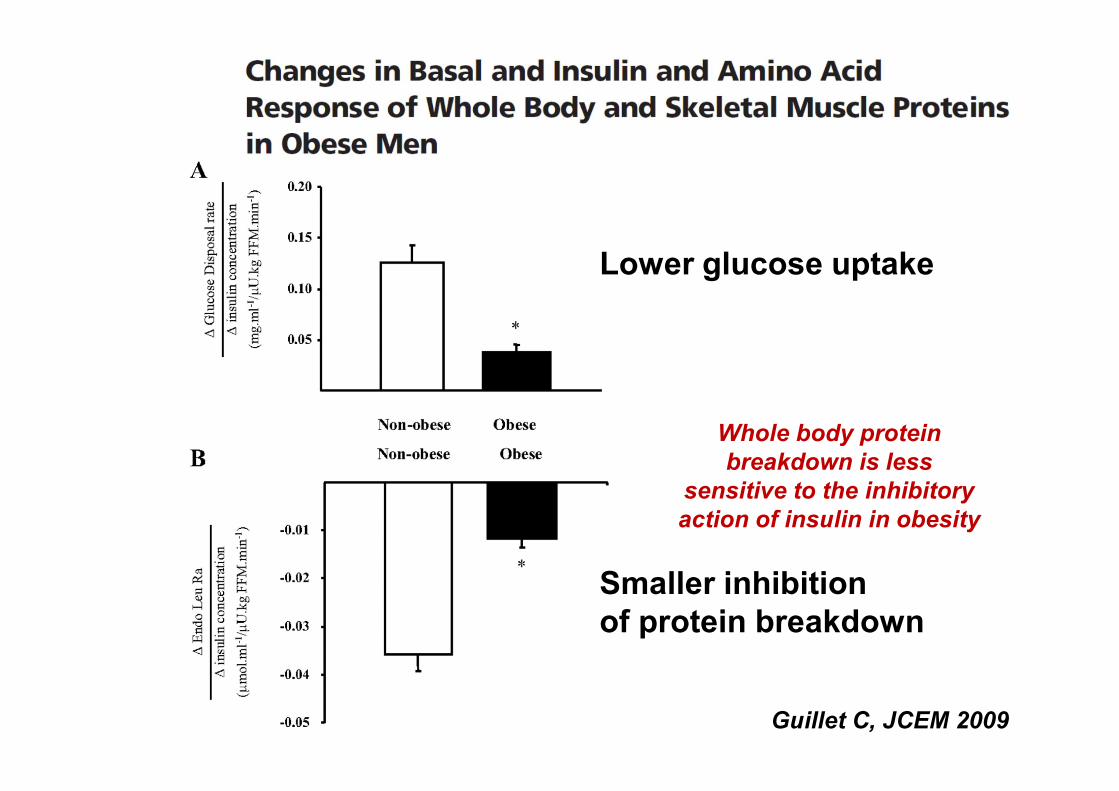
Whole body proteinbreakdown is less
sensitive to the inhibitoryaction of insulin in obesity
Lower glucose uptake
Smaller inhibition of protein breakdown
Guillet C, JCEM 2009
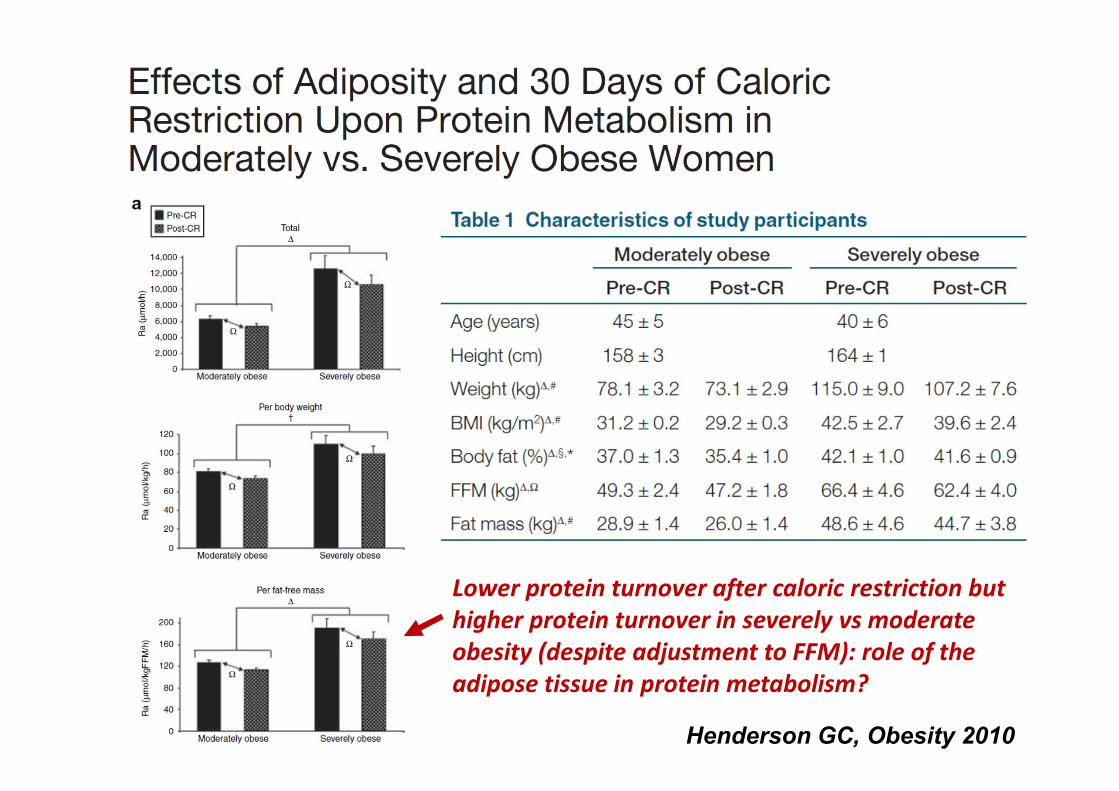
Henderson GC, Obesity 2010
Lower protein turnover after caloric restriction but higher protein turnover in severely vs moderateobesity (despite adjustment to FFM): role of the adipose tissue in protein metabolism?
Whole body protein metabolismof the obese patient
• WB protein turnover is higher in the obese but can be normalized after adjustment on lean body mass in stable conditions in moderately obesity
• Fat mass may contribute to whole body proteinmetabolism in severely obese patients
• The response of WB protein synthesis and breakdown to insulin and to meal intake isblunted ANABOLIC RESISTANCE ?
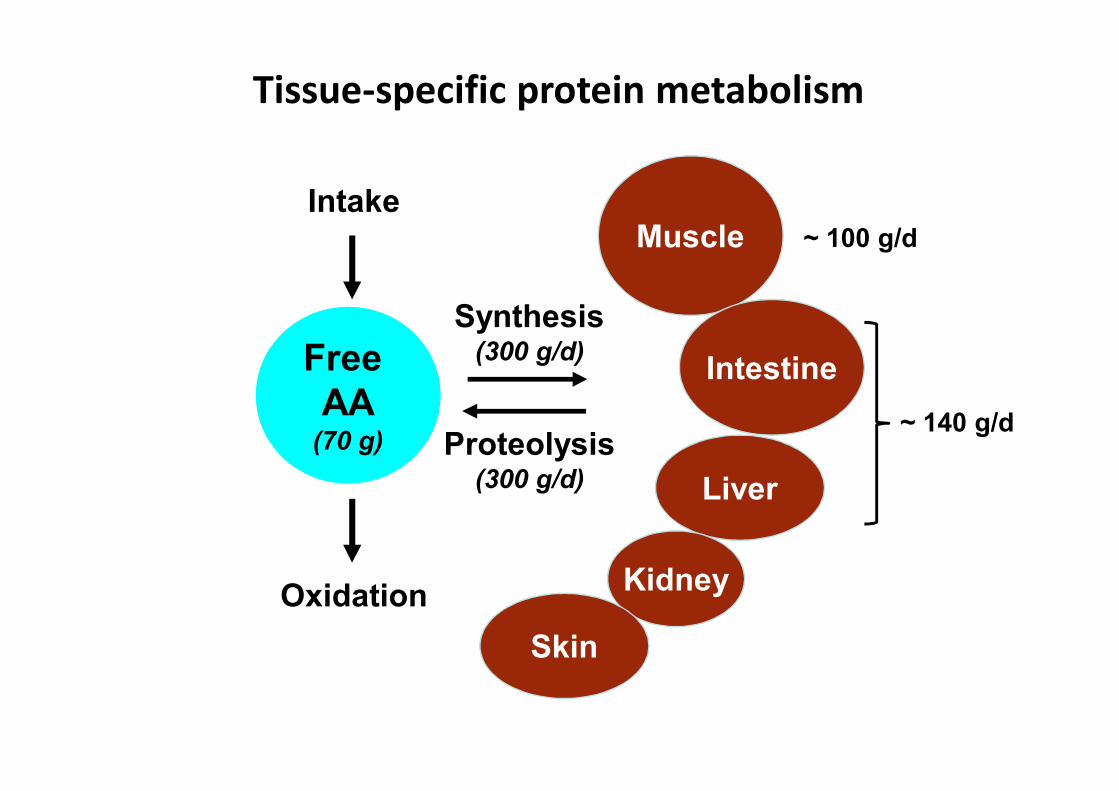
Muscle
Intestine
Liver
Kidney
Skin
~ 100 g/d
Tissue-specific protein metabolism
Free AA
(70 g)
Synthesis (300 g/d)
Intake
Proteolysis(300 g/d)
Oxidation
~ 140 g/d
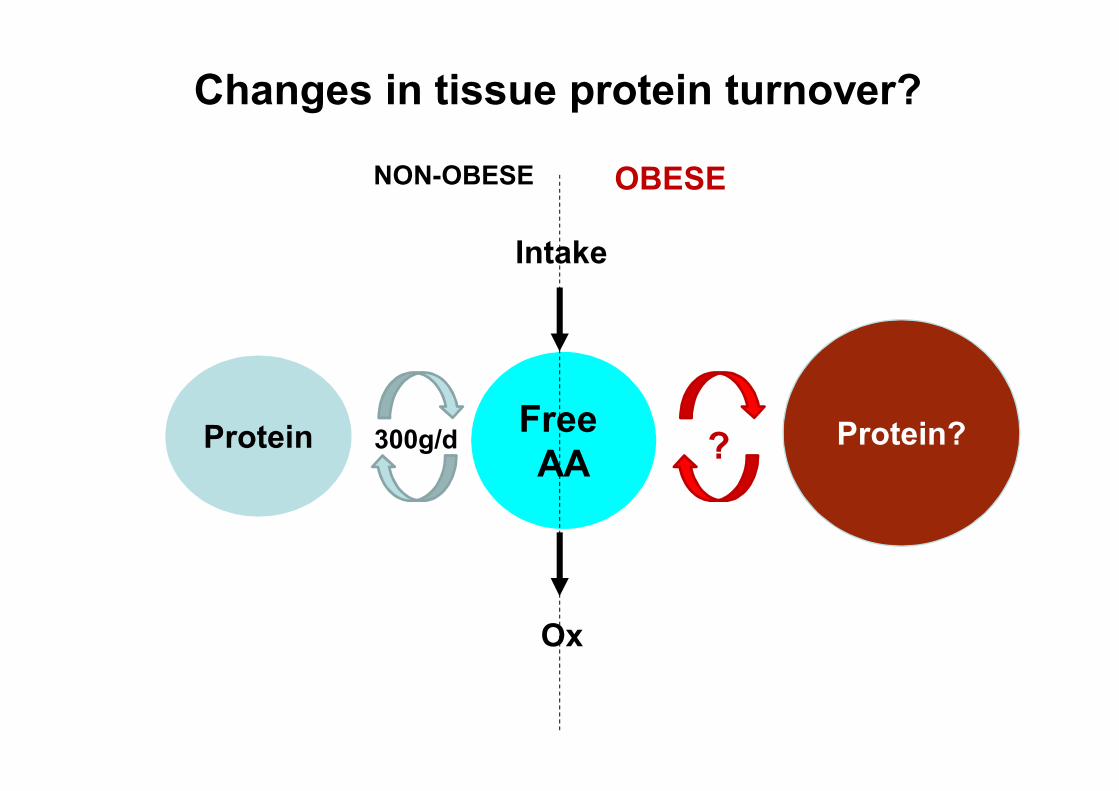
Changes in tissue protein turnover?
Free AA
Intake
Ox
Protein 300g/d
NON-OBESE
Protein??
OBESE
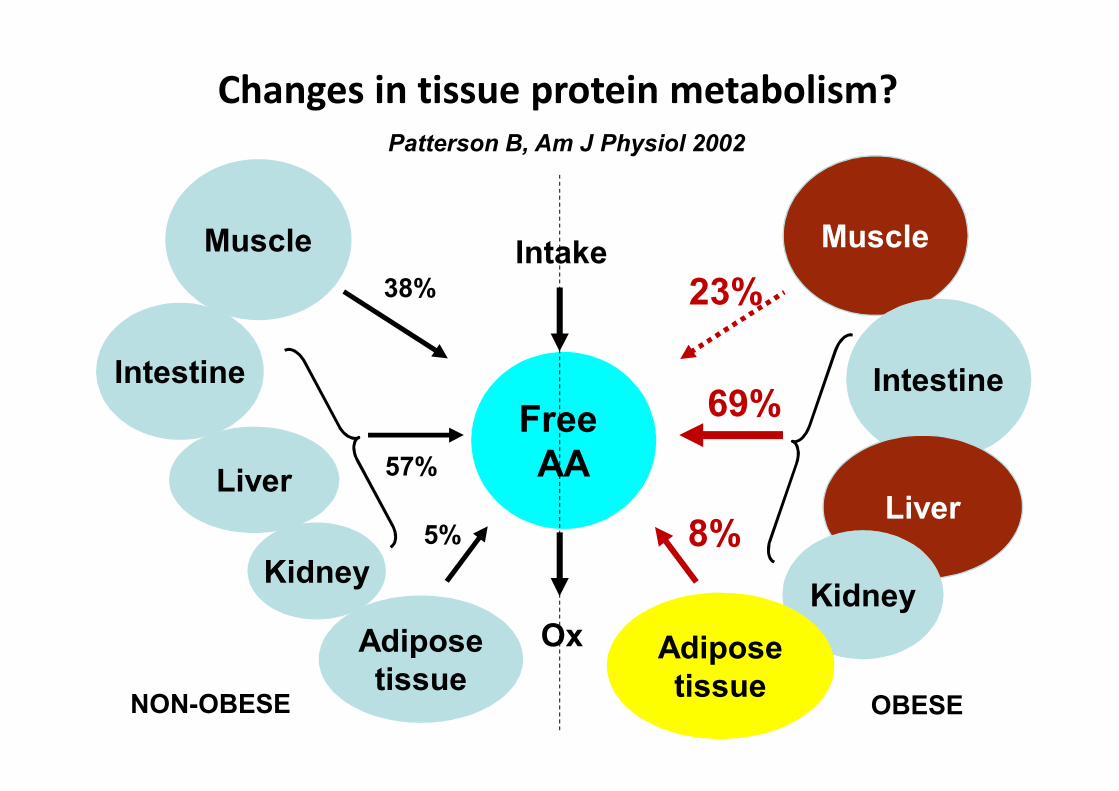
Changes in tissue protein metabolism?
Free AA
Intake
Ox
Muscle
Intestine
Liver
Kidney
Adiposetissue
38%
5%
57%
NON-OBESE
Muscle
Intestine
Liver
KidneyAdiposetissue
23%
8%
69%
OBESE
Patterson B, Am J Physiol 2002
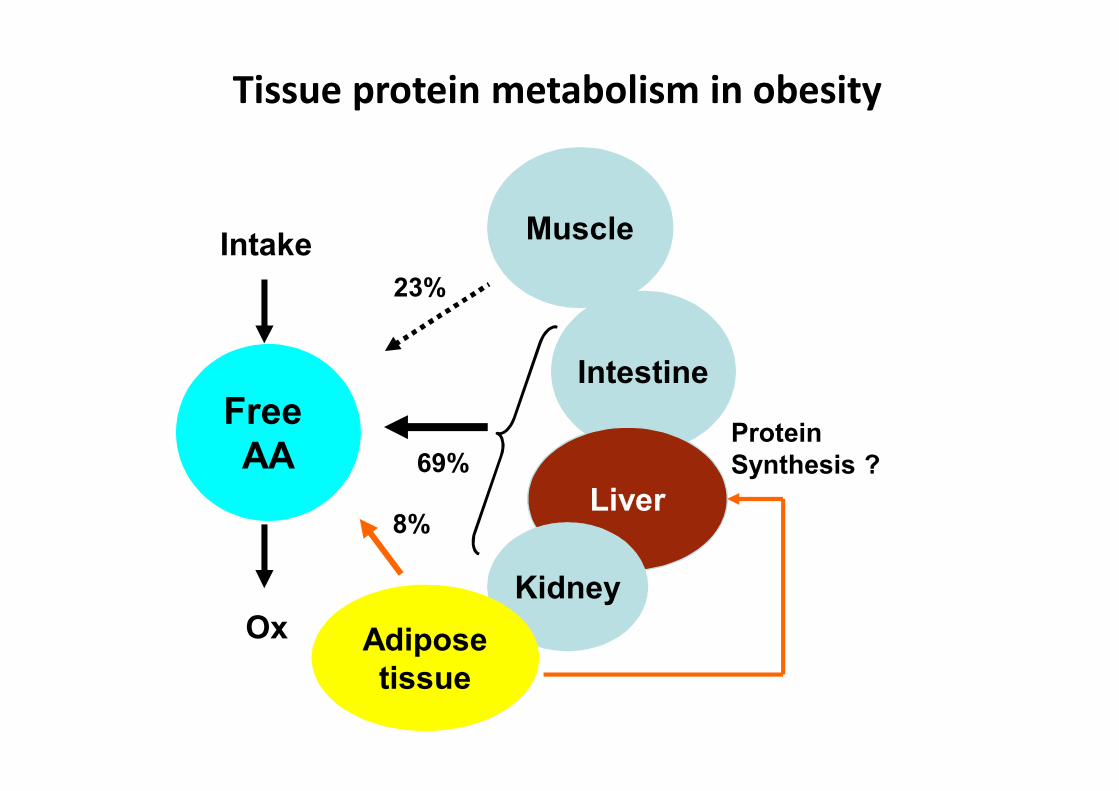
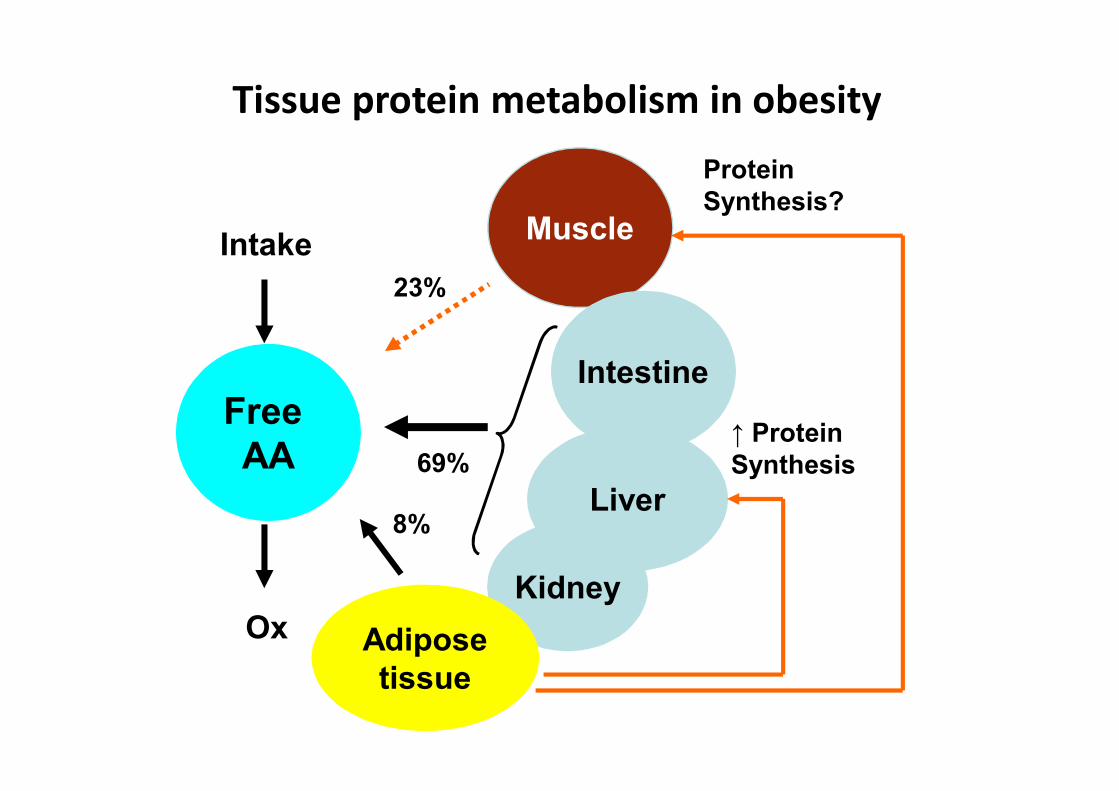
Muscle
Intestine
Liver
KidneyAdiposetissue
Tissue protein metabolism in obesity
Free AA
Intake
Ox
23%
8%
69%ProteinSynthesis ?
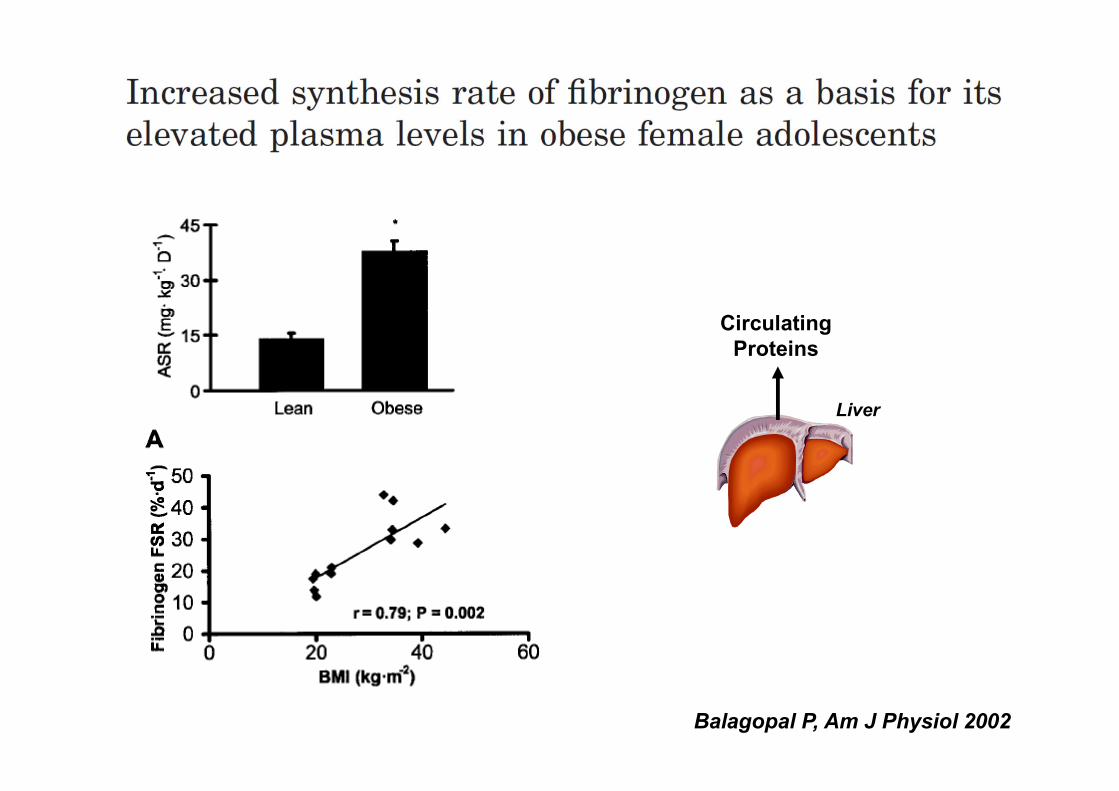
Balagopal P, Am J Physiol 2002
CirculatingProteins
Liver
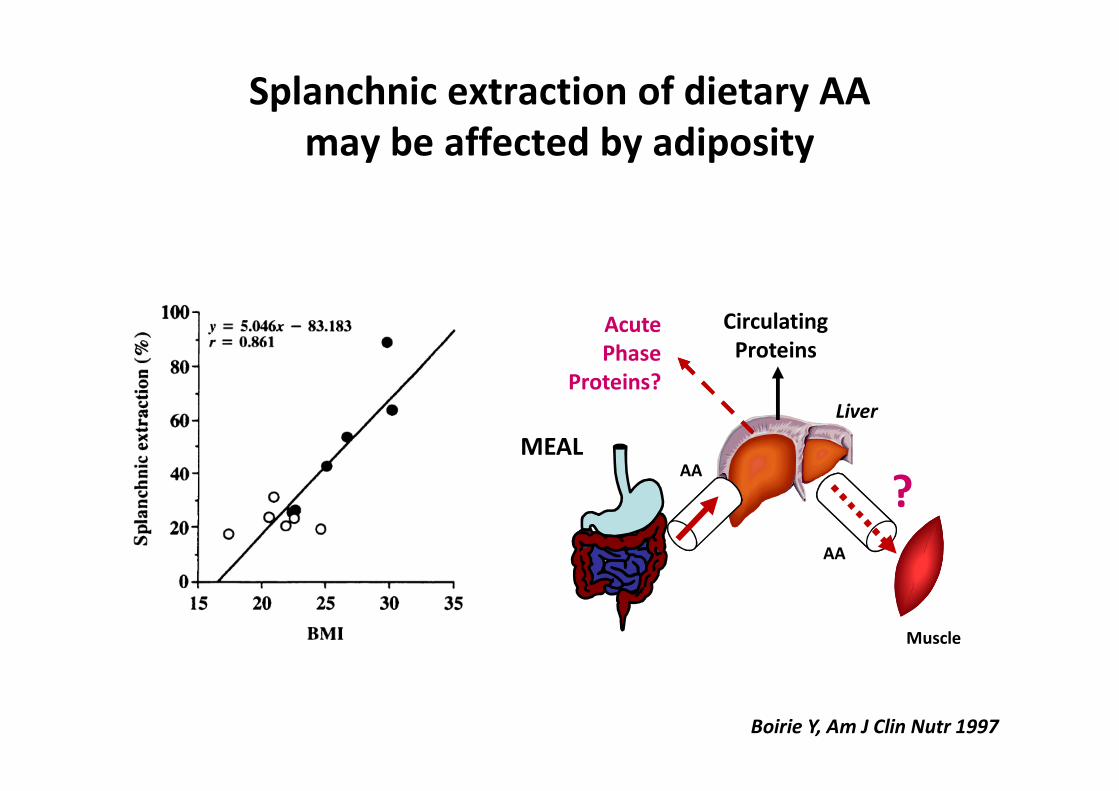
CirculatingProteins
AcutePhase
Proteins?
AA
AA
Muscle
?MEAL
Boirie Y, Am J Clin Nutr 1997
Splanchnic extraction of dietary AA may be affected by adiposity
Liver
Muscle
Intestine
Liver
KidneyAdiposetissue
Tissue protein metabolism in obesity
Free AA
Intake
Ox
23%
8%
69%
ProteinSynthesis?
↑ ProteinSynthesis
Changes in body and muscle composition in obesity
• Increased intramyocellular lipids
• Decreased oxidative capacity
• Mitochondrial dysfunction
• Less type 1 fibers
• More glycolytic fibers (type 2)
• Decreased capillary density
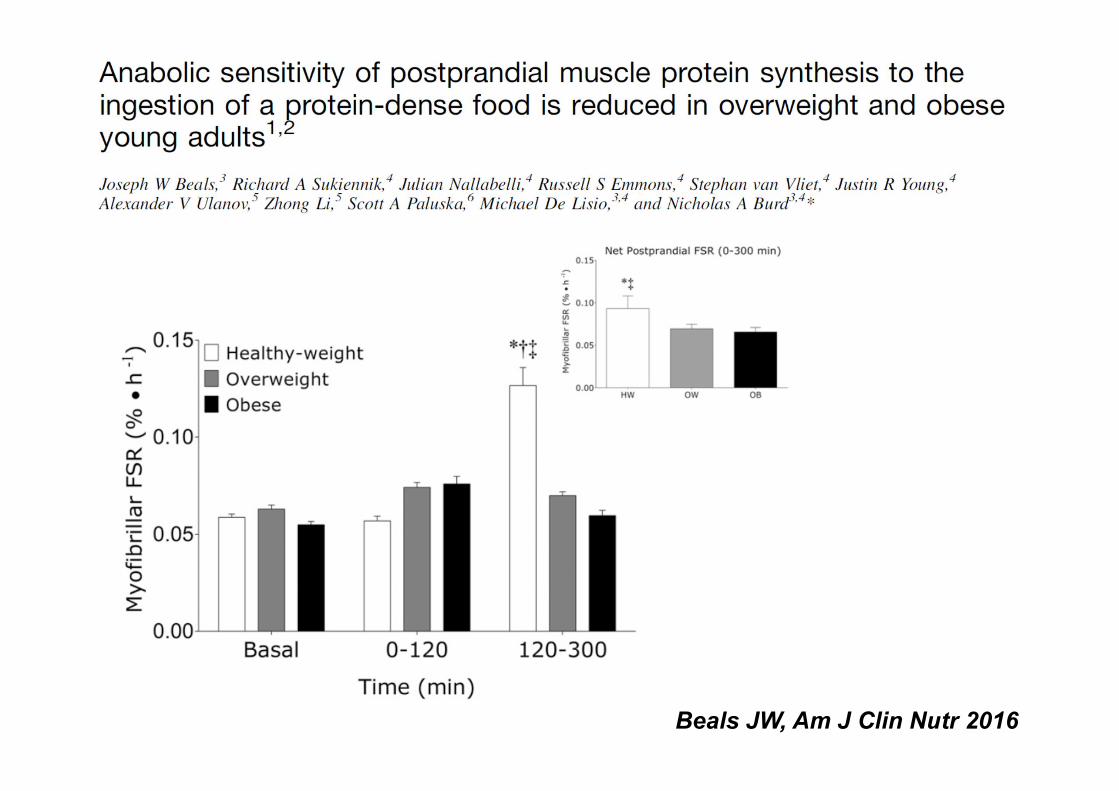
Beals JW, Am J Clin Nutr 2016
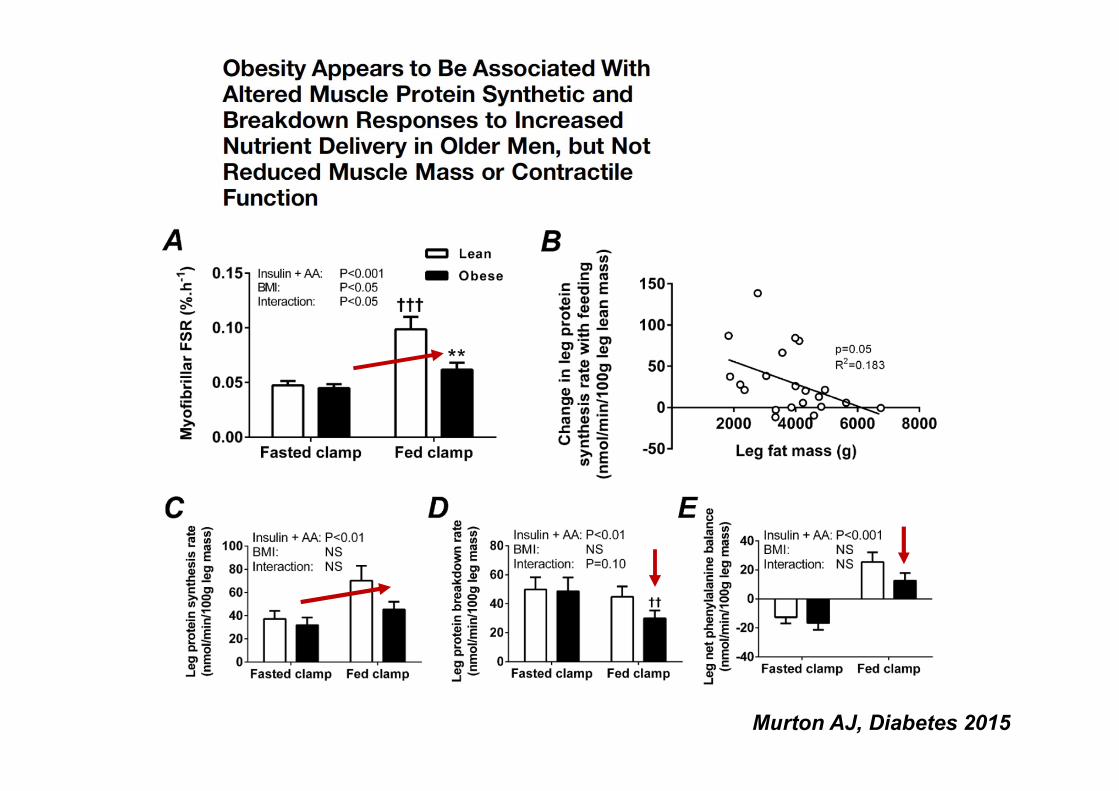
Murton AJ, Diabetes 2015
PostabsorptiveInsulin + AA clamp
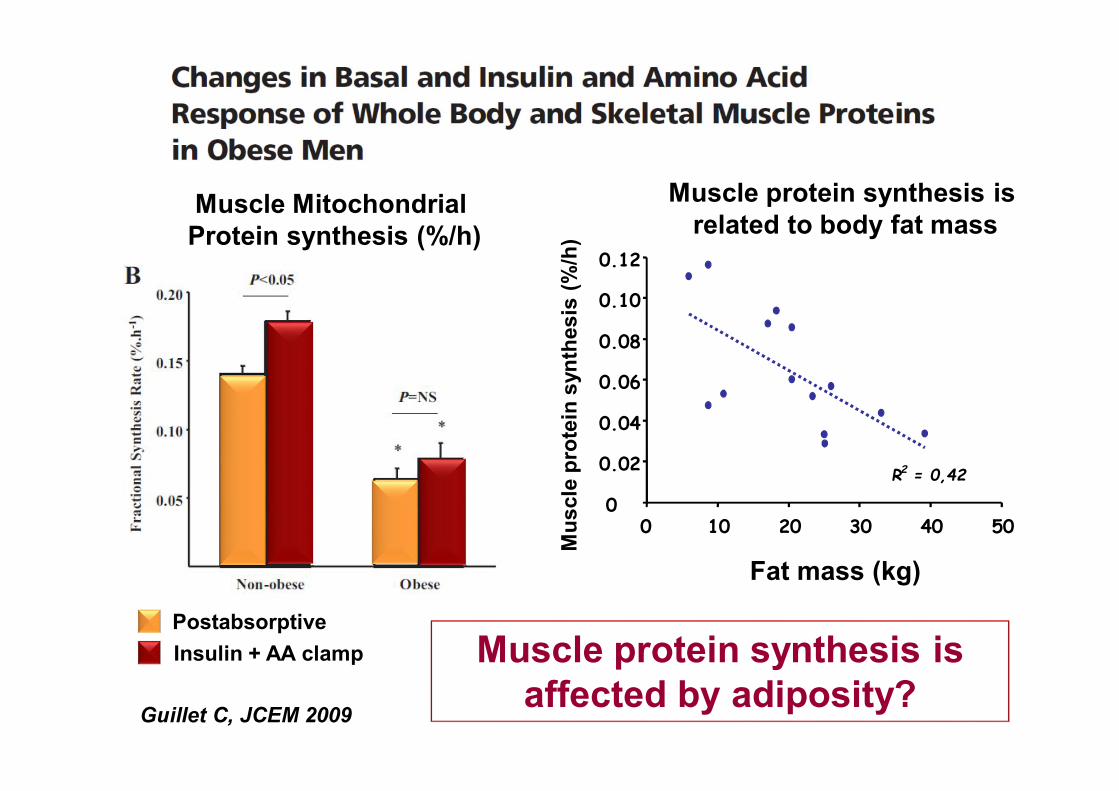
Guillet C, JCEM 2009
Muscle Mitochondrial Protein synthesis (%/h)
R2 = 0,42
0
0.02
0.04
0.06
0.08
0.10
0.12
0 10 20 30 40 50
Mus
cle
prot
ein
synt
hesi
s(%
/h)
Fat mass (kg)
Muscle protein synthesis isaffected by adiposity?
Muscle protein synthesis isrelated to body fat mass
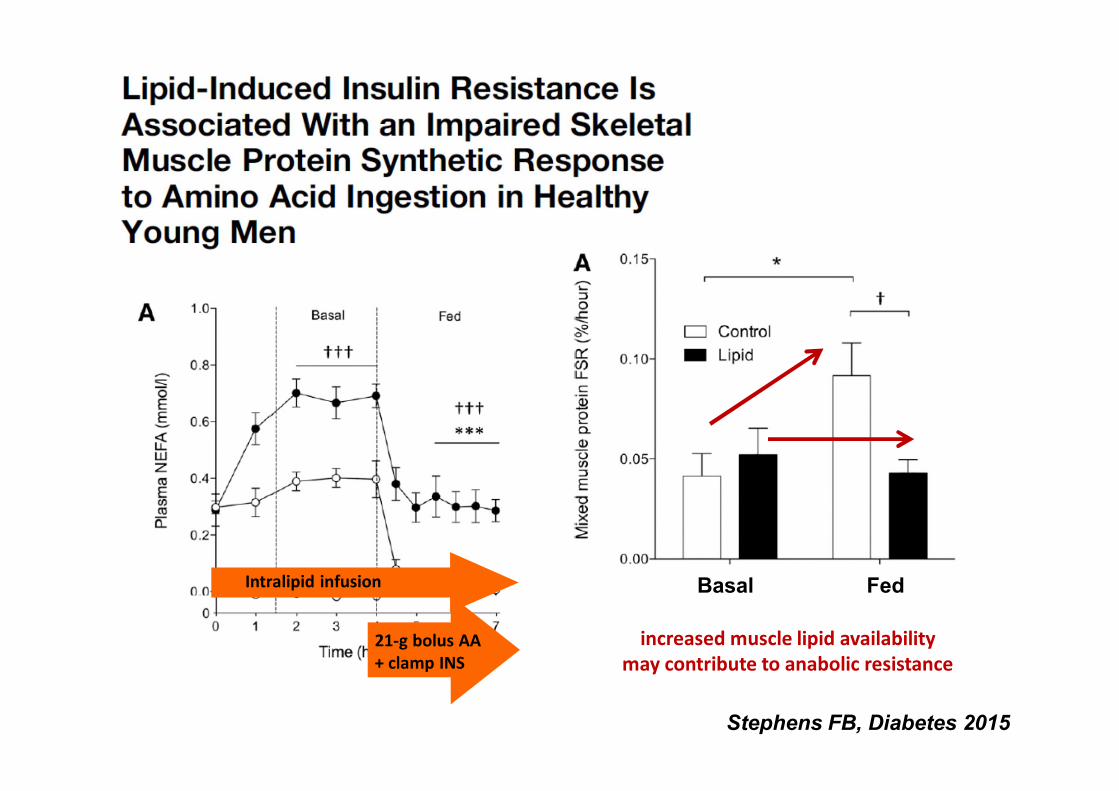
Stephens FB, Diabetes 2015
Basal FedIntralipid infusion
21-g bolus AA + clamp INS
increased muscle lipid availabilitymay contribute to anabolic resistance
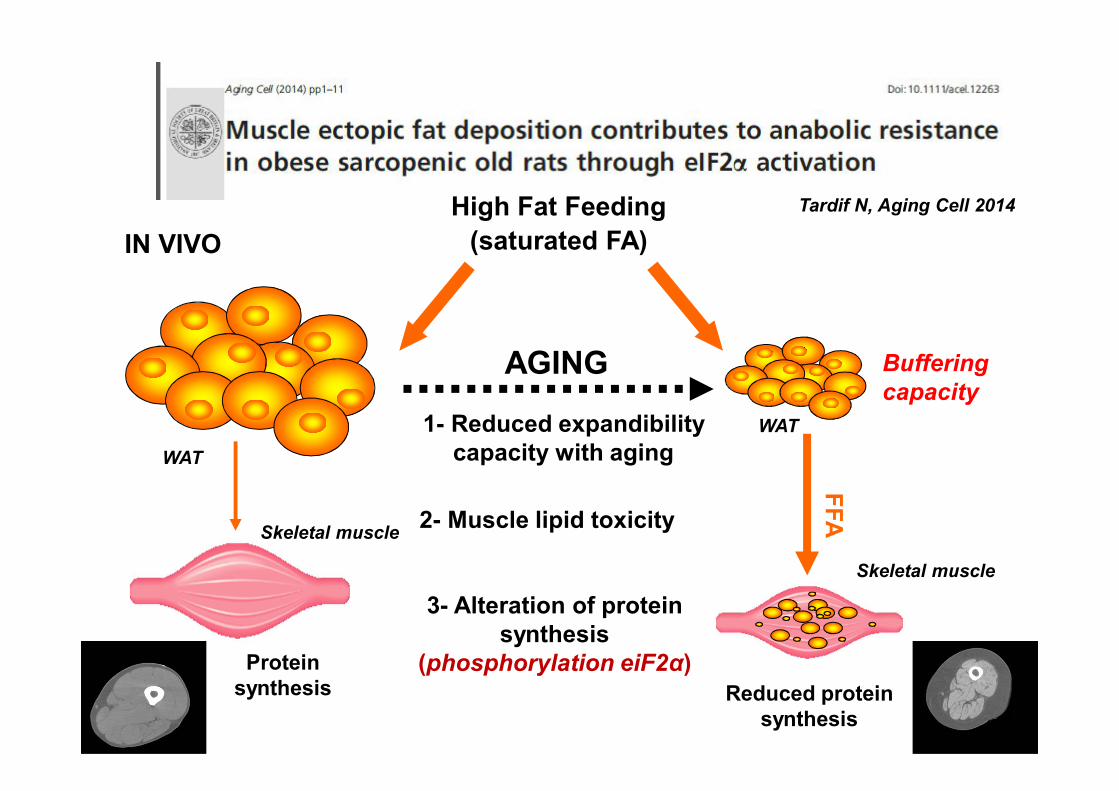
High Fat Feeding(saturated FA)
WAT
Buffering capacity
WAT1- Reduced expandibility capacity with aging
AGING
FFA2- Muscle lipid toxicity
Reduced protein synthesis
Skeletal muscle
3- Alteration of proteinsynthesis
(phosphorylation eiF2α)
IN VIVO
Protein synthesis
Skeletal muscle
Tardif N, Aging Cell 2014
Muscle protein metabolism is impaired in obesity
• Reduced muscle protein turnover and lesser contribution to whole body protein metabolism
• Lower muscle protein synthesis especially mitochondrial protein synthesis in response to insulin or to meal intake
• Intramyocellular lipids may affect muscle proteinmetabolism by interacting on translation initiation pathways
• Insulin resistance, inflammation and lipoxicity may limitprotein synthesis on a long term basis especially duringaging
Guillet C, Obes Rev 2012
Obésité et Métabolisme protéique
• Trop de gras ou trop peu de maigre ?
• Masse maigre, moteur du renouvellement
protéique : spécificités de l’obésité
• Applications cliniques potentielles
Clinical conditions associated with muscle lossand obesity (sarcopenic obesity)
• Hypercortisolism• Diabetes• Hypogonadism• Long-term immobilization• Chronic organ disease (CKD, COPD, HF)• Cancer, neurological disorders, …• Weight cycling ? Bariatric surgery ?
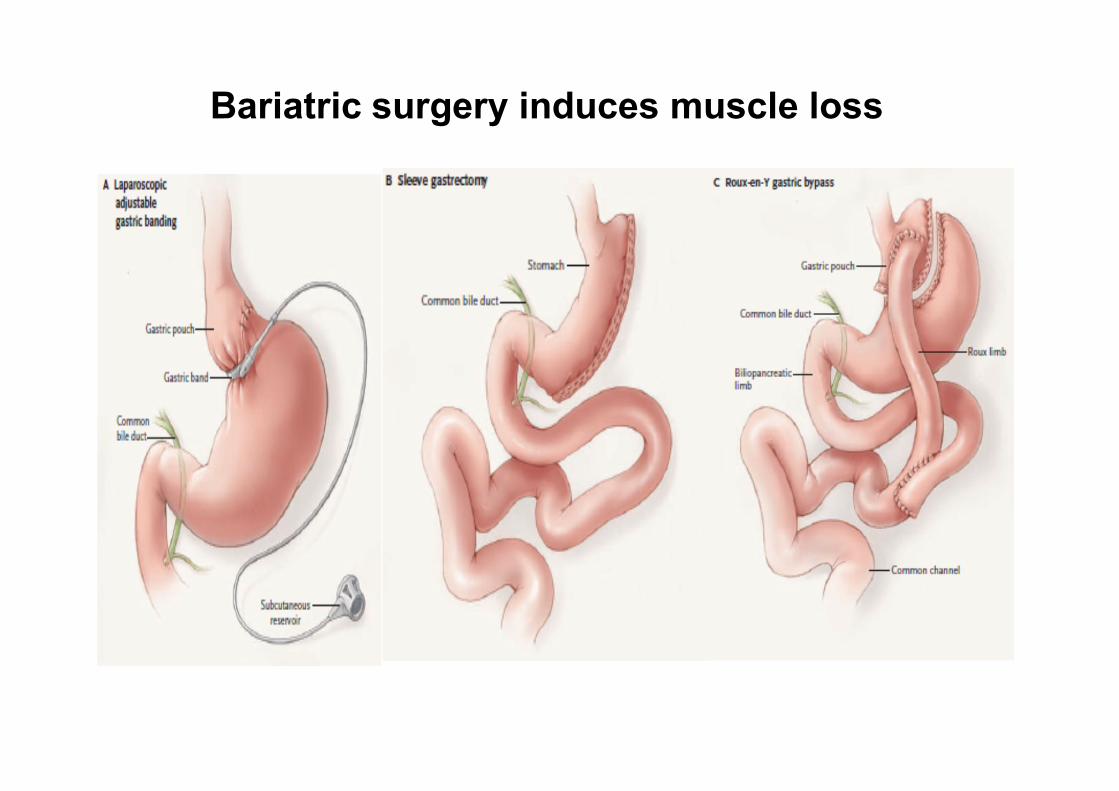
Bariatric surgery induces muscle loss
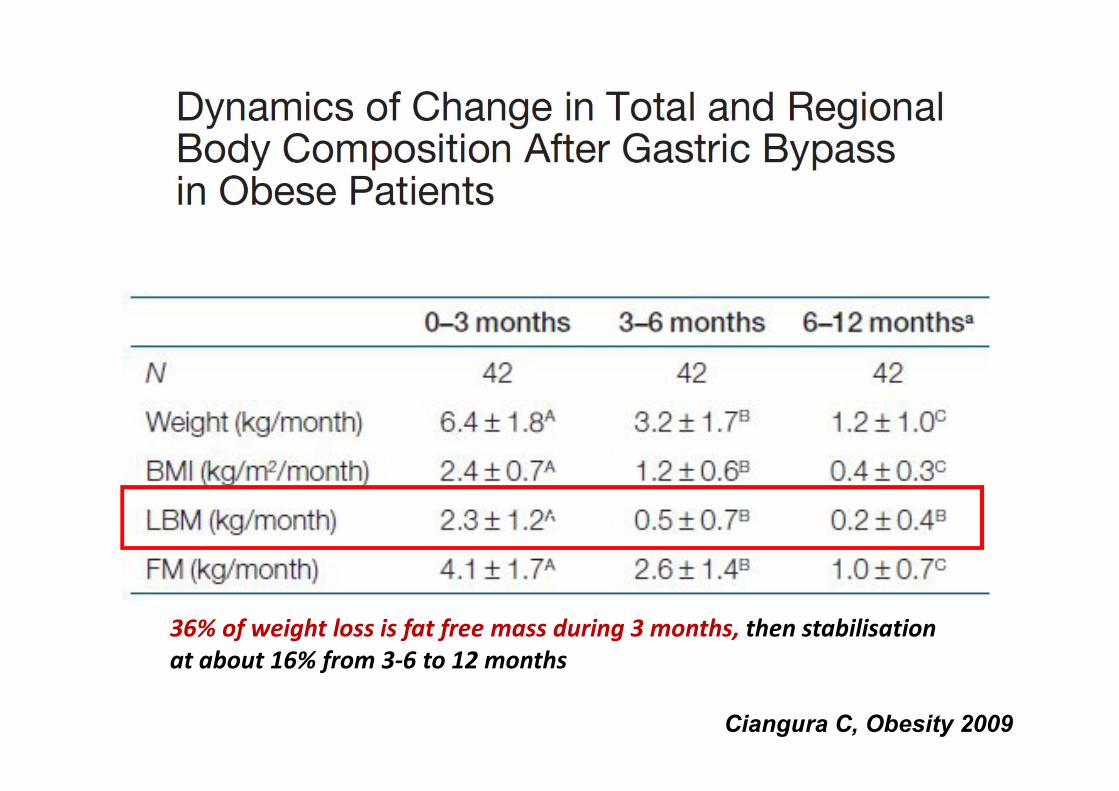
36% of weight loss is fat free mass during 3 months, then stabilisation at about 16% from 3-6 to 12 months
c
Ciangura C, Obesity 2009
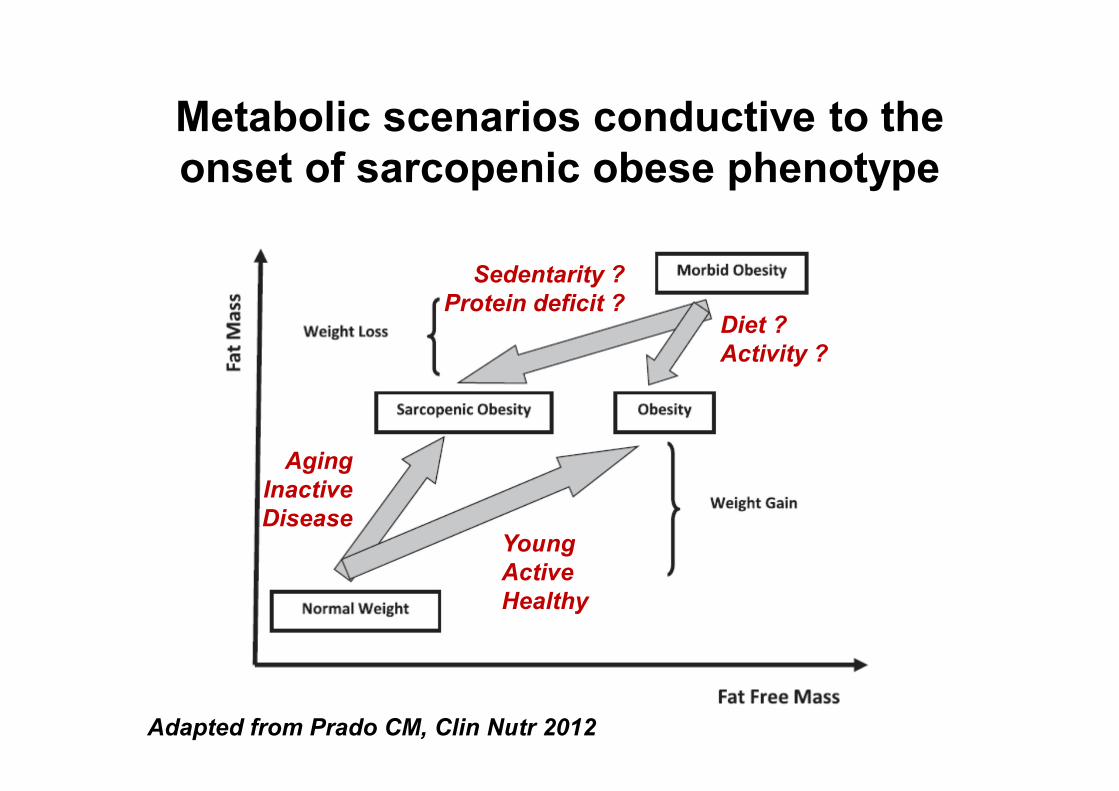
Metabolic scenarios conductive to the onset of sarcopenic obese phenotype
Young ActiveHealthy
AgingInactiveDisease
Diet ?Activity ?
Sedentarity ?Protein deficit ?
Adapted from Prado CM, Clin Nutr 2012
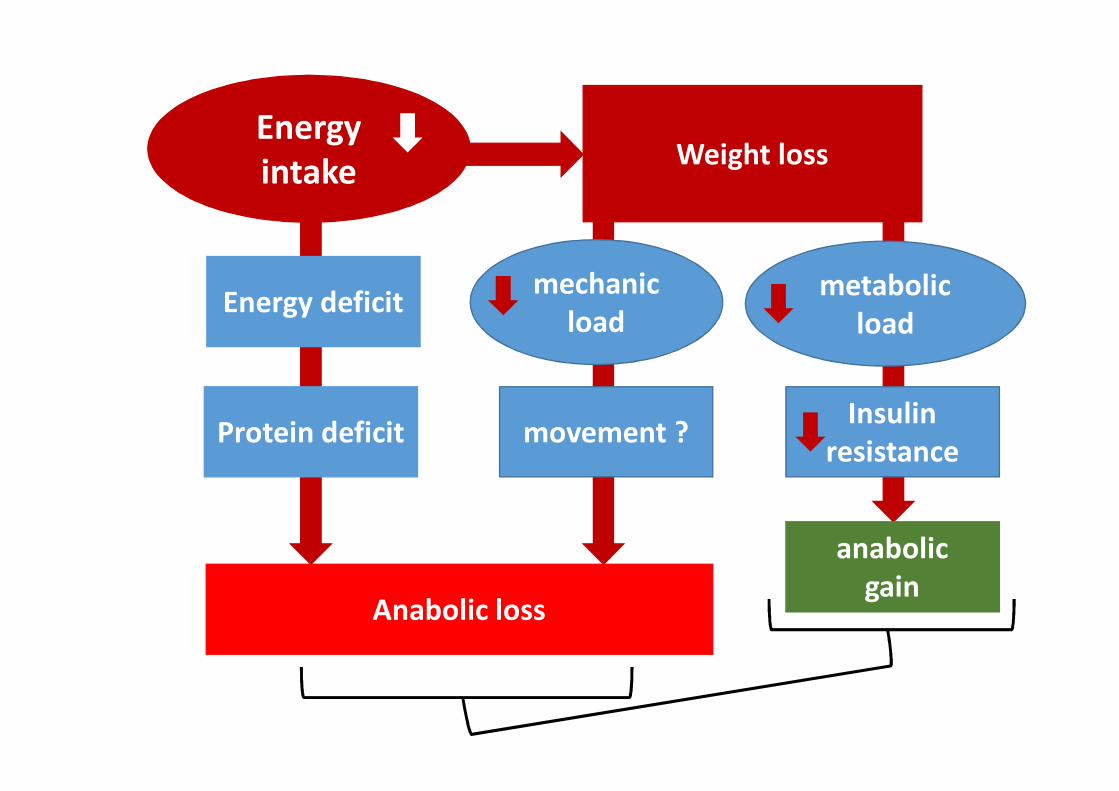
mechanicload
metabolicload
Insulinresistancemovement ?
anabolicgain
Energyintake
Protein deficit
Anabolic loss
Weight loss
Energy deficit
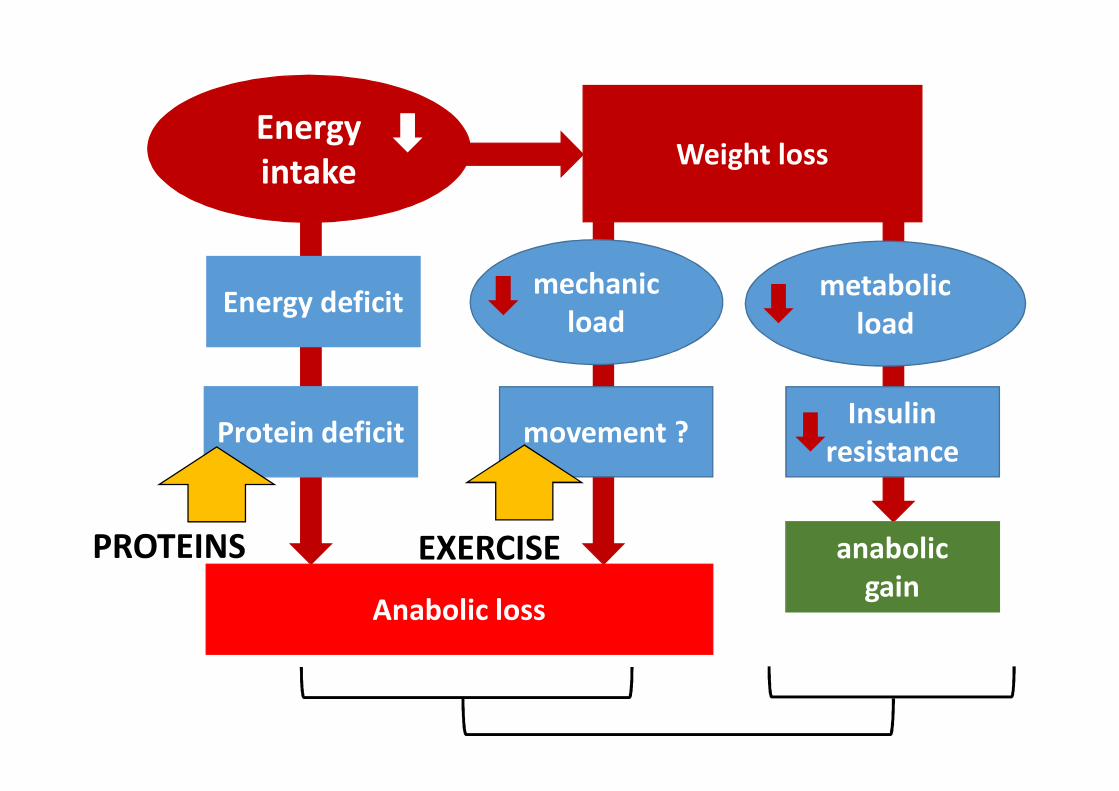
mechanicload
metabolicload
Insulinresistancemovement ?
anabolicgain
Energyintake
Protein deficit
Anabolic loss
Weight loss
Energy deficit
PROTEINS EXERCISE
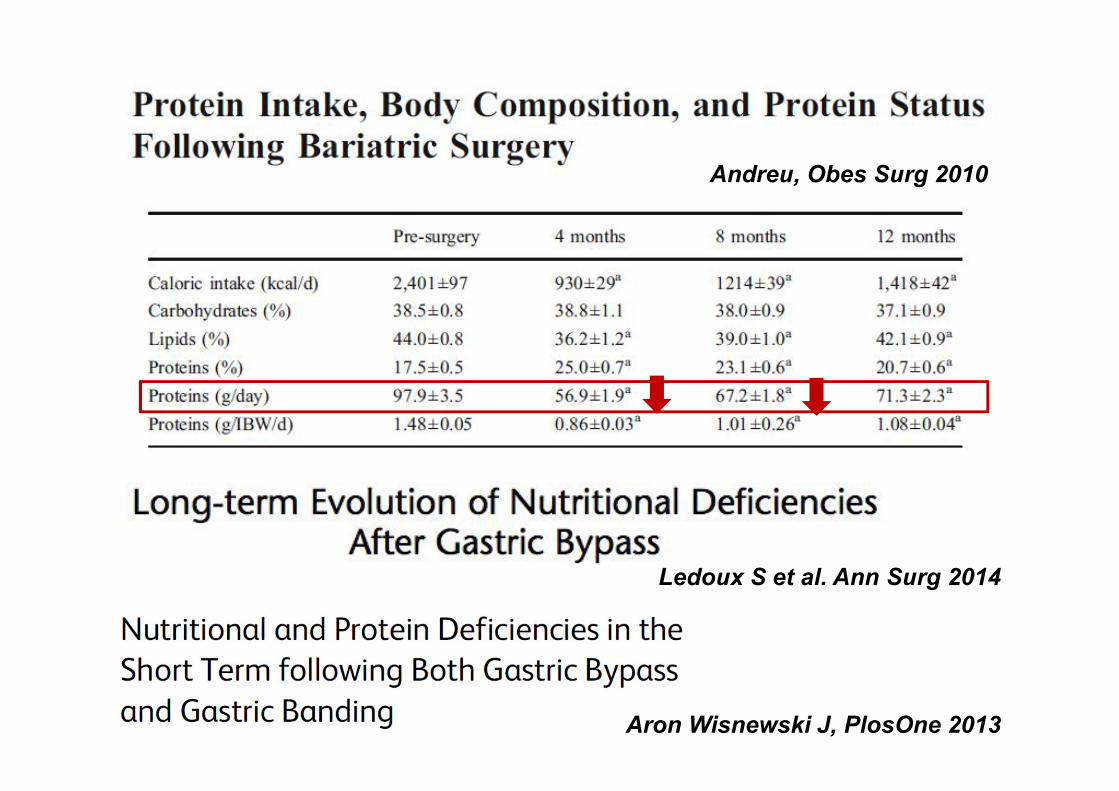
Andreu, Obes Surg 2010
Ledoux S et al. Ann Surg 2014
Aron Wisnewski J, PlosOne 2013
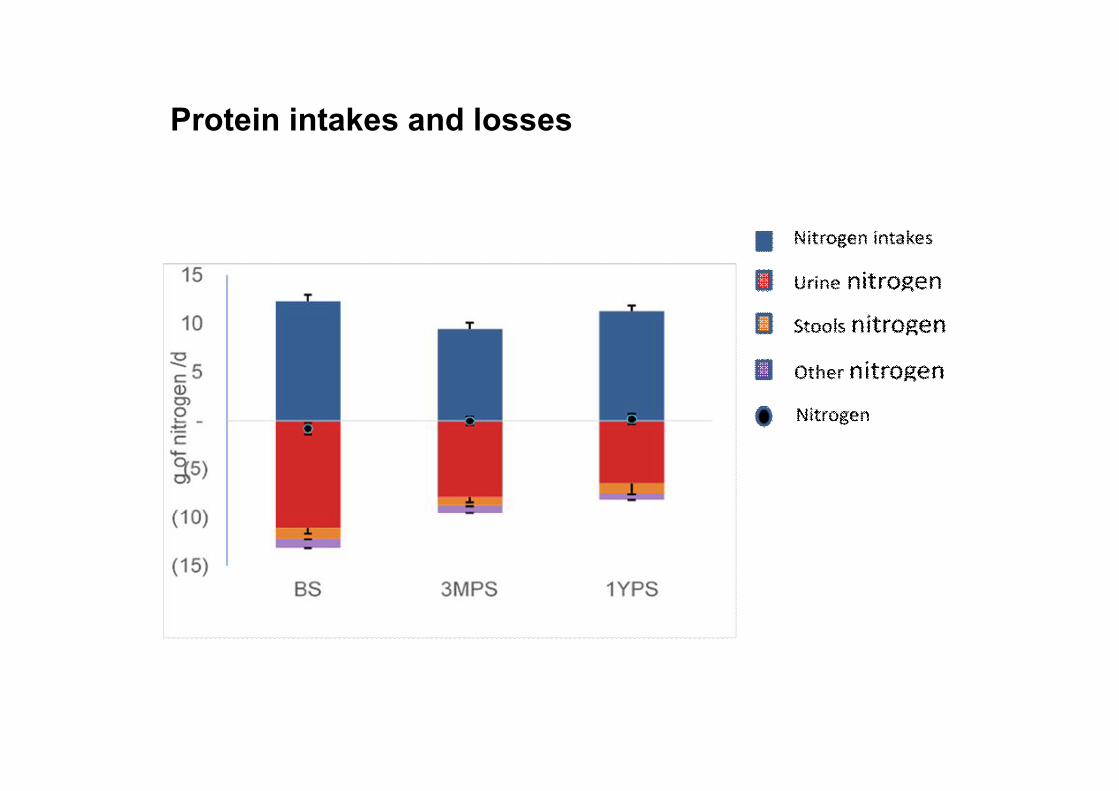
Protein intakes and losses
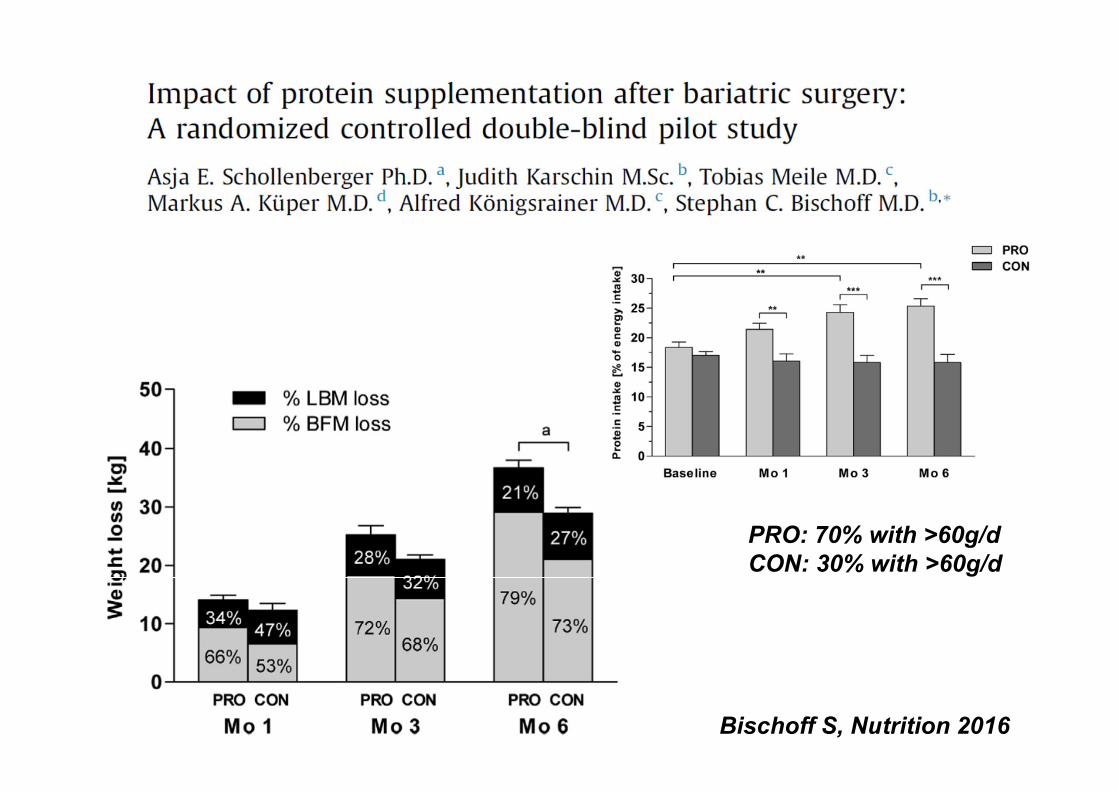
Bischoff S, Nutrition 2016
PRO: 70% with >60g/dCON: 30% with >60g/d
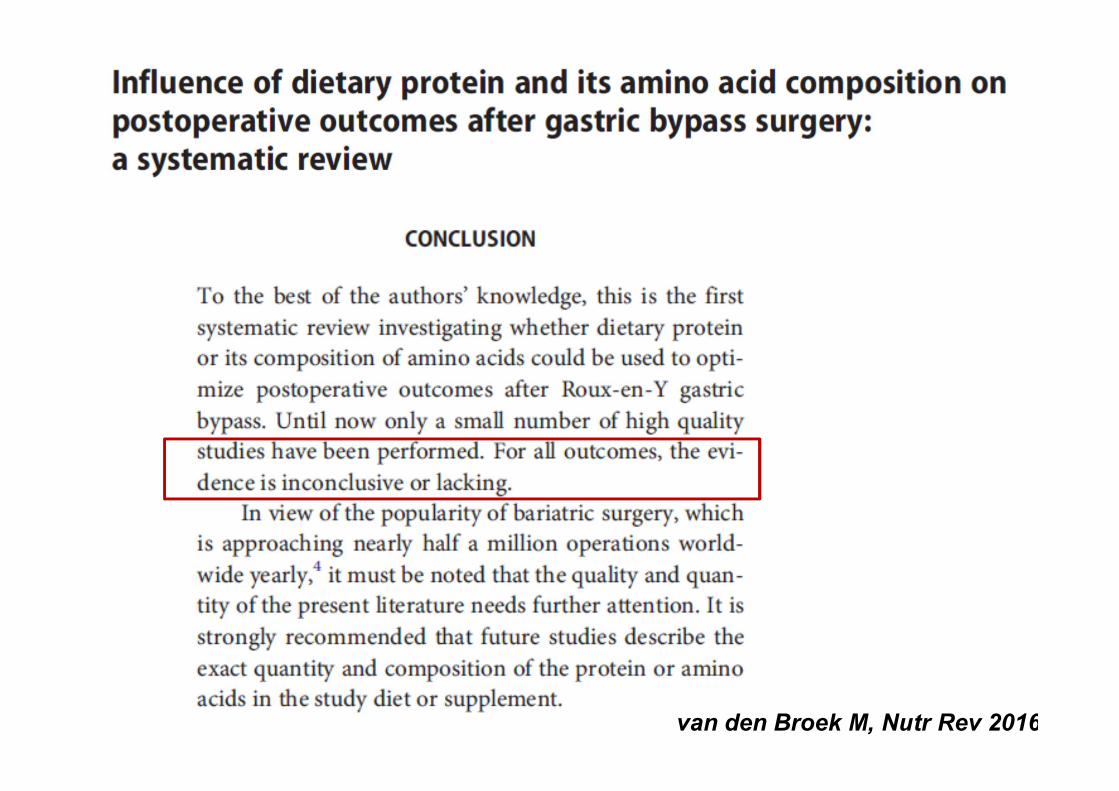
van den Broek M, Nutr Rev 2016
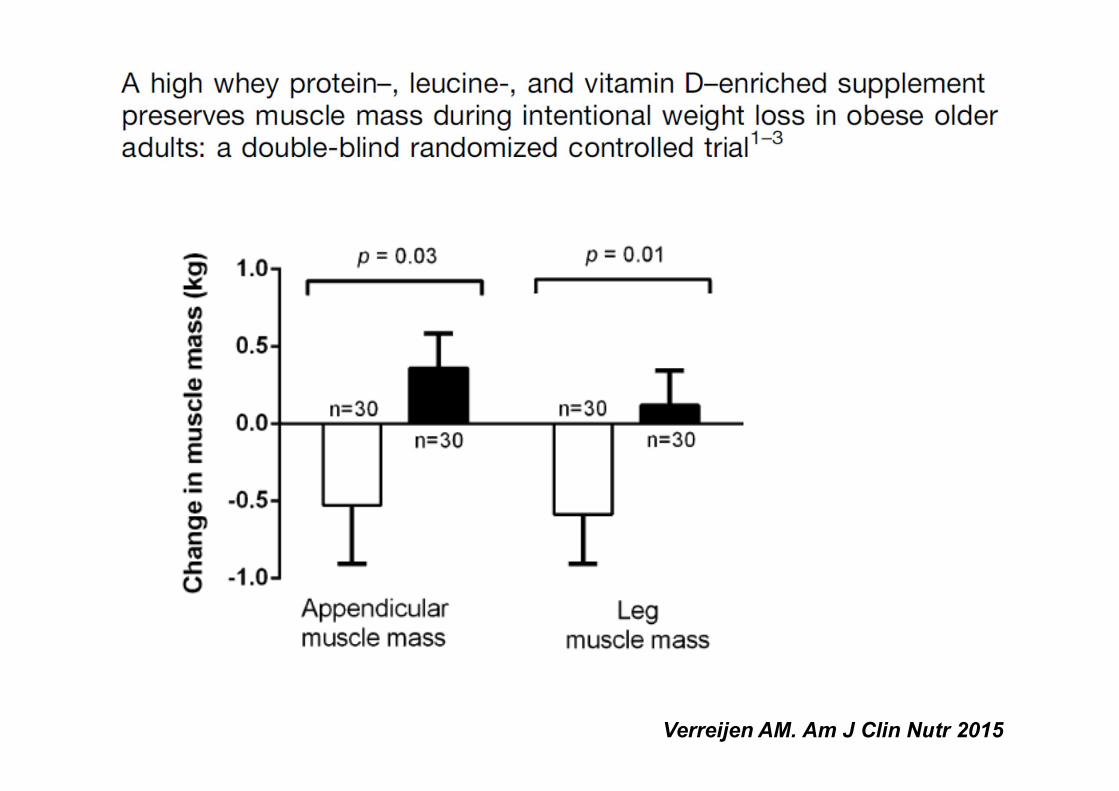
Verreijen AM. Am J Clin Nutr 2015
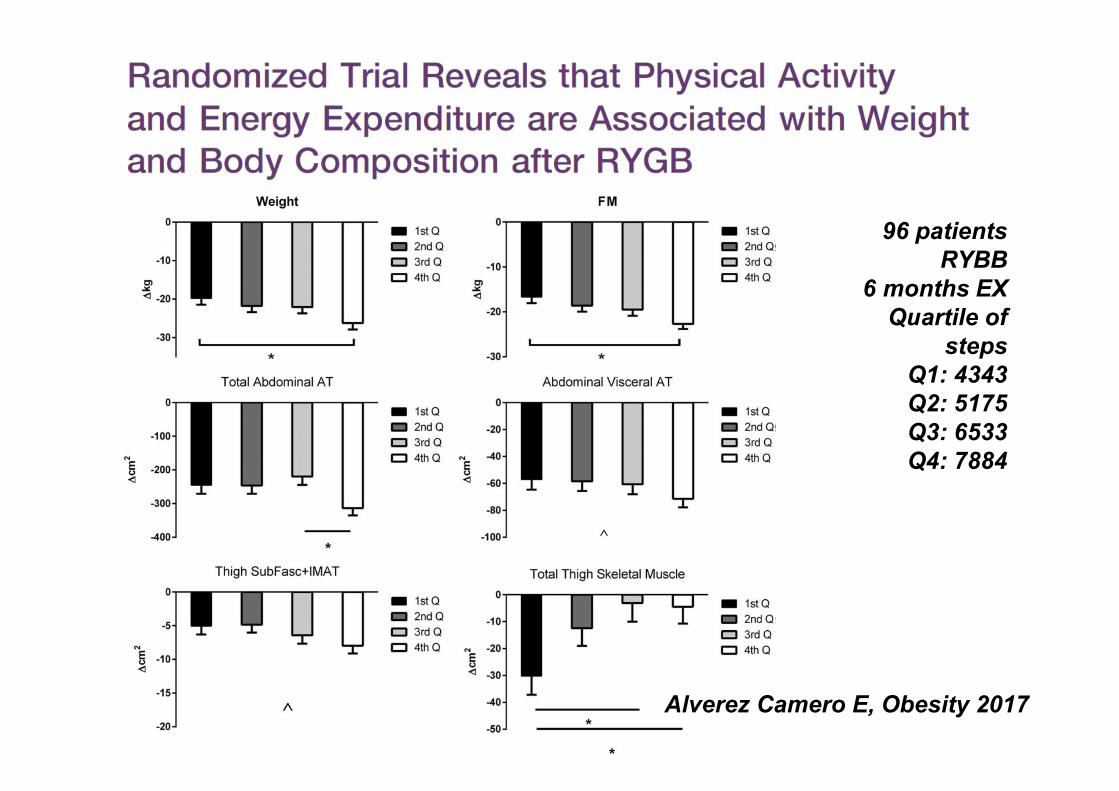
Alverez Camero E, Obesity 2017
96 patientsRYBB
6 months EXQuartile of
stepsQ1: 4343Q2: 5175Q3: 6533Q4: 7884
Conclusions
• Fat mass and fat free mass changes are not sodependent: FM/FFM ratio may be very variable among the obese population
• Ectopic muscle fat accumulation promotesanabolic resistance through signalling alterations
• Weight loss or gain over time may promotesarcopenic obesity development
• New strategies targeting muscle anabolicresistance in obesity should be proposed
Human Nutrition research Unit
Merci
Team “Diet and muscle -skeletal Health”