les nouvelles modalités de prise en charge des
TRANSCRIPT

1
Les nouvelles modalités de prise en charge des hépatopathies virales chez
le transplanté rénal
A. Vallet-PichardHépatologie, Hôpital Cochin
Inserm U 567
Cas clinique: VHB / TR• Femme , 03/05/1952, 55 kg, 1, 60 m• Histoire rénale
– Hémodialyse de 1985 à 1990 pour NIC– TR en 06 1990– Traitement IS actuel: solupred et prograf– Traitement HTA: amlor
• Histoire hépatique– Ag HBs + connu depuis 1987– 1988:
• ALAT N, ADN indétectable (< 1 000 000 copies/ml), • Ag HBe - Ac anti-HBe + sérologie VHD -• PBH : foie normal• Pas de traitement
2
Histoire hépatique suite…
• 1990-1998: – ALAT fluctuantes N à 2-3N– ADN entre 6 et 7 log (1 000 000 à 10 000 000 copies/ml)– Ag HBe +, Ac anti HBe -, sérologie VHD –– PBH 1992: A1 F1– Pas de traitement– PBH 1995: A2 F2 – Vaccinothérapie: échec– PBH 1998: A2F3– Lamivudine 100 mg/j (créatinine 86 μmol/l, 60ml/mn)
Histoire hépatique suite• 1998-2000: efficacité de la lamivudine biochimique et
virologique sans séroconversion e– Transaminases normales– ADN < 700 000 copies/ml– Ag HBe + Ac anti HBe-
• 2001:– Transaminases 2N– ADN 8 log, e+ / ae-– Plaquettes 200 000/mm3– Echographie: foie stéatosique– PBH: A2 F3 – Créatinine: 100 μmol/l cl 52 ml/mn
3
Questions
• A quoi correspond la remontée de la charge virale du VHB en 2001?
Réponses
• Echappement: réascension d’au moins 1 log de l’ADN du VHB sous traitement antiviral
(Rechute: réascension d’au moins 1 log de l’ADN du VHB après arrêt du traitement antiviral)Résistance à la lamivudine: mutant YMDD

4
Questions
• Quel traitement proposez-vous à ce stade ?
Réponses
• Adefovir (Hepsera 10 mg/j) avec surveillance de la créatinine en association avec la lamivudine
• Adaptation posologique en fonction de la clairance• Toxicité rénale pour des doses de 60 à 120 mg/j
Adaptation en fonction de la clairance de la créatinineCl > 80 ml/mn 10 mg/j50 < Cl < 80 ml/mn 10 mg/2 j20 < Cl < 49 ml/mn 10 mg/3 j10 < Cl < 20 ml/mn 10 mg/4 jdialysis 10 mg/7 j

5
Histoire hépatique suite• Entre 2002 et 2005:
– Normalisation des transaminases– e+ / e-– ADN < 3 log– Echographie: stéatose
• En 2006 – ALAT 2N, – ADN 5 log, e+ / ae –– Echographie: stéatose– Plaquettes: 140 000– PBH: A3 F4, stéatose 35%– Créatinine 100 μmol/l (48 ml/mn)
Questions
• A quoi correspond la remontée de la CV du VHB?
• Quel traitement doit-on proposer?
• Pourquoi refaire une PBH? Les tests non invasifs sont-ils validés?
6
Réponses
• Echappement à l’adéfovir: recherche des mutations de résistance à l’adéfovir
• Disponibilité du Baraclude (entecavir) – 1mg/j en cas de résistance à la lamivudine– 0,5 mg/j chez les non résistants– à adapter à la fonction rénale selon recommandation du
laboratoire • Pas de validation des test FibroTest / FibroScan dans la
population rénale infectée par le VHB
Questions
• Comment doit-on surveiller cette patiente?
• S’il y avait une indication à une 2ème TR (dégradation de la fonction rénale), que ferait-on du foie?

7
Réponses
• Surveillance d’une cirrhose– Echographie tous les 4 à 6 mois avec dosage de l’AFP
dépistage CHC– FOGD: dépistage HTP
• Si VO g 2 et 3: béta-bloquant / ligature de VO prophylactique
• Si VO g 1: FOGD tous les 2 ans• Si pas de VO: FOGD tous les 3 ans
• Il n’y a plus d’indication à une greffe hépatique associée en cas de cirrhose compensée
Cas cliniques: VHC/TR
• Homme 12/03/1960• Originaire du Maghreb• Hémodialyse de 1995 à 2005• En France depuis 2004• TR depuis 06/2006: cellcept, neoral, cortancyl• VHC G1 (CV: 6 log) post TS 1988• PBH 01/2004 A0F0
8
Question
• Y a-t-il une indication thérapeutique à ce stade?
• Si oui, quel traitement doit-on proposer?
Réponses
• En théorie: non car A0F0, G1, forte CV
• En pratique: oui chez le patient hémodialysé à visée d’éradication virale avant la TR
• Traitement par interferon standard 3MU X 3 /sem après la dialyse
9
Histoire hépatique suite
• Le patient négative sa PCR à M3, elle reste négative à M6 et à M12
• Le patient garde une PCR négative 6 mois après l’arrêt du traitement.
• Il est transplanté en juin 2006.
Questions
• Si le patient avait été non répondeur ou rechuteur, pouvait-il être transplanté?
• Si le patient avait été cirrhotique initialement, pouvait-il être transplanté?
10
Réponses
• TR possible chez les non répondeurs: (PCR constamment positive pendant le ttt) et les rechuteurs (repositivation de la PCR dans les 6 mois suivant l’arrêt du traitement antiviral)
• En cas de cirrhose: double greffe
Questions
• Si le patient est transplanté alors que la PCR virale C est positive, quelles sont les options thérapeutiques?
• Comment doit-on le surveiller?
11
Réponses
• Interféron pégylé contre-indiqué• Ribavirine en monothérapie si F3F4• Privilégier le foie au risque d’un retour en dialyse
lorsque la maladie hépatique est grave (FHC, cirrhose très active)
• Surveillance: biologie standard, (FT ?, FS ?), échographie par an en l’absence de cirrhose (par 4 à 6 mois en cas de F4)
HBV and HCV infection in renal failure
• Frequent: - HBV < 5% (45% before 1985)- HCV: 10 to 65%
Prevalence is decreasing with antiHBV vaccination, blood screening and universal precautions
• Infections: transfusion-acquired before 1989nosocomial (allograft) and community-acquired
• Replication: long lasting 75% HBV & 90 to 100% HCV
• High viremia in kidney recipients (cholestatic hepatic fibrosis)Zylberberg et al. Transplantation 1998
12
HBV and HCV infection in renal failure
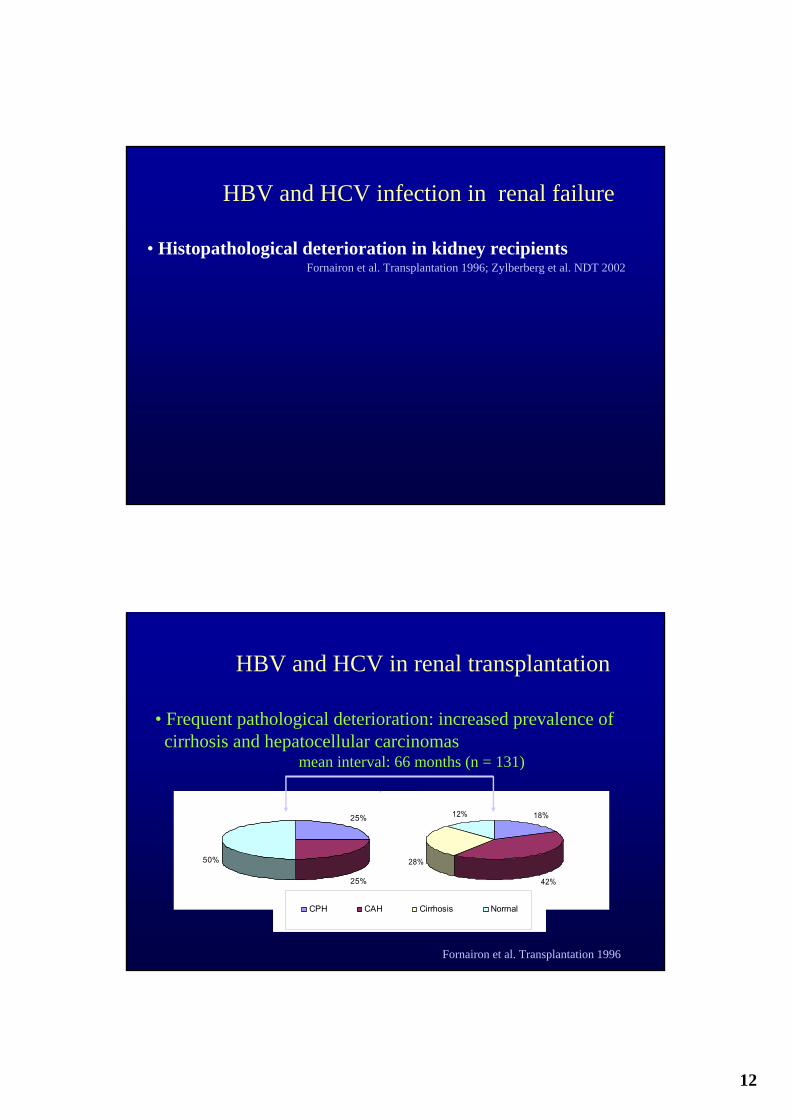
• Histopathological deterioration in kidney recipientsFornairon et al. Transplantation 1996; Zylberberg et al. NDT 2002
25%
25%
50%
18%
42%
28%
12%
CPH CAH Cirrhosis Normal
HBV and HCV in renal transplantation
• Frequent pathological deterioration: increased prevalence of cirrhosis and hepatocellular carcinomas
mean interval: 66 months (n = 131)
Fornairon et al. Transplantation 1996
13
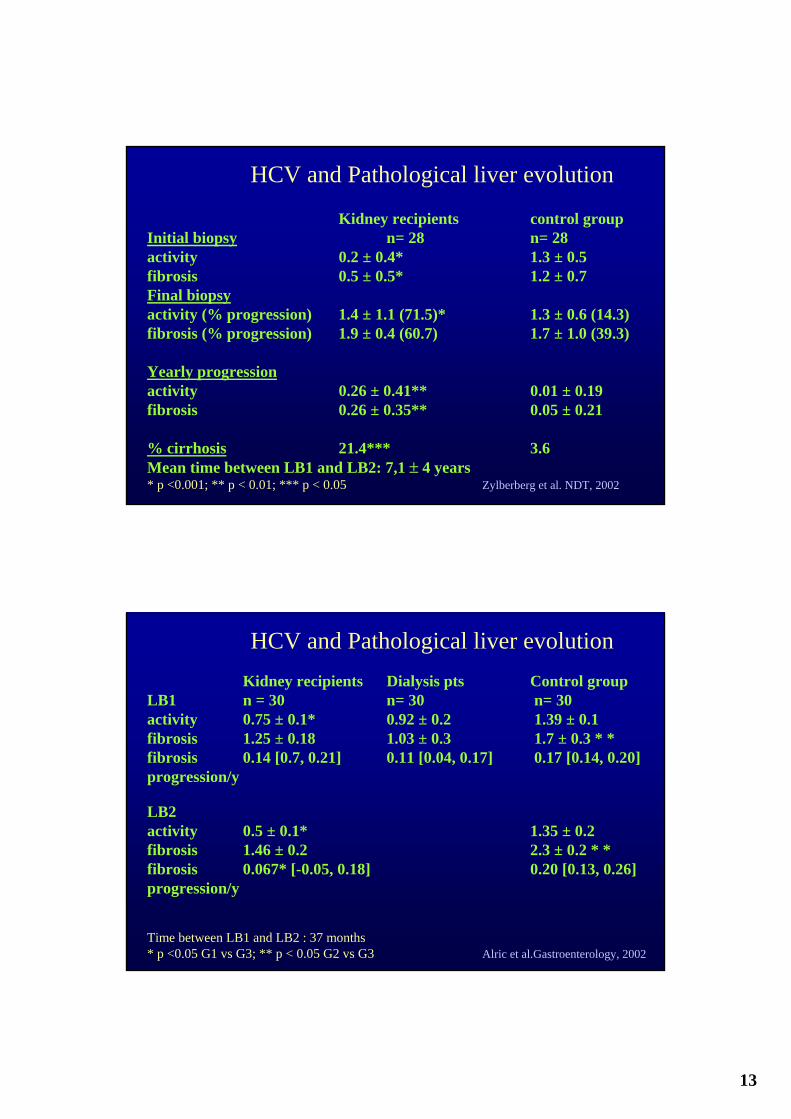
Kidney recipients control groupInitial biopsy n= 28 n= 28activity 0.2 ± 0.4* 1.3 ± 0.5fibrosis 0.5 ± 0.5* 1.2 ± 0.7Final biopsyactivity (% progression) 1.4 ± 1.1 (71.5)* 1.3 ± 0.6 (14.3)fibrosis (% progression) 1.9 ± 0.4 (60.7) 1.7 ± 1.0 (39.3)
Yearly progressionactivity 0.26 ± 0.41** 0.01 ± 0.19fibrosis 0.26 ± 0.35** 0.05 ± 0.21
% cirrhosis 21.4*** 3.6Mean time between LB1 and LB2: 7,1 ± 4 years* p <0.001; ** p < 0.01; *** p < 0.05 Zylberberg et al. NDT, 2002
HCV and Pathological liver evolution
Kidney recipients Dialysis pts Control groupLB1 n = 30 n= 30 n= 30activity 0.75 ± 0.1* 0.92 ± 0.2 1.39 ± 0.1fibrosis 1.25 ± 0.18 1.03 ± 0.3 1.7 ± 0.3 * *fibrosis 0.14 [0.7, 0.21] 0.11 [0.04, 0.17] 0.17 [0.14, 0.20] progression/y
LB2 activity 0.5 ± 0.1* 1.35 ± 0.2fibrosis 1.46 ± 0.2 2.3 ± 0.2 * *fibrosis 0.067* [-0.05, 0.18] 0.20 [0.13, 0.26] progression/y
Time between LB1 and LB2 : 37 months* p <0.05 G1 vs G3; ** p < 0.05 G2 vs G3 Alric et al.Gastroenterology, 2002
HCV and Pathological liver evolution

14
HBV and HCV infection in renal failure • Histopathological deterioration in kidney recipients but stability in dialysis patients (cirrhosis: 10%)
• Negative impact of chronic infection on- patients survival- allografts survival
Hiesse et al. Clin Transplant 1992; Parfrey et al. Transplantation 1984; Legendre et al. Transplantation 1997
Mathurin et al. Hepatology 1999; 29: 257
Renal transplantationSurvival according to HCV and HBV status
15
HBV and HCV infection in renal failure • Histopathological deterioration in kidney recipients but stability in dialysis patients (cirrhosis: 10%)
• Negative impact of chronic infection on- patients survival- allografts survival
• Drug-related hepatitis (azathioprine)Pol et al. Transplantation 1996
HBV and HCV infection in renal failure
• Histopathological deterioration in kidney recipients but stability in dialysis patients (cirrhosis: 10%)
• Negative impact of chronic infection on- patients survival- allografts survival
• Drug-related hepatitis (azathioprine)Pol et al. Transplantation 1996
• Negative impact of HCV on survival of dialysis patients8-year survival: 52 vs. 32%
Espinosa et al. NDT 2001

16
Consequences of the impact of allograft on viral hepatitis
• To diagnose
• To prevent
• To evalute
• To treat
HBs Ag HBV DNA by PCRAntiHBs/antiHBc Liver biopsy (or bio-markers?)
VaccinationYearly serological Treatment ?Follow-up
+
_
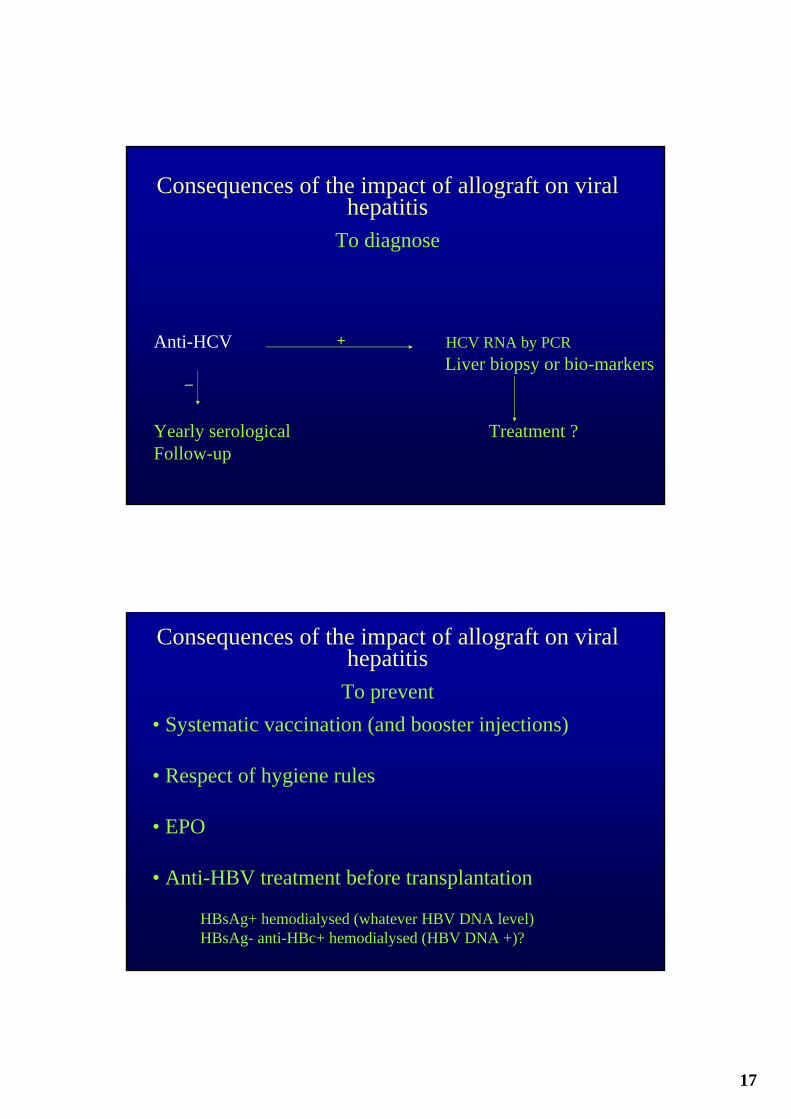
Consequences of the impact of allograft on viral hepatitis
To diagnose
17
Anti-HCV HCV RNA by PCRLiver biopsy or bio-markers
Yearly serological Treatment ?Follow-up
+
_
Consequences of the impact of allograft on viral hepatitis
To diagnose
• Systematic vaccination (and booster injections)
• Respect of hygiene rules
• EPO
• Anti-HBV treatment before transplantation
HBsAg+ hemodialysed (whatever HBV DNA level)HBsAg- anti-HBc+ hemodialysed (HBV DNA +)?
Consequences of the impact of allograft on viral hepatitis
To prevent

18
Reactivation hepatitis (fulminant hepatitis in 25%)- at initiation of immunosuppressive regimen - after modification
Cholestatic hepatic fibrosis
Consequences of the impact of allograft on viral hepatitis
To prevent
Chan et al. Hepatology, 2002
Pre-emptive treatment by nuc. analogues
Liver biopsyMETAVIR:Fibrosis/activity
F1 F2 F3
F4F0
Consequences of the impact of allograft on viral hepatitis
To evaluate

19
Haptoglobin
Alpha2Macroglobulin
Apolipoprotein A1
Bilirubinemia
Gamma GT
In Situ SerumLiver Injury
Activated Stellate Cells
Scar Matrix
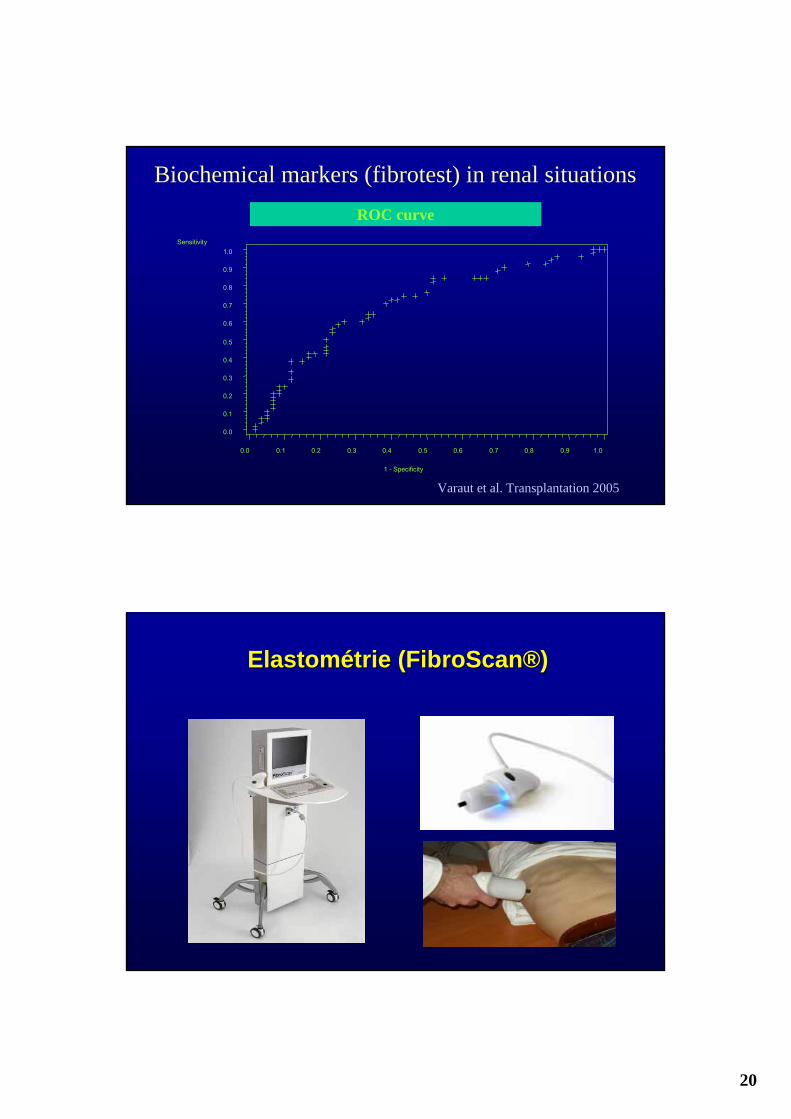
Biochemical markers (fibrotest) in renal situations
757872Diagnosticaccuracy
252228% discordance
170.71
130.69
40.75
Score > 0.6PPV (F2-4)
350.77
140.86
21 0.71
Score < 0.2NPV (F≤1)
Totaln = 110
Txn = 60
Dialysisn = 50
Biochemical markers (fibrotest) in renal situations
Mean length : 19 ± 7 mm; mean portal spaces n : 14 ± 7; 50 patients (45%) ≥ F2Varaut et al. Transplantation 2005
20
Sensitivity
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
1 - Specificity
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
Biochemical markers (fibrotest) in renal situationsROC curve
Varaut et al. Transplantation 2005
ElastométrieElastométrie ((FibroScanFibroScan®®))
21
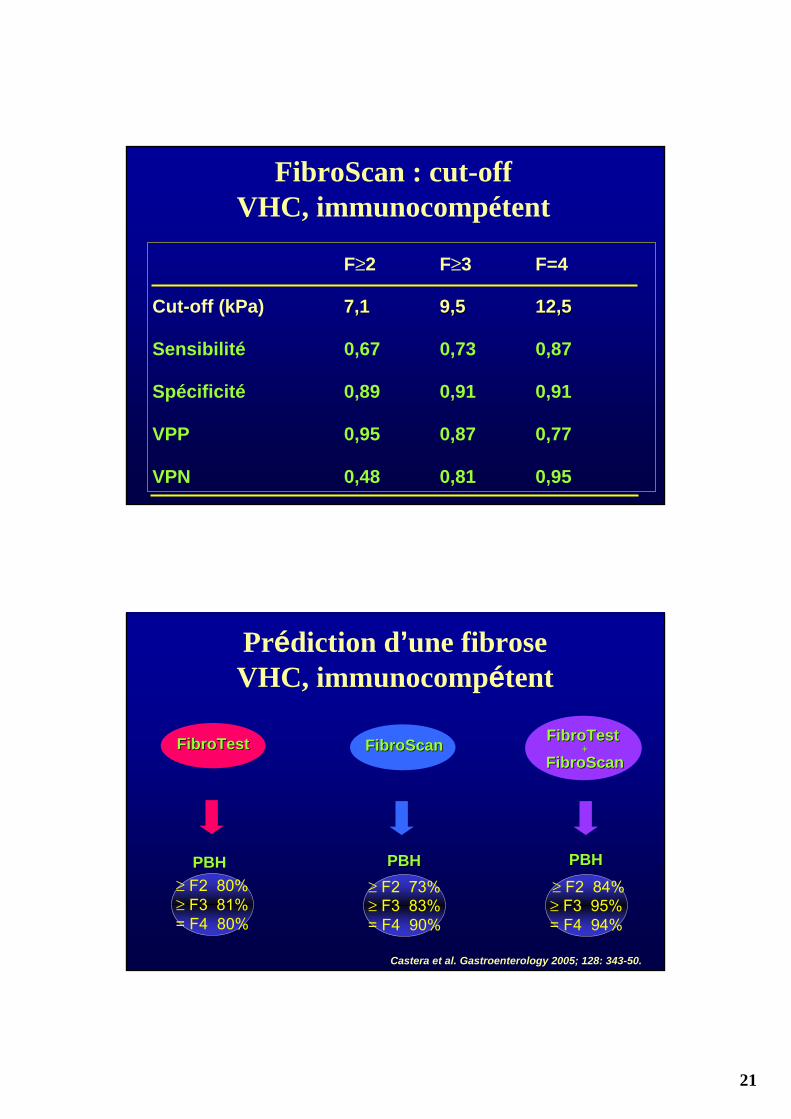
FibroScan : cut-offVHC, immunocompétent
F≥2 F≥3 F=4
Cut-off (kPa) 7,17,1 9,59,5 12,512,5
Sensibilité 0,67 0,73 0,87
Spécificité 0,89 0,91 0,91
VPP 0,95 0,87 0,77
VPN 0,48 0,81 0,95
Prédiction d’une fibroseVHC, immunocompétent
FibroTestFibroTest FibroScanFibroScan FibroTest FibroTest ++
FibroScanFibroScan
PBHPBH≥ F2 80%≥ F3 81%= F4 80%
≥ F2 84%≥ F3 95%= F4 94%
PBHPBH≥ F2 73%≥ F3 83%= F4 90%
PBHPBH
Castera et al. Gastroenterology 2005; 128: 343-50.
22
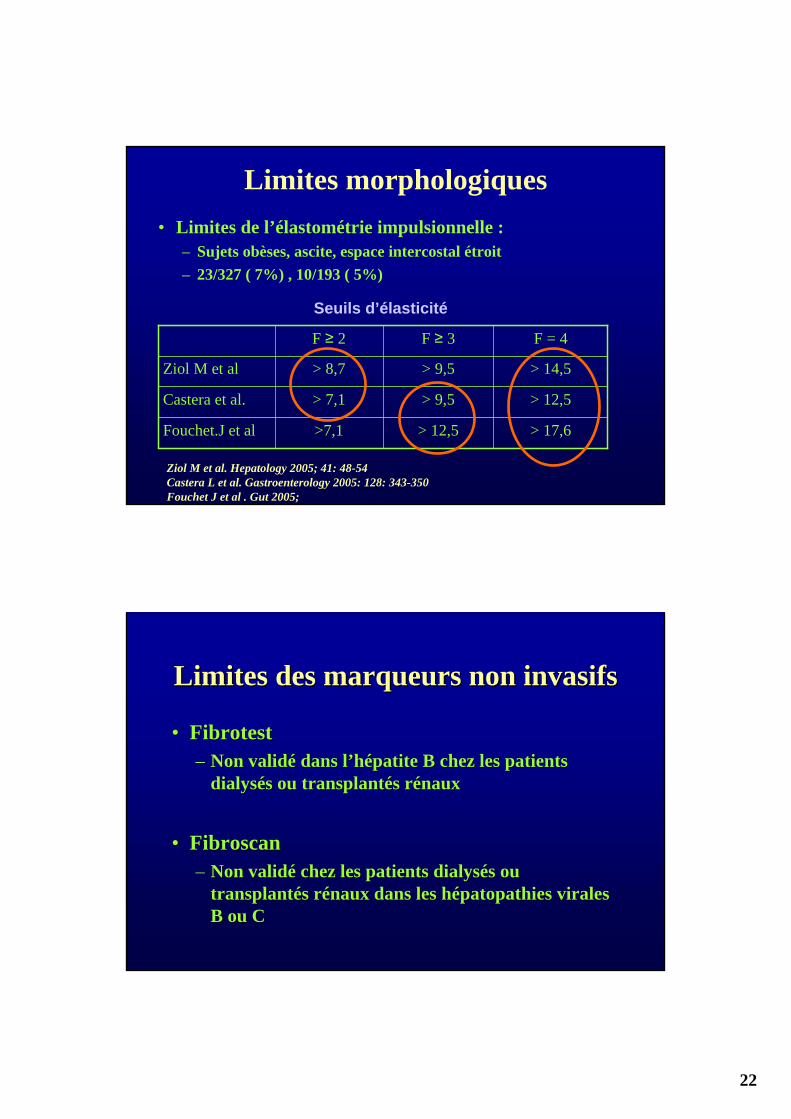
Limites morphologiques• Limites de l’élastométrie impulsionnelle :
– Sujets obèses, ascite, espace intercostal étroit – 23/327 ( 7%) , 10/193 ( 5%)
Ziol M et al. Hepatology 2005; 41: 48-54Castera L et al. Gastroenterology 2005: 128: 343-350Fouchet J et al . Gut 2005;
> 17,6> 12,5>7,1Fouchet.J et al
> 12,5> 9,5> 7,1Castera et al.
> 14,5> 9,5> 8,7Ziol M et al
F = 4F ≥ 3F ≥ 2
Seuils d’élasticité
Limites des marqueurs non Limites des marqueurs non invasifsinvasifs
•• FibrotestFibrotest–– Non validé dans l’hépatite B chez les patients Non validé dans l’hépatite B chez les patients
dialysés ou transplantés rénauxdialysés ou transplantés rénaux
•• FibroscanFibroscan–– Non validé chez les patients dialysés ou Non validé chez les patients dialysés ou
transplantés rénaux dans les transplantés rénaux dans les hépatopathies hépatopathies virales virales B ou CB ou C

23
Algorithm in dialysis pt or renal recipientantiHCV+/HCV RNA+
Fibrotest
< 0.2 > 0.2 <0.6 > 0.6Dialysis patient - No candidate to Tx : follow-up biopsy Treatment
- Candidate to Tx : Treatment biopsy biopsy (combined Tx?)Treatment Treatment
Kidney recipientfollow-up biopsy biopsy (surestimation ?)
RibavirinVaraut et al. Transplantation 2005
Antiviraltreatments
Lamivudine (zeffix)Adefovir (hepsera)Entecavir (baraclude)Tenofovir (viread)Tenofovir + emtricitabine (truvada)Other
α -interferonpeg-interferon
Immunomodulatorytreatments
Vaccine therapyPassive transfertof immunity
ImmunostimulationThymosinGM-CSFPolyadenur
Consequences of the impact of allograft on viral hepatitis
To Treat HBV
24
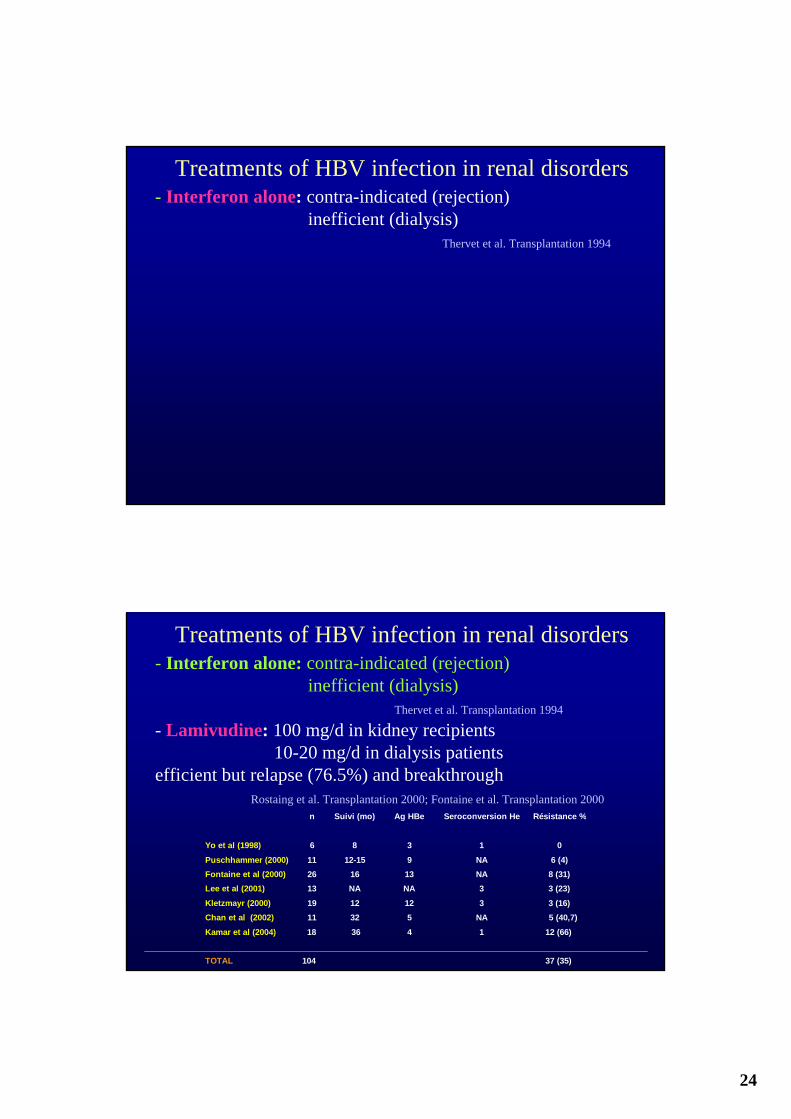
Treatments of HBV infection in renal disorders- Interferon alone: contra-indicated (rejection)
inefficient (dialysis)Thervet et al. Transplantation 1994
Treatments of HBV infection in renal disorders- Interferon alone: contra-indicated (rejection)
inefficient (dialysis)Thervet et al. Transplantation 1994
- Lamivudine: 100 mg/d in kidney recipients10-20 mg/d in dialysis patients
efficient but relapse (76.5%) and breakthroughRostaing et al. Transplantation 2000; Fontaine et al. Transplantation 2000
Yo et al (1998)
Puschhammer (2000) Fontaine et al (2000) Lee et al (2001)
Kletzmayr (2000) Chan et al (2002)
Kamar et al (2004) TOTAL
n
6
11 26 13
19 11
18 104
Suivi (mo)
8
12-15 16 NA
12 32
36
Ag HBe
3
9 13 NA
12 5
4
Seroconversion He
1
NA NA 3
3 NA
1
Résistance %
0
6 (4) 8 (31) 3 (23)
3 (16) 5 (40,7)
12 (66) 37 (35)
25
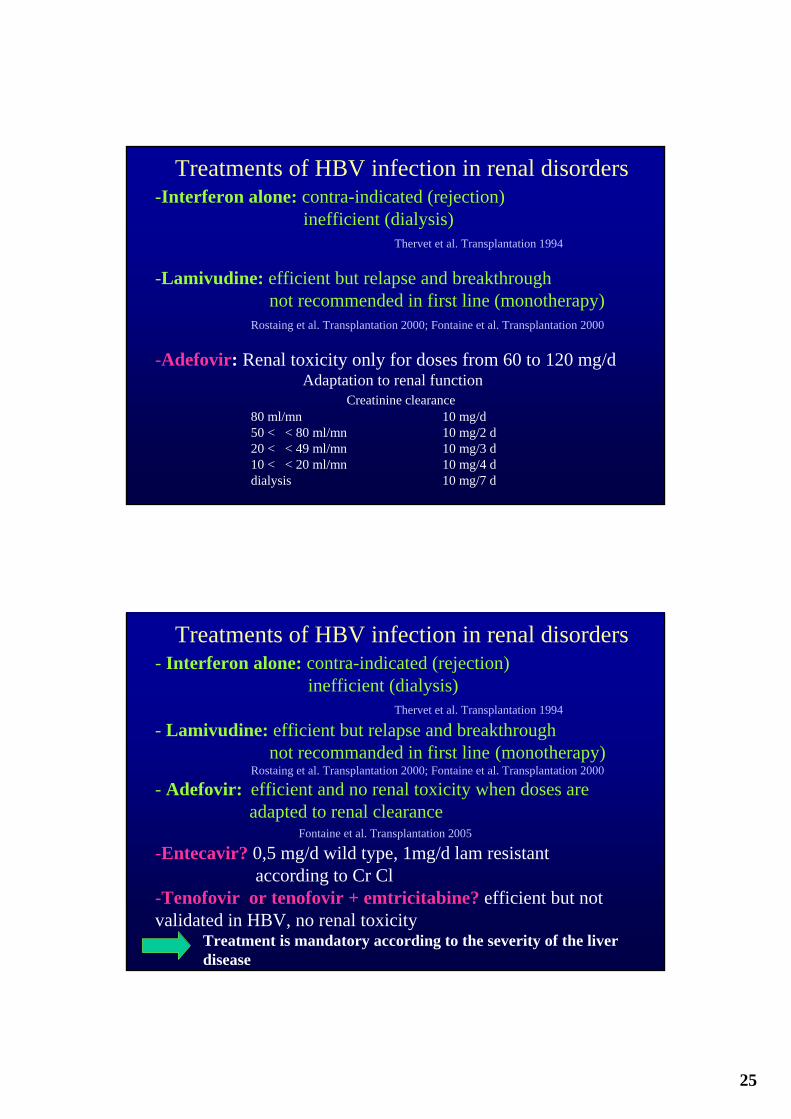
Treatments of HBV infection in renal disorders-Interferon alone: contra-indicated (rejection)
inefficient (dialysis)Thervet et al. Transplantation 1994
-Lamivudine: efficient but relapse and breakthroughnot recommended in first line (monotherapy)
Rostaing et al. Transplantation 2000; Fontaine et al. Transplantation 2000
-Adefovir: Renal toxicity only for doses from 60 to 120 mg/dAdaptation to renal function
Creatinine clearance80 ml/mn 10 mg/d50 < < 80 ml/mn 10 mg/2 d20 < < 49 ml/mn 10 mg/3 d10 < < 20 ml/mn 10 mg/4 ddialysis 10 mg/7 d
Treatments of HBV infection in renal disorders- Interferon alone: contra-indicated (rejection)
inefficient (dialysis)Thervet et al. Transplantation 1994
- Lamivudine: efficient but relapse and breakthroughnot recommanded in first line (monotherapy)
Rostaing et al. Transplantation 2000; Fontaine et al. Transplantation 2000
- Adefovir: efficient and no renal toxicity when doses are adapted to renal clearance
Fontaine et al. Transplantation 2005
-Entecavir? 0,5 mg/d wild type, 1mg/d lam resistantaccording to Cr Cl
-Tenofovir or tenofovir + emtricitabine? efficient but not validated in HBV, no renal toxicity
Treatment is mandatory according to the severity of the liver disease
26
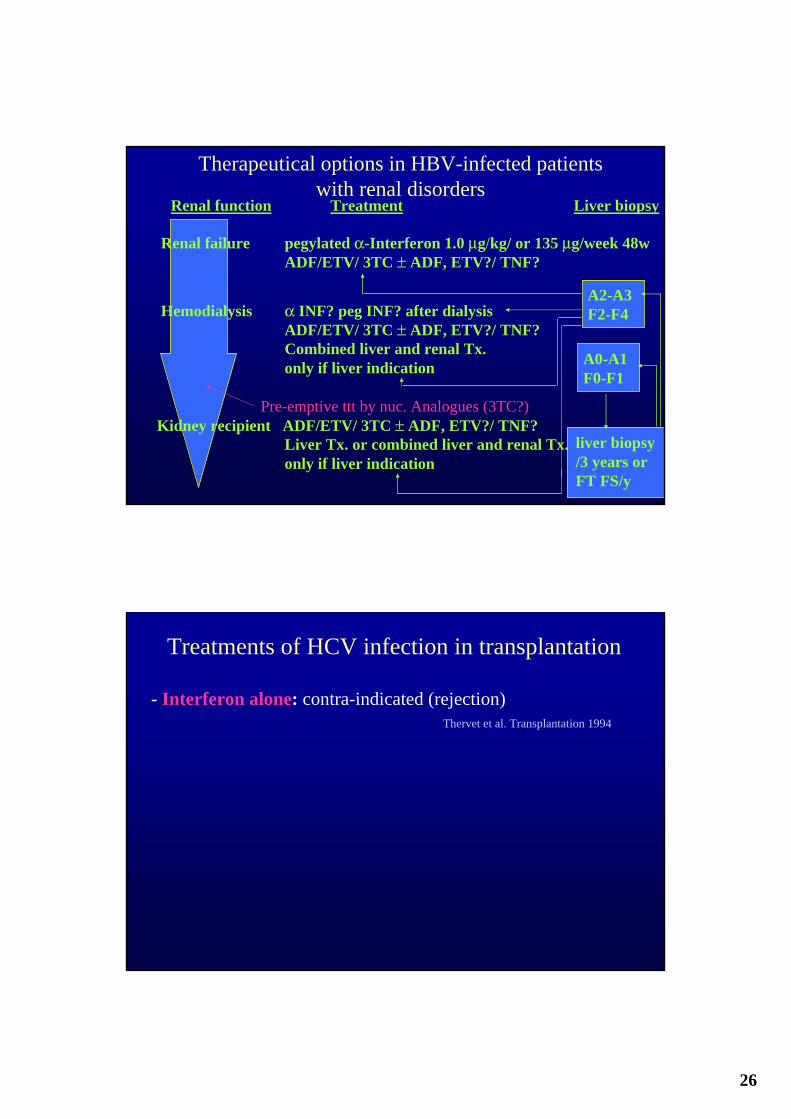
A2-A3F2-F4
A0-A1F0-F1
liver biopsy/3 years orFT FS/y
Renal failure pegylated α-Interferon 1.0 μg/kg/ or 135 μg/week 48wADF/ETV/ 3TC ± ADF, ETV?/ TNF?
Hemodialysis α INF? peg INF? after dialysis ADF/ETV/ 3TC ± ADF, ETV?/ TNF?Combined liver and renal Tx.only if liver indication
Pre-emptive ttt by nuc. Analogues (3TC?)Kidney recipient ADF/ETV/ 3TC ± ADF, ETV?/ TNF?
Liver Tx. or combined liver and renal Tx.only if liver indication
Therapeutical options in HBV-infected patients with renal disorders
Renal function Treatment Liver biopsy
Treatments of HCV infection in transplantation
- Interferon alone: contra-indicated (rejection)Thervet et al. Transplantation 1994

27
Interferon-α in HCV-infected kidney recipientsInterferon-α 3 MU 3X/week 6 to 12 months
Thervet et al. Rostaing et al.
• 2 studies Transplantation 1994 Transplantation 1995n = 13 n = 16
% discontinuation 54 25% biochemical response 8 77% virological efficacy 8 25% virological LTR 0 0
% allograft rejection 15 29% drug-related 7 -
tubulonephritis
• Overall results (n=42 kidney recipients)48% ARF (65% dialysis) 6% LTR
Treatments of HCV infection in transplantation
- Interferon alone: contra-indicated (rejection)
- Ribavirin alone: inefficient ?
Biochemical but not virological efficacyGarnier et al. Transplant Proc 1997
Renal benefit without pathological benefitKamar et al. Transplantation 2003
Histo-pathological benefit in 71%Fontaine et al. Transplantation 2004
28
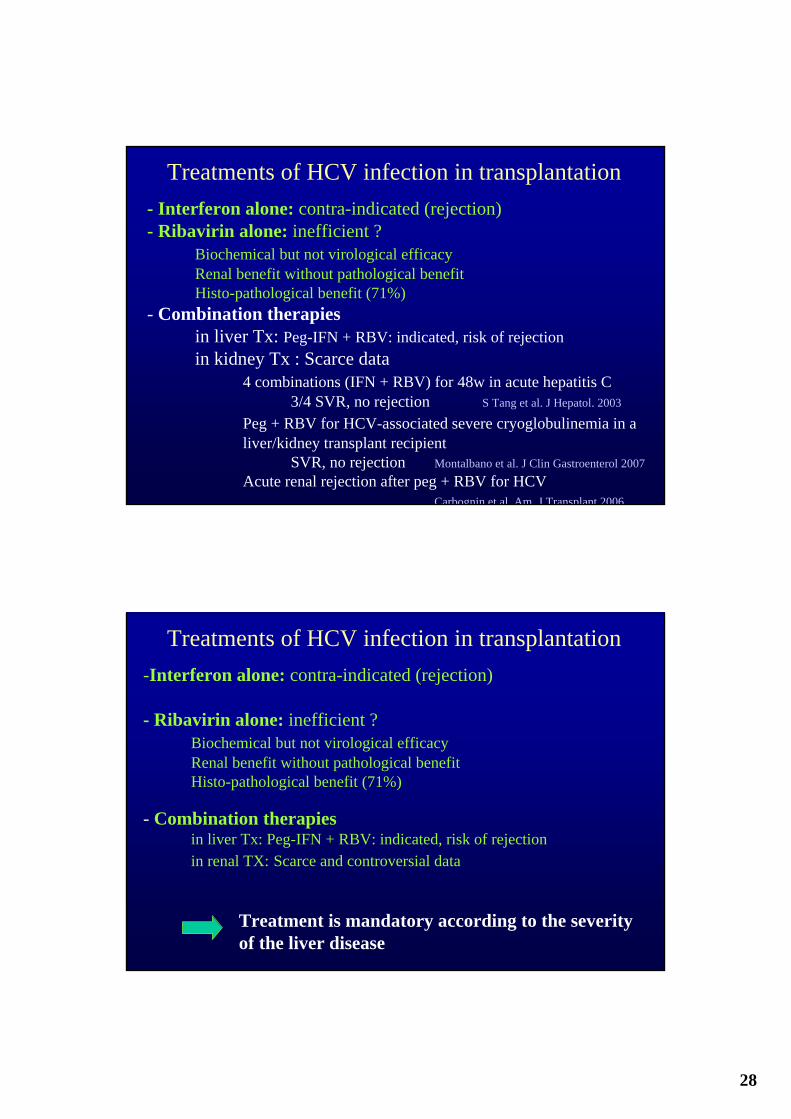
Treatments of HCV infection in transplantation- Interferon alone: contra-indicated (rejection)- Ribavirin alone: inefficient ?
Biochemical but not virological efficacyRenal benefit without pathological benefitHisto-pathological benefit (71%)
- Combination therapiesin liver Tx: Peg-IFN + RBV: indicated, risk of rejectionin kidney Tx : Scarce data
4 combinations (IFN + RBV) for 48w in acute hepatitis C 3/4 SVR, no rejection S Tang et al. J Hepatol. 2003
Peg + RBV for HCV-associated severe cryoglobulinemia in a liver/kidney transplant recipient
SVR, no rejection Montalbano et al. J Clin Gastroenterol 2007Acute renal rejection after peg + RBV for HCV
Carbognin et al. Am J Transplant 2006
Treatments of HCV infection in transplantation-Interferon alone: contra-indicated (rejection)
- Ribavirin alone: inefficient ?Biochemical but not virological efficacyRenal benefit without pathological benefitHisto-pathological benefit (71%)
- Combination therapiesin liver Tx: Peg-IFN + RBV: indicated, risk of rejectionin renal TX: Scarce and controversial data
Treatment is mandatory according to the severityof the liver disease

29
A2-A3F2-F4
A0-A1F0-F1
LB/3 yearsFT FS/ year
Renal failure pegylated α-Interferon (+ RIBA if creat < 200 μmol)1.-1.5 μg α-2b /kg or 180 μg α-2a weekly 6-12 months
Hemodialysis α-Interferon 3 MU after dialysis (Peg 135/week + riba 3/week) ?
12 months (if PCR- at M3)Combined liver and renal Tx.(F4)
Kidney recipients Ribavirin ?Liver Tx. (F4) orcombined liver and renal Tx.(F4)
Therapeutical options in HCV-infected patients with renal disorders
Renal function Treatment Liver biopsy
Viral hepatitis and renal failureConclusions
• HBV/HCV hepatitis may be associated with a risk of severe disease (immunosuppression)liver-related overmortalitydecreased patients and grafts survival
• Thus requiring:- prevention (vaccination, universal precautions, non-infected
graft in non life-threatening Tx)- pathological (or biochemical) evaluation- antiviral (mono-)therapies