immuno - lec 20
TRANSCRIPT
7/31/2019 Immuno - Lec 20
http://slidepdf.com/reader/full/immuno-lec-20 1/13
1
Inflammation
Dua'a Herzallah
Ziad Al-Nasser
Sunday, 31/7/2011
25
20
7/31/2019 Immuno - Lec 20
http://slidepdf.com/reader/full/immuno-lec-20 2/13
Immunology- Lecture #20
.. : " ...
".. ..
...
Peace up colleagues Ramadan Karim! I tried to make this lecture as easy as I could!
Study it thoroughly, & remember that nothing we learn in this world is ever wasted.
A very BEAUTIFUL saying of the prophet (PBUH) to start with:
"Acquire knowledge. It enables its possessor to distinguish right from wrong; it
lights the way to heaven; it is our friend in the desert, our society in solitude, our
companion when friendless".
The professor completed chapter 21, finished chapter 22, and started with 23, so
let’s get going:
We will continue with the innate immune system, we talked about macrophages and
natural killer cells, and how do they play a role in defense.
Natural killer cells use the same mechanisms of the cytotoxic T cells, they have
small granules in their cytoplasm contain proteins such as perforin and proteases known
as granzymes, but NK cells are non-specific. The role of NK cells start when there is
suppression or there is no presence of the MHC antigens. NK cells have two receptors
that sense the presence/absence of the MHC antigens, so the one the we call KIR
(Killer-cell immunoglobulin-like receptors) and the CD94 (or NKG2), if the MHC
antigen is present it will give a negative signal and won’t be activated and vice versa.
The activation of the NK cells is through a mechanism called Antibody-dependent
cellular cytotoxicity (ADCC). NK cells express the Fc receptor (FcR) molecule whichis an activating biochemical receptor that binds the Fc portion of antibodies. When
antigen binds to an antibody, this antibody will bind to the NK cell through its receptor,
if this happens and MHC was there, then the NK cell will be activated, pores will
develop in the cytoplasmic membrane, granzymes will enter inside and induce the
process of apoptosis.
We talked about Apoptosis and its importance in many aspects in the body.
We also said that in our body we have anti-apoptotic pathways in order to keepthese cells alive for a longer period of time like the BCL-2 gene, that interferes with the
7/31/2019 Immuno - Lec 20
http://slidepdf.com/reader/full/immuno-lec-20 3/13
Immunology- Lecture #20
function of the cascades enzymes and no destruction to the DNA is going to take place.
And sometimes we need these cells to stay in our body for a longer period of time, like
memory cells for example. You should know what triggers the activation of BCL-2
mechanisms; one of them is the production of IL-2 which is very important in cell
development. It has to be produced for a while then it has to stop otherwise the reactionwill keep going on for a longer period of time.
Binding of IL-2 to its receptor is going to activate the cell to express more of the BCL-2
to keep the cell alive for a longer period of time. Any problem related to the expression
of BCL-2 anti apoptotic pathways keep the lymphocytes proliferating abnormally
which will lead to lymphoma.
Do you know that BCL-2 has been implicated in many cancers and diseases
such as schizophrenia, as wiki says: Apoptosis plays a very important role in
regulating a variety of diseases that have enormous social impacts. For
example, schizophrenia is a neurodegenerative disease that may result from an
abnormal ratio of pro- and anti-apoptotic factors. There is some evidence that
this defective apoptosis may result from abnormal expression of Bcl-2 and
increased expression of caspase-3.
We talked about parasites; they have to be destroyed by mast cells in an acute type of
inflammation. Some parasites like schistosoma are so evasive that they cover
themselves with body antigens, red blood cells, & MHC antigens so the body will
recognize them as self so they stay in the body without even noticing them. Theproblem comes when the female of the schistosomal couple lays down so many eggs,
so these eggs will be washed back to the liver through the venous blood where a
chronic inflammatory process takes place.
So in parasitic infections, you could end up with a chronic inflammation that is going to
induce lots of interferon gamma & TNF that will lead to liver damage and failure.
Sometimes these eggs lodge in the urinary bladder or in the bowl and while trying to
get out into the lumen they get trapped there and induce severe inflammatory type of
reaction. So eosinophils play a major role in that and we talked about the molecules
that we have inside, the cationic proteins, peroxidases, and beside all of the vasoactive
amines. They play a major role in that. I want you to remember that sometimes the
killing process and the presence of hyperesoniphelia could induce a chronic
inflammation and we could die as a sequel of that chronic inflammation.
Finally he finished, and I am sure this is the 15th
time he repeats what he said on the
same subject, so study it from the previous lectures.
7/31/2019 Immuno - Lec 20
http://slidepdf.com/reader/full/immuno-lec-20 4/13
Immunology- Lecture #20
Chapter 22:
So this will bring us into the process of inflammation
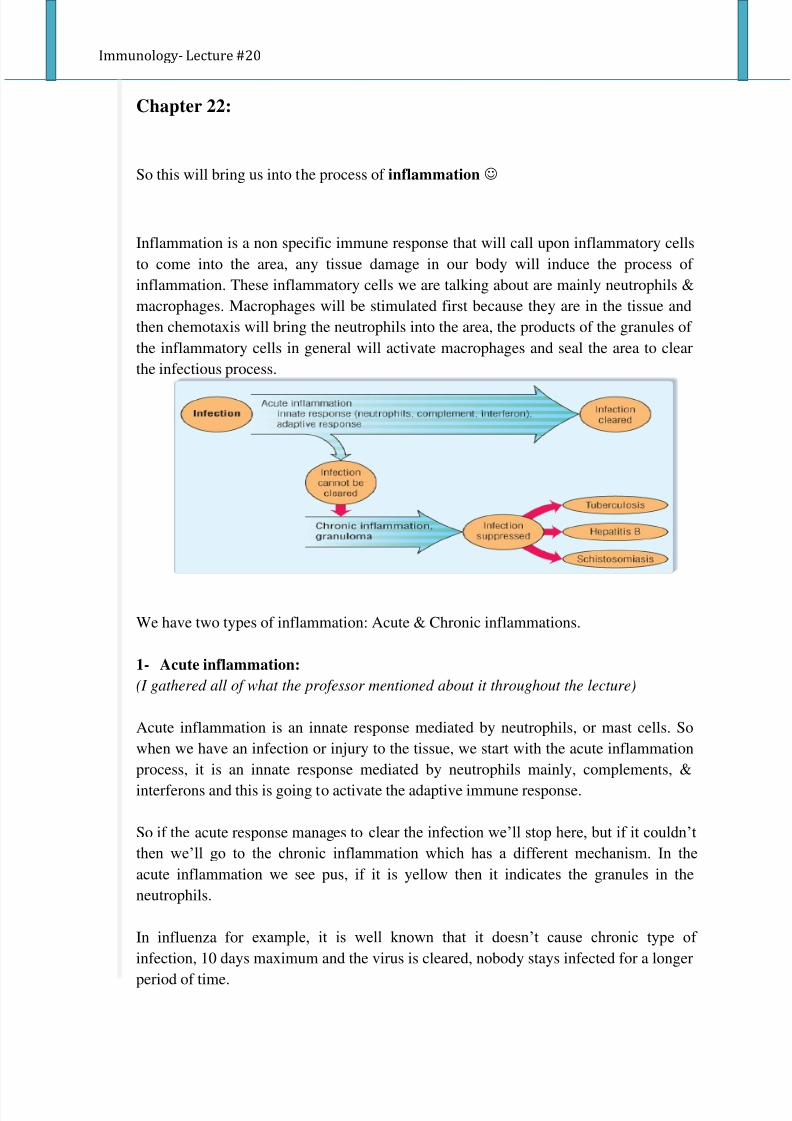
Inflammation is a non specific immune response that will call upon inflammatory cells
to come into the area, any tissue damage in our body will induce the process of
inflammation. These inflammatory cells we are talking about are mainly neutrophils &
macrophages. Macrophages will be stimulated first because they are in the tissue and
then chemotaxis will bring the neutrophils into the area, the products of the granules of
the inflammatory cells in general will activate macrophages and seal the area to clear
the infectious process.
We have two types of inflammation: Acute & Chronic inflammations.
1- Acute inflammation:
(I gathered all of what the professor mentioned about it throughout the lecture)
Acute inflammation is an innate response mediated by neutrophils, or mast cells. So
when we have an infection or injury to the tissue, we start with the acute inflammation
process, it is an innate response mediated by neutrophils mainly, complements, &
interferons and this is going to activate the adaptive immune response.
So if the acute response manages to clear the infection we’ll stop here, but if it couldn’t
then we’ll go to the chronic inflammation which has a different mechanism. In the
acute inflammation we see pus, if it is yellow then it indicates the granules in the
neutrophils.
In influenza for example, it is well known that it doesn’t cause chronic type of
infection, 10 days maximum and the virus is cleared, nobody stays infected for a longer
period of time.
7/31/2019 Immuno - Lec 20
http://slidepdf.com/reader/full/immuno-lec-20 5/13
Immunology- Lecture #20
And when I talk about the process of inflammation I talk about hotness, redness, edema
(because of the vasoactive amines) and tenderness (painful and itchy area).
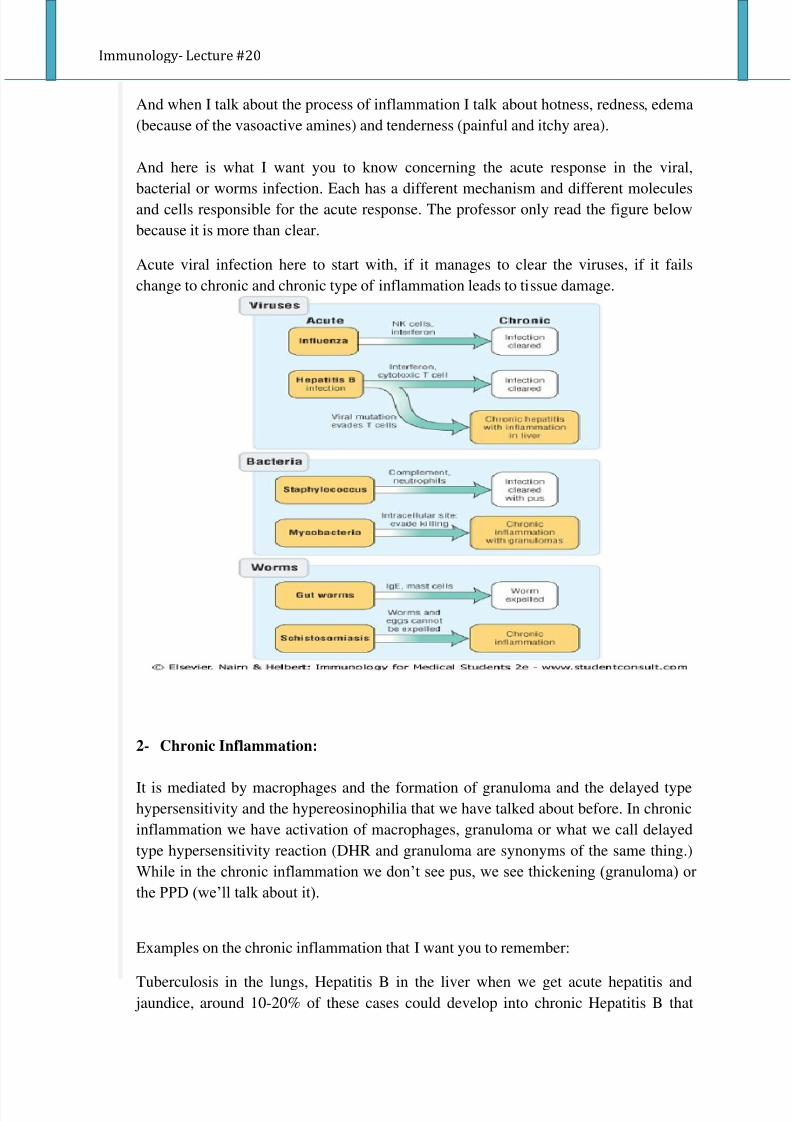
And here is what I want you to know concerning the acute response in the viral,
bacterial or worms infection. Each has a different mechanism and different moleculesand cells responsible for the acute response. The professor only read the figure below
because it is more than clear.
Acute viral infection here to start with, if it manages to clear the viruses, if it fails
change to chronic and chronic type of inflammation leads to tissue damage.
2- Chronic Inflammation:
It is mediated by macrophages and the formation of granuloma and the delayed typehypersensitivity and the hypereosinophilia that we have talked about before. In chronic
inflammation we have activation of macrophages, granuloma or what we call delayed
type hypersensitivity reaction (DHR and granuloma are synonyms of the same thing.)
While in the chronic inflammation we don’t see pus, we see thickening (granuloma) or
the PPD (we’ll talk about it).
Examples on the chronic inflammation that I want you to remember:
Tuberculosis in the lungs, Hepatitis B in the liver when we get acute hepatitis and jaundice, around 10-20% of these cases could develop into chronic Hepatitis B that
7/31/2019 Immuno - Lec 20
http://slidepdf.com/reader/full/immuno-lec-20 6/13
Immunology- Lecture #20
leads to liver damage, and the Schistosomiasis that I have talked about in the
entrapment of eggs in the liver, urinary bladder or the GIT.
The signs and symptoms of the inflammation: hotness redness, edema tenderness,
swelling, pain, white blood cells, & tissue infiltration. Remember that neutrophils are
not present in tissues; they are called upon so the stimulation starts with the
macrophages.
We have the physical stimulation, & the immunological stimulation (TNF which comes
mainly from macrophages and it causes necrosis to tumors in animals but it raises our
body temperature and plays a major role in apoptosis.) If stimuli could not be removed
by the acute process, then it changes into the chronic. And macrophages will take
release here.
So we start with pyogenic (pus forming) infection in the acute, ends up with activated
macrophages and granuloma.
Acute viral infection here to start with, if it manages to clear the viruses, if it fails
change to chronic and chronic type of inflammation leads to tissue damage.
Edema comes from mast cells and we talked about that and the diapedesis of the plasma
into the area and the eosinophils and how can they damage the parasite and the
vasoactive amines in these eosinophils also induce tissue damage. I want you to
remember that the ultimate goal of these inflammatory cells is to get rid of the invading
microorganisms but sometimes if they fail, if you have immunocomplexes and thesecomplexes are adherent to the basement membrane of the kidneys, so the macrophage
will come and try to phagocytose the immunecomplexes but they can’t because they are
so stuck to the B.M of the kidney, so they release their vasoactive amines mediators to
the basement membrane and this causes damage to the kidney. so this is an outcome, it
was not designed to damage our tissues but the process lead to that.
In chronic bronchitis in smokers, why do they cough? Because macrophages come to
the area trying to clear the carbon molecules in the respiratory tract, and they fail!! So
they release their hydrolytic enzymes and cause damage to the mucosal lining of the
respiratory tract because of the stimulation of mucous secreting glands and so on.
So remember the term Delayed-type hypersensitivity reaction, here we are talking
about TH1 cells and macrophages. And we know that we have (DTH) by performing
skin tests, like the PPD skin testing & lepromin testing.
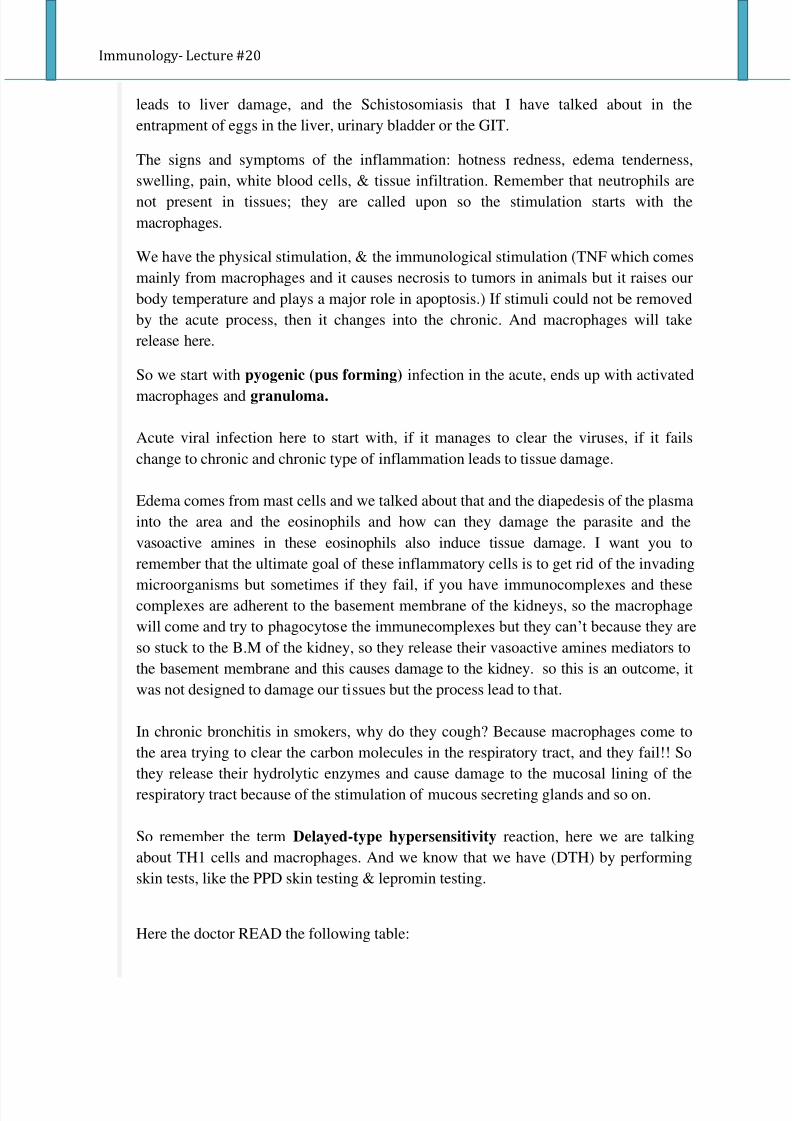
Here the doctor READ the following table:
7/31/2019 Immuno - Lec 20
http://slidepdf.com/reader/full/immuno-lec-20 7/13
Immunology- Lecture #20
So when we talk about inflammation, we are talking about a network of cytokines that
induces all of these changes that occur in our body. In acute inflammation we have a
cytokine network, it is supposed to clear the infection and if it fails it changes into a
chronic inflammation. So the cytokines that are involved:
IL-1, and IL-1 is present within macrophages and many other cells as well, suchas ) and it is needed to activate the macrophages & T helper cells.
TNF (tumor necrosis factor), remember it is involved in fat metabolism, fever &
apoptosis.
GM-CSF, which recruit more neutrophils and monocytes into the area of
infection.
IL-12 to which will stimulate the differentiation of T helper into TH1.
IL-18, it is almost the same as that of IL-12.
Remember that NK cells produce Interferon gamma ( it is secreted by Th1 cells, Tccells and NK cells) which is important in MHC Ag expression, Ag processing,
Macrophage activation, NK cell activity, TH2 suppression, and has an antiviral effect.
IFN-γ is the primary cytokine which defines Th1 cells: Th1 cells secrete IFNg, which in
turn causes more undifferentiated CD4 cells (Th0 cells) to differentiate into Th1 cells,
representing a positive feedback loop - while suppressing Th2 cell differentiation.
Always we have a balance, when TH1 is activated then TH2 is suppressed and vice
versa.
So, here we talk about cytokines network, here macrophages will be activated first,
production of IL-12 which will stimulate the differentiation of T helper into TH1, here
7/31/2019 Immuno - Lec 20
http://slidepdf.com/reader/full/immuno-lec-20 8/13
Immunology- Lecture #20
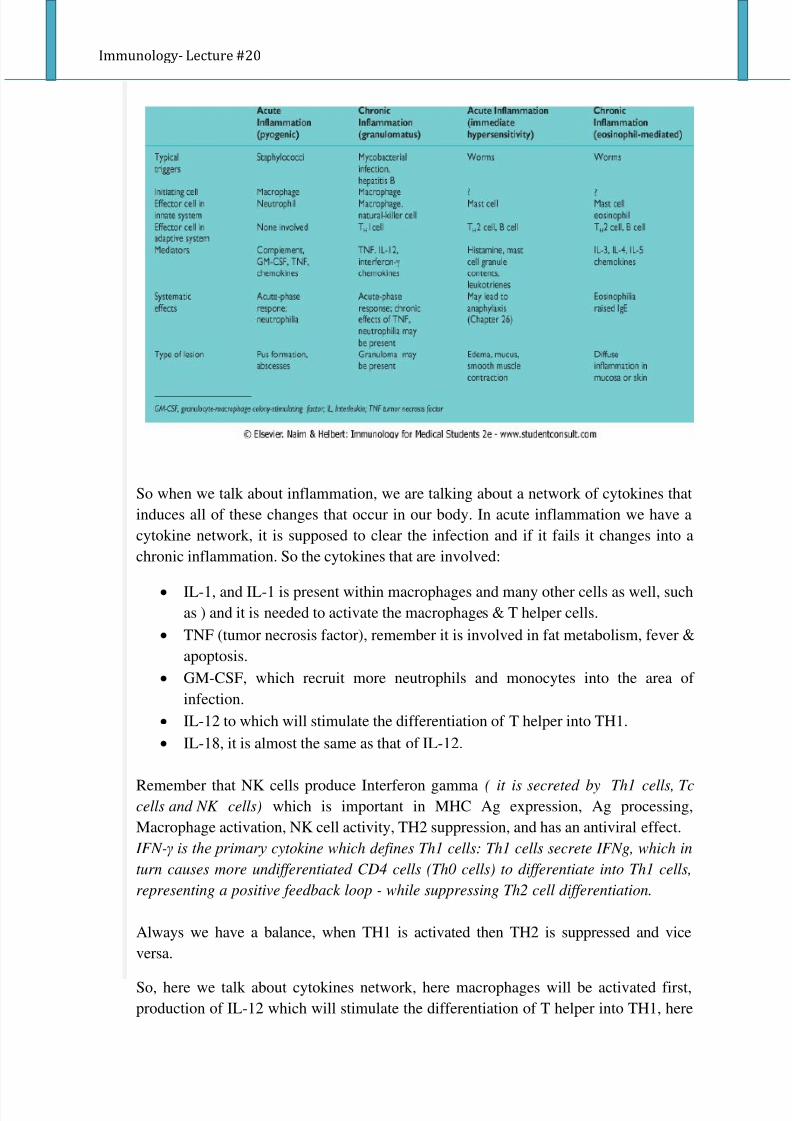
in this case for example interferon gamma and how interferon gamma will act on the
NK cells and NK cells can produce interferon gamma which will act on cytotoxic T
cells which to perform the killing and the activation of macrophages and formation of
granuloma.( please refer to the figure below to understand the idea more thoroughly).
Tuberculosis is a classical example of chronic inflammation and the development of granuloma (what we call delayed - type hypersensitivity reaction), we are talking about
lymphocytes of TH1 and activated macrophages. Tuberculosis is a reemerging
infectious disease, nowadays because of using immunosuppressive drugs, radiotherapy
& cytotoxic drugs; we can see the M. tuberculosis is on the return again, so we have to
be aware that patients might be getting this infection. Simply, here what we are getting
in this chronic inflammation is activated macrophages and this will occur through the
toll-like receptors like TLR-2 & TLR-4 for example, and the warning signals that will
come out of the macrophages, IL-1, IL- 12, IL-6, IL-8 & TNF all of these come from
macrophages.
In M. tuberculosis, the bacteria structurally have mycolic acid, waxes and so on that
they can stay in our body in a longer period of time and stimulate the delayed-type
hypersensitivity response, so it changes into a chronic inflammation with granuloma
and activated macrophages, epitheliod & giant cells that will kill the mycobacterium
tuberculosis.
We call the infection when we are firstly infected the primary infection, and usually it
occurs in the lungs so alveolar macrophages are going to phagocytose those bacteria
and they resist killing here.
7/31/2019 Immuno - Lec 20
http://slidepdf.com/reader/full/immuno-lec-20 9/13
Immunology- Lecture #20
If we are already vaccinated with the BCG vaccine or exposed to antigens of M.
tuberculosis then things will be different, we will have more of the activated
macrophages that will clear the site of infection. So when the macrophages are
activated through the cytokines network that we have mentioned, macrophages will
come into the area, activated macrophages will change into epitheliod cells and multi-nucleated giant cells. TNF will be produced, necrosis in the center of the lesion will be
found and it is a cheesy necrosis we call it casiation necrosis.
Tuberculosis outcomes:
1- If the granuloma was near a bronchus for example,and we had excessive production
of TNF, then it will open into the air and the microbes would have access into the
environment, we call this open TB.
2- The bacteria could be taken with these macrophages through the circulation into
anywhere of the body, we call this military TB or tuberculosis meningitis if it
reached the CNS. Widespread primary TB occurs in a small proportion of young
patients, with dissemination all over the body.
And wherever bacteria go to the body, to the brain, kidney or bone, granuloma will be
formed and this will damage the tissue that granuloma is landing on!
In most patients, the primary infection heals to leave a small scar visible on radiograph.Mycobacteria remain alive inside the phagocyte.
Mild immune deficiency leads to reactivation, as we said in losing a spouse for
example usually in the upper parts of the lung.
Severe immune deficiency leads to more widespread infection which is likely to
spread beyond the lungs.
Remember in M.tuberculosis it is TH1 activity, it means INF gamma in particular is
going to be produced here. Milliary tuberculosis (dissemination) and reactivation if the
bacteria present in the macrophages could not be killed and they stayed in our body.
We call that latency it is “delayed” somehow, and if our immune defenses for one
reason or another dropped like for example we get exposed to chronic stress, and here
we talk about the old man who lost his wife or the old wife who lost her husband
“losing a spouse” we call that then Mineralocorticoids will be released and so our
immunity will be suppressed so we get what we call reactivation of a primary TB or
latent TB and so the disease will start to be open and damage will take place in the area
where those were located in the beginning.
7/31/2019 Immuno - Lec 20
http://slidepdf.com/reader/full/immuno-lec-20 10/13
Immunology- Lecture #20
So here when we talk about M.tuberculosis we are talking about pulmonary
tuberculosis mainly. And those micros they can be hanged in the air as I said for a
longer period of time that’s why we have to have what we call respiratory isolation,
we should be using masks all the time because we could be inhaling those organisms
that could go to the into the alveoli and induce the chronic granuloma, and usually wesee those in the upper part of the lungs, where oxygen concentration is high.
When we are exposed to those, a granuloma develops (activation of macrophages), then
we can test for those in a test we call it the PPD – the Purified Protein Derivative. This
is one example to see if we are sensitized or not, and if you remember in the
microbiology course we talked about what does it mean to have a positive PPD testing,
how we do the PPD testing, we inject the PPD protein, the Purified Protein Derivative
intradermally, why interdermally? Because we do have Langerhans cells
(macrophages) there, we want them to be activated and then we just draw a circle &
write the date and time and we read that from 48 to 72 hours- two to three days- till thechronic inflammation develops and the granuloma. so you will see a thickening and
then you will measure the diameter of the thickening, if it is 10 or more, it is positive, if
it is 5 or less then it is negative, and between 5 and 10 it is intermediate, and nowadays
any thickening they consider it positive but you have to take it in consideration with the
case of the patient, if the patient is on steroids, weather you are vaccinated or not,
infected in the past or not.
And at the same time you can measure even the level of cytokines; IL-1 and IFN
gamma which is produced when TH1 cells are activated. If the level of IFN gamma is
so high, this is an indication that you have granuloma and a chronic inflammation. So
remember M.tuberculosis and the destructive effect to the tissues is because of the
granuloma rather than the direct effect of the organism itself .
Remember what a granuloma is, macrophages in the centre with the bacteria
engulfed and TH1 cells producing cytokines INF gamma to activate the
macrophages to kill the mycobacteria.
So this is the whole process how the granuloma develops when we get infected with
M.tuberculosis, the bacteria is going to bind to toll-like receptor on macrophages and
then the cytokines are produced and we can follow that up in 12-24 hours and how theycall upon the macrophages to come into the area, TH1 cells produce cytokines (INF
gamma), IL-6, IL-8 and the granuloma is formed.
So this is the test I was telling you about here to check for the presence of INF gamma,
here mycobacterium peptides are added to a blood sample, so if you have the
macrophages, then you will be seeing lots of INFs that are produced in a patient
exposed to M.tuberculosis. In a patient who has never been exposed, there are no
suffiecient numbers of TH1 cells to produce INF gamma, so measurement of INF is an
indication of TH1, exposure to antigens of M.tuberculosis.
7/31/2019 Immuno - Lec 20
http://slidepdf.com/reader/full/immuno-lec-20 11/13
Immunology- Lecture #20
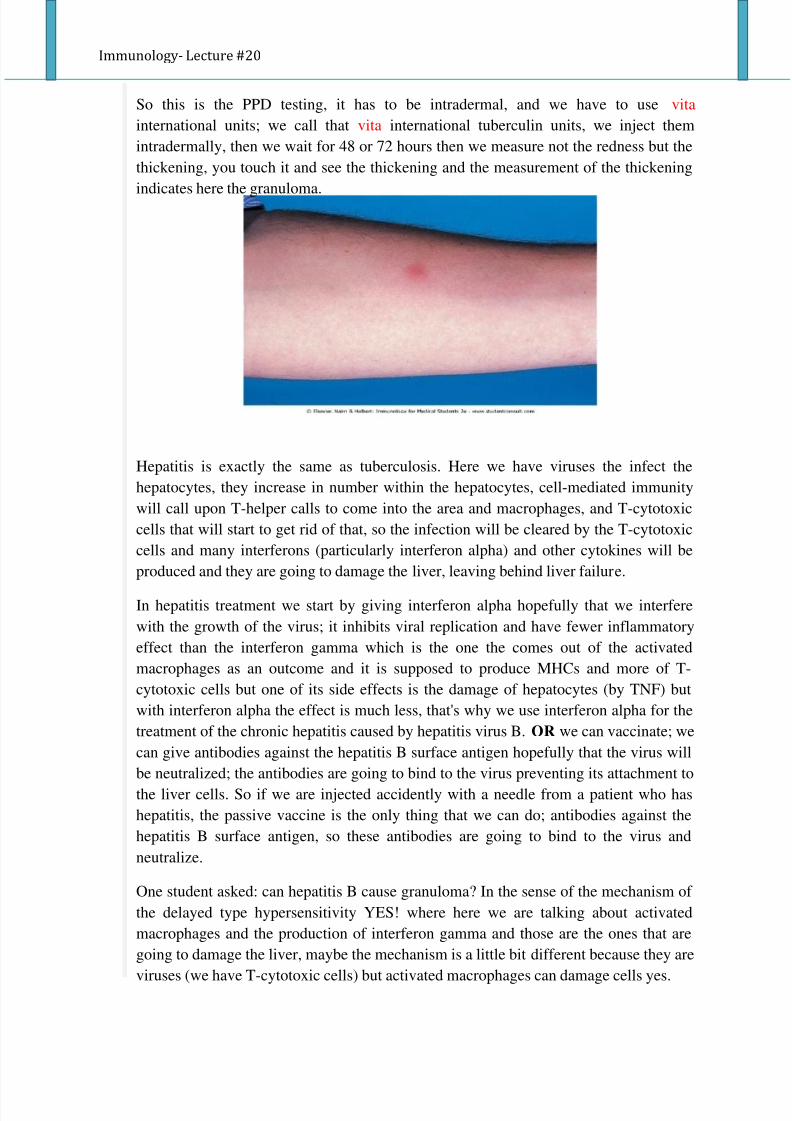
So this is the PPD testing, it has to be intradermal, and we have to use vita
international units; we call that vita international tuberculin units, we inject them
intradermally, then we wait for 48 or 72 hours then we measure not the redness but the
thickening, you touch it and see the thickening and the measurement of the thickening
indicates here the granuloma.
Hepatitis is exactly the same as tuberculosis. Here we have viruses the infect the
hepatocytes, they increase in number within the hepatocytes, cell-mediated immunity
will call upon T-helper calls to come into the area and macrophages, and T-cytotoxic
cells that will start to get rid of that, so the infection will be cleared by the T-cytotoxic
cells and many interferons (particularly interferon alpha) and other cytokines will be
produced and they are going to damage the liver, leaving behind liver failure.
In hepatitis treatment we start by giving interferon alpha hopefully that we interfere
with the growth of the virus; it inhibits viral replication and have fewer inflammatory
effect than the interferon gamma which is the one the comes out of the activated
macrophages as an outcome and it is supposed to produce MHCs and more of T-
cytotoxic cells but one of its side effects is the damage of hepatocytes (by TNF) but
with interferon alpha the effect is much less, that's why we use interferon alpha for the
treatment of the chronic hepatitis caused by hepatitis virus B. OR we can vaccinate; we
can give antibodies against the hepatitis B surface antigen hopefully that the virus will
be neutralized; the antibodies are going to bind to the virus preventing its attachment to
the liver cells. So if we are injected accidently with a needle from a patient who has
hepatitis, the passive vaccine is the only thing that we can do; antibodies against the
hepatitis B surface antigen, so these antibodies are going to bind to the virus and
neutralize.
One student asked: can hepatitis B cause granuloma? In the sense of the mechanism of
the delayed type hypersensitivity YES! where here we are talking about activated
macrophages and the production of interferon gamma and those are the ones that are
going to damage the liver, maybe the mechanism is a little bit different because they are
viruses (we have T-cytotoxic cells) but activated macrophages can damage cells yes.
7/31/2019 Immuno - Lec 20
http://slidepdf.com/reader/full/immuno-lec-20 12/13
Immunology- Lecture #20
Chapter 23
Cytokines in the immune system
So now the integrated from that we have an innate immune response and we have an
adaptive immune response. The innate the one that is fast, do not have memory, notspecific, complement can be activated, phagocytosis and so on, and gives warning
signals to the adaptive immune system that we have been attacked. So we have a
relationship between the innate and the adaptive and there must be some
communication pattern between them which occurs by molecules and these molecules
are cytokines.
If cytokines are produced from lymphoid cells we call them lymphokines, if they are
produced from WBCs we call them interleukins, we have interferons which interfere
with viral replication, we have Tumor Necrosis Factor which causes, as its name
implies, apoptosis of the virally infected cells and tumor cells, but the overall name forthese are cytokines.
Cytokines are mediators, cells communicate through those between the innate and the
adaptive immune system. Macrophages in the innate, for example, when they get
stimulated by the toll-like receptors they produce these cytokines that will act on the
adaptive, so the adaptive can be stimulated warning the we have been attacked, so the
signaling that takes place on the innate and the adaptive cells because of the cytokines.
So cytokines are the molecules that do the communication between the cells; in the
adaptive and the innate.
Cytokines are proteins, usually they are produced when the cells are stimulated, and
they act upon receptors; when the molecule binds to its receptor the cell will be
activated and produce the act. Some of these receptors are not there, but the minute
these cytokines are produced they activate the production of the receptors. Those
cytokines could act on the same cell that has produced it, we call that autocrine
reaction or on the neighboring cells and we call that paracrine reaction.
Chemokines are cytokines involved with chemotaxis. Chemokine receptors are
receptor on cells where the cytokines which are involved in chemotaxis act upon.
Cytokines can be activators or suppressors. Activators: cause up-regulation like IL-2,
IL-4. Suppressors: cause down-regulation like IL-10, TGF-beta, with temporary
receptors to perform the suppression then these receptors disappear; we don't want the
effect continuously.
We have the interferons (alpha, beta and gamma) which are also cytokines. Interferons
alpha and beta are involved in controlling viral infections and gamma in the activation
of macrophages, expression of MHCs.
TNF: in fever and causes damage to cells and apoptosis as well.
7/31/2019 Immuno - Lec 20
http://slidepdf.com/reader/full/immuno-lec-20 13/13
Immunology- Lecture #20
Cytokines are not just produced by inflammatory cells, they could be produced from
non-inflammatory cells, so when a cell is damaged those could be produced as a sequel
to that.
Very important point to remember is that cytokines are secreted at low levels when
needed and the low levels usually like a maintenance dose for those cells for the
interaction. The minute we see them produced at high levels, that means that we have
an extraordinary interaction is taking place.
Redundancy: it means that we have cytokines that share the same function like TNF
and interferons. One form of the clinical significance of knowing that the cytokines are
redundant is that in many autoimmune diseases I need to block the production of TNF.
If I use monoclonal antibodies against TNF, I'm supposed to clear the problem because
in autoimmune diseases this is where we are going to have chronic inflammation where
it's not needed, but you'll see when we block the TNF, things will improve but it will
not be cleared completely because we have other cytokines that perform the same
function like IL-1. So till now things are not perfect as we want it to be.
Pleotropism: it means that one cytokine can act on many cells.
Finally the professor decided to stop
Dear colleagues, find a way to live your life, that it doesn’t make a mockery of YOUR
values, it’s better to be hated for what you are than to be loved for what you are not!
And remember to carry your personality with you wherever you go! " ... "
Dua’a Herzallah ™
(You can skip this part if you want :P):
Dima BaniEssa, Dima Dima Dima <3 I can’t thank you enough my dear sister <3, youare absolutely one of your kind Thank you for everything!
& to my everyday partner and soul sister, Samah Abu Omar (SEAomar), I dedicate
this special dabsheh for you: <3<3
W a5eeran wa laysa a5eran, my dear little cute loquacious Mais Z3ieter ;)) thank you
for helping me and tolerating the agony of summarizing with me, lots of love!
Best of luck to you all my lovely friends <3Thanks folks!