i tumori desmoidi: attualità terapeutiche · i tumori desmoidi: attualità terapeutiche verona, 23...
TRANSCRIPT
I tumori desmoidi: attualità terapeutiche
Verona, 23-24 Novembre 2010Verona, 23-24 Novembre 2010
Dott.ssa S. Stasolla, Dott.ssa D. Bocale, Dott.ssa M. T. Rotelli, Dott. A. Cavallini, Prof. D. Altomare
Sez. Chirurgia Generale e Trapianti di Fegato
D.E.T.O
Dir: Prof. Vincenzo Memeo
Università degli Studi di Bari
Desmoid tumor, also known as aggressive fibromatosi s, is a rare
disease
Desmoid tumors
Greek “Desmos” : aponeurosis, tendon
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
• Rare clonal proliferation of fibroblasts with an
abundant collagen matrix that may arise in deep soft
tissue
• DT are locally aggressive and characterized by
Desmoid tumors
infiltrative or expansive growth and high risk of local
recurrence
• They do not, however, have the capacity to
metastatize. Hence, desmoid tumors are considered
benign and not malignant
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
Desmoid tumors
• Desmoid tumors may occur sporadically, or in
association with familial adenomatous polyposis (FAP)
(Gardner’s syndrome)
• Desmoid tumors are the 2 nd leading cause of disease-
related mortality in patients with FAP (Clark et al. Br J Surg
1999)
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
Aetiology of Desmoids
� Gene mutation (APC and beta catenin)Lazar AJF et al. Specific mutations in the b-catenin gene (CTNNB1) correlate with local
recurrence in sporadic desmoid tumors. Am J Pathol.2008; 173:1518-27
� Hormonal effects
� Trauma
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
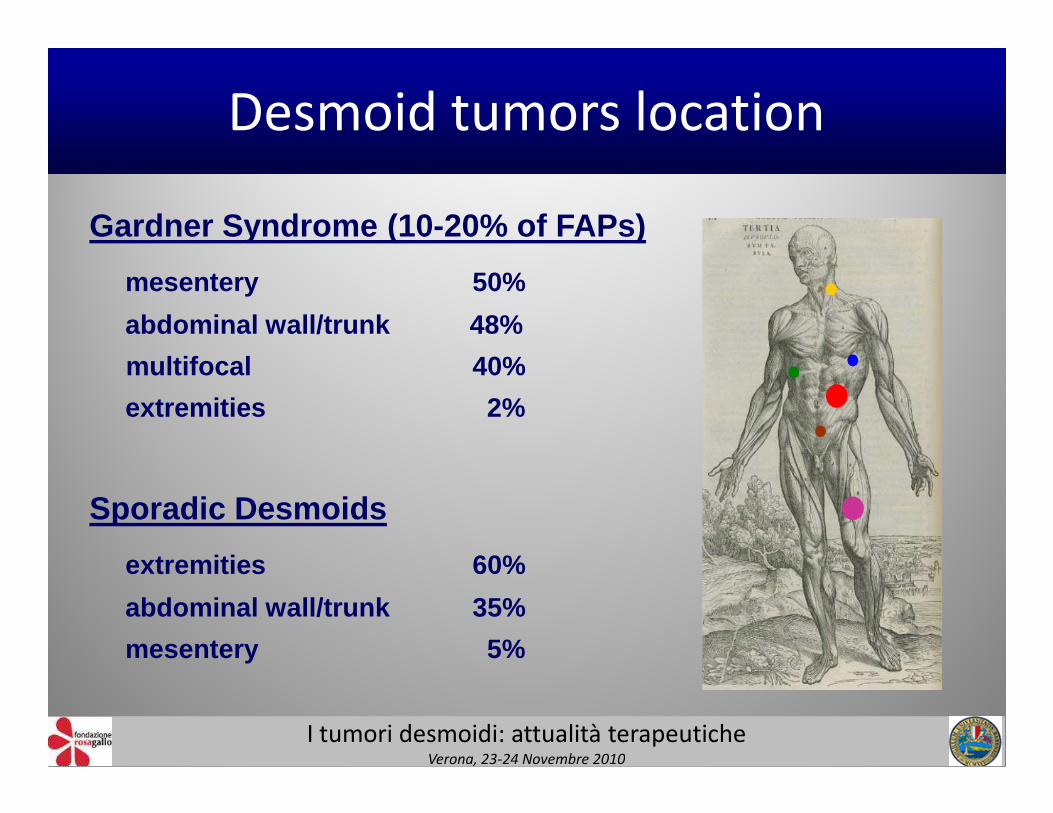
Desmoid tumors location
Gardner Syndrome (10-20% of FAPs)
mesentery 50%
abdominal wall/trunk 48%
multifocal 40%
extremities 2%extremities 2%
Sporadic Desmoids
extremities 60%
abdominal wall/trunk 35%
mesentery 5%
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
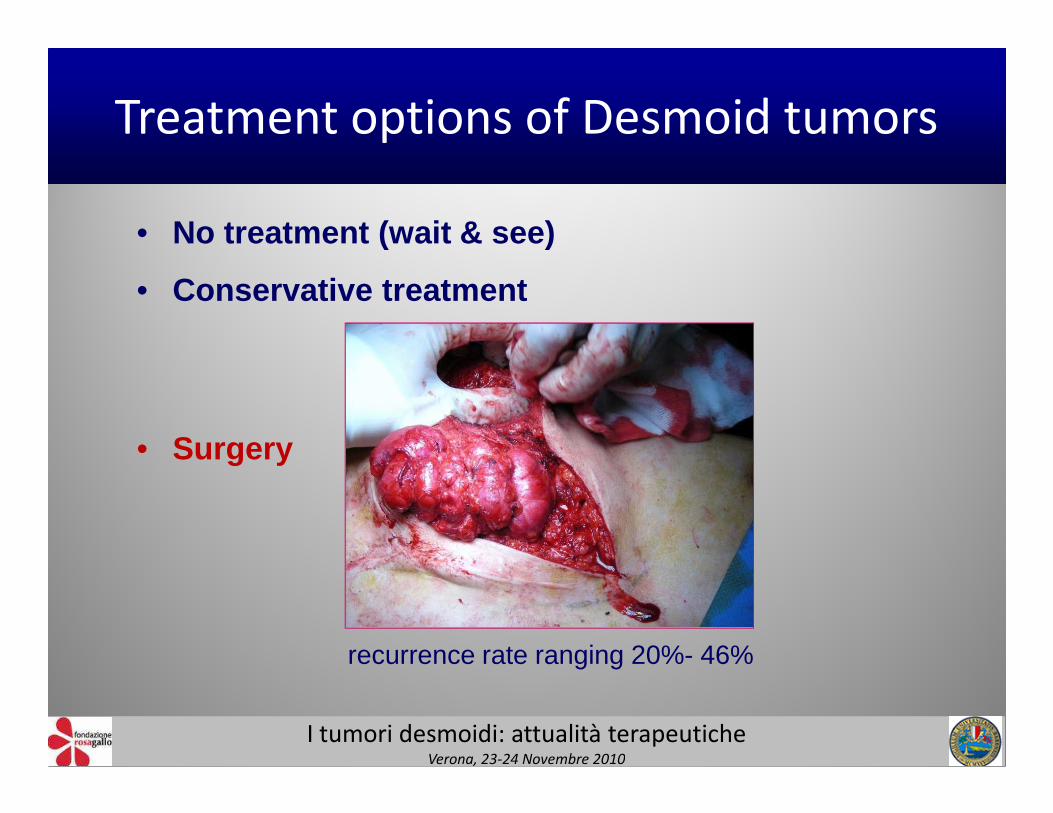
Treatment options of Desmoid tumors
• No treatment (wait & see)
• Conservative treatment
• Surgery
recurrence rate ranging 20%- 46%
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
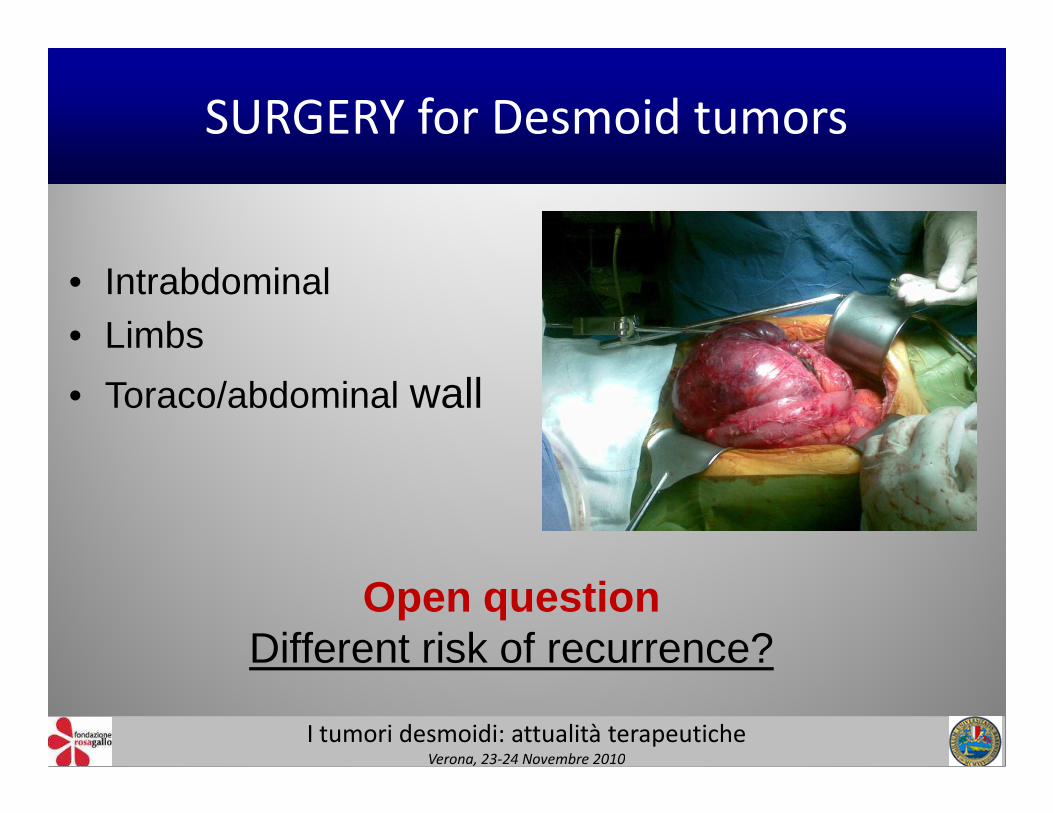
SURGERY for Desmoid tumors
• Intrabdominal • Limbs
• Toraco/abdominal wall• Toraco/abdominal wall
Open questionDifferent risk of recurrence?
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
• Resection margins ?• Infiltrative vs capsulated desmoids ?• Re-recurrence ?
Risk factors for Desmoid recurrence
• Re-recurrence ?• Gender ?• Association with FAP ?• Genetic predisposition ?
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
SURGERY for Desmoid tumors
always feasible?
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
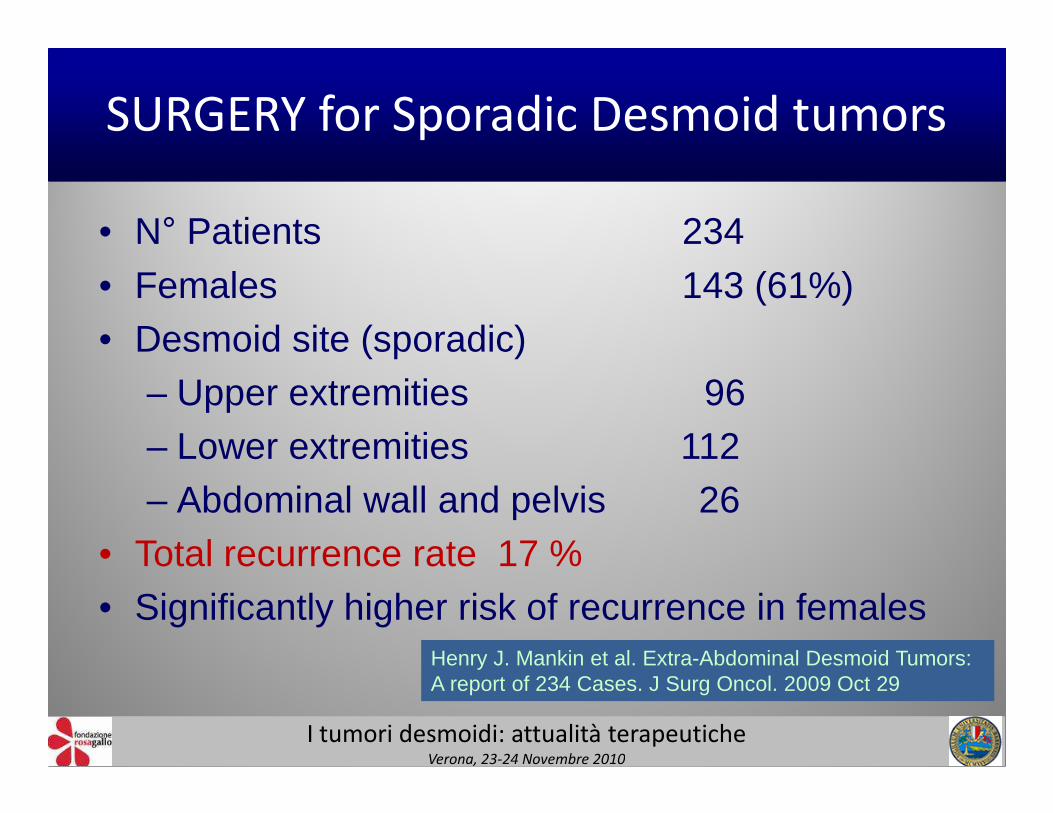
• N° Patients 234
• Females 143 (61%)• Desmoid site (sporadic)
– Upper extremities 96
SURGERY for Sporadic Desmoid tumors
– Upper extremities 96– Lower extremities 112– Abdominal wall and pelvis 26
• Total recurrence rate 17 %• Significantly higher risk of recurrence in females
Henry J. Mankin et al. Extra-Abdominal Desmoid Tumors: A report of 234 Cases. J Surg Oncol. 2009 Oct 29
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
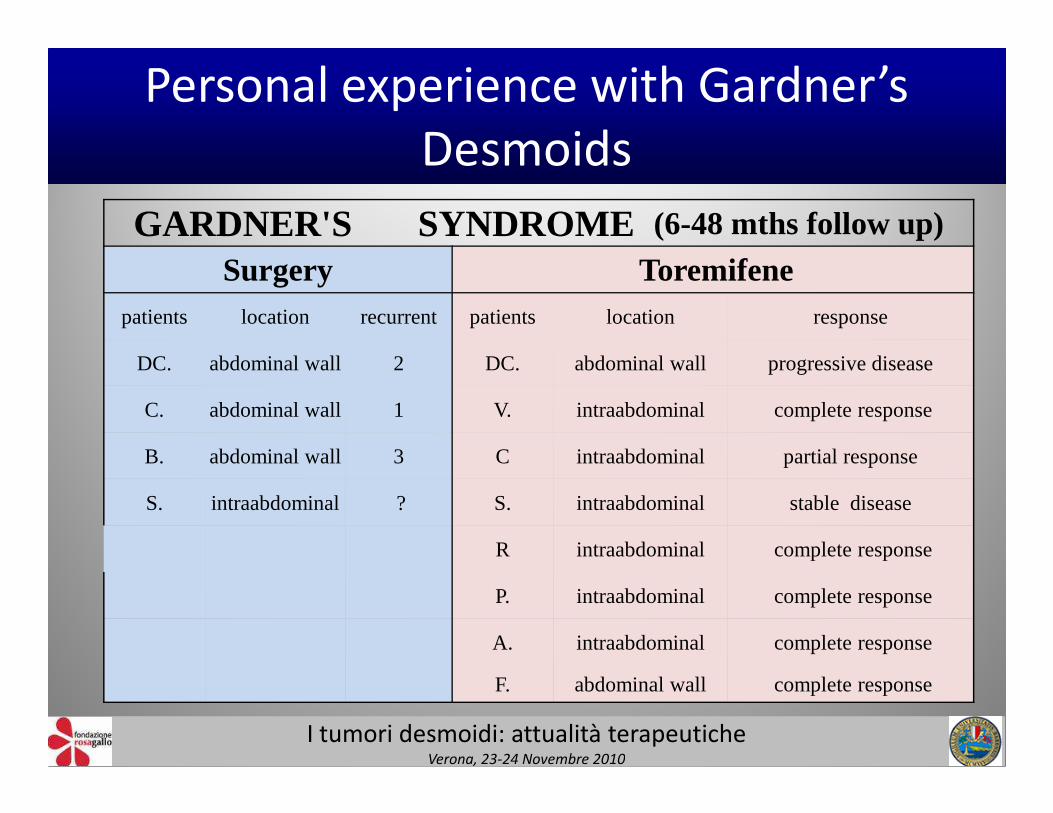
Personal experience with Gardner’s
Desmoids
GARDNER'S SYNDROME (6-48 mths follow up)
Surgery Toremifenepatients location recurrent patients location response
DC. abdominal wall 2 DC. abdominal wall progressive disease
C. abdominal wall 1 V. intraabdominal complete response
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
C. abdominal wall 1 V. intraabdominal complete response
B. abdominal wall 3 C intraabdominal partial response
S. intraabdominal ? S. intraabdominal stable disease
R intraabdominal complete response
P. intraabdominal complete response
A. intraabdominal complete response
F. abdominal wall complete response
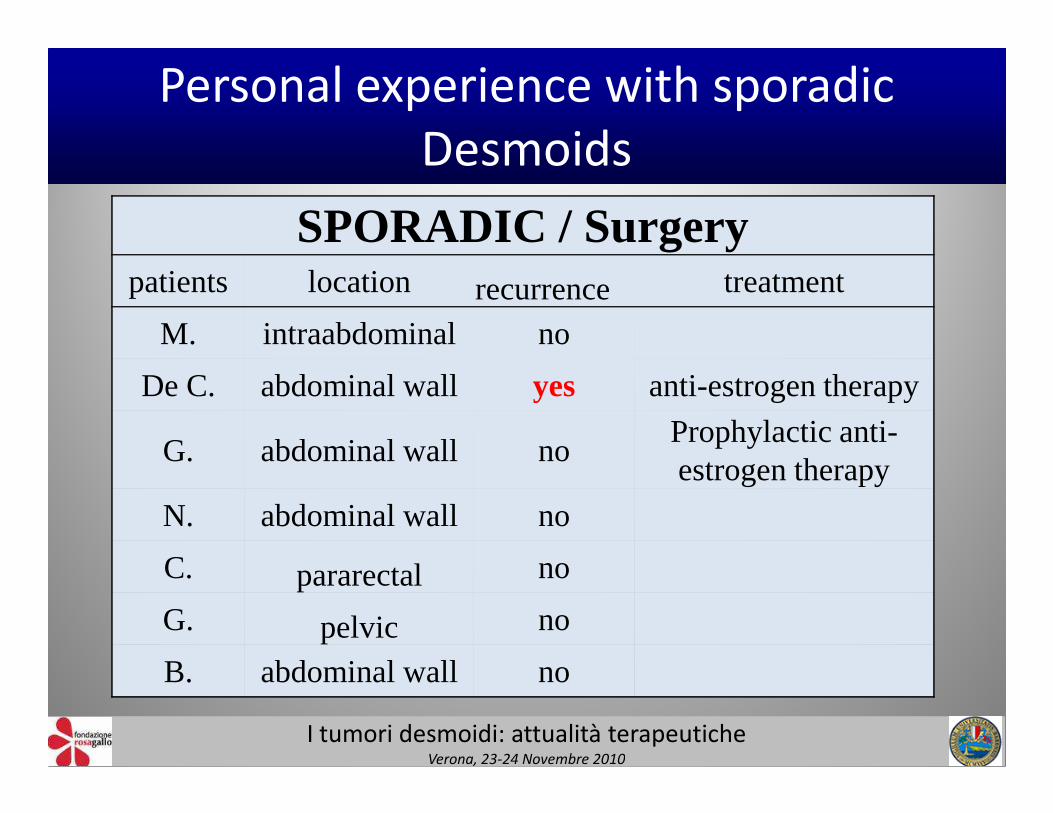
SPORADIC / Surgerypatients location recurrence treatment
M. intraabdominal no
De C. abdominal wall yes anti-estrogen therapy
Personal experience with sporadic
Desmoids
G. abdominal wall noProphylactic anti-estrogen therapy
N. abdominal wall no
C. pararectal no
G. pelvic no
B. abdominal wall no
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
• Medical therapy :
- Cytotoxic
Treatment options of Desmoid tumors
- Non cytotoxic
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
Non citotoxic treatment of Desmoid tumors
• Hormonal agentsAnti-estrogen receptors
Tamoxifene - Toremifene - Raloxifene
Progesterone, Medroxyprogesterone acetate, Prednizolone, Testolactone, Gosereline Gosereline
• Anti-inflammatory agentsSulindac (NSAID) , Celecoxib (COX-2 inhibitor)
• Other molecules Pirfenidone (antifibrotic agent)
Melatonin, Interferon alpha, Imatinib, (tyrosine kinase inhibitor)
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
Non citotoxic therapy of desmoids tumors
• Still based on empirical or anedoctical dataobtained by case reports or short caseseries where anti-hormonal, anti-inflammatory drugs, and so on.. have beeninflammatory drugs, and so on.. have beenused with alternate fortune
• Anti-estrogen therapy is the most widelyused medical treatment for DT
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
Why considering anti-estrogen therapy for desmoids?
• Female sex more frequently involved
• Often triggered by pregnancy• Often triggered by pregnancy
• Low incidence after menopause
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
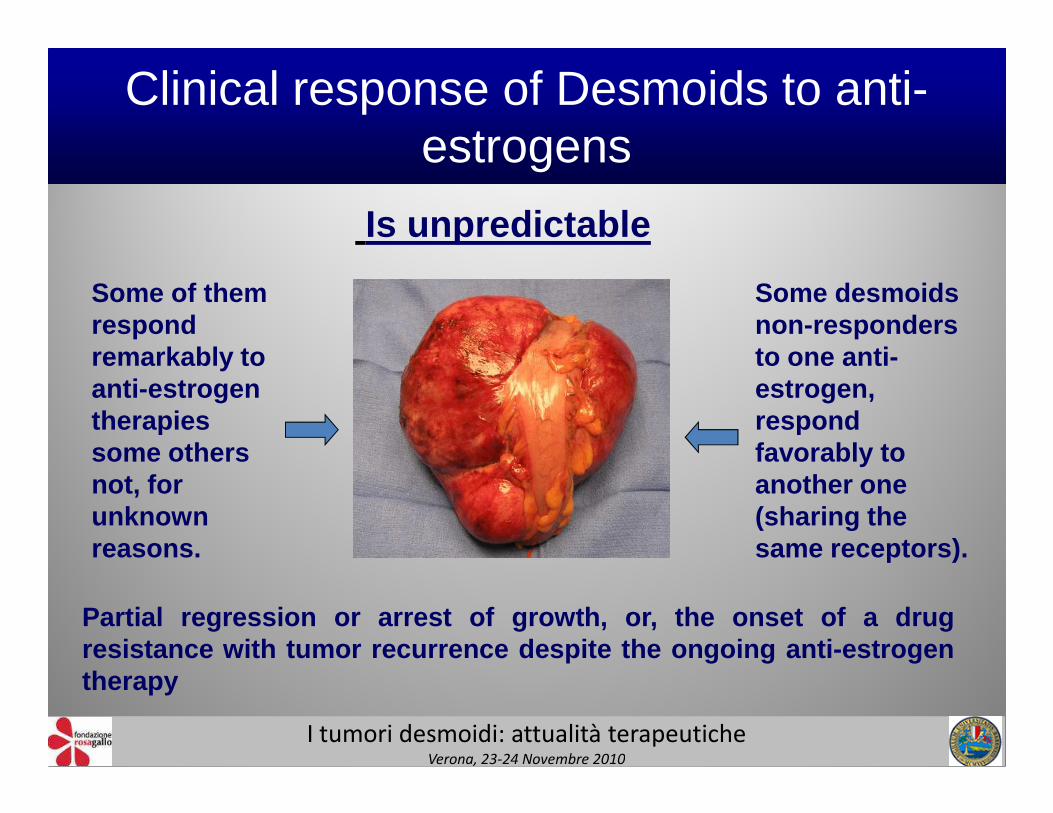
Clinical response of Desmoids to anti-estrogens
Is unpredictable
Some of them respond remarkably to anti-estrogen therapies
Some desmoids non-responders to one anti-estrogen, respond
Partial regression or arrest of growth, or, the onset of a dru gresistance with tumor recurrence despite the ongoing anti- estrogentherapy
therapies some others not, for unknown reasons.
respond favorably to another one (sharing the same receptors).
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
Anti-estrogen therapy for desmoid tumorSystematic review
• PubMed search, Excerpta Medica Database(EMBASE) , Cochrane Library, Google
• Only patients treated by Toremifene, Tamoxifeneand Raloxifene alone or in association with otherand Raloxifene alone or in association with otherdrugs
• Patients with prophylactic antiestrogen therapywere excluded
• Patients included in papers with insufficientinformation about the treatment were excluded
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
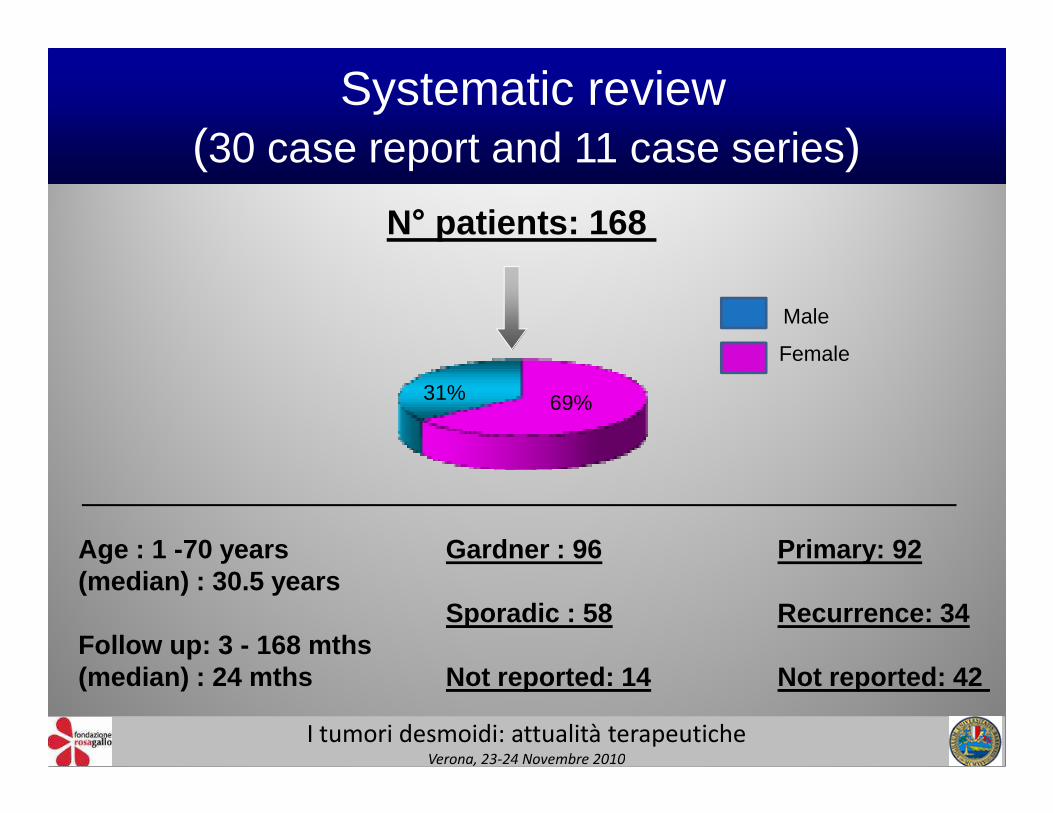
N° patients: 168
Male
Female
69%31%
Systematic review (30 case report and 11 case series)
Age : 1 -70 years(median) : 30.5 years
Follow up: 3 - 168 mths(median) : 24 mths
Primary: 92
Recurrence: 34
Not reported: 42
Gardner : 96
Sporadic : 58
Not reported: 14
69%
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
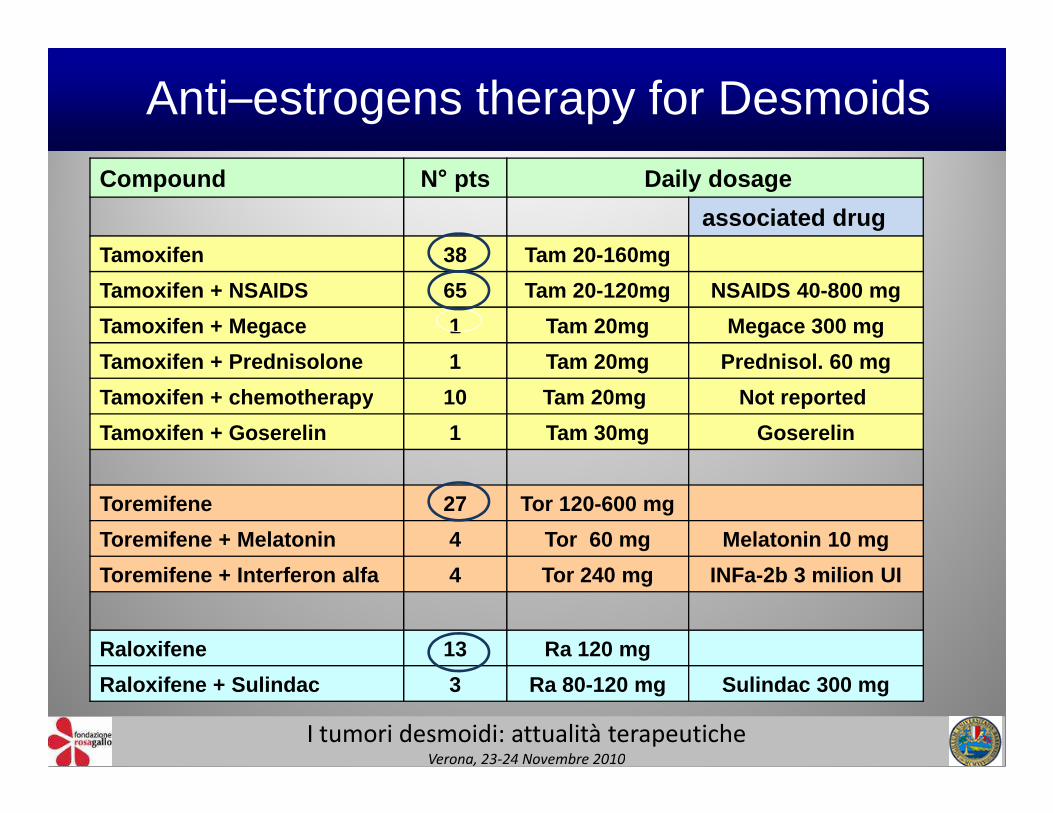
Compound N ° pts Daily dosage
associated drug
Tamoxifen 38 Tam 20-160mg
Tamoxifen + NSAIDS 65 Tam 20-120mg NSAIDS 40-800 mg
Tamoxifen + Megace 1 Tam 20mg Megace 300 mg
Tamoxifen + Prednisolone 1 Tam 20mg Prednisol. 60 mg
Tamoxifen + chemotherapy 10 Tam 20mg Not reported
Anti–estrogens therapy for Desmoids
Tamoxifen + chemotherapy 10 Tam 20mg Not reported
Tamoxifen + Goserelin 1 Tam 30mg Goserelin
Toremifene 27 Tor 120-600 mg
Toremifene + Melatonin 4 Tor 60 mg Melatonin 10 mg
Toremifene + Interferon alfa 4 Tor 240 mg INFa-2b 3 m ilion UI
Raloxifene 13 Ra 120 mg
Raloxifene + Sulindac 3 Ra 80-120 mg Sulindac 300 mg
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
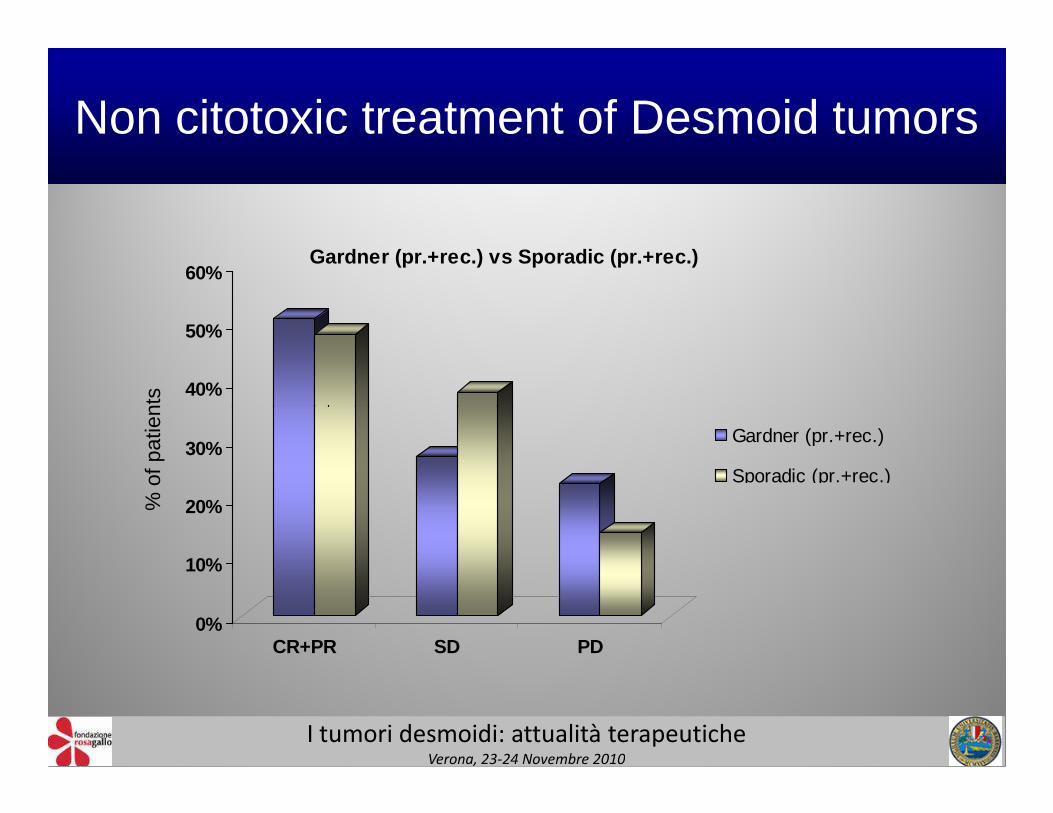
Non citotoxic treatment of Desmoid tumors
40%
50%
60% Gardner (pr.+rec.) vs Sporadic (pr.+rec.)
% o
f pat
ient
s
0%
10%
20%
30%
CR+PR SD PD
Gardner (pr.+rec.)
Sporadic (pr.+rec.)
% o
f pat
ient
s
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
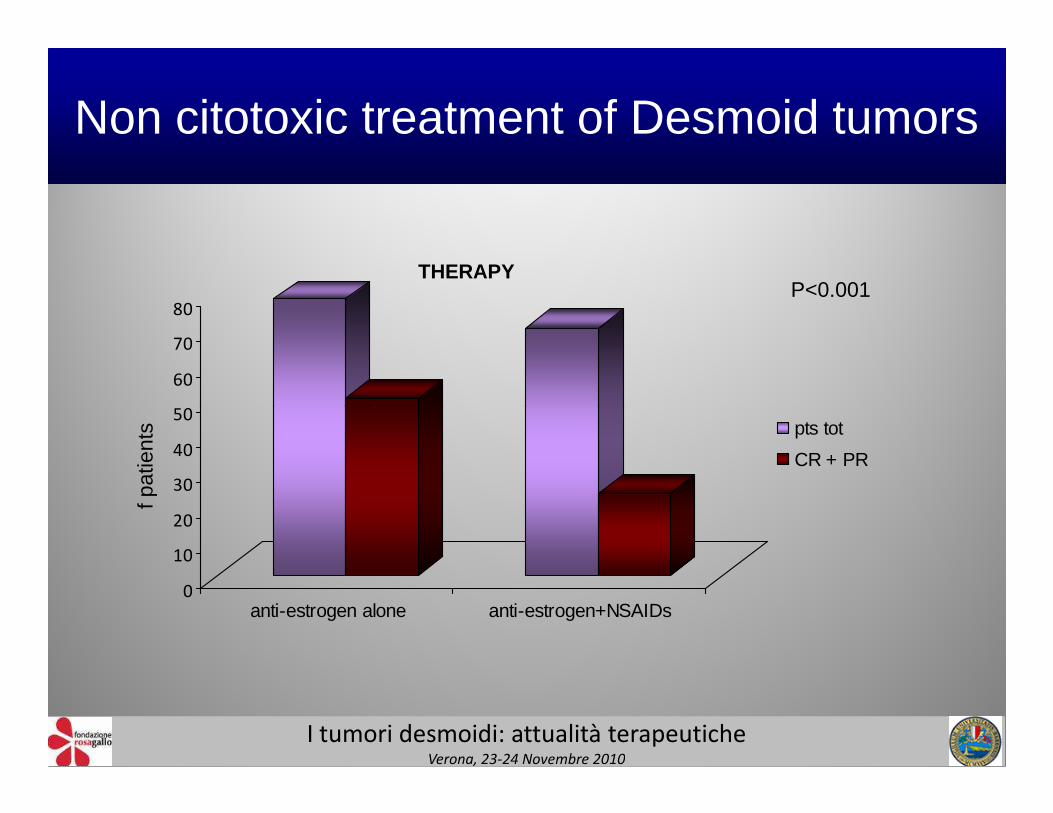
Non citotoxic treatment of Desmoid tumors
50
60
70
80
THERAPYP<0.001
0
10
20
30
40
50
anti-estrogen alone anti-estrogen+NSAIDs
pts tot
CR + PR
f pat
ient
s
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
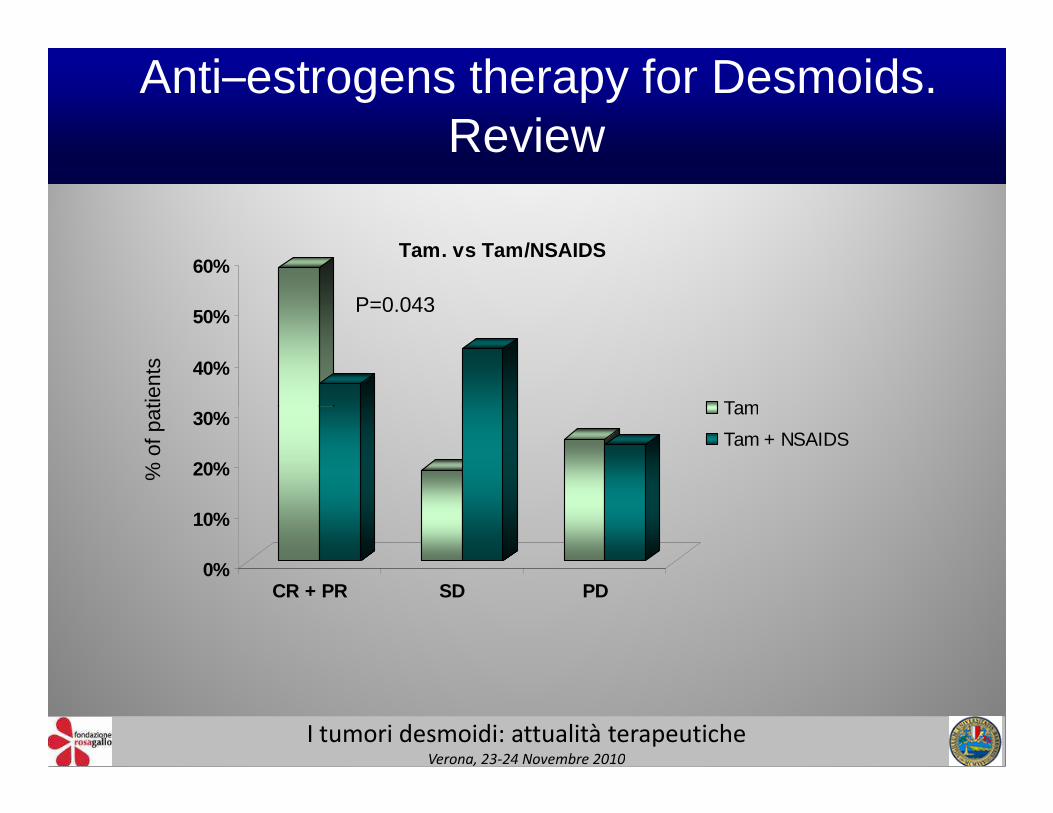
40%
50%
60%
Tam
Tam. vs Tam/NSAIDS
Anti–estrogens therapy for Desmoids. Review
% o
f pat
ient
s
P=0.043
0%
10%
20%
30%
CR + PR SD PD
Tam
Tam + NSAIDS
% o
f pat
ient
s
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
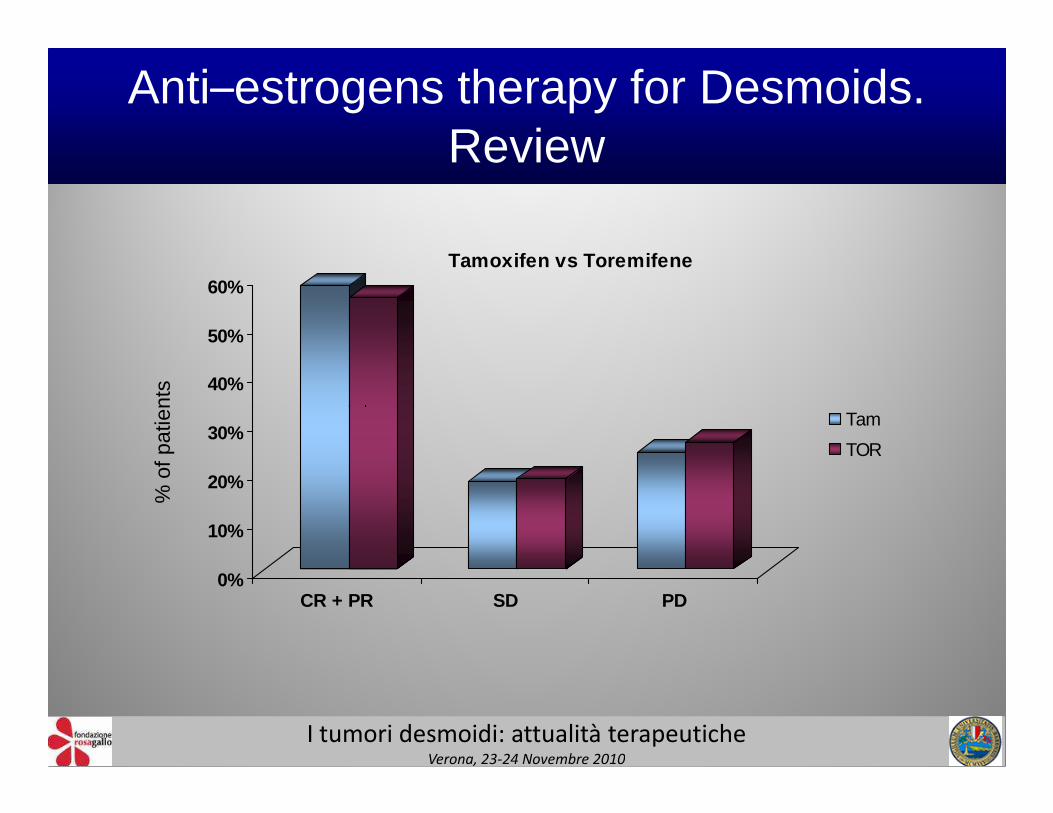
Anti–estrogens therapy for Desmoids. Review
40%
50%
60%Tamoxifen vs Toremifene
% o
f pat
ient
s
0%
10%
20%
30%
CR + PR SD PD
Tam
TOR
% o
f pat
ient
s
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
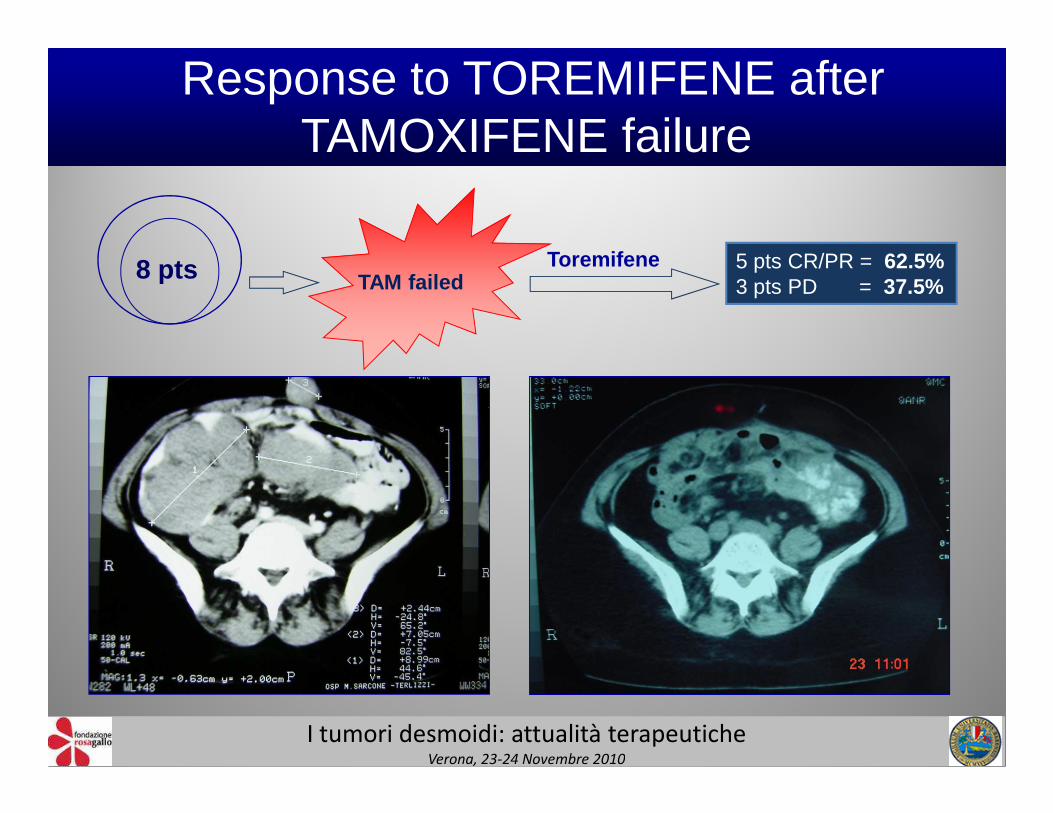
8 pts TAM failedToremifene 5 pts CR/PR = 62.5%
3 pts PD = 37.5%
Response to TOREMIFENE after TAMOXIFENE failure
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
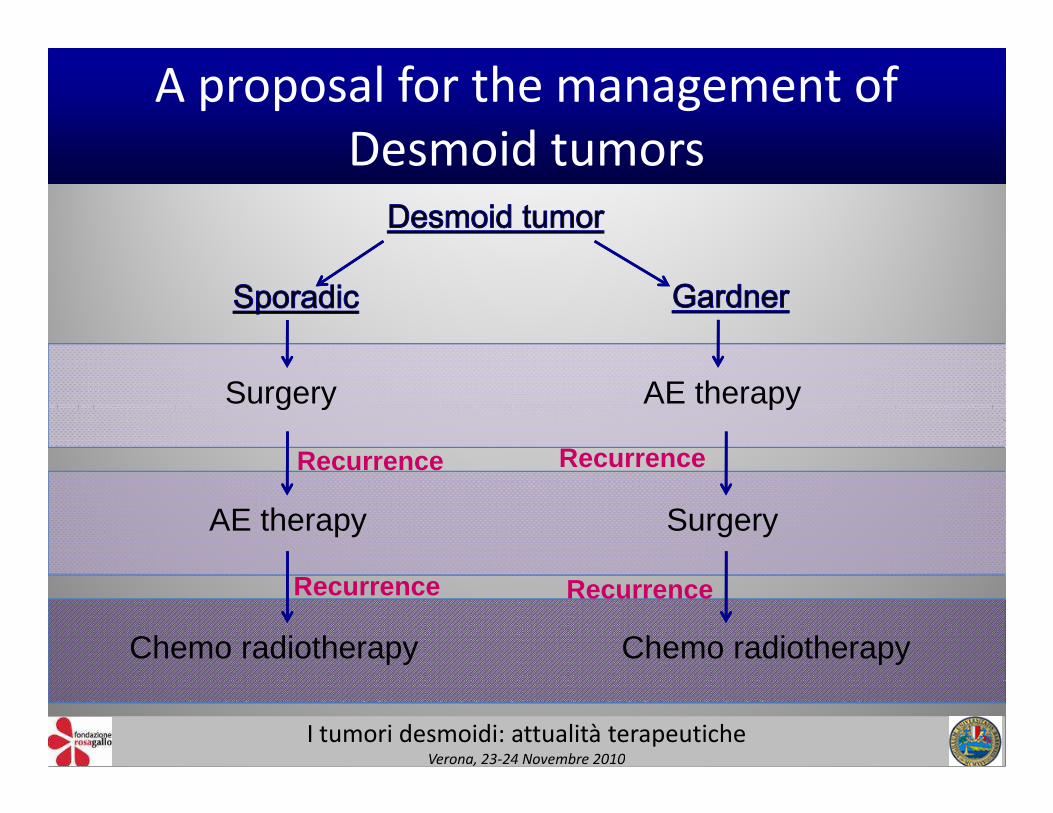
A proposal for the management of
Desmoid tumors
Surgery AE therapy
AE therapy Surgery
Chemo radiotherapy Chemo radiotherapy
Surgery AE therapy
Recurrence
Recurrence Recurrence
Recurrence
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010
CONCLUSIONS
Despite several bias can limit the reliabilityof the data reported in the literature, theuse of anti-oestrogen is fully justified as analternative to chemo or radiotherapy beforealternative to chemo or radiotherapy beforeor instead of surgery, particularly whensurgical removal is life-threatening orimpossible
(level of evidence III, grade of recommendation D)
I tumori desmoidi: attualità terapeuticheVerona, 23-24 Novembre 2010

Grazie per l’attenzione