ablation ou traitement pharmacologique pour la fa : quelles stratégie à suivre ? (pr l. jordaens)
TRANSCRIPT
Ablation ou traitement
pharmacologique pour la FA:
quelle stratégie a suivre ?
Luc Jordaens
Nouvelles frontières pour la prise en chargede la fibrillation auriculaire
Brussels 29-11-2014
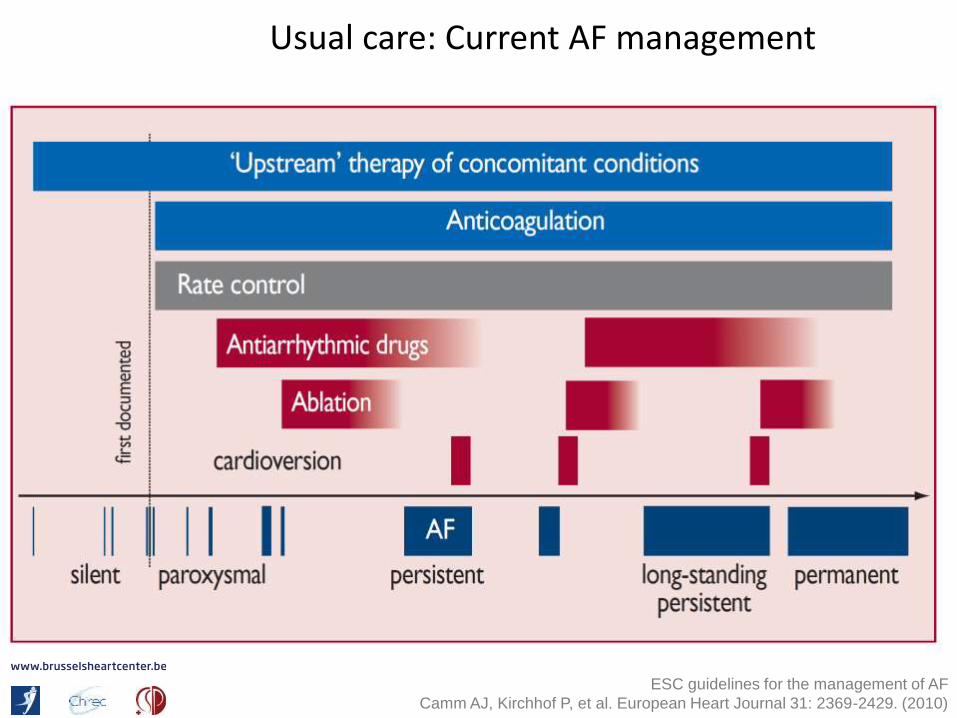
Usual care: Current AF management
ESC guidelines for the management of AF
Camm AJ, Kirchhof P, et al. European Heart Journal 31: 2369-2429. (2010)

Maintenance of sinus rhythmin atrial fibrillation
received a bad reputation in the early years 2000
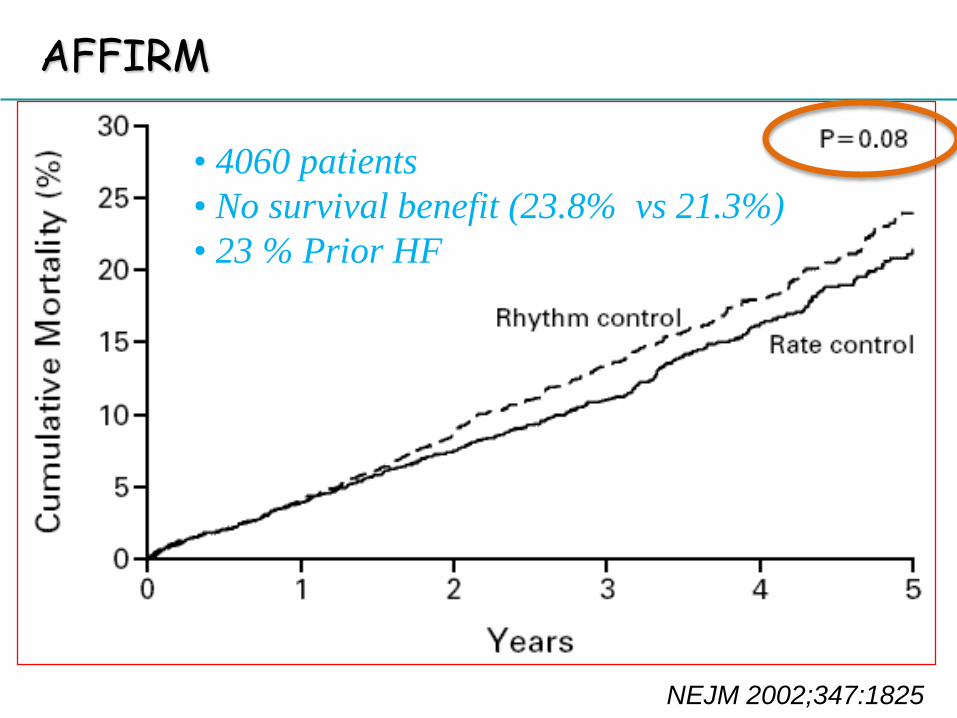
AFFIRM
NEJM 2002;347:1825
• 4060 patients
• No survival benefit (23.8% vs 21.3%)
• 23 % Prior HF
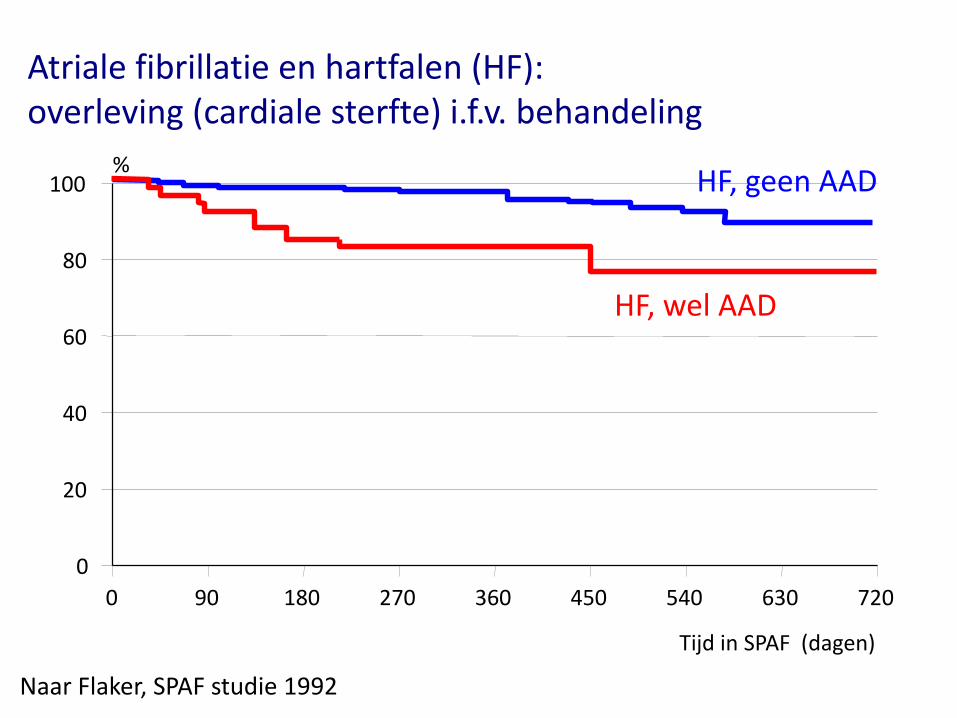
Atriale fibrillatie en hartfalen (HF):overleving (cardiale sterfte) i.f.v. behandeling
Naar Flaker, SPAF studie 1992
0 90 180 270 360 450 540 630 720
Tijd in SPAF (dagen)
0
20
40
60
80
100%
HF, wel AAD
HF, geen AAD
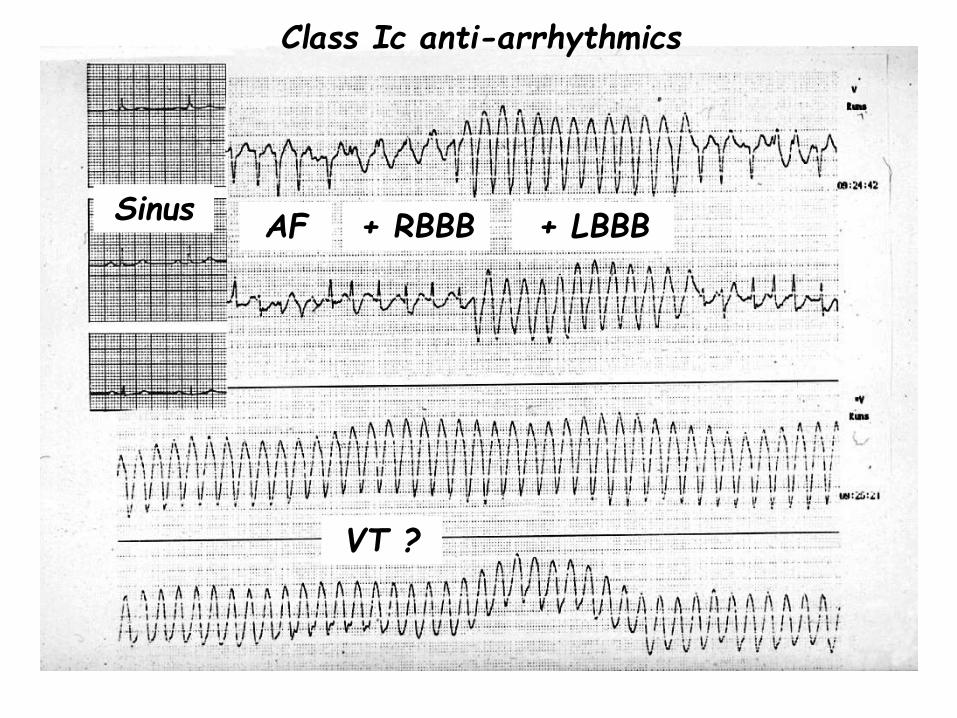
Class Ic anti-arrhythmics
AF + RBBB + LBBB
VT ?
Sinus
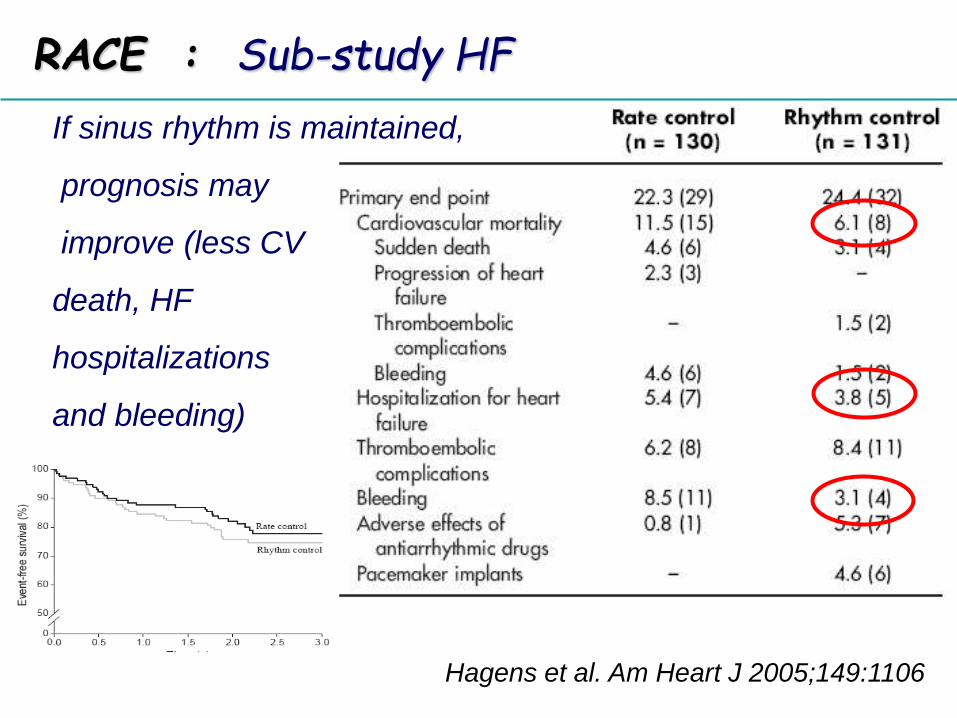
RACE : Sub-study HF
Hagens et al. Am Heart J 2005;149:1106
If sinus rhythm is maintained,
prognosis may
improve (less CV
death, HF
hospitalizations
and bleeding)
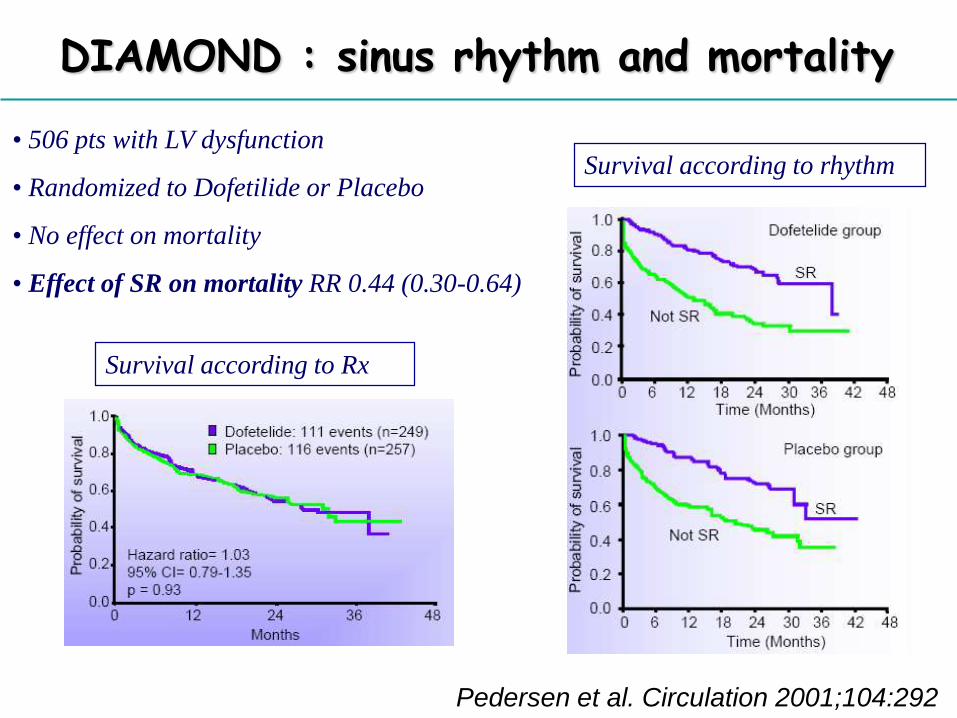
DIAMOND : sinus rhythm and mortality
Pedersen et al. Circulation 2001;104:292
• 506 pts with LV dysfunction
• Randomized to Dofetilide or Placebo
• No effect on mortality
• Effect of SR on mortality RR 0.44 (0.30-0.64)
Survival according to Rx
Survival according to rhythm
Atrial fibrillation: rate or rhythm control ?
Rate control can be acceptable
Rhythm control has some
advantages , when wisely used
SINUS RHYTHM IS BETTER !
Catheter / surgical ablationis aimed to
achieve sinus rhythm
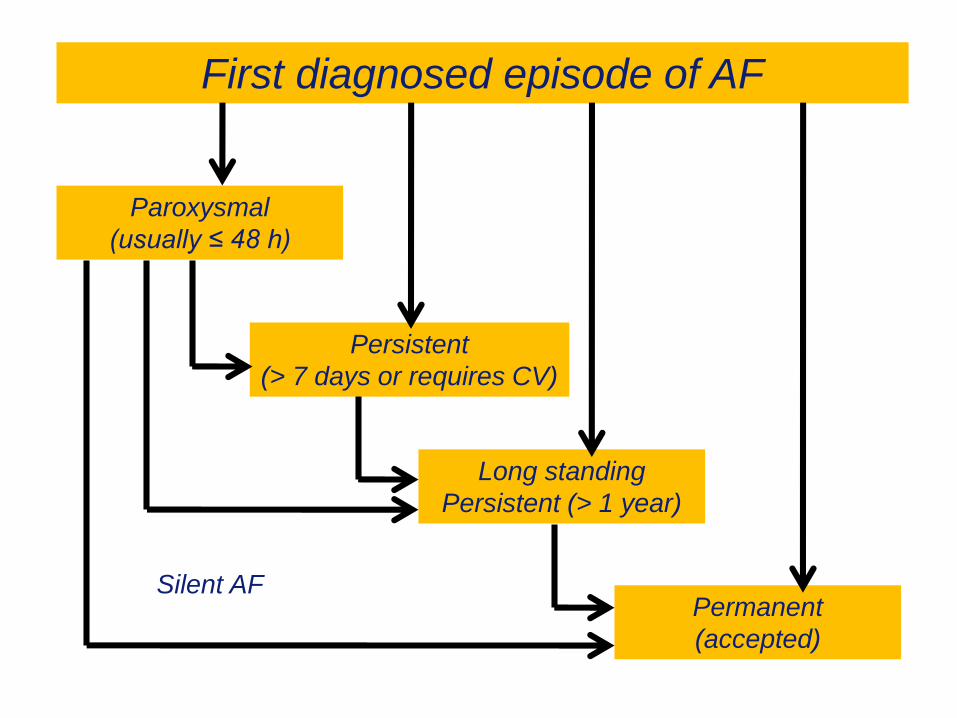
First diagnosed episode of AF
Persistent
(> 7 days or requires CV)
Long standing
Persistent (> 1 year)
Permanent
(accepted)
Paroxysmal
(usually ≤ 48 h)
Silent AF
12
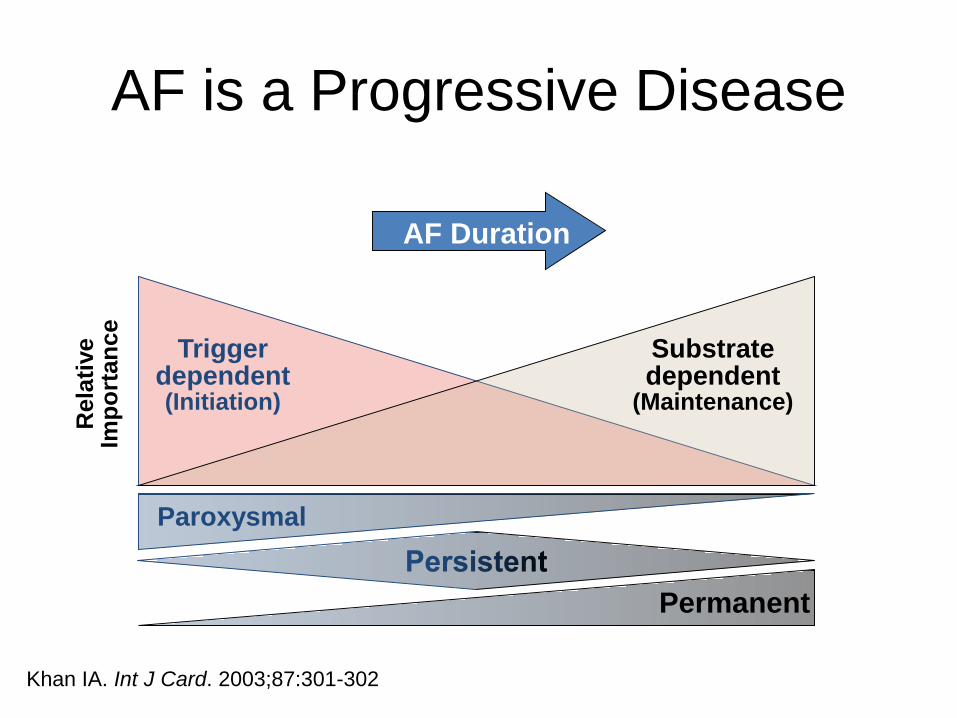
AF Duration
AF is a Progressive Disease
Paroxysmal
Trigger dependent(Initiation)
Permanent
Substrate dependent
(Maintenance)
Rela
tive
Imp
ort
an
ce
Khan IA. Int J Card. 2003;87:301-302
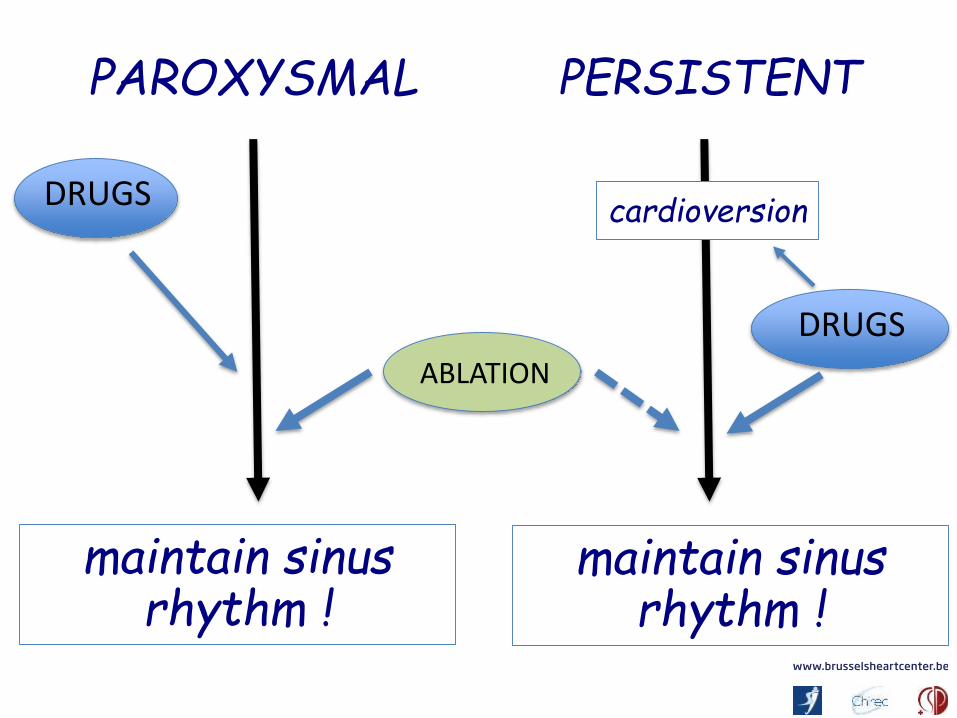
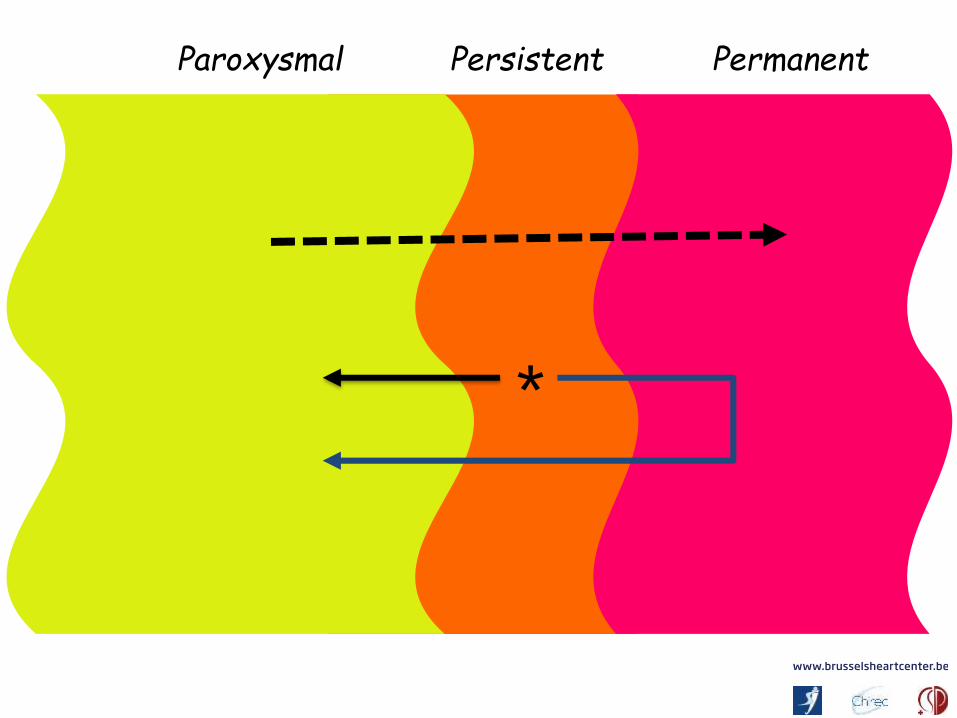
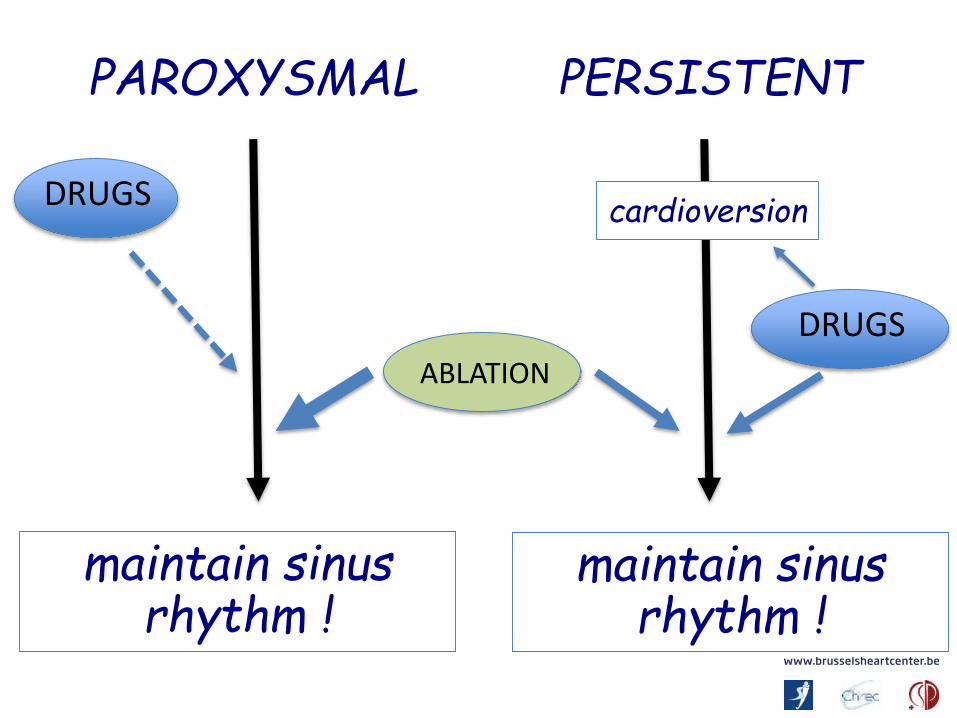
PAROXYSMAL PERSISTENT
maintain sinusrhythm !
maintain sinusrhythm !
cardioversionDRUGS
DRUGS
ABLATION
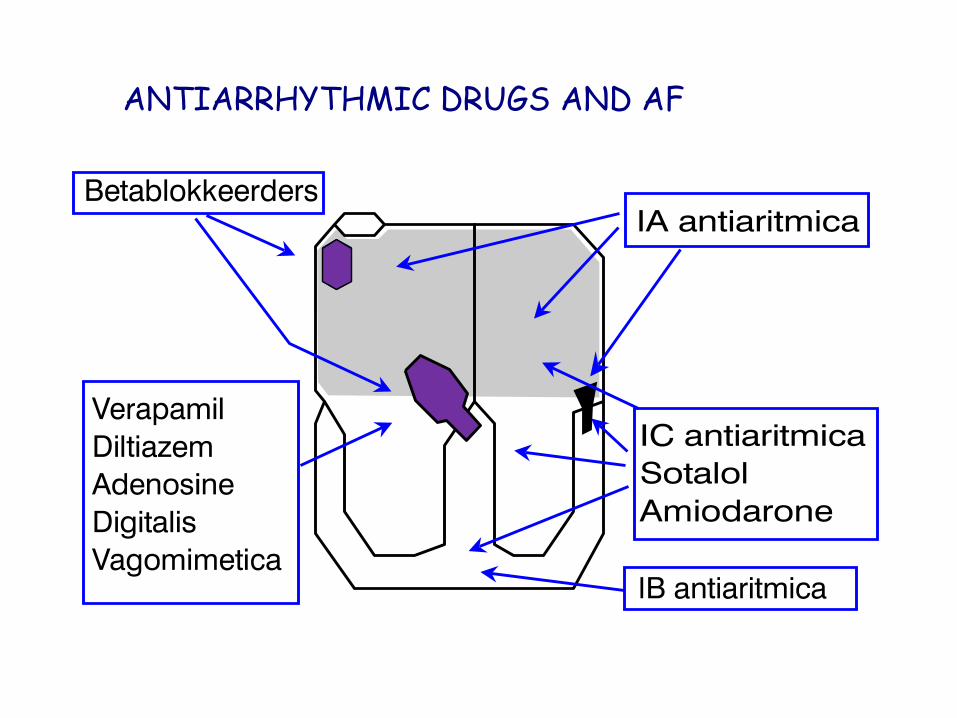
ANTIARRHYTHMIC DRUGS AND AF
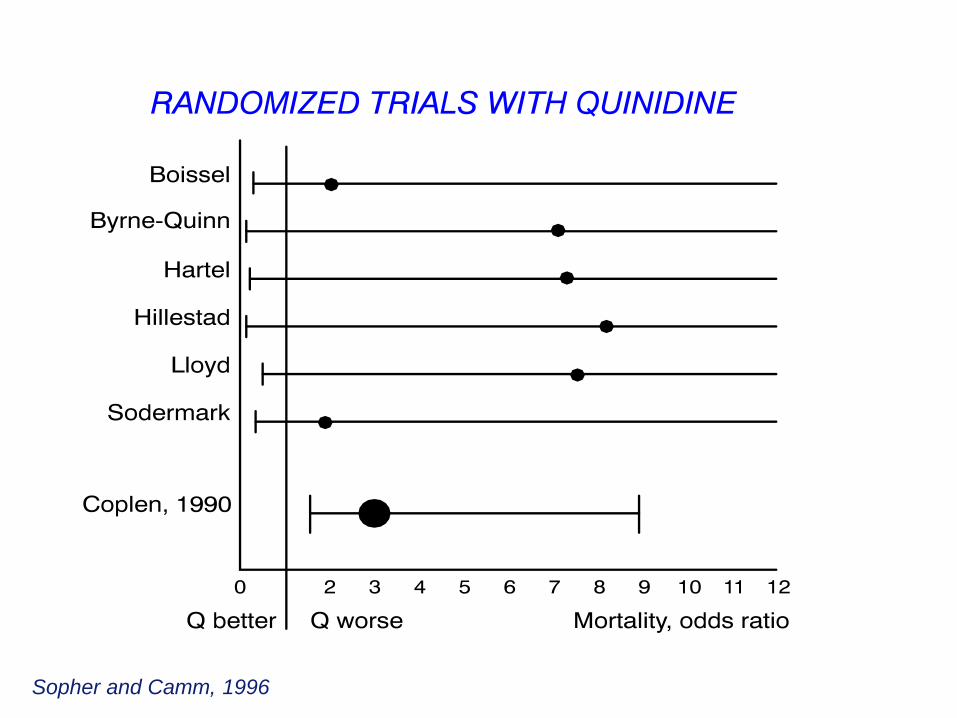
Sopher and Camm, 1996
?
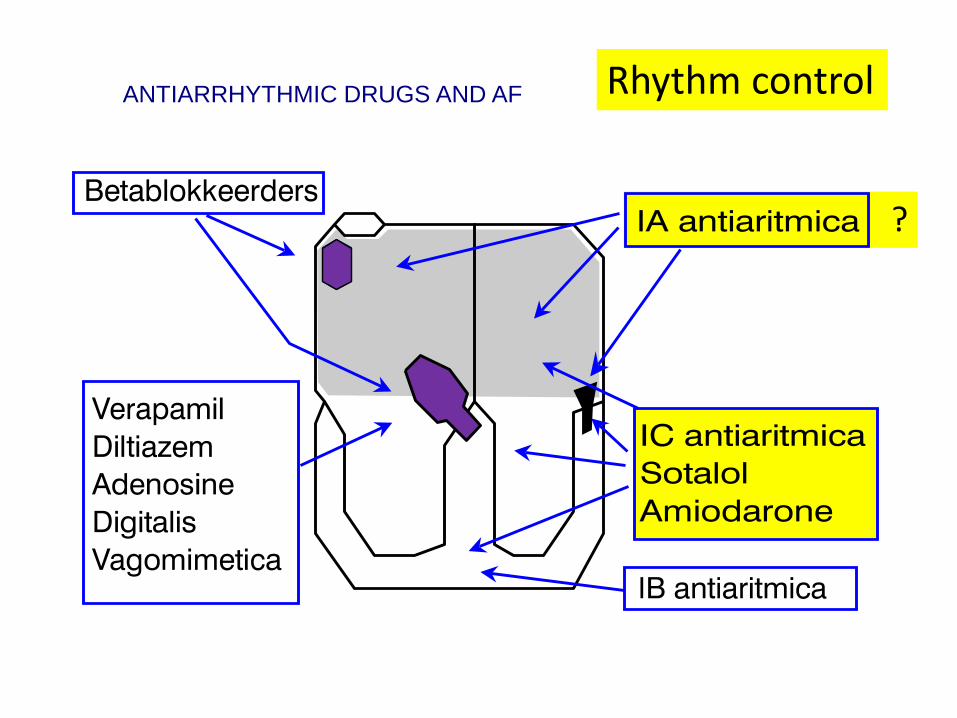
ANTIARRHYTHMIC DRUGS AND AF Rhythm control
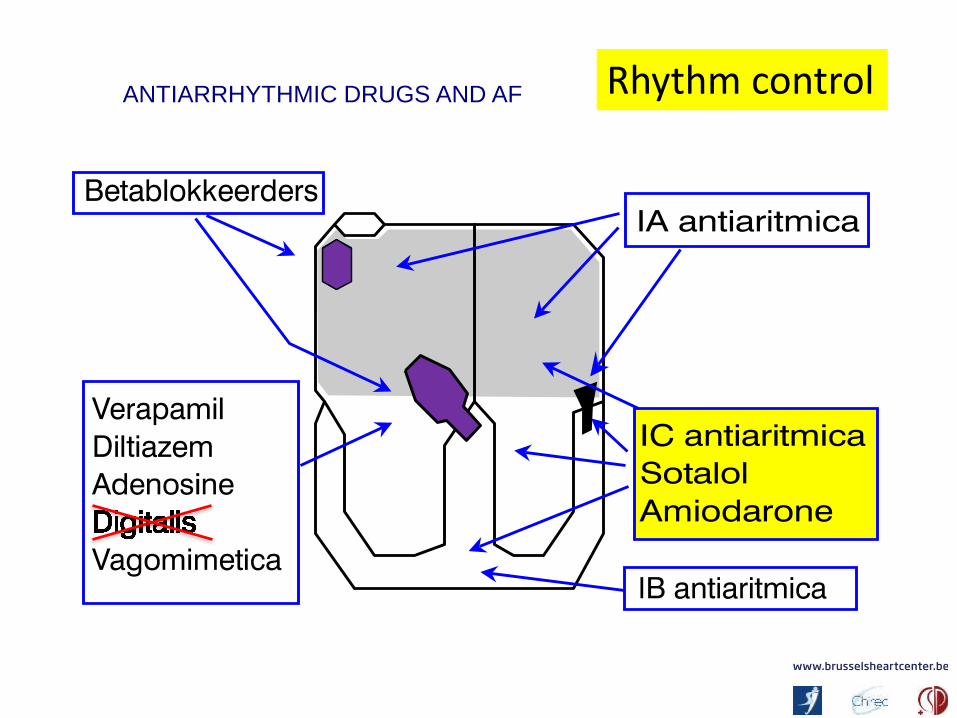
ANTIARRHYTHMIC DRUGS AND AF Rhythm control
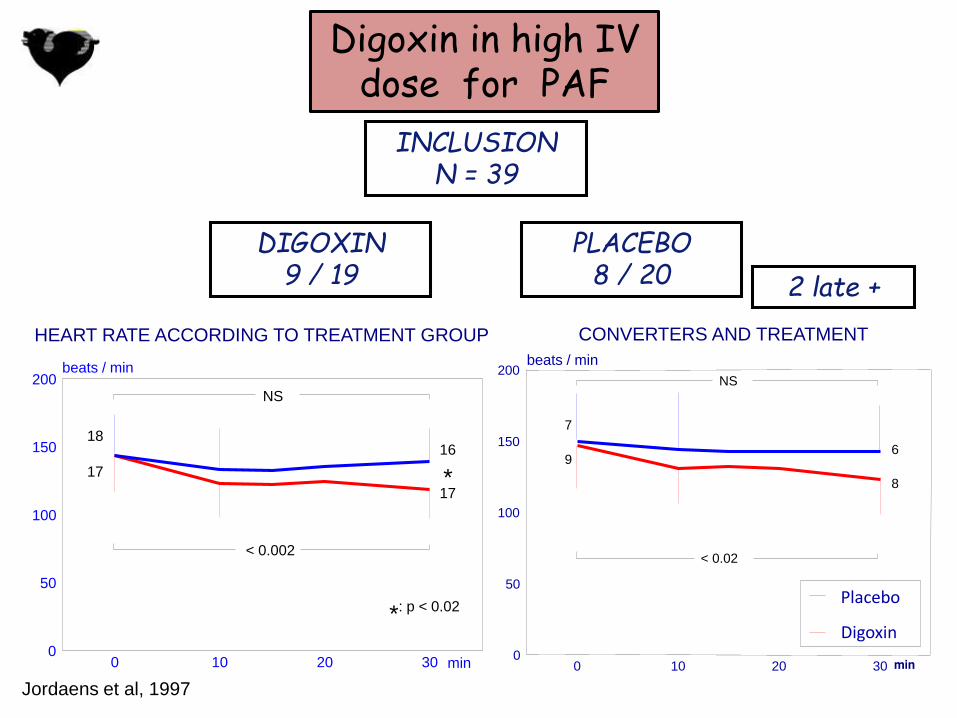
2 late +
INCLUSIONN = 39
DIGOXIN9 / 19
PLACEBO8 / 20
Digoxin in high IV dose for PAF
Jordaens et al, 1997
HEART RATE ACCORDING TO TREATMENT GROUP
0 10 20 300
50
100
150
200beats / min
18
17
16
17
min
: p < 0.02*
*
NS
< 0.002
CONVERTERS AND TREATMENT
0 10 20 300
50
100
150
200beats / min
< 0.02
NS
7
96
8
Placebo
Digoxin
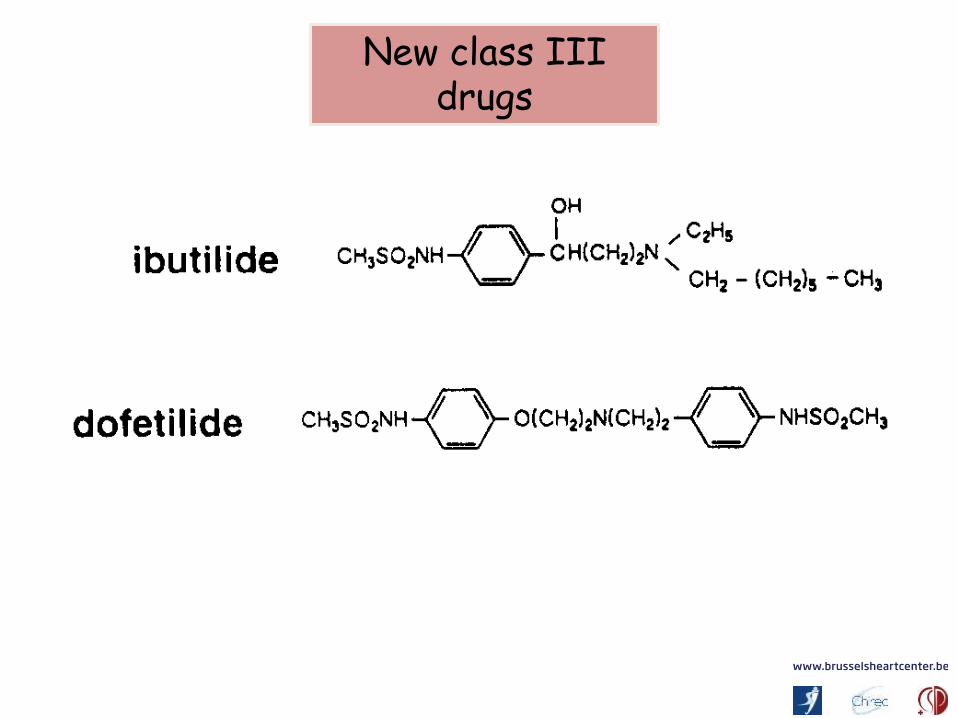
New class IIIdrugs
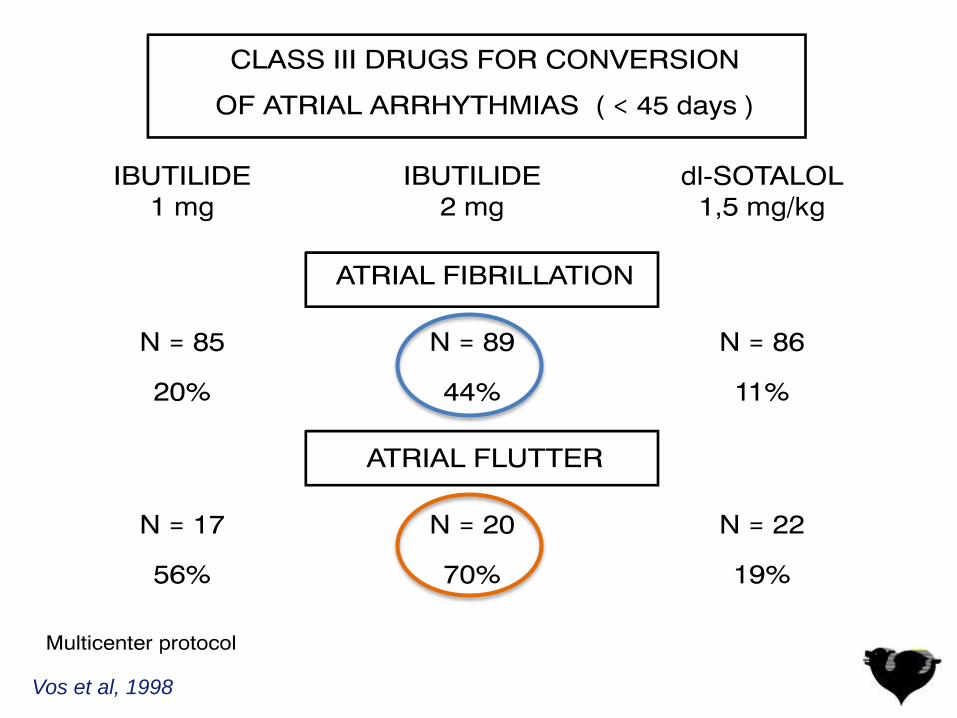
Vos et al, 1998
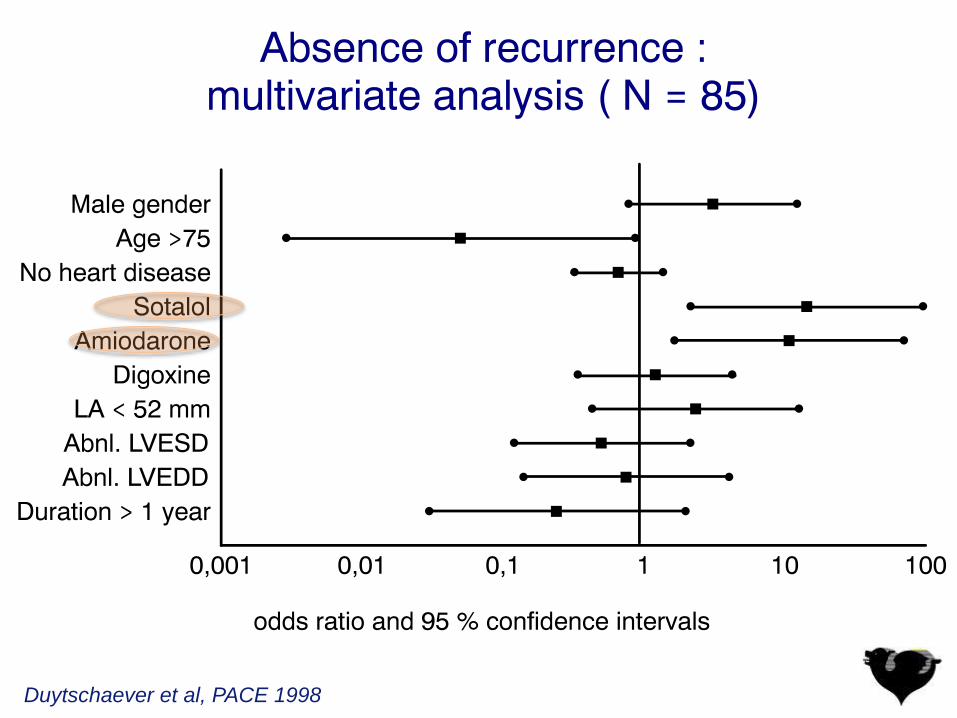
Duytschaever et al, PACE 1998

Roy et al, 2000
Patients without
recurrence (%)
Prophylactic antiarrhythmic therapy
in ’’ paroxysmal” atrial fibrillation
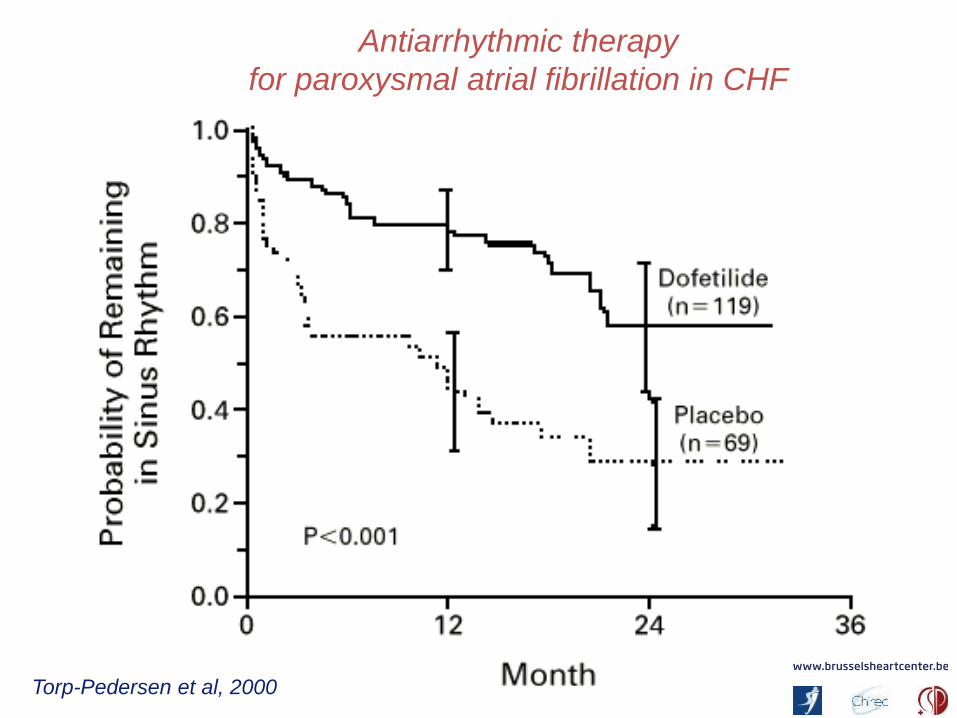
Torp-Pedersen et al, 2000
Antiarrhythmic therapy
for paroxysmal atrial fibrillation in CHF
Meta analysis of drugs: mortality
11 new studies comprising 20.771 patients.
Compared with controls, class IA drugs quinidineand disopyramide (OR 2.39, 95% confidenceinterval (95%CI) 1.03 to 5.59, number needed toharm (NNH) 109, 95%CI 34 to 4985) and sotalol (OR 2.47, 95%CI 1.2 to 5.05, NNH 166, 95%CI 61 to1159) were associated with increased all-causemortality. Other antiarrhythmics did not seem tomodify mortality.
Cochrane review, 2012
• Several class IA (disopyramide, quinidine), IC (flecainide, propafenone) and III (amiodarone, dofetilide, dronedarone, sotalol) drugs significantly reduced recurrence of AF (OR 0.19 to 0.70, number needed to treat (NNT) 3 to 16).
• Beta-blockers (metoprolol) also reducedsignificantly AF recurrence (OR 0.62, 95% CI 0.44 to 0.88, NNT 9).
Meta analysis of drugs: efficacy
Cochrane review, 2012
• All analysed drugs increased withdrawals dueto adverse affects and all but amiodarone, dronedarone and propafenone increased pro-arrhythmia.
• Possible benefits on clinically relevant outcomes (stroke, embolisms, heart failure) remain to be established.
Meta analysis of drugs: adverse effects
Cochrane review, 2012
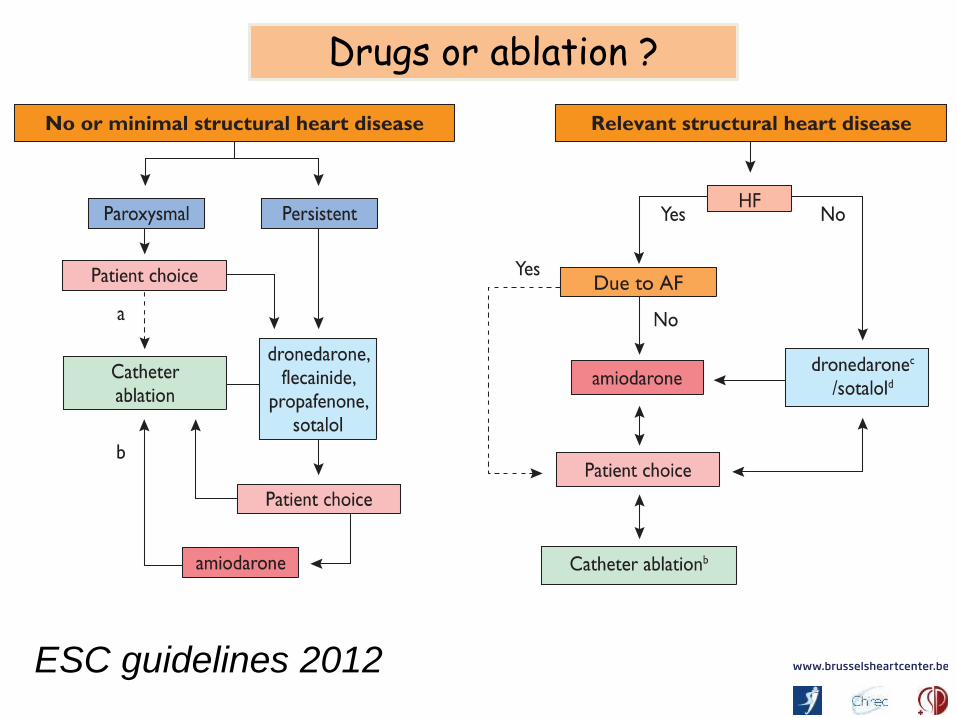
ESC guidelines 2012
Drugs or ablation ?

Wilber et al, 2012
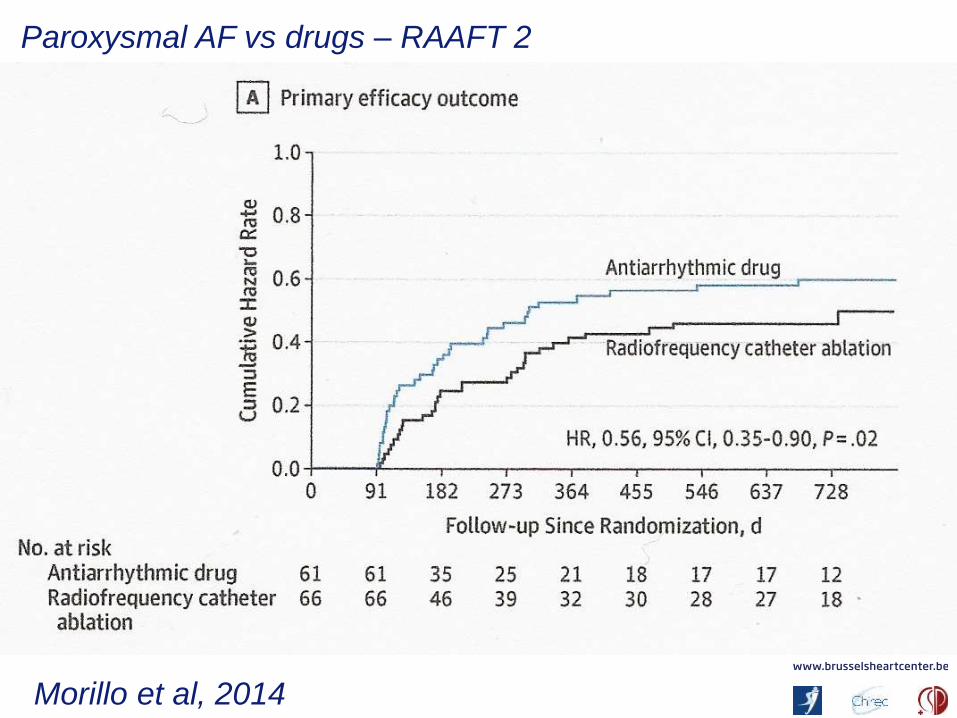
Morillo et al, 2014
Paroxysmal AF vs drugs – RAAFT 2
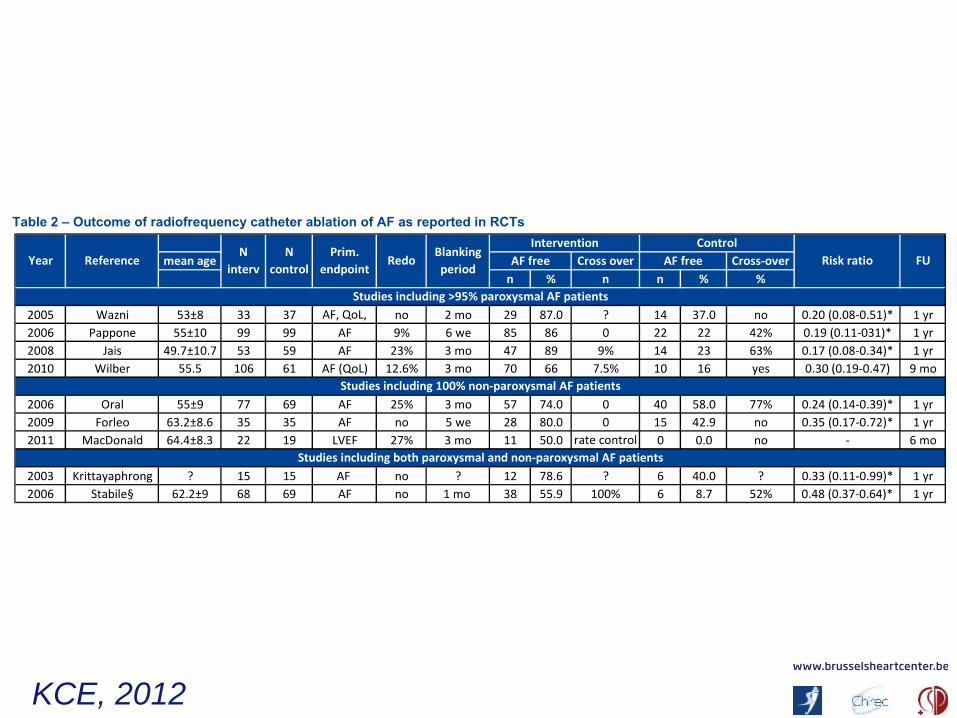
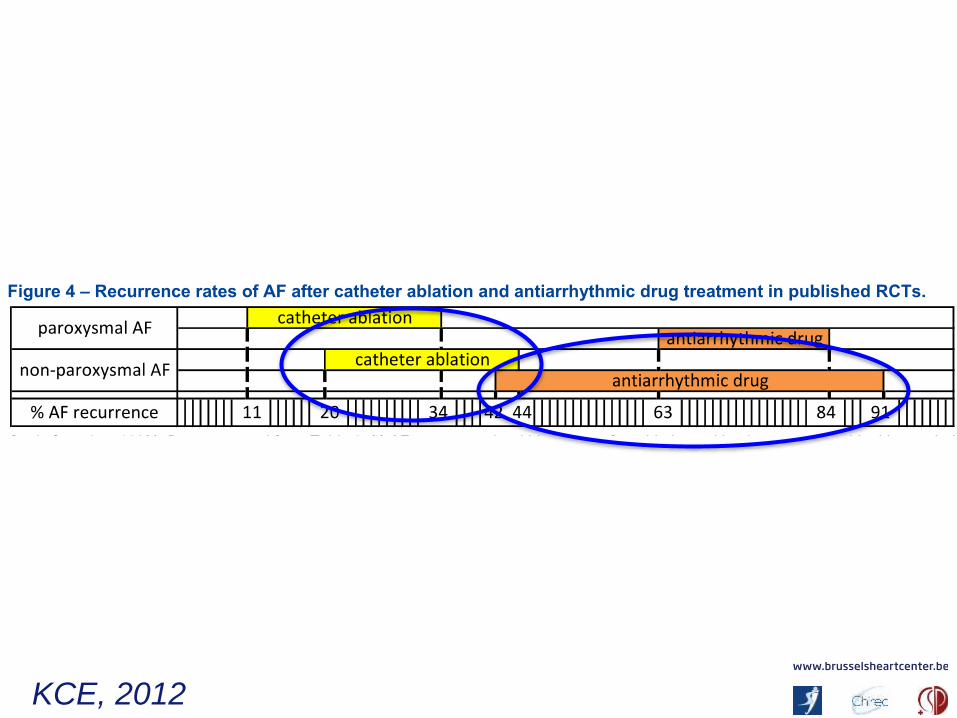
KCE, 2012
KCE, 2012
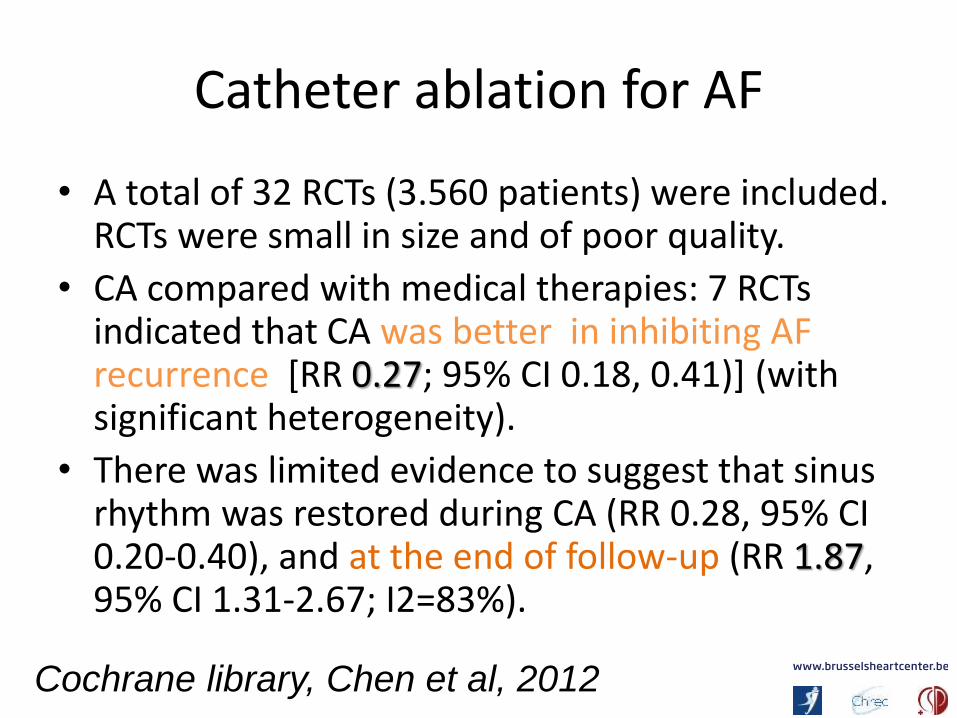
Catheter ablation for AF
• A total of 32 RCTs (3.560 patients) were included. RCTs were small in size and of poor quality.
• CA compared with medical therapies: 7 RCTsindicated that CA was better in inhibiting AF recurrence [RR 0.27; 95% CI 0.18, 0.41)] (withsignificant heterogeneity).
• There was limited evidence to suggest that sinus rhythm was restored during CA (RR 0.28, 95% CI 0.20-0.40), and at the end of follow-up (RR 1.87, 95% CI 1.31-2.67; I2=83%).
Cochrane library, Chen et al, 2012
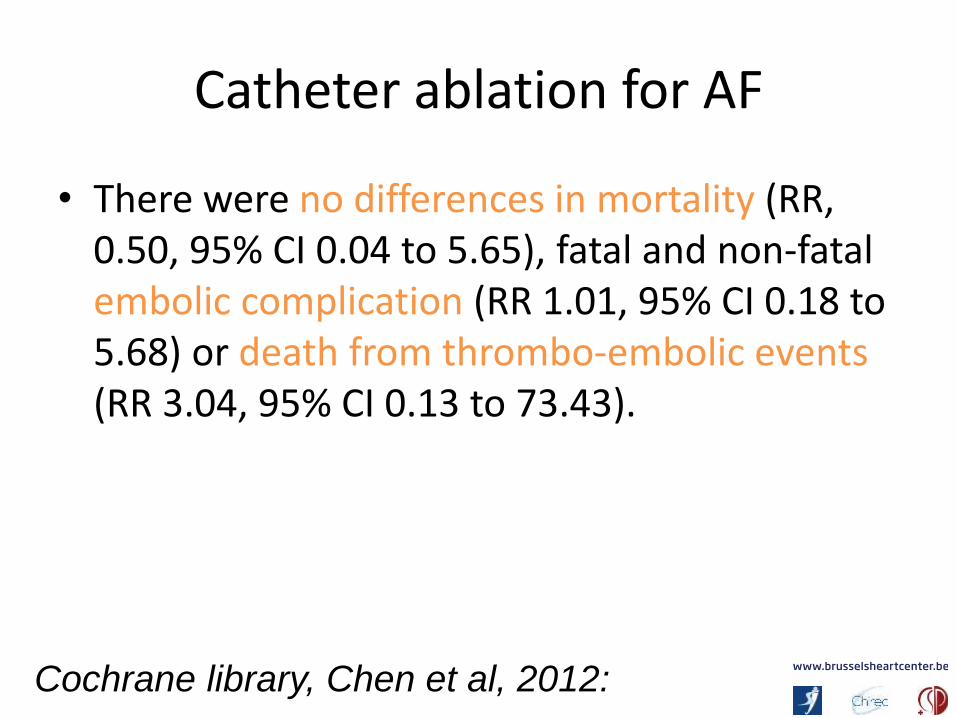
Catheter ablation for AF
• There were no differences in mortality (RR, 0.50, 95% CI 0.04 to 5.65), fatal and non-fatalembolic complication (RR 1.01, 95% CI 0.18 to 5.68) or death from thrombo-embolic events (RR 3.04, 95% CI 0.13 to 73.43).
Cochrane library, Chen et al, 2012:
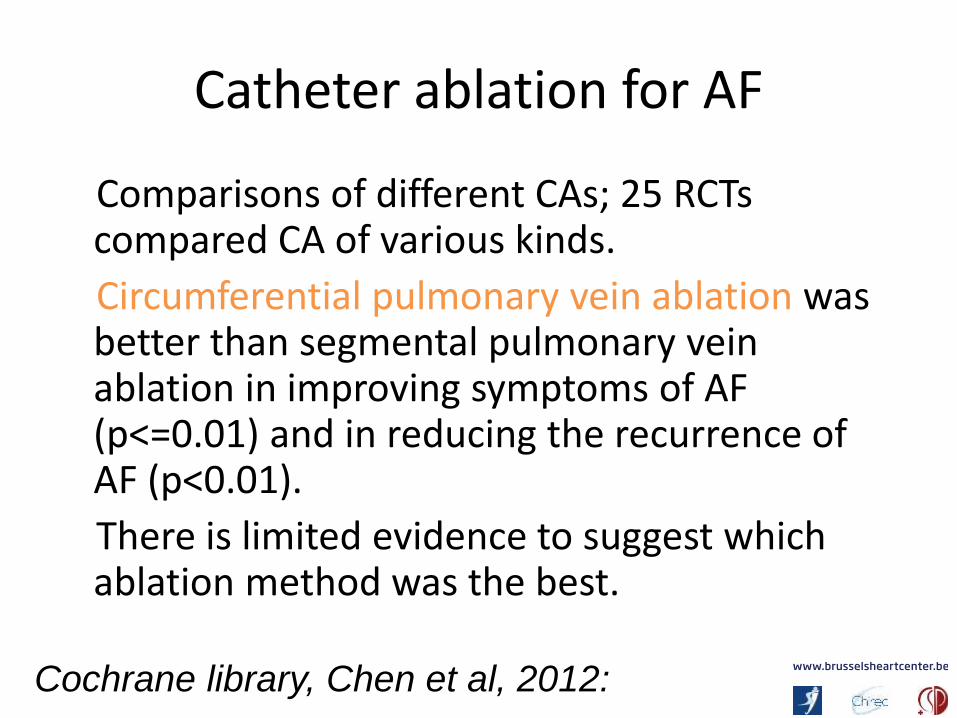
Catheter ablation for AF
Comparisons of different CAs; 25 RCTscompared CA of various kinds.
Circumferential pulmonary vein ablation was better than segmental pulmonary veinablation in improving symptoms of AF (p<=0.01) and in reducing the recurrence of AF (p<0.01).
There is limited evidence to suggest whichablation method was the best.
Cochrane library, Chen et al, 2012:
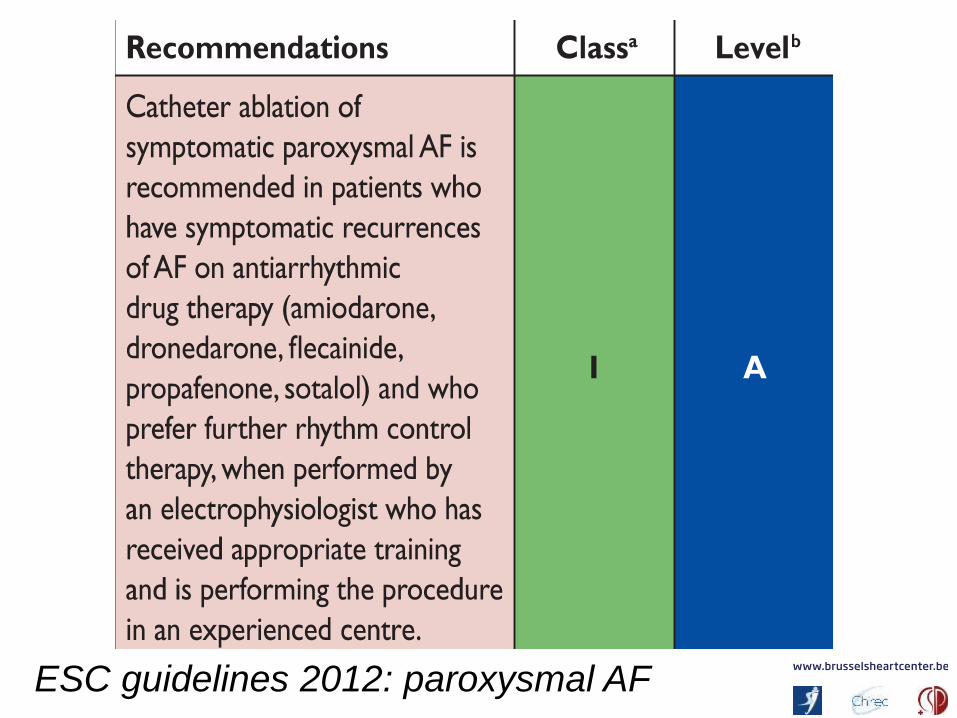
ESC guidelines 2012: paroxysmal AF
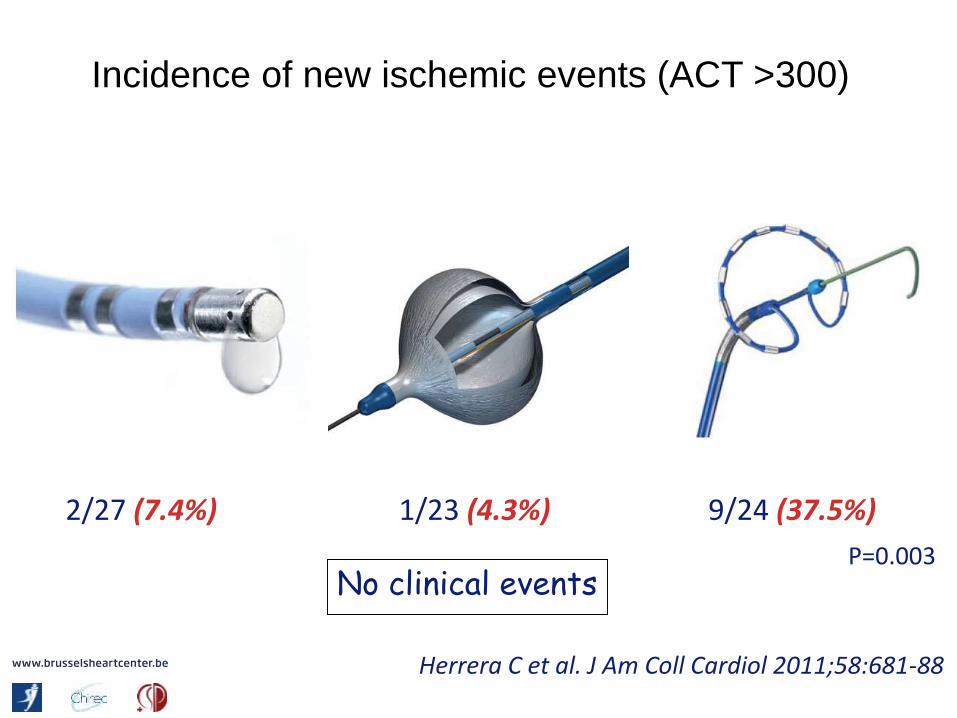
Incidence of new ischemic events (ACT >300)
No clinical events
2/27 (7.4%) 1/23 (4.3%) 9/24 (37.5%)
P=0.003
Herrera C et al. J Am Coll Cardiol 2011;58:681-88

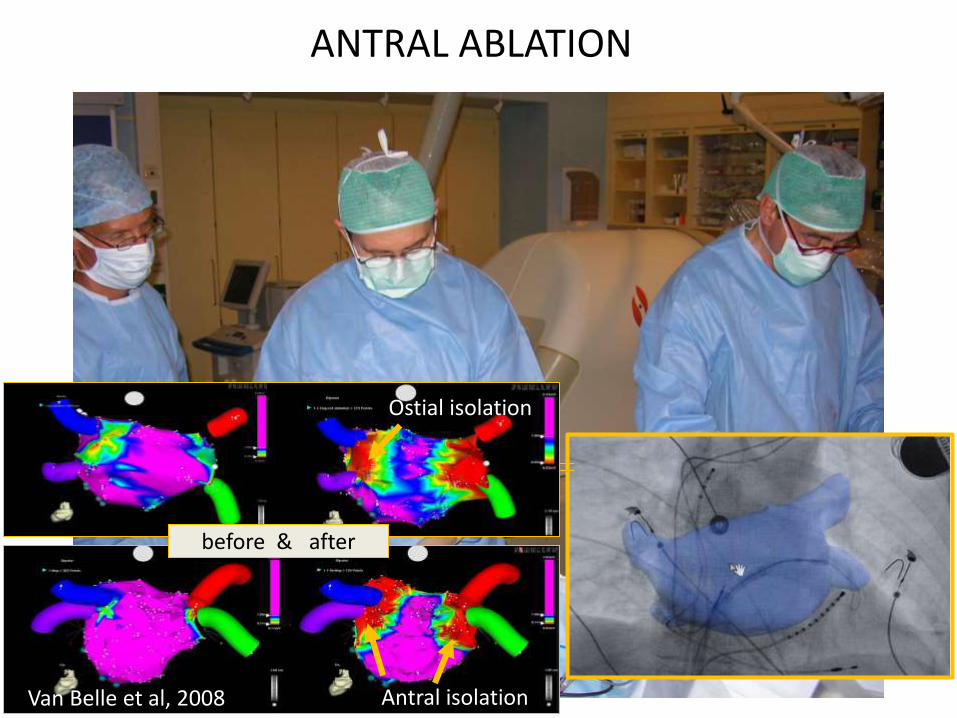
Antral isolation
Ostial isolation
before & after
ANTRAL ABLATION
Van Belle et al, 2008
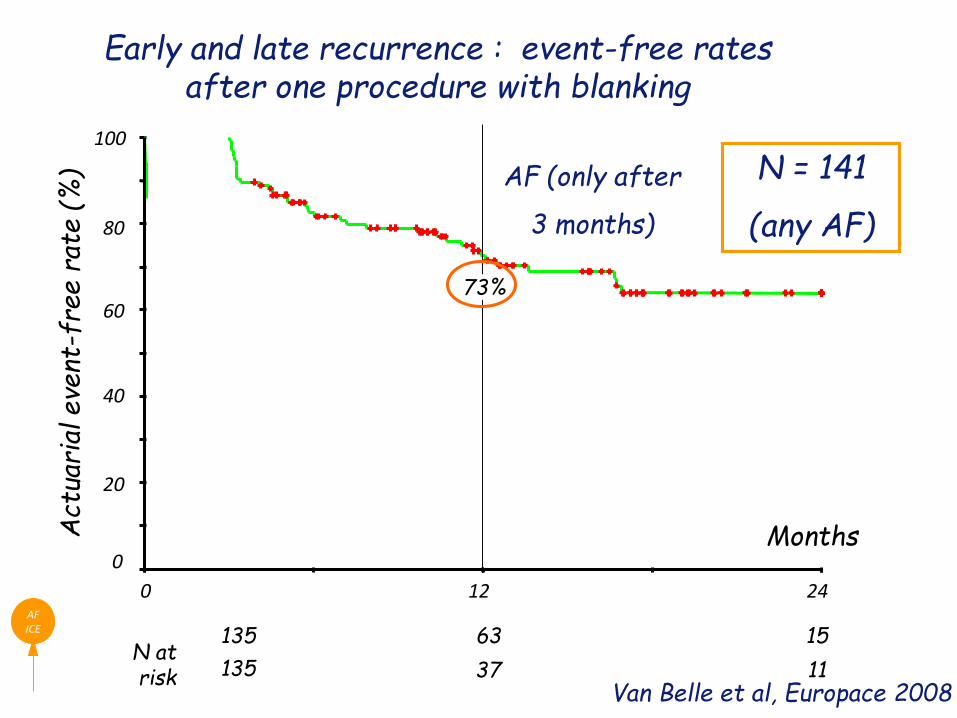
Early and late recurrence : event-free rates after one procedure with blanking
AFICE
Months
24120
Act
uari
al e
vent
-fre
e r
ate (
%)
100
0
80
60
40
20
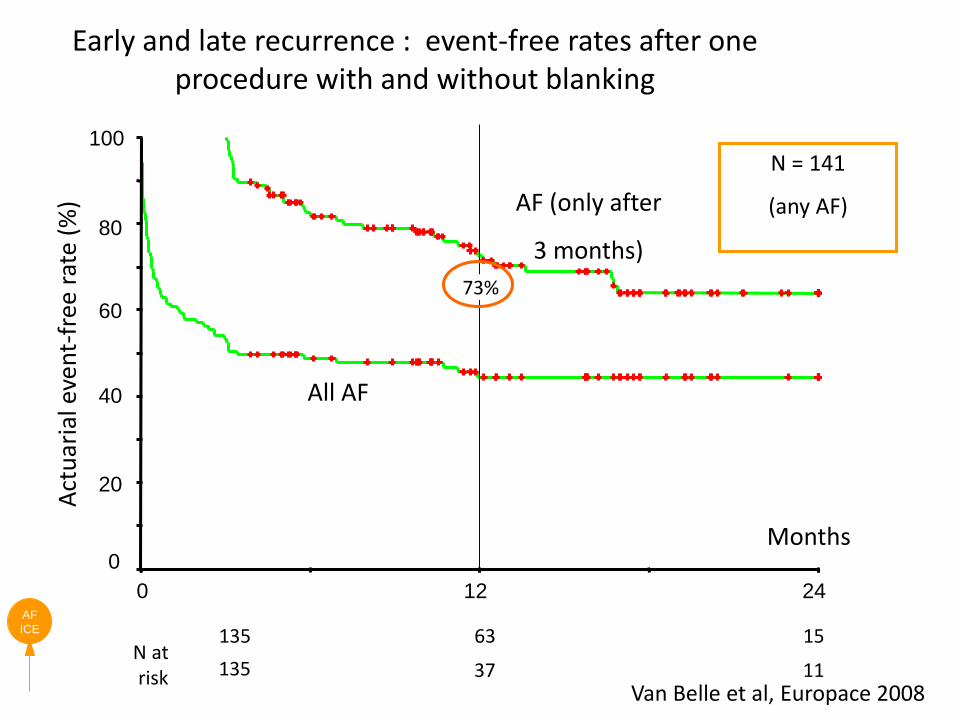
N atrisk 1137
135 1563
73%
AF (only after
3 months)
N = 141
(any AF)
135Van Belle et al, Europace 2008
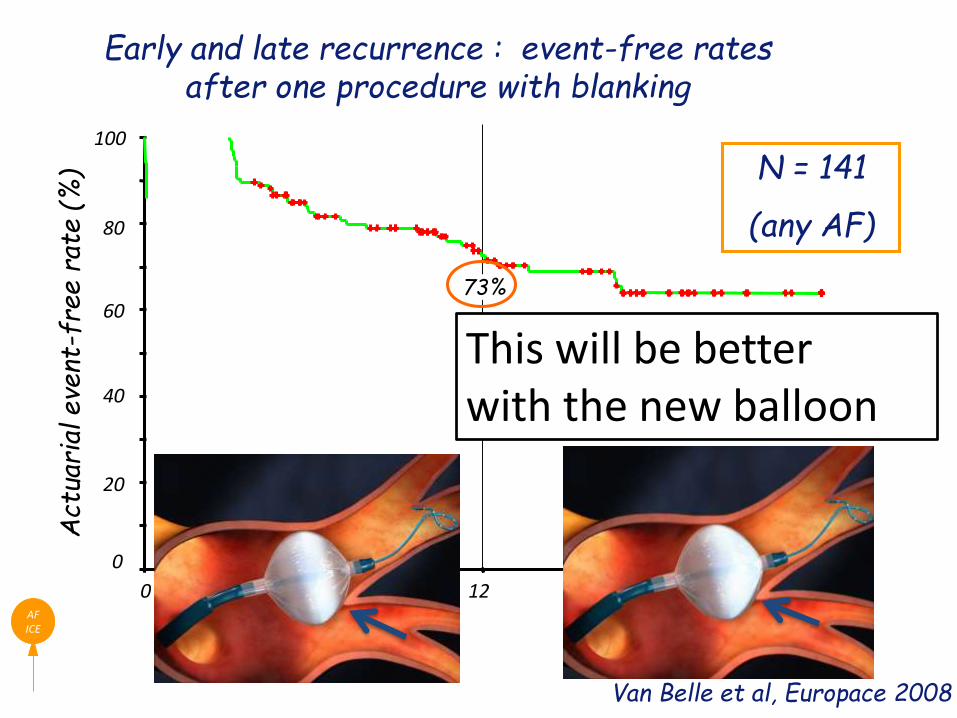
Early and late recurrence : event-free rates after one procedure with blanking
AFICE
Months
24120
Act
uari
al e
vent
-fre
e r
ate (
%)
0
40
20
100
80
6073%
N = 141
(any AF)
Van Belle et al, Europace 2008
This will be betterwith the new balloon
AF
ICE
Months
24120
Act
uar
ial e
ven
t-fr
ee r
ate
(%)
100
0
80
60
40
20
All AF
N atrisk 1137
135 1563
73%
Early and late recurrence : event-free rates after one procedure with and without blanking
AF (only after
3 months)
N = 141
(any AF)
135Van Belle et al, Europace 2008
• No PV narrowing (30% criterion; repeated MRI)
• Phrenic Nerve Palsy: 26/346 patients, usual with the small balloon
• No fistula, death, stroke…
Cryoablation with the ICE balloon:results of a multicentre study
Neumann et al, JACC 2008
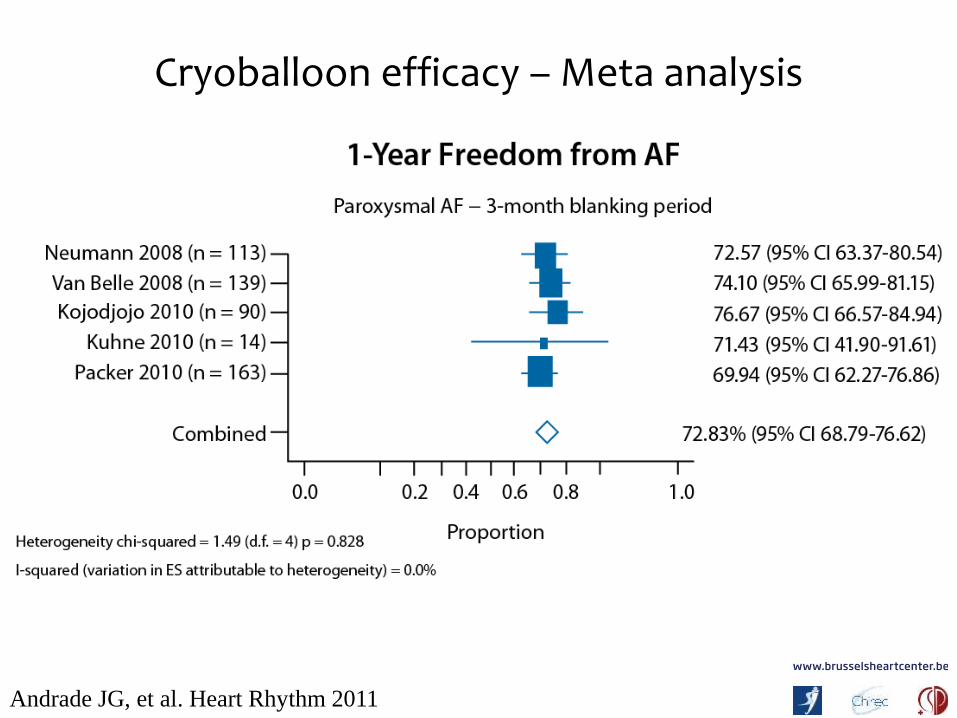
Cryoballoon efficacy – Meta analysis
Andrade JG, et al. Heart Rhythm 2011
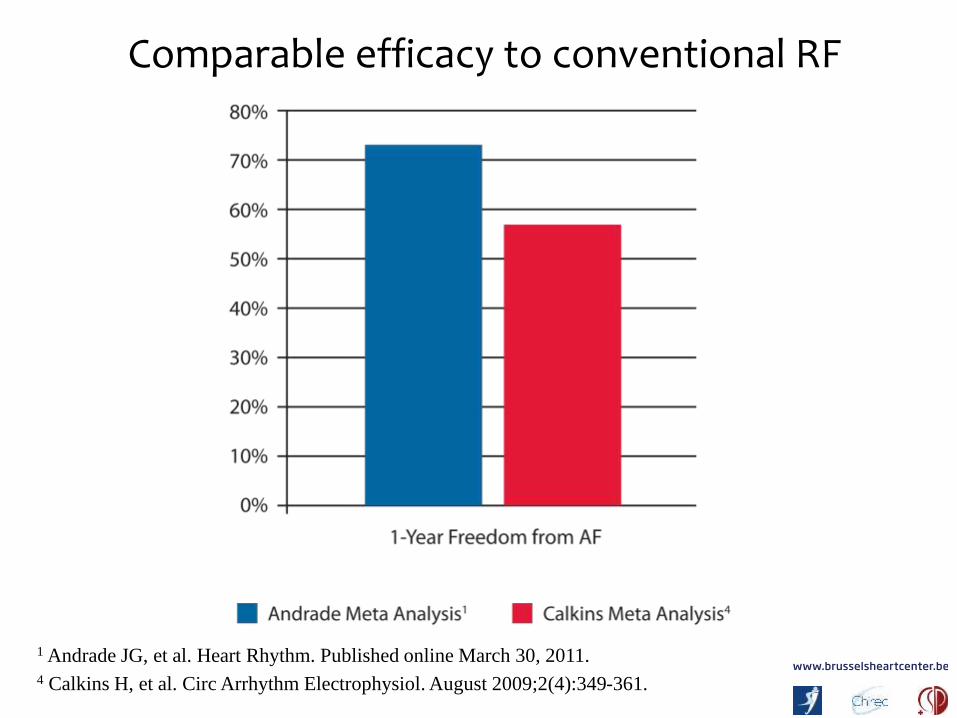
Comparable efficacy to conventional RF
1 Andrade JG, et al. Heart Rhythm. Published online March 30, 2011.4 Calkins H, et al. Circ Arrhythm Electrophysiol. August 2009;2(4):349-361.
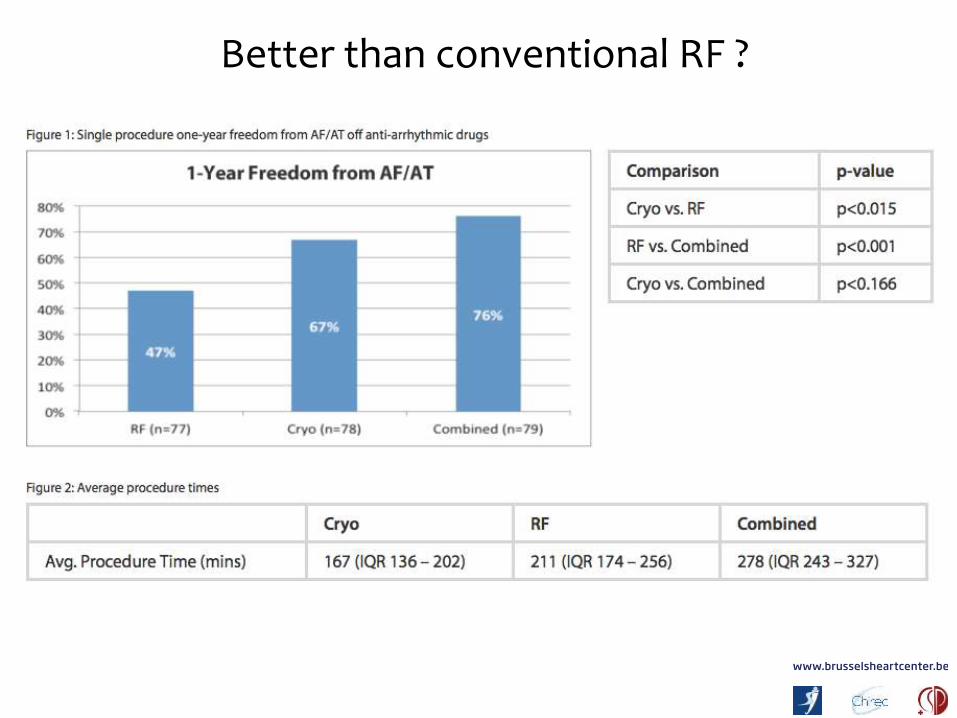
Better than conventional RF ?
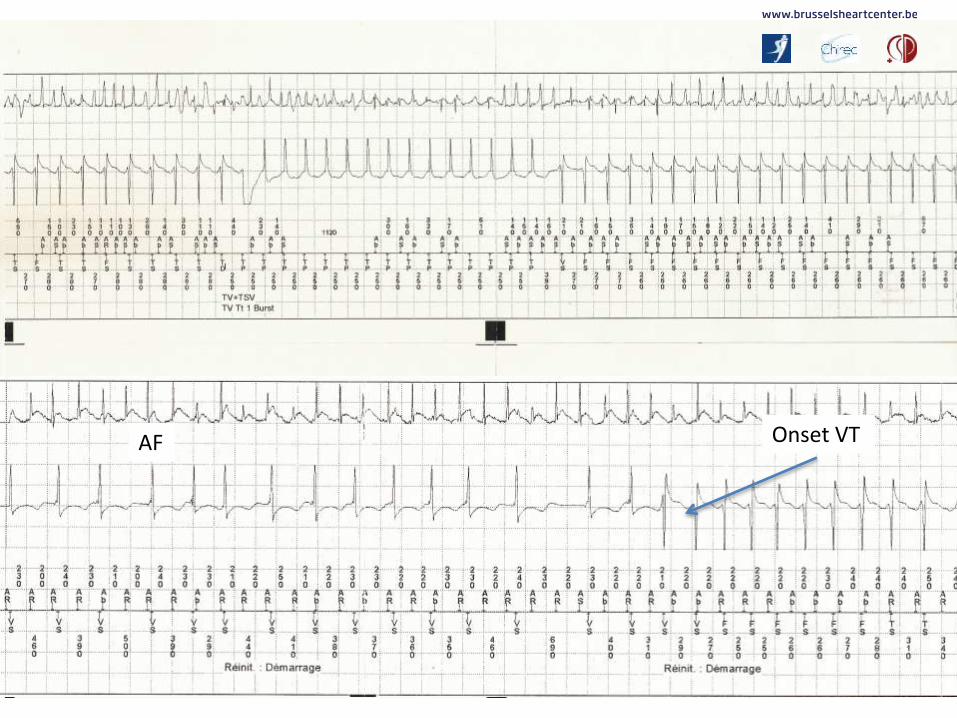
Onset VTAF
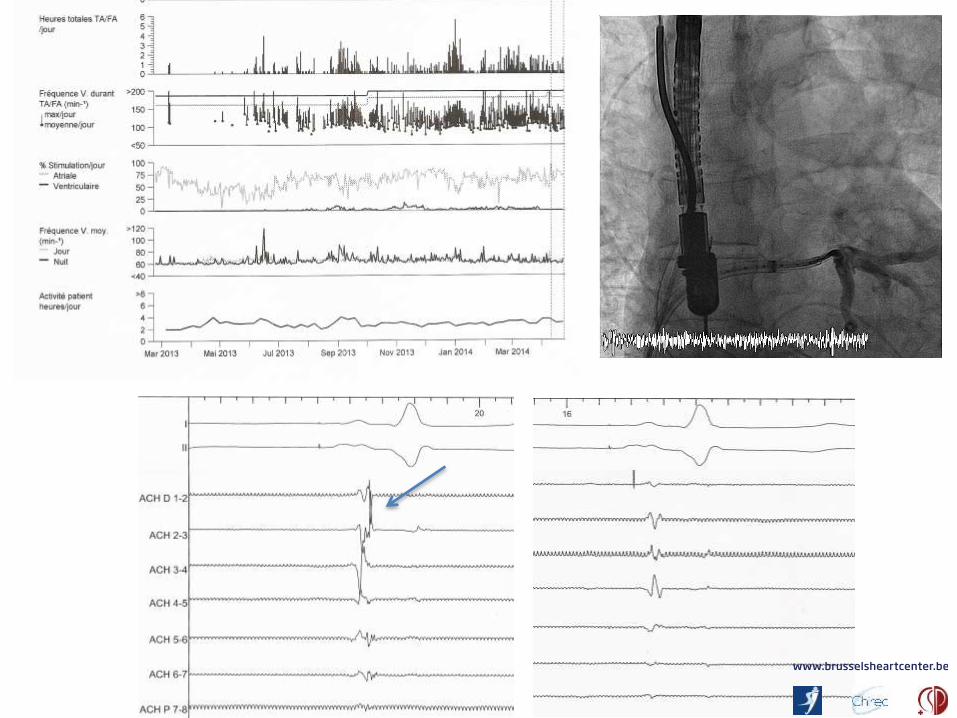
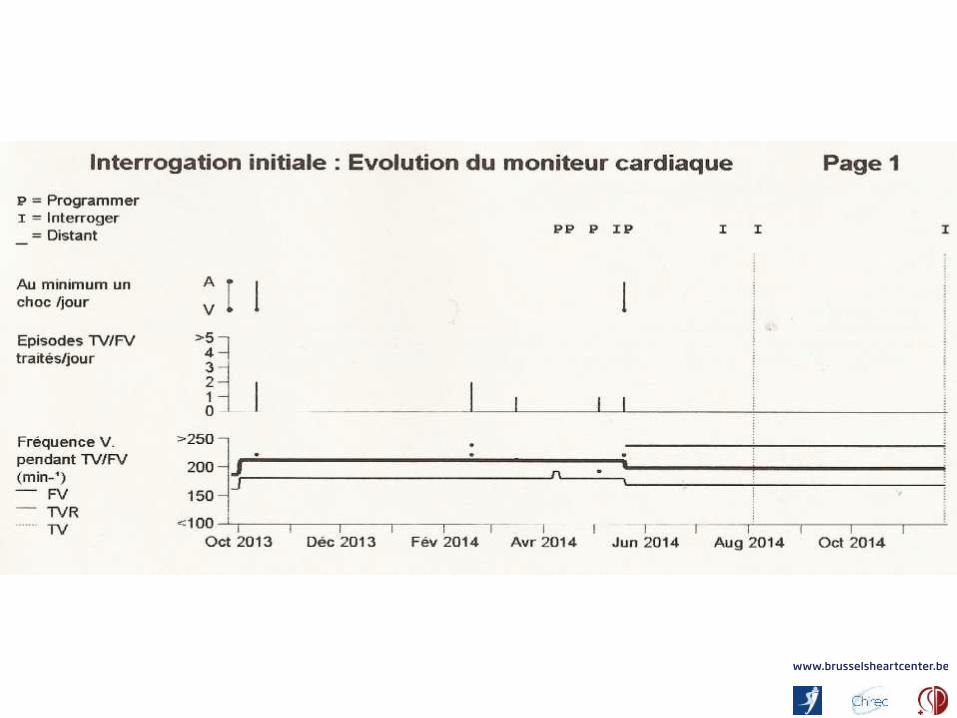
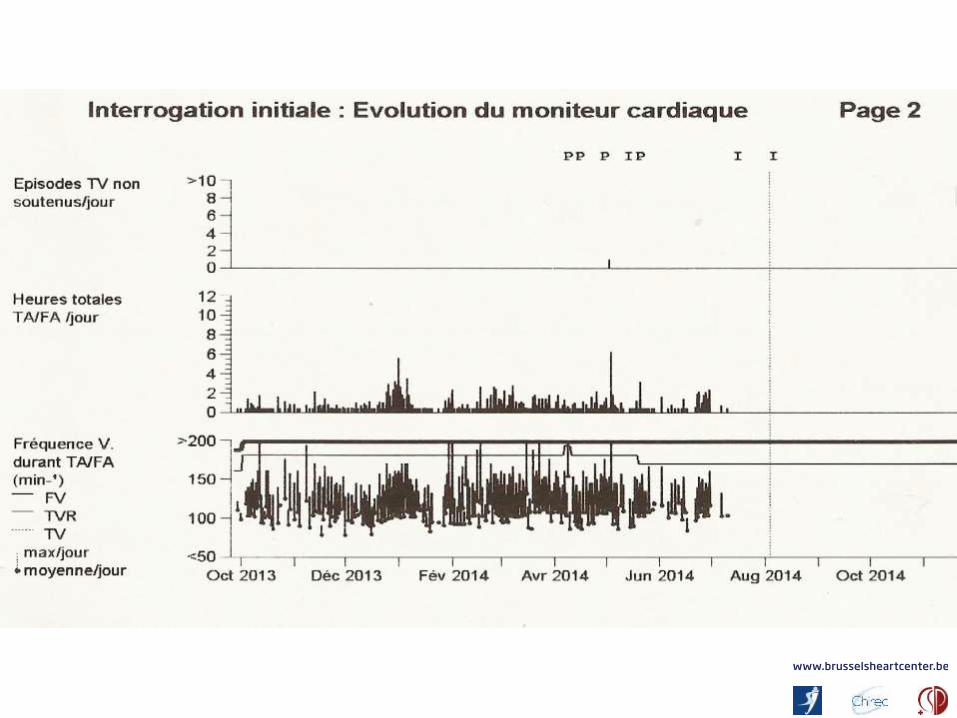
Wat zijn onze resultaten ?
blijven de zelfde na 550 procedures
( > 100 in BHC)
Geen CVA / TIA
Geen PV stenose
Geen overlijden
Persistent Atrial fibrillation: suitable for catheter ablation?
Paroxysmal Persistent Permanent
*
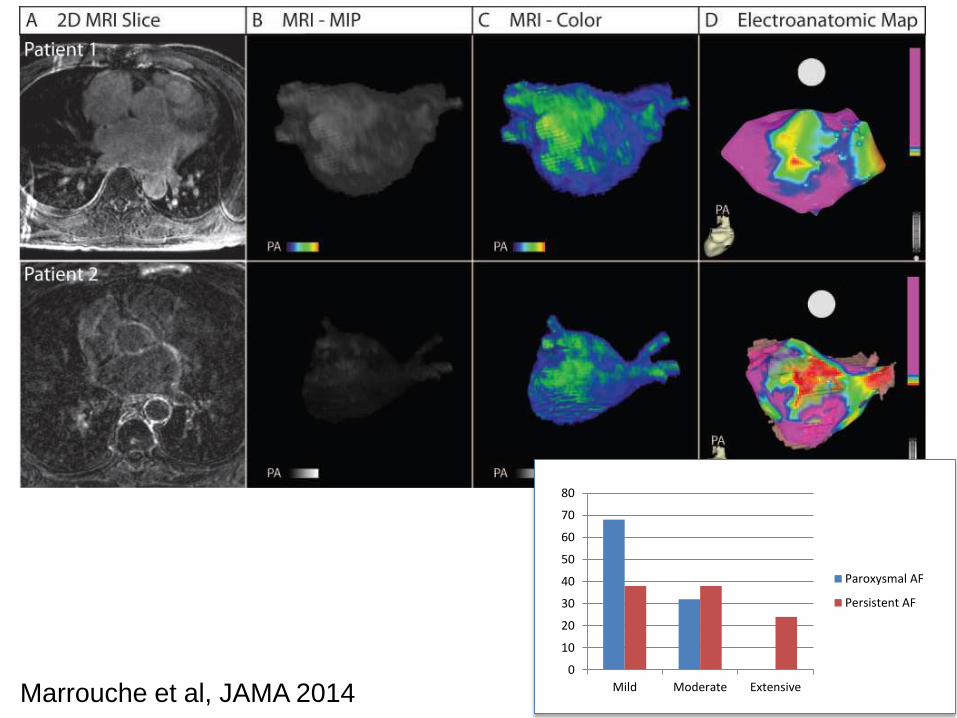
0
10
20
30
40
50
60
70
80
Mild Moderate Extensive
Paroxysmal AF
Persistent AF
Marrouche et al, JAMA 2014
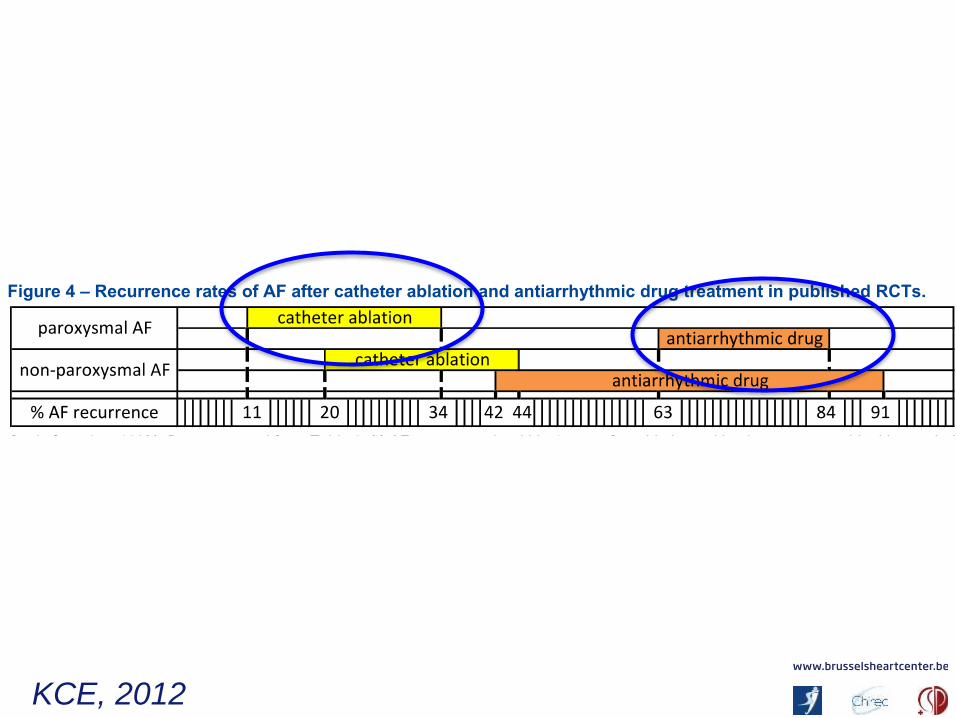
KCE, 2012
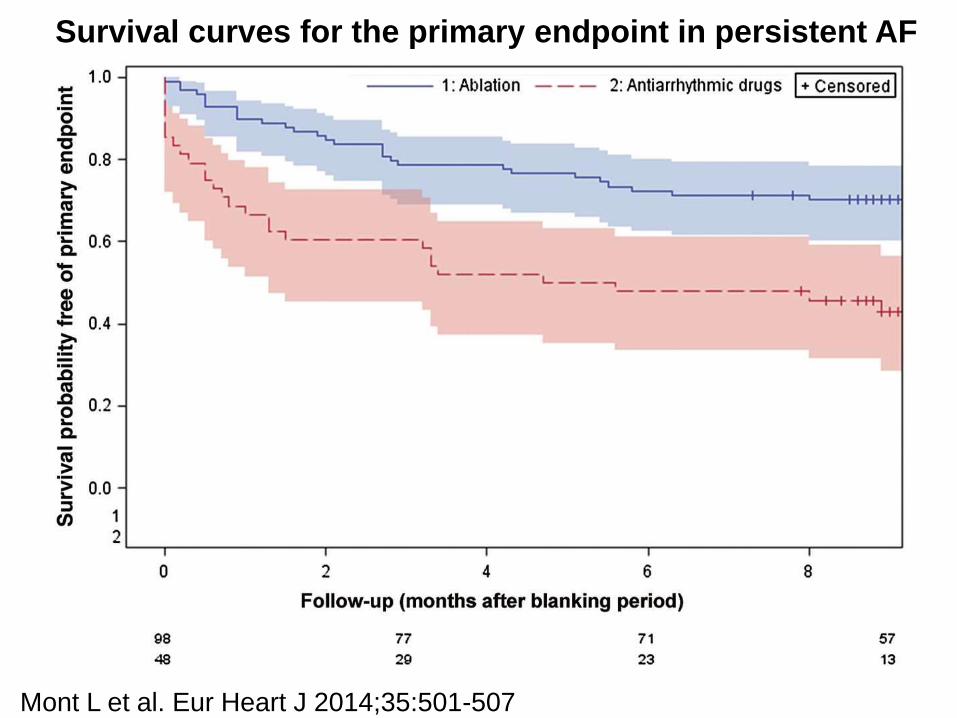
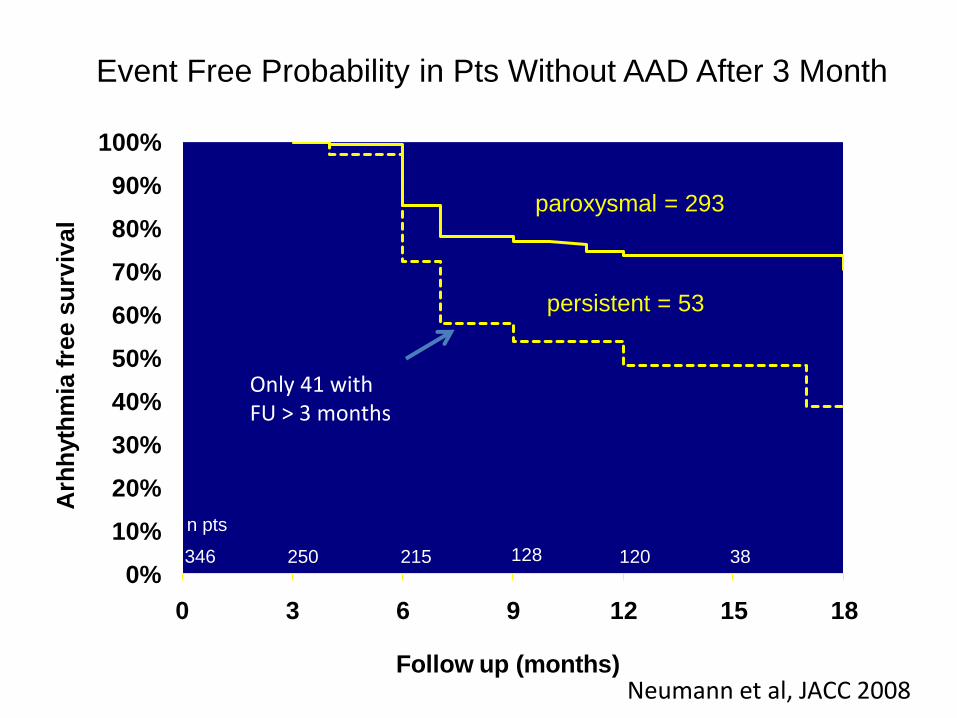
Survival curves for the primary endpoint in persistent AF
Mont L et al. Eur Heart J 2014;35:501-507
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 3 6 9 12 15 18
Arh
hyth
mia
fre
e s
urv
iva
l
Follow up (months)
346 250 38120128215
n pts
paroxysmal = 293
persistent = 53
Event Free Probability in Pts Without AAD After 3 Month
Neumann et al
Only 41 with FU > 3 months
Neumann et al, JACC 2008
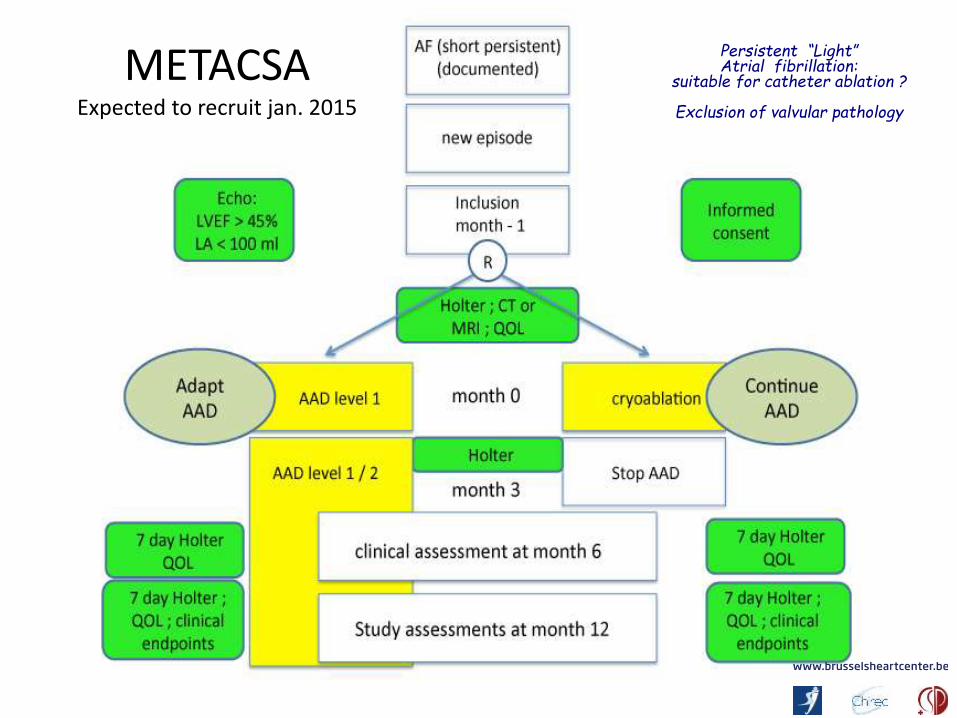
METACSAExpected to recruit jan. 2015
Persistent “Light” Atrial fibrillation:
suitable for catheter ablation ?
Exclusion of valvular pathology
METACSA (PROSPECTIVE STUDY OF MEDICAL
THERAPY AGAINST CRYOBALLOON ABLATION IN PATIENTS WITH SYMPTOMATIC RECENT ONSET
PERSISTENT ATRIAL FIBRILLATION)Expected to recruit jan. 2015
Persistent “Light” Atrial fibrillation:
suitable for catheterablation ?
Exclusion of valvularpathology
Normal atrial size
More info or a candidate ?
BHCSt LucULgUZ GentR’dam
1. Catheter ablation seems to be betterthan drug therapy for paroxysmal AF (widecircumferential ablation)
2. Persistent atrial fibrillation without valvular pathology and normal anatomyseems to be treatable with catheterablation
3. There are not enough goodantiarrhythmic drugs on the market in Belgium
PAROXYSMAL PERSISTENT
maintain sinusrhythm !
maintain sinusrhythm !
cardioversionDRUGS
DRUGS
ABLATION